
Abstract
Following someone’s death, bereaved people may struggle with their grief. When a patient receives palliative care, bereavement support for the patient’s family is an expected function of specialist palliative care services. To date, detailed descriptions of the purpose, function and provision of support from bereavement services are limited. This study examined how specialist palliative bereavement services self-defined their functions and described any support and interventions they offer. The aim was to synthesise how services satisfied their responsibilities for continuity of support to the family following a patient dying. A scoping review was undertaken to examine the literature on bereavement support within palliative care services to codify how they initiated post-death contact, the purpose of contact and what interventions were offered. Seven databases were interrogated in 2020 using search terms developed by CareSearch (www.caresearch.com.au) with refinement. Items needed to be in English and detail the aims and functions of service-initiated contacts and support. Information was thematically analysed using an inductive approach. Bereavement contact from palliative care services had an overall aim of offering guidance through the provision of information, access to a risk assessment and counselling. The analysis demonstrated the provision of bereavement information, describing support pathways and delivery of accessible grief interventions provided a ‘safety net’. Other themes revealed services often monitored adjustment through scheduled reviews, were aware of their limitations and completed referrals to other services as needed. This study adds to our understanding of palliative care bereavement services and provides valuable information about their intended functions. To improve understanding of bereavement functions, services need to clearly define their primary purpose and how this meets the needs of bereaved people and national standards. Ideally, future research would interview bereavement staff directly to ensure accurate descriptions of service aims and model.
Plain language summary
Bereavement care and contact is an expected component of specialist palliative services and is written into standards and guidelines. The purpose of service-led contact is not clear and there is some suggestion that it is unnecessary. While not every person bereaved from an anticipated death will require formal grief intervention, around 10% of bereaved people a higher level of morbidity, mortality and/or prolonged grief. Few studies have identified the aim of service-led bereavement contact. Our review of the literature identifies they have a common purpose. Thematic analysis showed that service-led contact aims to act as a safety net bereaved individuals following an anticipated death. This study demonstrates the importance of bereavement support from specialist palliative service. Contact provides an important support of people who need more information about grief and/or formal interventions. However, greater consistency in describing the purpose of service-led bereavement support is needed. Further research is required to examine current models of service-led contact from palliative bereavement teams to identify how they align with standards and expectations of care.
Introduction
The World Health Organization describes palliative care as an approach that improves patients quality of life, respects choices, and supports patients families during the illness and into bereavement. 1 In keeping with the World Health Organization’s definition, Palliative Care Australia has developed standards that include the expectation to support the patient and their family. 2
Evidence reflects that service-initiated contact with bereaved caregivers is a standard practice in many services, written into guidelines, and generally provided through a paid position within palliative care services.3 –7 Services typically provide contact using telephone, in-person or mailed information.7 –10 Service-led contact is characterised as sharing information, offering a review of coping and provision of additional grief interventions where available.3,4,6 –8 The case for contacting newly bereaved caregivers seeks to be justified given the concerns regarding the risk of increased morbidity including depression, anxiety, prolonged grief and increased rates of mortality.11 –19 Negative changes in health or an exacerbation of existing health concerns may be experienced for several months following the death of someone significant. Health-related bereavement impacts may include major depression, anxiety, post-traumatic stress disorder, substance abuse, suicide risk, heart conditions and gastrointestinal disorders as well as poor sleep. Similarly, research recognises there may be negative financial and practical impacts through bereavement, including access to superannuation or funeral payments and loss of an income.19,20 Information to carers and families should facilitate knowledge of typical grief reactions and where to access support if required. 21 The intention of service-led contact is to provide information (grief literacy) and, for a smaller proportion, grief counselling. Such support potentially aids in identifying and supporting those at risk of struggling to adjust. However, there is little or no evidence available that such contacts and interventions lead to better outcomes for people.
