
Abstract
Objective
This rapid scoping review was undertaken as part of a larger study to design a statewide operational model of grief and bereavement supports in South Australia. The aim of the review was to describe the structures, services, and components of supports offered by grief and bereavement programs in South Australia.
Methods
The review was preceded by a desktop review of gray literature and informed by the Joanna Briggs Institute methodology for scoping reviews. Databases searched included Cumulated Index in Nursing and Allied Health Literature (CINAHL), MEDLINE, PsycINFO, and PubMed. Data were extracted about specific supports, services and programs, and imported into NVivo for thematic analysis.
Results
A total of 2383 articles were retrieved, with the findings from 88 articles extracted and included. Eleven themes relating to supports for grieving and bereaved people comprised: (1) follow-up bereavement care (with health professionals); (2) counseling support; (3) bereavement coordination; (4) peer support; (5) information about grief and loss; (6) referrals and risk assessment; (7) memorial services and mementos; (8) other practical and informal emotional supports; (9) personnel; (10) staff training; and (11) staff support.
Conclusions
This review advocates for including all identified supports in comprehensive grief and bereavement care. While implementing this in full may be challenging for individual services and providers due to time and resource constraints, integrating these components at a population level should be considered. Each element plays a role in delivering holistic care, requiring the combined efforts of community action and formal service provision.
Introduction
Grief and bereavement have become pressing public health concerns globally, driven by increased mortality rates and the broad range of negative health outcomes linked to unresolved grief. 1 International research emphasizes the importance of comprehensive, coordinated bereavement support services that prioritize early intervention and personalized care for complex grief-related challenges, positioning bereavement as a critical issue across clinical practice, preventive care, and the broader community.2–4 In Australia and South Australia, despite the importance of bereavement support being articulated in strategy,5,6 this remains an area of unmet need, emphasizing the necessity to further develop grief and bereavement support services.
Much of the bereavement care literature focuses on the palliative care sector, and reviews typically limit their scope to a single bereaved population and setting.7–13 This rapid scoping review looked at grief and bereavement supports and services in Australia and New Zealand, across all bereaved populations and settings. The rapid scoping review question was “What grief and bereavement information, supports, and programs are described in the literature, and how are these characterized in terms of their scope, availability, and critical dimensions?”
This rapid scoping review was undertaken as part of a larger study looking at the costs and benefits of establishing statewide grief and bereavement support in South Australia. 14 A subset of the full review is presented in this article with the aim to understand how grief and bereavement programs or services are structured and coordinated, including key components and personnel.
Materials and Methods
This rapid scoping review used a systematic, reproducible approach 15 informed by the Joanna Briggs Institute methodology for scoping reviews. 16 Eligibility criteria were structured using the Population, Concept, Context (PCC) framework (Table 1), which enables the broad capture of literature on a topic. 17 The primary focus was grief and bereavement support provided in operational programs, rather than theoretical models.
Eligibility Criteria.
