
Abstract
Introduction
Being by the bedside of a loved one who is dying can be challenging, as relatives juggle a multitude of practical problems, emotional difficulties as well as an uncertainty about what to expect.1-3 Existing research shows that relatives seek jargon-free and honest information and communication as well as compassionate care that will help them to understand what to expect before, around the time of death, and immediately after.2-6 This includes practical information about looking after their loved one in those final days or hours, exploring fears and dispelling any myths, being prepared for the physical process of dying, and given opportunities to say goodbye.2,3,7 Yet, research shows that relatives’ information and communication needs are not always met,3,8 and when this happens, relatives may feel isolated, disillusioned, frustrated and distressed.9,10 This makes the need for explicit, honest and understandable information and communication ever more urgent. 11
In response to relatives’ need for jargon-free and honest communication at the end of life of their loved one, the Centre for the Art of Dying Well at St Mary's University, UK, in collaboration with Lancaster University Medical School and St Oswald's Hospice, Newcastle, UK, created a guide called ‘Deathbed Etiquette’ – an A4 sized sheet with 15 short statements, offering guidance and gentle reassurances about being by the bedside during the last days or hours of someone's life. 12 The guide, designed by a group of clinicians, academics and communications experts, was first released in 2019, and another for when relatives cannot be present was released in 2020 in response to the Covid-19 pandemic. Both versions have received widespread media coverage, including the Financial Times, The Guardian and the BBC, among others.13-18
The aim of this study was to explore the views of healthcare practitioners on the guide and how it might be used within end-of-life care. Providing an account of their views will contribute to the evidence base needed to develop effective information and communication for relatives at the end of life.
Methods
The study was designed to develop a deep and accurate understanding of the views of healthcare practitioners on the guide, hence the case study design was selected. 19 The study was approved by the Research Ethics Committee in the Faculty of Health and Medicine at Lancaster University (reference number: FHMREC 20078 1 Feb 2021).
Sample and Recruitment
The study was carried out in the UK. A purposive sample of hospice staff working in one of three participating hospices was selected as well as a purposive sample of practitioners with experience in end-of-life care who had previously commented on the guide on social media. Sampling and data collection continued until data saturation. The inclusion criteria for the participants were: (a) working in a UK health or social care setting in a role that primarily or partly encompasses support for patients at the end of life and their families, (b) aged 18 +, and (c) English speaking.
Potentially eligible hospice staff were approached via email by hospice site staff and invited to take part. Other practitioners with experience in end-of-life care who had previously commented on the guide on social media were approached by a member of the research team using contact details available in the public domain. Other eligible practitioners were also recruited via social media channels. An online recruitment flyer was distributed via Twitter and Facebook, and eligible practitioners were invited to contact the research team. All participants were informed about the aim and objectives of the research. Consent was obtained from all participants before the start of data collection.
Data Collection
Semi-structured focus groups were conducted online, and individual semi-structured interviews were conducted either online or over the phone. When data collection took place online, a secure digital video conferencing software was used. A topic guide was used to guide the discussions (available in the supplemental material) and to ensure consistency across focus groups and interviews. The same topic guide was used for focus groups and individual interviews. Focus groups were conducted by LD, MF and KS, and interviews were conducted by LD and MF, all with previous experience in conducting focus groups or interviews. Focus groups lasted approx. 1 h and on average, the interviews lasted 40 min (range 30-50 min). They were digitally recorded, anonymised and transcribed verbatim. Data were collected between February and April 2021.
Data Analysis
Data were analysed inductively using thematic analysis. 19 Following familiarisation with the data, transcripts were coded using Nvivo 12 Plus. An initial set of codes was generated and developed into a coding scheme that was applied across the dataset. Comparison across the dataset allowed regularities (themes) to be identified. MKF led on the data analysis with input from LD, MF and AG, who had all read the transcripts. Emerging themes and findings were discussed with the team on a bi-weekly basis.