It has been argued that universal service-led contact leads to unnecessary interventions.22 –27 Examples of references to unnecessary interventions ‘ineffective outreach’ where bereaved individuals are ‘offered help without them asking for it’ 28 or that ‘most palliative care services tend to provide blanket interventions . . . regardless of (people’s) support needs’. 25 In contrast, other research notes the difference between bereavement services providing ‘access’ to support and the bereaved person’s engagement in grief counselling interventions. 6 Claims about unnecessary interventions may lead to a reduction of bereavement support availability, as specialist palliative services look to rationalise staff time to meet broader service demands. Other studies report that not all bereaved people who are aware of and eligible to receive support use it. Therefore, concerns regarding unnecessary offers of assistance may not be warranted.10,29,30 It has also been noted that bereaved people may not seek out bereavement support directly. 31 If service-initiated bereavement contact does not occur, it is unclear how those who are grieving will locate information about available services or receive guidance on when to seek support – especially as bereaved people can become disconnected from health and care services. 32 People experiencing bereavement have expressed such concerns themselves through not knowing how to access desired support or describe discomfort in asking for help.10,33,34 Bereaved caregivers may also report a sense of feeling abandoned following the patient’s death, especially when care had been intensive or provided over long periods of time.35,36 When seeking information about how bereavement services are structured and function, detailed descriptions of services are difficult to locate. Where information is available (typically through surveys of palliative care services), even then, it often lacks details about service models and functions. 37 Understanding both the intention and practice of palliative bereavement services models are necessary given an increasing rate of deaths and service funding pressures, which could make it difficult to fulfil specified standards of bereavement care.
Research objectives
While surveys identify the general characteristics of adult palliative bereavement services, clarity about their aims and purposes was lacking. To bring the literature together, we conducted a scoping review to examine adult palliative care services’ self-described approaches to service-initiated bereavement contacts and intervention practices following a patient’s death. There was a specific focus on how the services described the aim of their contact and any subsequent interventions.
Materials and methods
A scoping review was selected to undertake a comprehensive examination of how adult palliative bereavement services described their models. The approach was chosen following recommendations.38 –40 A scoping review is ideally suited when exploring a topic when the available evidence is unclear. 39 Scoping reviews are a systematic search for information through a transparent and reproducible method. 39 Ensuring that a clear protocol is followed that reduces error and extracts and presents data in a structured manner will increase reliability. For a standardised and reliable scoping study process, a five-stage methodology is suggested where research questions are identified; relevant studies are identified and selected; data are charted; and results are gathered, analysed and reported. 40 The PRISMA Extension for Scoping Reviews (PRISMA-ScR) template was used as a guide in planning, conducting and reporting the study, though the review was not registered (Supplemental Material 1). 41 Our emphasis was placed on developing a clearly written, comprehensive research protocol. Critical features of our protocol included defining the study rationale, eligibility criteria, information sources, data charting processes and summarising evidence. Scoping studies have the capacity to increase the sensitive review of information through an iterative process as the study completes the analysis of the literature.39 –41 To facilitate a thorough examination of the information, an extraction template was developed to consistently record details regarding the described function and method of service-led bereavement contact and approach to grief interventions. The scoping review was directly influenced by the primary researcher’s clinical experience in adult palliative care services. This led to limiting the review to specific information that was identified as difficult to obtain and the potential impacts of this gap. It is recommended that researchers recognise and discuss how the research and data examined influence one another, both prospectively regarding decisions made at the outset of the study and retrospectively when writing the results. This process is referred to as reflexivity. 42 Responding to claims about unnecessary interventions being undertaken, we reviewed the literature that described bereavement services in specialist palliative or hospice services for adults with life-limiting illnesses. In deciding to focus on adult-only services, the primary researcher considered her clinical experience in adult specialist palliative care. An earlier unpublished literature review by the primary researcher highlighted the need to locate evidence regarding the aims and functions of bereavement services in adult palliative care settings. 43 Therefore, we excluded information about paediatric services. We also limited the review to information on the specific actions undertaken by bereavement services, rather than any condolence actions completed by the wider palliative care or hospice team for the same reason. To enhance the rigour of this study, two independent co-reviewers (a Clinical Psychologist and a PhD qualified Social Worker) supported the primary researcher in the initial screening of abstracts and titles, full review of the included articles, and thematic analysis. Literature was included if it provided sufficient details regarding palliative bereavement service-initiated contact with an identified person from the patient’s medical record after they died.
Search strategy and eligibility criteria methodology
Search terms for the review were initially identified by examining searches used within the Australian palliative care knowledge database, CareSearch (Caresearch.com.au), to identify relevant literature and evidence. CareSearch is a specialised online database of palliative care and its associated disciplines. 44 Further refinement was undertaken to identify descriptions of service-initiated bereavement contact from palliative or hospice services themselves (Supplemental Material 2). A specialist university research librarian was consulted and worked alongside the primary researcher to ensure the best results. We jointly worked through our existing knowledge, use of database thesauruses and joint brainstorming of useful search terms. Search terms were refined through trial searches until the expected literature was retrieved. A systematic search was conducted on 29 February 2020 (rerun with original date parameters on 31st December 2024) using seven databases. CINAHL, Cochrane, PsychINFO, Web of Science, Scopus, ProQuest and MEDLINE databases were used. Additional visual scanning of the reference lists from the relevant studies was also performed. The results were screened based on inclusion and exclusion criteria which are provided below in Table 1.