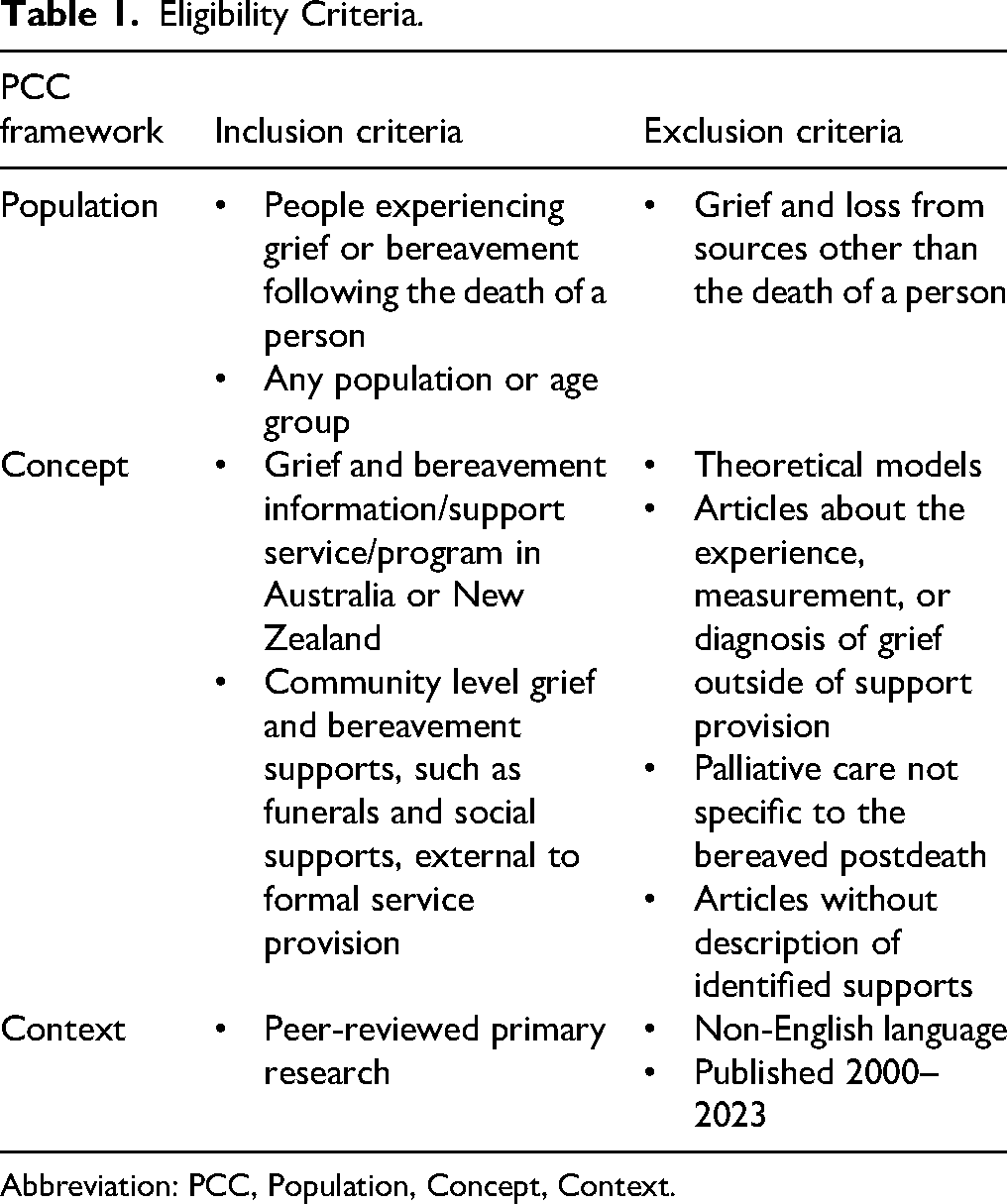
Abbreviation: PCC, Population, Concept, Context.
Comprehensive database searches were conducted through Cumulated Index in Nursing and Allied Health Literature (CINAHL), MEDLINE, PsycINFO, and PubMed in August 2023 (see Supplemental File 1), combining the following concepts: (bereavement or grief) AND (support or service or program or model) AND (Australia or New Zealand). Citations were exported to Endnote 18 where duplicates were removed, and then imported into Covidence. 19
Articles were screened in Covidence 19 by two independent reviewers, by title and abstract, then by full text using the eligibility criteria in Table 1. Conflicts were managed by a third reviewer. Reasons for exclusion were documented (see Figure 1).