Results
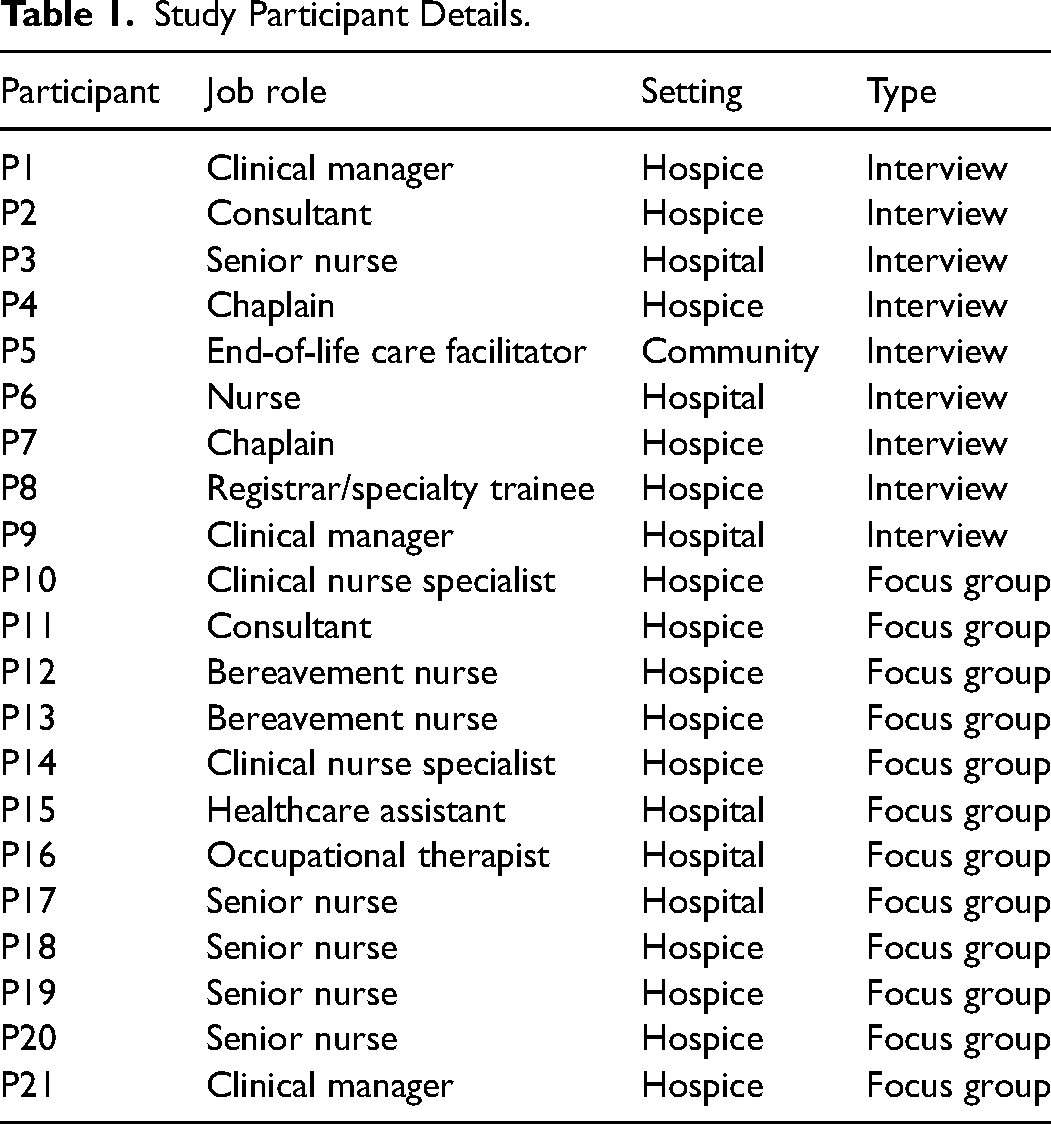
Three focus groups (n = 5, 3, 4) and nine individual interviews were conducted. In total, 21 participants took part in the study, all with university/degree level education except the healthcare assistant. See Table 1 for further details on participants. Most of the participants had not yet used the guide in a professional context, only two participants had.