Inclusion and exclusion criteria.
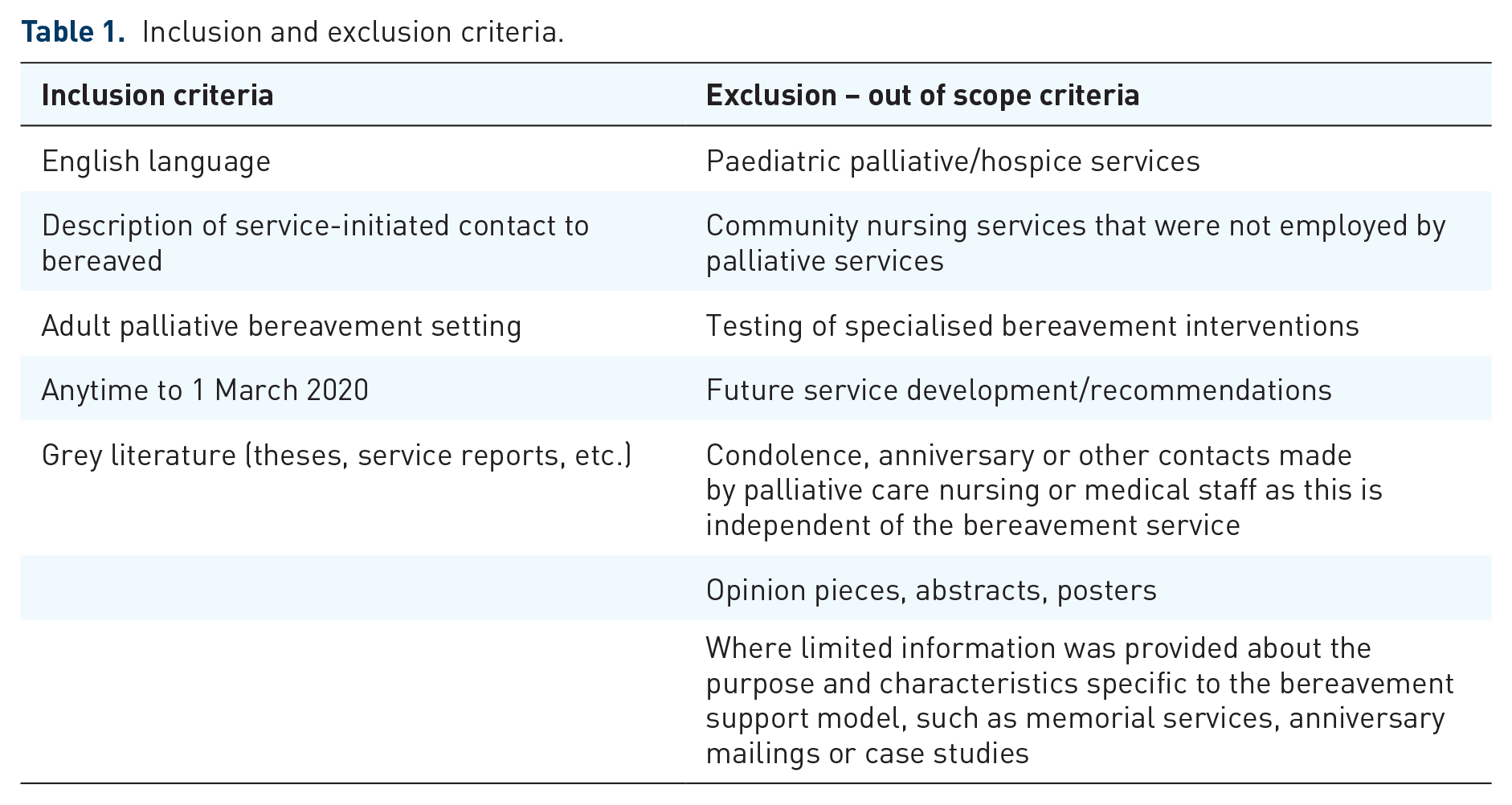
The database search identified 10,276 articles and grey literature, which were then imported into Covidence. Covidence is a web-based collaboration software platform that streamlines the production of systematic and other literature reviews (Covidence systematic review software; Veritas Health Innovation, Melbourne, VIC, Australia). A PRISMA flow diagram of the screening process is shown in Figure 1. Duplicates were removed, leaving 5990 records. The primary researcher screened titles and scanned abstracts, checking the articles against the exclusion/inclusion criteria. Co-reviewers randomly checked 210 (3.5%) articles at this stage, reviewing both the excluded ones and those to be screened in more detail. A 97% agreement rate was achieved for title and abstract screening, with conflicts being resolved through consensus. Next, the primary researcher thoroughly reviewed the abstracts of 482 full-text articles for descriptions of service-initiated bereavement contact. Survey reports regarding palliative bereavement services were excluded. This decision was based on reporting typical features of service models where the research did not clarify the aim or function of interviewing bereavement staff. Texts focussed solely on describing the process of bereavement contact through sending anniversary cards or condolence notes or that failed to clearly describe service-initiated contact of bereaved family were also excluded.