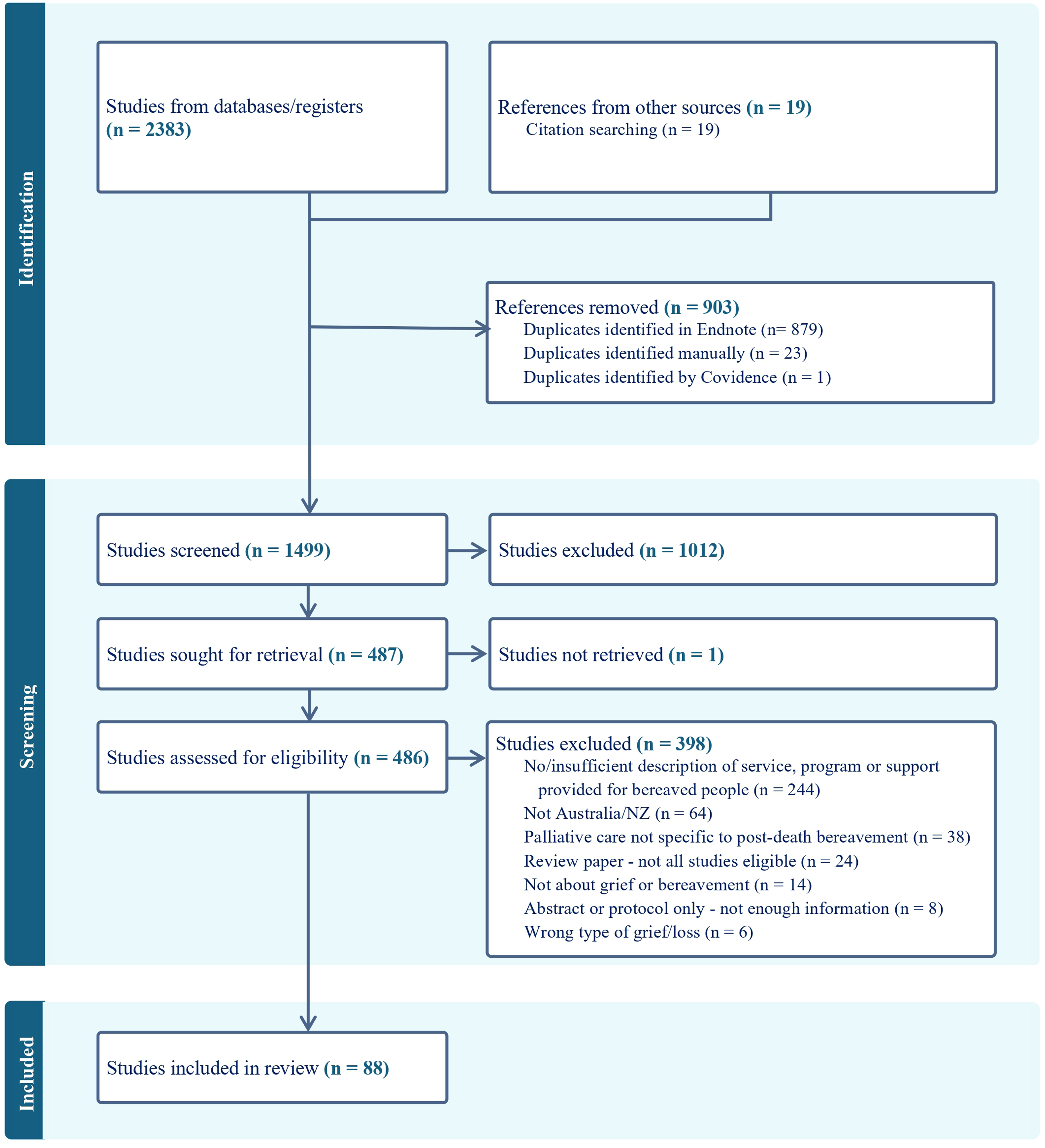
PRISMA Flow Diagram of Screening Processes. 24
Data Extraction, Analysis, and Synthesis
Data extraction was performed by four reviewers (DF, GRB, BS, and NM), then coded and themed by 1 reviewer (DF). A second reviewer checked the coding and themes (KD).
Data from eligible studies were extracted into a custom Excel 20 spreadsheet, including: author, year, title, type of study/article, sources of bereavement support, location, types of grief/death, target population/s, program/service/provider name, components/structures, links/connections to other services, innovative approaches, and tools (eg, grief risk assessment). Study and publication characteristics were tabulated. All other extracted data were coded using NVivo, 21 from which themes were generated inductively 22 using an adapted version of Braun and Clarke's methodology. 23
Results
Database searches identified 2383 articles. Twenty-three review papers were pearled, resulting in 19 additional primary studies. After removal of duplicates, 1499 papers were screened; and 88 articles describing components of grief and bereavement support were included (Figure 1).