Study Participant Details.
All participants were very positive and supportive of the guide, viewing it as a potentially very effective tool in supporting relatives with advice and reassurance.
Three broad themes emerged from the discussions: the importance of normalising experiences of being by the bedside of a dying loved one; the guide as an important and effective training tool for healthcare practitioners; and participants’ reflections on how best to introduce and implement the guide in practice.
Normalising Experiences of Being by the Bedside of a Dying Loved one
A Need to Talk About Death and Dying
Participants discussed how they often see relatives not knowing what to do or say at the bedside, and participants were therefore very supportive of the guide in its aim to normalise the need to talk about death and dying. The guide was described as giving relatives the words to talk about death and dying with participants commending its short sentences and simple language for being ‘extremely reassuring’. I know there are lots of books and textbooks and there are some generalised resources which are okay, but I think I love the simplicity of this material. (P7)
Yet, a tension around the use of the words ‘death’ and ‘dying’ was identified. On the one hand, participants felt that the words can be harsh sounding and expressed worry about upsetting relatives, yet on the other hand, they agreed that it is important to tell it as it is, and not speak in codes, as doing so can lead to confusion and relatives not realising that their loved one is in their final days or hours of life.
Many participants expressed concerns about the word ‘deathbed’ and its connotations, especially how it would be perceived by the public. They described the word as old-fashioned and not commonly used and expressed concern about some people possibly not understanding what it means. Some did not like the bluntness of the phrase, viewing it as ‘quite harsh in its sounding’ (P17) and ‘a mouthful’ (P4). Others did not mind the word, but still commented on its unusualness, ‘it just sounds odd’ (P6). The discussions highlighted a need to have a shared vocabulary for talking about death and dying that should be familiar and accessible to everyone.
No Rules for How to Behave
Participants felt that it was important to convey how experiences of being by the bedside can be varied and that what is right for one person is not necessarily right for another. Some participants, therefore, did not like the word ‘etiquette’ in the title. I think sometimes people think ‘my relative is dying so now I have to hold a bedside vigil and wait for them to die’, and that is really difficult, I think, so I think sometimes giving people that acceptance that we wouldn’t expect that, there's no judgement, we won’t judge you, whether you’re here or you’re not here, because you need to do what's right for you. (P8)
The discussions highlighted a need for the guide to not set up certain expectations for how to behave, especially since end-of-life situations can potentially be very difficult experiences for relatives. Participants spoke about relatives struggling to accept that their loved one is dying and about relatives who find the death of their loved one very distressing. They thought that the guide should be portrayed and introduced as a supportive guide, and therefore suggested using a different title.
De-Medicalising End-of-Life
Participants shared a concern with death, in general, being too medicalised. They, therefore, expressed a dislike with the image that many of them thought looked ‘medicalised’, and not realistically representing what death and dying is like, describing the image as ‘very hospital focused’ (P16) and ‘too clinical’ (P15). They worried about false expectations and unnecessary worry on behalf of relatives. There's, like, a drip hook, which you wouldn’t have with somebody necessarily who was actively dying. That's another thing that we have lots of conversations around the ward. (P16).