PRISMA flow diagram of search results.
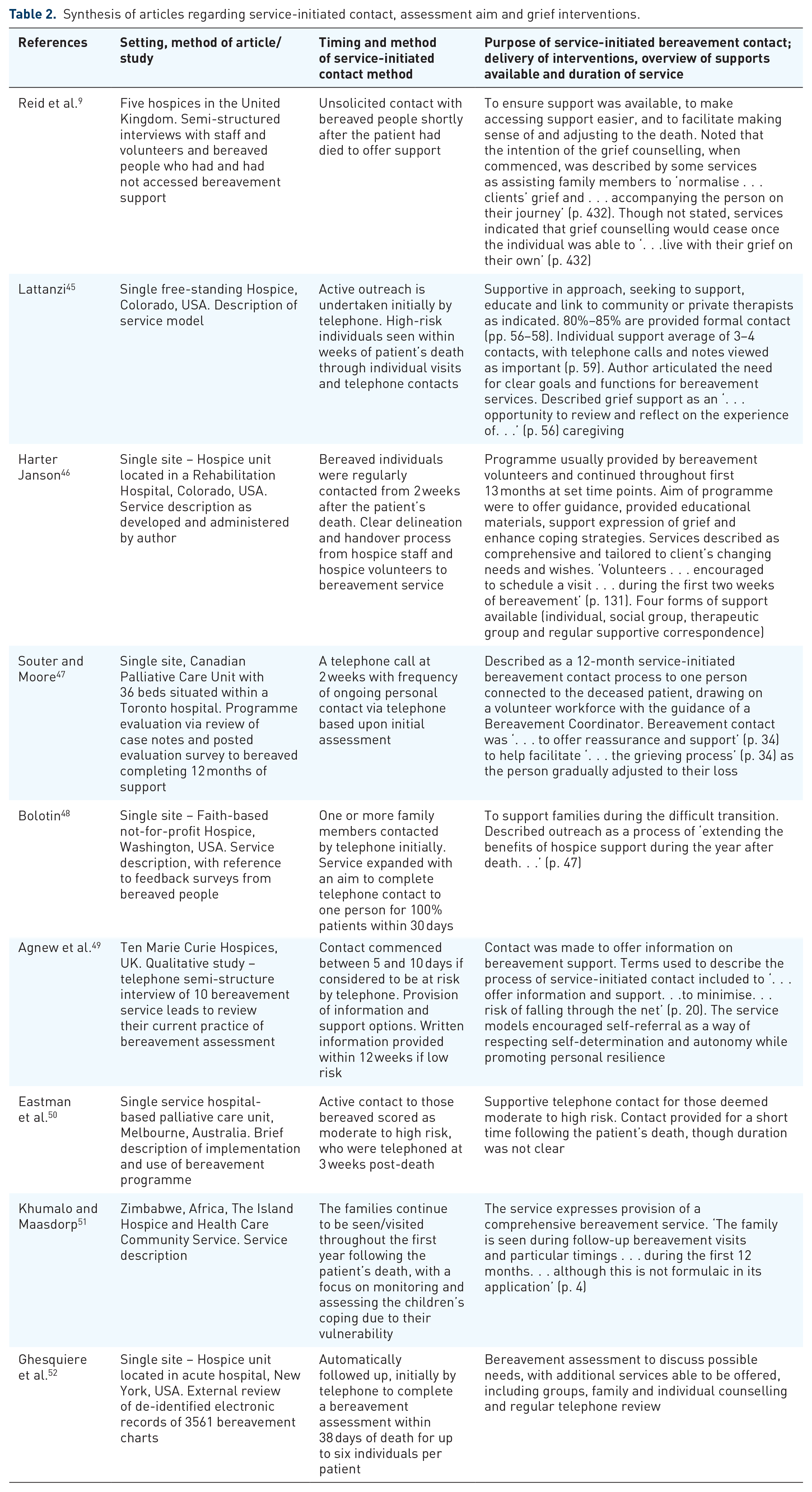
Initially, 26 articles had preliminary data extracted by the primary researcher. The results were then shared between the two reviewers for independent reading before the team discussion. The team review resulted in a significant refinement of the extraction focus, with 18 articles subsequently excluded. Articles were removed if they did not adequately describe the bereavement service contact or method. Consensus was sought again before the final decision regarding inclusion was made. Nine papers met the criteria for inclusion in the review, with the evidence summarised in Table 2. The data-extraction template is provided (Supplemental Material 3).