Study and Publication Characteristics
Supplemental File 2 shows study and publication characteristics of all included articles. Most studies discussed supports offered for people bereaved from any type of death (n = 36) or specifically from terminal illness/in palliative care (n = 28). The remaining studies focused on suicide (n = 14) or infant/child loss (n = 12). Some studies described targeted supports, such as for families (n = 25), parents (n = 14), carers (n = 5), health professionals (n = 5), Aboriginal and Torres Strait Islander or Māori people (n = 4), and women (n = 3). Some services targeted bereaved adults only (n = 6), adolescents (n = 4), children (n = 4), or young adults (n = 3).
Service providers were most commonly hospitals (n = 27), bereavement-specific services (n = 19), or palliative care services (n = 11). Community supports were also common as part of a specific community bereavement program (n = 7), a community health service (n = 4), or other community setting (n = 6). Internet-based supports (n = 6), school-based supports (n = 3), government social welfare services (n = 3), clinical psychology services (n = 3), and other counseling services (n = 3) were also seen in multiple studies (see Supplemental File 2).
Themes: Components of Bereavement Support
Grief and bereavement services offered a variety of supports across eleven themes: (1) follow-up bereavement care (with health professionals); (2) counseling support; (3) bereavement coordination; (4) peer support; (5) information about grief and loss; (6) referrals and risk assessment; (7) memorial services and mementos; (8) other practical and informal emotional supports; (9) personnel; (10) staff training; and (11) staff support.
Follow-Up Bereavement Care (With Health Professionals)
Follow-up was seen primarily across hospital and palliative care bereavement services, where a team of health professionals were connected to the family predeath. Many studies conveyed the value of routine follow-up,25–28 with evidence that bereaved people often feel distressed or abandoned if this is absent, 26 or if there is sudden withdrawal of health professionals postdeath.27,28 One study in residential aged care found bereaved families were only offered follow-up if the resident had been referred to community palliative care predeath. 26
Bereavement follow-up care was mostly offered through phone calls. A survey of Australian palliative care services showed 70% of bereavement services included phone calls. 29 Similarly, rural and remote health professionals reported 73% of services offered postbereavement follow-up, primarily through phone calls. 30 Phone calls are widely used across palliative care,31,32 suicide support programs, 33 and intensive care units (ICUs).28,34–36
Written communication such as condolence cards or letters were sometimes offered instead of or alongside phone calls, soon after the death,37,38 or at milestones like the first anniversary. 30 The importance of personal, handwritten notes for sincerity was highlighted. 32 While again most commonly seen from hospital and palliative care programs, participants in one study desired this from funeral directors. 39 Some programs sent cards annually for up to 5 years, allowing families to opt in to ongoing support, 33 and some included memorial service invitations and regular newsletters.30,33,38
Home visits occasionally formed part of bereavement care, particularly immediately postdeath or after a few weeks.40–42 Face-to-face follow-up with families was also offered in some hospitals,35,43 while bereavement follow-up from other healthcare professionals, such as general practitioners (GPs), was desired but often lacking. 44 Some people who did access GPs during bereavement found them unhelpful. 27
Follow-up timing and duration varied across programs. Initial contact usually occurred within the first week postdeath, with another contact at 6 to 10 weeks.30,33,37,45,46 Some palliative care services contacted families within 3 to 6 weeks, while others provided contact at 6 months.47,48 Duration depended on the program's resources and philosophy, 32 with some tapering off after a few months to promote independence, 49 while others suggested maintenance for at least 6 months to promote continuity of care. 27 Follow-up concerns included distress when bereavement support was discussed predeath, 50 and perceived intrusiveness of phone calls. 46
Counseling Support and Other Therapies for Grief
Counseling or psychology formed one major component of bereavement care, with many articles discussing the need for or availability of grief counselors or psychoeducation,26,31,34,44,51–53 and others outlining specific counseling programs or services. Phone-based counseling services were commonly 24h crisis support lines, although the same organizations often also offered other types of counseling.53,54–57 Many bereavement programs included face-to-face counseling, or referral to formal counseling, as part of their suite of services.33,35,45,49,50,58–60 One article mentioned a codesigned online perinatal bereavement support program 61 ; 3 articles discussed a camp which included counselling support and other group therapies62–64; and 3 articles described school-based programs involving psychosocial bereavement support.65–67
Specific therapies described included Family-Focused Grief Therapy, 68 Cognitive Behavioural Therapy69,70 and trauma-specific interventions, such as Eye Movement Desensitization and Reprocessing (EMDR). 71 Other grief therapies, offered independently or as part of a counseling program, utilized nonverbal emotional processing strategies including writing,59,72–76 photography, 75 and music.73,77,78