Guide to Support Practitioners in Having Conversations with Relatives
Discussions highlighted the importance of the guide being used to support healthcare practitioners and students in having conversations with relatives, either in person or over the phone. This includes new and less experienced practitioners as well as those who do not feel confident or comfortable having conversations with relatives of a dying person. There is a massive need for this across the board really, not just with nurses and doctors and certainly not just with palliative care […] GPs, district nurses, they all need this. (P4)
Providing an End-of-Life Language
The guide was described as providing practitioners with ideas on what to say, including a ‘repertoire of phrases’ (P8), and helping them to think about ‘hints and tips’ for how to support families (P4). It was thought to give practitioners the reassurance that ‘having a kind heart’ and ‘just presence and being there’ can make a big difference to relatives (P12). This was considered important, especially since some participants expressed the view that there still exists an unease among practitioners about talking about death and dying. Now it's a bug bear with me that people who work with the dying don’t like having these sort of conversations […] We’re supposed to be the specialists of dying and we won’t talk about dying, which I do find quite frustrating sometimes. (P4)
Others commented on the need for ‘getting the language right’ (P3), and not ‘talking in euphemisms’ (P5) that can lead to misunderstandings, and how the guide could help address this need.
The Guide as a Training Tool
Participants saw the guide as an important training tool helping practitioners to understand and communicate what is happening at the very end of life. Participants discussed several approaches for its introduction such as including the guide as part of training packages, for example, as part of e-learning modules on end-of-life care or induction sessions for new staff and students. A personal introduction was thought to be the best and most effective approach to engage staff, for example, introducing the guide at training days that would allow people to discuss the guide and ask questions, rather than emailing the guide to staff.
While most agreed an introduction to the guide is needed, other participants thought it was best to incorporate the guide into ad hoc training on the wards. Some suggested using ‘champions’ or ‘ambassadors’, who could have a chat with each staff member. They could individualise its introduction, taking into account each person's experiences and be attentive to any reluctance that could hinder its uptake in practice. Leaving the guide as a poster in the staff room, as another participant had suggested, was therefore thought to be ineffective.
Despite disagreement on how best to introduce the guide, most participants agreed that the guide needs to be introduced to staff and into clinical practice for it be effective.
Implementation of the Guide in Practice
Timely Introduction of the Guide to Relatives
Participants agreed that the guide must be introduced in a timely and compassionate way. Rather than leaving the guide to be picked up by relatives themselves or the guide becoming ‘a tick box thing’ (P21), most participants thought it best to introduce the guide to relatives following an initial conversation with a healthcare practitioner about their loved one dying. Some suggested that the guide could be introduced once relatives start to ask questions.
Getting to know the relatives and building up rapport with them were highlighted as important in order to assess when to introduce the guide. Introducing the guide too soon could potentially be distressing. Tailoring its introduction to the needs of each family was, therefore, felt to be important. [S]ometimes some people aren’t ready to hear those things or don’t want to hear those things even though they are happening right in front of them. And so I think it is getting to know the family, the relatives, and sort of using it sort of bespokely to that person who needs it. (P12)
Participants agreed that the guide should be introduced by the person who will have that initial conversation about their loved one dying. Being able to answer questions about the process was seen as crucial, and delivery would therefore be challenging for practitioners who cannot provide an answer.
Discussion
The study findings highlight several potential benefits of using the guide to Deathbed Etiquette in end-of-life care, particularly how the guide with its simple, yet impactful messages and format was seen to provide relatives with a language and reassurances to talk about death and dying. Our findings thus support existing research on the importance of effective information and communication for relatives at the end of life.2,3,5,6,8,9,11,20-23 This includes research that evidences the benefits of using information pamphlets in end-of-life care for relatives’ experiencing bereavement.24-26 Other benefits highlighted by the study include the guide's effort to de-medicalise death and dying, thus contributing to a growing trend emphasising the social nature of death and dying.27,28 Although, our findings show that more could be done to de-medicalise the image used in the guide, making it appear less clinical.