Synthesis of articles regarding service-initiated contact, assessment aim and grief interventions.
Data charting and synthesis
A selective data-extraction process to meet our objectives was undertaken following Noyes and Lewin, 53 who advised three central foundations are needed for the examination and extraction of qualitative evidence. First, the purpose of the review forms the basis for data gathering. Second, an extraction template is designed to match the purpose of the study. The final central foundation recommends that the research process is an iterative one. This involves a process of reading, data extraction and synthesis of information that is cyclic, allowing key themes to emerge. The primary researcher developed an extraction template to allow for the documentation of keywords and information. Content for the template followed Johanna Briggs Institute38,41 recommendations of participant, concept and context, known as PCC. Study quality and bias analyses were not completed because the purpose of the study was to obtain reasonable descriptions of bereavement service contact and aim rather than to examine the quality of the article or interventions. The extraction template recorded the following information:
(a) Article identifiers (author, year, funding sources);
(b) Setting of bereavement support (participants and context);
(c) Method and purpose of service-initiated bereavement contacts; and
(d) Approach to assessment and grief interventions.
Additional information was extracted, although this has not been reported here.
Process of thematic analysis and synthesis of evidence
The extracted information was thematically analysed using an inductive approach, to identify the purpose and nature of service-initiated contact in palliative bereavement services. A manual process was used to extract data because of the small number of articles. The primary researcher read and re-read the data to familiarise themselves with the data and develop an initial coding framework. Co-researchers then independently reviewed the initial codes. Adjustments to coding and themes continued through the regular revisiting of the data, with consensus established by review and discussion.
Results
Primary theme: Acting as a safety net
We identified the primary purpose of service-initiated contact was to ‘act as a safety net’ with important elements shown in Figure 2 that were undertaken by bereavement services. Authors used a range of terms to describe the process of service-initiated bereavement contact and the provision of grief interventions. Service-initiated contact and intervention were perceived to provide a level of protection for the bereaved and aimed to increase grief literacy, self-awareness and coping. The findings are indicative of a continuum of care following the patient’s death to support people as they adjusted to their loss.

Palliative bereavement services acting as a safety net through service-led contact and supportive interventions.
Two articles,9,47 referenced feedback from service users which provided some evidence of benefit. This was achieved through written information and various forms of grief-focussed interventions. Another article 48 noted risk assessments targeting those with complex mental health needs. As reflected in Figure 2 and supported by the quotes in Table 2, most articles defined facilitating adjustment through a time-limited, supportive, active listening and educational approach to help make sense of the experience of grief. The safety net incorporated easy access to supportive grief counselling and/or group gatherings when desired by the bereaved individual, without incurring additional costs or the need for external referrals. Two sub-themes also emerged, comprising scheduled reviews and recognising service limits by referring to additional or specialist services. Indicative extracts from the articles are provided in Table 3.
Sub-themes of safety through scheduled reviews and recognition of service limits.