Coordination and Navigation of Supports
Some services identified bereavement care coordination as a key component, while other studies noted its absence. Coordination was often mentioned in palliative care services, but continuation postdeath was unclear.27,79–81 Family caregivers were perceived as having the task of connecting services in the absence of formal coordinators. 47 Coordination was also called for more broadly, for example, in a nationally coordinated community disaster response strategy. 51
Several studies highlighted the need for a single point of contact to help with navigation of bereavement supports,27,30,40,52,81 and prevent distress caused by bereaved individuals having to repeatedly recount their stories. 81 Awareness of available local supports and where to seek information was limited.25,44,82
Collaboration between service providers was most evident in infant loss services, where the hospital, community health professionals, and families worked together.83–85 Funeral services also collaborated with support providers, 86 and 4 suicide-specific programs described clear collaboration and coordination processes.33,54,82,87–91 In services where this was lacking, fragmented support hindered effective bereavement care.56,81
Peer Support
Peer support from individuals or groups with similar lived experiences was another component frequently provided or desired.25,44,92,93 Some services worked to connect people or families together for in-person peer support.54,94 Virtual peer support was also offered through 24h helplines and live chats with trained volunteers,56,95 and online forums.92,96–98 One-directional support was found in written materials such as books sharing bereaved parents’ stories. 99 Some peer support also occurred organically, such as at annual memorial services. 100 Support from bereaved peers was often perceived as more helpful than from others. 101
Formal bereavement support groups, peer-led or facilitated by professionals, were widely utilized.25,27,56,102 Groups could be structured with set participants, agenda, and duration, 59 or be informal and flexible.33,92 While primarily in-person, some groups were telephone-based. 103
Community groups not specifically for bereavement, like rotary and probus clubs, church groups, Men's Shed, and mothers’ groups, also offered informal support.52,83,101,104 Additionally, staff in settings with frequent exposure to death often relied on each other for peer support. 105
Information About Grief and Loss
Another core component of bereavement care was providing grief information. One survey reported that 53% of bereaved carers were offered information about grief by palliative care services. 47 Information was usually provided in written form,29–31,37,45,47,51,54,58,59,80,94,96,106 including online.107,108 Dual verbal and written information offered at different stages of bereavement, 83 and tailored resources 58 may improve information uptake. A desire for more information was seen, 44 particularly practical information around funeral planning and legal tasks.25,39,40
Community grief education or capacity building was another essential aspect, although often suggested for future action. Potential initiatives included media guidelines for loss reporting, community grief events, and school-based education programs.51,65,75 Some support organizations emphasized raising community grief awareness as part of their core work.56,94
Referrals and Risk Assessment
Referrals to counselors, GPs, social workers, community agencies, and bereavement groups were common.27–31,37,39,41,43–47,50–52,54,59,79,80,95,109 However, referral pathways were not described, except for one study where referrals were made by hospital staff or online self-referral. 95 Counseling or specialist support referrals were usually triggered “if required,”43,45,46,79 implying informal assessments to determine those with additional needs. One survey reported that 66% of Australian palliative care services conducted some assessment process to identify high-risk individuals, but only 16% used formal tools. 29 Notwithstanding assessment results, 94% offered support to all bereaved persons. 29
Only 6 articles discussed risk assessment as part of an existing bereavement program: 4 mentioned informal assessments by research teams, multidisciplinary palliative care teams, or community nurses45,58,79,110; 2 discussed using the Bereavement Risk Index (BRI), with risk assessment outcomes influencing care or referrals.30,111 One study developed an assessment framework for secondary stressors, like financial and legal issues. 112
Memorial Services, Funerals, Rituals, and Memory-Making Activities
Memorial services or funerals were another key aspect of bereavement support, seen frequently in palliative care and hospital bereavement programs.26,28–31,35,39,42,44,45,48,100,104,112–114 Most studies emphasized family presence at these events, but some suggested that medical staff attendance increased family sense of support.25,28,32 COVID-19 restrictions presented challenges, such as limits on number of attendees, deferral of services, reduced cultural or religious rites, and shifts to virtual services.26,34,114–116 These changes caused distress among the bereaved, 26 highlighting the significance of these rituals. Public memorials, such as those held by churches, were also valuable grief support. 51 Other memory-making activities, included handprints, footprints, and photos,28,41,61,114,117,118 and memorial books, 45 quilts, 75 walls, 67 and chains. 119