The guide was also described as a potentially important training tool that can support healthcare practitioners in having conversations with relatives, giving them the confidence and language to talk to relatives. 29 As existing research has found that death and dying within the healthcare profession remain challenging and difficult topics with some practitioners feeling inadequately trained for having such conversations,20,30,31 the guide to Deathbed Etiquette could potentially play an important role in addressing this unmet need. This is crucial since existing research has found that a willingness to discuss death and dying at the end of life is one of the most important needs of relatives.2,32
In terms of the guide's effective introduction to relatives, the findings highlight a need for introducing the guide in a timely and compassionate way and following an initial conversation with relatives about their loved one entering their final days or hours of life. It is worth noting that the guide may need adapting and evaluating for different cultural contexts, something which the discussions only briefly touched upon. While the guide has been adapted for different religious groups, 12 more research is needed to explore its cultural appropriateness, including whether it could be introduced effectively through a mobile application.
Challenges were also identified, particularly in relation to the title of guide. Concerns were raised about the public perception of the word ‘deathbed’, which was thought to be blunt as well as unfamiliar to many, and the word ‘etiquette’, which was thought to not fit with the aim of the guide to offer support and guidance to relatives in a way that does not set up certain expectations for how to behave. Existing research on the taboo associated with death and dying could help explain the negative connotations connected to the word ‘deathbed’. This includes a discomfort with dying's physicality as well as difficulties explaining or relating to ‘deathbed visions’,33,34 but also more generally, the thesis that we live in a death-denying society, spurred on by the medicalisation of death and the individualism of the twentieth century, 35 and which has since been embraced as public knowledge and become normalised.36,37 That the word ‘etiquette’ is found to be problematic could be explained by practitioners’ familiarity with clinical etiquette as taught in medical school and practiced in healthcare as a way to maintain politeness and integrity.38,39
Strengths and Limitations
The strength of the study is its inclusion of a variety of healthcare practitioners with experience in end-of-life care, including nurses and doctors, chaplains, allied health professionals, and managers which allowed for rich data on their views on the guide and its introduction into practice. Practitioners with less extensive experience in non-hospice settings, however, may respond differently to this resource. The study findings are also limited by focusing on professional views. Understanding the perspective of relatives and other loved ones, including differences in settings (ICU patients vs hospice and ward patients) will be paramount for further development and implementation of the guide.
Conclusion
Exploring the views of practitioners with experience in end-of-life care, the study found that the guide to Deathbed Etiquette could potentially be an effective tool in supporting relatives as well as practitioners in end-of-life care. Key findings demonstrate the importance of normalising experiences of being by the bedside of a dying loved one, including the need to talk about death and dying. Having honest and compassionate conversations with relatives about death and dying is crucial, and the guide was found to potentially contribute to this aim with its simple messages and reassuring language. Further research is needed on relatives’ views on the guide, ensuring that broad perspectives are captured. There is also a need for more research on how to implement the guide in healthcare settings, which will include exploring the suitability of different terminology and language around death and dying, and how communication resources can be designed and implemented in settings where practitioners and patients are likely to have different preferences regarding language.
Supplemental Material
sj-docx-1-pal-10.1177_08258597231158325 - Supplemental material for Deathbed Etiquette – The Guide: A Qualitative Study Exploring the Views of Practitioners on its Introduction into End-of-Life Care Settings
Supplemental material, sj-docx-1-pal-10.1177_08258597231158325 for Deathbed Etiquette – The Guide: A Qualitative Study Exploring the Views of Practitioners on its Introduction into End-of-Life Care Settings by Mette Kragh-Furbo, Maddy French, Lesley Dunleavy, Sophie Hancock, Karen Sanders, Margaret Doherty and Amy Gadoud in Journal of Palliative Care
Footnotes
Acknowledgements
We would like to thank the contributors to the guide, who developed and shaped the content and format of the guide. They are Dr Kathryn Mannix, Professor Julia Riley, Dr Jo Elverson, Dr Lynn Bassett, Ms Margaret Doherty and Dr Amy Gadoud.
Disclaimer
The views expressed in the article are the authors’ own views and not an official position of the institution or funder.
Ethical Approval
The study was approved by the Research Ethics Committee in the Faculty of Health and Medicine at Lancaster University (reference number: FHMREC 20078 1 Feb 2021).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Strategic Priorities Fund at St Mary's University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.