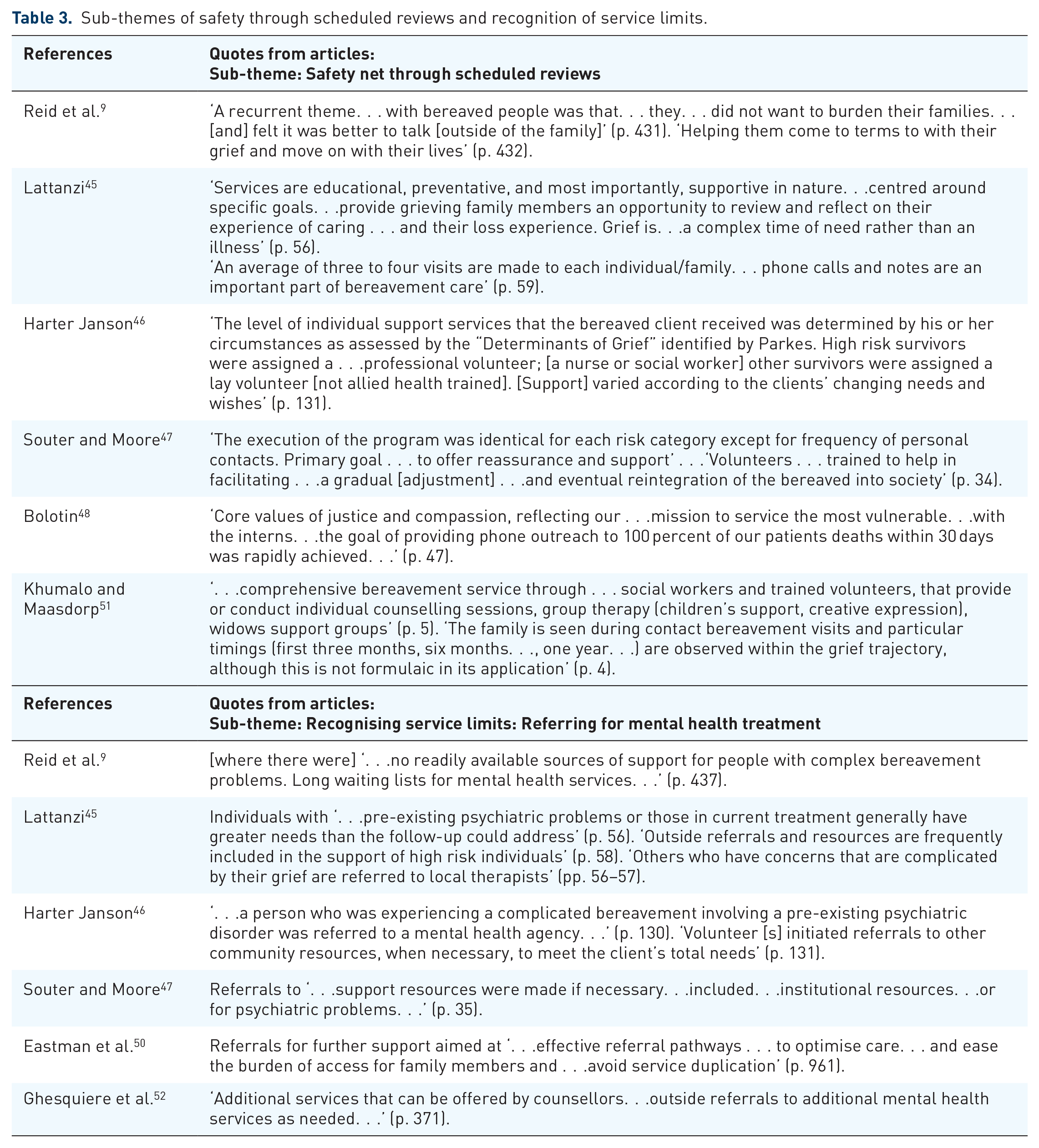
Sub-theme: Safety net through scheduled reviews
Several services described the provision of regular reviews as standard in their delivery of bereavement care. This form of safety net aimed to monitor adjustment through in-person reviews at set time points. Additional support options were also available, including group meetings, workshops, educational sessions and telephone contact. Services emphasised or indicated their continued relationship with the family throughout the first year of bereavement, typically as a process for regular review and monitoring of adjustment.9,44 –48,51 Key descriptions of monitoring through scheduled reviews recognised grief as an adaptive process, involving complexity and challenge, and the need for services to be available. It was important that bereaved individuals were well informed that they could opt out if not wanting continued contact. Provision of scheduled reviews functioned as a safety net consisting of typically three to four face-to-face visits with supplementary telephone calls and various forms of group options made available. One article described a minimum of nine scheduled contacts in their programme. 46
Sub-theme: Recognising service limits and referring for mental health services
The second sub-theme was the ability of services to know their limitations and ‘recognise the need for mental health’ interventions. Articles conveyed a process of referring to external services or additional support (where available). This was demonstrated through observations such as ‘outside referrals for mental health services’46,47,52 and ‘acknowledging existing therapy relationships’.45,46 One article notes ‘long waiting lists for mental health services’ though no further details are provided. 9 When described, a distinction was typically made between referring for mental health or psychiatric services and the role of grief counselling. Differing locations for palliative services (such as the United Kingdom, Zimbabwe and the United States) influenced several factors. Access to mental health treatment options, long waiting times and availability of support, and a need to be covered by insurance, were considerations noted. As reflected in Figure 2 and supported by the quotes in Tables 2 and 3, articles described their role as time-limited, supportive contact to assess risk, monitor and facilitate adjustment and the provision of grief counselling. No service identified their primary purpose as therapy for prolonged grief. There was a recognition that bereavement services needed to be mindful of not creating dependence, as the purpose was to support people through a time of crisis as they transitioned and learnt to live with their loss.9,45 –48
All articles highlighted the importance of a responsive approach to tailor support for individual needs and desires or the need for self-referral as a way of respecting individual resilience and autonomy. Six articles provided risk assessment information45 –47,49–50,52 with the primary components of assessment outlined in Table 4. Where in-person contact occurred with the bereaved individual, a review of how they were responding to their grief would be attempted/completed as the primary risk assessment. A heightened risk of problems in adjusting to bereavement was indicated by experiencing concerning physical, psychological, emotional and spiritual symptoms, including anxiety or depression, suicidal ideation, overt anger, unintended weight changes, sleep disturbances, absence of family or social support, overwhelming stress and/or sense of hopelessness.