Other Practical and Emotional Supports
Practical and emotional supports, often provided informally by family, friends, and neighbors included phoning, visiting, sending cards or flowers, providing meals, assisting with childcare and household tasks, helping with funeral arrangements, attending funerals, and offering financial assistance.28,101,104,120 However, many articles noted these supports as more desired than experienced, especially regarding assistance with administrative tasks and legal obligations such as funeral planning, notifying organizations of the death, transferring ownership of accounts, estate settlements, and managing changes to pensions and government support.3,40,121,122 Anderson et al 123 highlighted concerns about bereavement leave entitlements, particularly impacting Aboriginal and Torres Strait Islander people. While social networks often provide valued emotional support,101,120 nearly a third of grieving individuals did not receive the support they desired. 124 Effective social support, when perceived as helpful, is crucial for positive bereavement outcomes.57,124
Personnel
Few articles detailed the specific professionals involved in bereavement support provision. Two studies surveyed palliative care bereavement services across Australia: coordinators were typically nurses or had specific grief-related titles, and professional qualifications included nursing, social work, counseling, religion/theology, and psychology.3,29 In ICU settings, Australian services were largely provided by social workers, while New Zealand services were mainly managed by nurses. 35
Ten more studies reported providers’ professions. Social workers led bereavement support in palliative care units, 31 a hospital bereavement service, 38 ED, 37 and a suicide support program. 33 Nurses led some hospital follow-up services,43,109 and provided bereavement support in a cancer center alongside a counselor. 113 A multidisciplinary team led the Pregnancy After Loss Clinic, 85 and another perinatal program was supported by specially trained social workers and psychologists. 58 The StandBy Response Service utilized a skilled Crisis Response Team, though qualifications were unspecified. 54
Abbott et al 29 reported that bereavement coordinators were often part-time and salaried, with most services employing 2 to 3 personnel, and less than 5 volunteers. StandBy coordinators worked full-time, being on-call for crises. 91
In-Service Staff Training in Grief Support
One survey reported 62% of palliative care services provided specialized bereavement training to staff, ranging from less than 8 h to more than 16 h. 29 A similar survey in ICUs found that most staff received additional training for their bereavement roles (70.5%). 35 In New Zealand, two-thirds of hospice volunteers providing bereavement support had general volunteer training, but only 37% received training in bereavement support skills. 125 A few programs included staff training as part of their service.37,58,95 Bereavement care training in Australian maternity settings was considered ‘nonessential’ and consequently paused during COVID-19. 114
Staff Support for Grief
People who provide grief support, or otherwise encounter death, in paid or volunteer roles, may require emotional support themselves to deal with grief.51,126 Debriefing opportunities were often reported as missing,51,81,105 and few articles described this as a component of their programs. One article reported that 57% of hospices offered volunteers some supervision support (usually monthly) and most organized social gatherings. 114 Other articles mentioned staff utilizing limited employee assistance programs or other workplace counseling for debriefing.43,79,95,105 One program instigated a 6-monthly debrief with a specialist psychologist due to the emotional complexity of providing grief support. 46
Informal debriefing with colleagues appeared the most common form of staff support,43,79,127 often in the perceived absence of sufficient other options. 105 Colleagues also provided a listening ear from someone who understood the role and workplace context and were safe to discuss difficult issues with. 105 As with other supports, staff mentoring and peer support activities decreased during the COVID-19 pandemic.34,114
Two articles discussed external supervision for staff. One grief center offered clinical supervision for professionals from other organizations whose work involved bereaved or dying clients, 60 and one community suicide support program mandated external counselor supervision for coordinators to help them navigate the personal impact of dealing with constant complex trauma. 126
Discussion
As in previous reviews and studies internationally,7–9,11 much of the Australian and New Zealand literature focuses on bereavement support in palliative care and hospital settings. This review integrates this with other community settings and informal sources of support to offer a comprehensive overview of the components of grief and bereavement care in Australia and New Zealand. Eight components of support for bereaved people, and 3 themes relating to support providers were identified. Some components were offered more consistently in certain contexts, for example, individual peer support in community suicide postvention programs, or follow-up with health professionals in hospital and palliative care settings. However, all 8 identified components targeting bereaved people appeared applicable across all populations and settings.