Summary of indicators of concern when undertaking risk assessments.

Informing the bereaved caregiver of options, providing a pathway to link into those options and making grief interventions accessible were seen as important. Authors wrote of helping family members to transition through an emotional and complex experience. Generally, the authors described the bereavement intervention model as a supportive process. They detailed grief interventions as available to bereaved people for a limited time to aid adjustment. Options consisted of telephone calls, group sessions, informative mailings, memorial gatherings and face-to-face grief counselling. No articles described that bereavement contact was providing therapy or treatment for prolonged grief. This was not unexpected, as it fits with the usual 12–13 month timeframe that palliative bereavement services typically limit support to.6,7,10 Bereavement support was available for differing lengths of time, ranging from a few weeks to 13 months. By contrast, prolonged grief is thought to be more reliably diagnosable from 12 to 18 months, as described in the Diagnostic and Statistical Manual, version 5 (DSM-5).54,55
Service-led bereavement contact aimed to connect with, complete a review and assessment of needs (when in-person) and inform people about available services and supports. Active listening and support to understand and manage the understanding of the challenges faced were key features of service aims. All services described the role of being there to support and guide and to provide grief counselling or other forms of support if needed. Acting as a safety net was achieved through actions including assessment, time-limited intervention and/or completing external referrals. One service limited their support to a few weeks following a patient’s death 51 while others offered a continued relationship if required, through regular reviews during the first 12–13 months.45 –49 Completion of risk assessment was a key component of several service models, with most defining the literature that informed the assessment.45 –49,51,52 Provision of psycho-education about grief to assist in understanding grief experiences was claimed to promote personal resilience. There was a focus on building individual, family and community capacity in responding to the experience of grief. However, no articles provided a robust evidence base for their model of care which is an area worthy of much greater attention in future research.
Discussion
Characteristics of palliative bereavement services have previously been described in several research articles.3 –10,37,56 –59 There is a surprising lack of research and detailed information relating to the bereavement practices of palliative care, given the needs in the community and increasing interest in policy and standards. This study has allowed us to identify common themes in the literature included. Findings also provide insight into some long-standing and current models of palliative bereavement services.
What this study adds
Though only nine articles met the scoping review criteria, original pertinent data were extracted. The results showed the primary purpose and aim was for bereavement services to act as a safety net (see Figure 2). Sub-themes reiterate how bereavement services function as a safety net while knowing their limitations and the need to facilitate reconnection with personal networks. Support was directed at guiding and evaluating how the bereaved were adapting to the person’s death and to facilitating adjustment when indicated through grief-focussed interventions. Reviewed articles articulated the recognition of bereaved caregivers requiring time to adjust, the need to provide information, the benefit of connection with others and the encouraging use of the bereaved person’s natural network. In addition, most articles noted their time-limited, open-access approach to service provision and the necessity of time passing to allow grief to become integrated.
As such, the bereavement services can be seen to meet a need that may facilitate transition, and support a structured completion of the relationships with the palliative service. They offer a safety net to capture the more complex needs of those who are bereaved by an expected death within a palliative care service. This approach does not compete with the more purposeful interventions to address complicated grief, nor does it compete with the natural community networks that may wrap around the bereaved in ideal circumstances. Indeed, such contact can be seen to complement these strategies by normalising common grief experiences and the availability of community support resources, as well as prompting awareness of more formal pathways to respond to prolonged grief. The scoping review findings resonate with results from an unpublished companion study, a cross-sectional study of a specialist palliative bereavement service. 43 In this 2017 cross-sectional study participants valued knowing the bereavement service was available and that this knowledge was helpful and reassuring, whether they made use of it or not.