While our review did not focus on intervention effectiveness, our themes are reflected in the broader international literature. For some components, there is an extensive body of evidence to draw upon, for example, in regard to formal counseling and psychological interventions for grief.128,129 Some programs which coordinate postvention suicide support have also undergone numerous evaluations supporting their effectiveness,54,82,88–90 although more broadly, limited evidence of effectiveness of suicide postvention interventions has been reported. 130
Bereavement Follow-Up
The effectiveness of bereavement follow-up in the international literature is mixed. A review of follow-up programs in intensive care found inconsistency between symptom-based and experience-based outcomes: although follow-up seemed to be generally appreciated, some studies simultaneously reported no measured benefit or even worsening of grief symptoms. 131 Another review concluded that multicomponent follow-up was needed to lower the risk of prolonged grief. 132 Many of the components discussed in our review were examined in another review which reported that participants perceived brief contact interventions as valuable and necessary, and they demonstrated some positive outcomes including improved grief, depression, and wellbeing symptoms, but they were not always found helpful. 133 While follow-up is clearly an important aspect of bereavement support, the specific mechanisms and delivery of these supports may need further investigation. In addition, minimal, nonpersonal or noncompassionate follow-up that feels like tokenism is insufficient. 27 Where it applies, follow-up from the professionals most closely involved with the family predeath is important,36,37 highlighting a critical role for palliative care providers.
Peer Support and Memorial Activities
Peer support services for bereaved people also show potential benefits including reduced grief symptoms, improved wellbeing, and personal growth. 134 In addition, both our review and Bartone et al 134 found evidence that support from peers with similar loss experiences is perceived as more helpful than support from those without.
While international evidence is inconclusive regarding the impact of funeral practices on family mental health and bereavement outcomes, it suggests benefits from the social support and connection, and from after-death rituals that are personally meaningful. 135 Qualitative evidence also supports the value of opportunities to create or keep meaningful mementos.136,137 Peer support and memorial activities can form part of formal service provision, but they can also be offered informally within communities, suggesting these components of bereavement care intersect community and health/social care.
Infant Loss and Child Grief
Evidence from infant loss programs further underscores the importance of tailored, continuity-based models of care. Parents engaged in the Special Delivery Service felt less isolated and better able to normalize and negotiate their grief within their partnership. 84 Similarly, the Pregnancy After Loss Clinic was valued not only for its direct benefits to mothers but also for perceived positive effects on partners, children, and extended family. 85
Evaluation of grief-specific programs for children highlight both psychosocial and relational benefits. For example, participation in the Lionheart Camp for Kids reduced children's self-reported grief, while caregivers observed improved peer interactions. 119 These findings suggest that structured peer and caregiver supports can positively influence both child wellbeing and family dynamics, pointing to the broader relational impact of bereavement interventions. 119
Risk Assessment
Offering the right advice, information and/or referrals requires insight into individual needs, making assessment essential for the provision of bereavement support, 138 yet bereavement risk assessment was rare in our scoping review. Given the adverse impacts of prolonged grief, 4 and how different types of supports are best suited to different levels of need, 139 systematic bereavement risk assessment has potential to enable more effective and economical use and distribution of bereavement support resources. 138 Palliative care bereavement support standards recommend risk assessment predeath, within 3 to 6 weeks postdeath, and around 6 months postdeath where high risk of prolonged grief is identified. 140 However, there is little evidence that bereavement risk assessment is used in any consistent or widespread way.
Service Providers
The possibility of vicarious trauma in those working with traumatized populations has been long established, 141 including people working in death, dying, and bereavement. 142 However, emotional support systems for providers themselves in dealing with grief in their work appears infrequent as a core component of bereavement support services. While multiple reviews discuss supporting health professionals who experience patient deaths in clinical practice,143–145 there is little evidence of widespread integration of grief support for staff in the structures of bereavement programs. Similarly, reviews around grief training focus on the broader grief education of health professionals,146–148 rather than training offered within bereavement programs to equip those providing support with requisite knowledge and skills. Even external to bereavement support programs, Hall and Henning 149 conclude that death education remains inconsistently available across formal graduate and undergraduate degree programs, and while professional development opportunities in bereavement exist, there are significant access barriers.
Limitations
Due to constrained resources, the search was restricted to few databases and limited to English-language publications, so potentially relevant studies may not be captured. Only peer-reviewed literature was included; selected aspects of the gray literature were explored but these findings are reported separately. 14 The review was further limited to studies published after 2000, excluding earlier relevant work, though a preliminary search suggested this was unlikely to have significantly influenced the findings. The 2023 end-date also indicates possible missed recent publications, however, we believe retrieved and included articles remain relevant. Finally, the descriptive design of this rapid scoping review prevents conclusions from being drawn about the effectiveness of different grief supports or their impact on the quality of bereavement care.
Conclusion
This rapid scoping review identified varying levels and types of care, spanning from the specialist professional input from some types of counseling to the potential informality of supports that can be offered by families, friends, and local community members, building a case for the inclusion of all identified components in the provision of comprehensive grief and bereavement support. The practicality of this on the level of individual services and providers is questionable, with acknowledged limitations on both time and resources, but the integration and availability of all components at a population level should be considered. Consequently, service providers in palliative care and broader health and social welfare systems should seek to understand and harness community action and its potential for integration with formal processes and programs, to enable comprehensive grief and bereavement support across the population.124,139,150
Supplemental Material
sj-docx-1-pal-10.1177_08258597251392312 - Supplemental material for Components of Grief and Bereavement Supports and Programs in Australia and New Zealand: A Rapid Scoping Review
Supplemental material, sj-docx-1-pal-10.1177_08258597251392312 for Components of Grief and Bereavement Supports and Programs in Australia and New Zealand: A Rapid Scoping Review by Deborah Forsythe and Kate Davis in Journal of Palliative Care
Supplemental Material
sj-docx-2-pal-10.1177_08258597251392312 - Supplemental material for Components of Grief and Bereavement Supports and Programs in Australia and New Zealand: A Rapid Scoping Review
Supplemental material, sj-docx-2-pal-10.1177_08258597251392312 for Components of Grief and Bereavement Supports and Programs in Australia and New Zealand: A Rapid Scoping Review by Deborah Forsythe and Kate Davis in Journal of Palliative Care
Footnotes
Acknowledgments
This review was part of a larger project governed by a Project Board, and the authors acknowledge the contributions of its members. In particular, the authors thank Kate Swetenham and Mariana Ricci for their significant input. They also wish to acknowledge and thank Marion Eckert and Greg Sharplin for their contribution to planning and supervision of the review, and Kate Kennedy, Nicholas Marlow, Gabriele Raine Baljak and Barbora Skacelova for their contribution to the article screening and data extraction process.
Ethical Approval
This study did not involve research on human or animal subjects and was not subject to ethical approval. The research exclusively focused on a review of publicly available peer reviewed literature.
Author Contributions
DF, ME and GS were involved in scoping review concept and design; DF, KD, KK, GRB, BS and NM in screening of articles; DF, GRB, BS and NM in data extraction; and DF and KD in analysis, interpretation of the data, and drafting, critical revision and finalization of the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the South Australian Department for Health and Wellbeing and The Hospital Research Foundation Group under a Request for Quote [reference number A4771790].
Declaration of Competing Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the corresponding author, DF, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.