The findings from our scoping review reflect how palliative bereavement services work alongside or in conjunction with suggested public health and tiered models22,23,60 and the National Institute for Clinical Excellence, 61 approach to bereavement support. Our data indicates palliative bereavement services are an example of the suggested 3-tier or 4-tier models of bereavement support and are not replacing existing community networks.22,23,60,61 Services aimed to provide psycho-education about typical grief responses, to help normalise and self-assess grief reactions was a primary function (tiers 1–2) and provide grief-specific interventions (tiers 2–3) when required. Some articles acknowledged more complex mental health concerns could be present and, when noted, the focus was on supporting the bereaved person to receive appropriate treatment (tiers 3–4) if available. Lack of access to mental health services was recognised as a problem and highlights a limitation of bereavement services. A common philosophy and purpose were to develop personal and community capacity, through increasing grief literacy and supporting bereaved caregivers to build confidence in their own coping. Findings reflect a continuum of care and are particularly important for bereaved caregivers who can lose contact with their personal support networks.
There was evidence that bereavement services recognised some caregivers may form close bonds with palliative staff and can experience challenges in reconnecting to their broader support networks.46,47,49 Each service intended to provide an open model of access, 6 grief support, guidance and information during the first months of bereavement. This was a way of facilitating the transition from caregiving and reconnecting to everyday life while coming to terms with the loss. There was a general sense of knowing service limits and ability to identify mental health concerns, demonstrated by acknowledging referral out to mental health services where able to.9,45 –47,52 That said, it is critical to keep in mind the varying contexts of specialist palliative care and hospice services depending on their location and the influence of political and health systems, as there are implications for the provision of and access to bereavement support and grief counselling. While there were descriptions of support being provided to bereaved individuals until they felt able to manage on their own, discontinued support or required referral to more formalised interventions, we did not find any details on formally assessing outcomes following interventions.
Limitations of the study
The primary aim of this scoping review was to examine how palliative and hospice bereavement services described their purpose and service models. Though the examined articles provide more information as to their model than are usually available from external surveys of palliative services3,4,7,56–59 limitations remain in the level of details. Regarding comprehensive detail about bereavement service intervention models, five of the publications answered most of the review questions.45 –47,50,52 One article 9 provided only limited insight into the actual practices of service-initiated bereavement contact and assessment procedures. Future research needs to obtain more precise and accurate information when examining the function and aims of palliative bereavement services; otherwise, there is a risk that imprecise information and reports may influence decisions made at the local service level. Similarly, poor reporting of how services are configured and perceived in the policy and research setting limits the use of the available data. Further, how these findings relate to populations of bereaved people that are underserved by palliative care services and the groups of people who are not able to access palliative bereavement support, is uncertain, though may indicate a need for similar processes. Articles were limited to only English studies, only a small number of articles were retrieved, and then from almost four decades. This may limit how the findings can be applied.
Strengths of the study
This scoping has delivered unique evidence of bereavement models having a common approach through ‘acting as a safety net’ to the newly bereaved. A formally structured scoping review method has ensured rigour in the identification and extraction of core findings. To facilitate a thorough examination of the information, an extraction template was developed to consistently record details regarding the described function and method of service-initiated bereavement contact. To enhance the rigour of this study, two independent co-reviewers (a Clinical Psychologist, and PhD Social Worker) supported the primary researcher in the initial screening of abstracts and titles, full review of the included articles and thematic analysis. Themes were initially developed internally and then checked against two senior researchers (DC, JT) for their relevance and face validity. Review of the findings against public health and service bereavement approaches as well as a companion study further enable the value of the scoping review findings to be cross-checked.
Implications for service delivery
For palliative bereavement services to focus their support model on acting as a safety net, which may also involve scheduled reviews for a time to monitor and facilitate positive adjustment makes intuitive sense as some bereaved caregivers are reported to be at heightened risk of prolonged grief17,62 –65 often experience a decline in general health and experience other significant stressors.11 –20 Service-initiated contact is important, and a minimum ‘recommended’ component of palliative care services in the immediate time following a patient’s death. 21 Using standardised and validated methods of review would improve the evidence base for bereavement services.17,27,65,66 The provision of information on common grief reactions and promotion of self-determination in accessing grief counselling can be viewed as increasing grief literacy. Following individual preferences, tailoring support through regular reviews of adjustment and promotion of self-referral was evident. Analysis of service descriptions reflected the use of support when desired or indicated though did not suggest that blanket interventions were occurring. Nonetheless, the literature also notes there are some bereaved who find it difficult to accept support, or who do not recognise the need for intervention as they see their struggle as normal. 31 Consequently, scheduled in-person reviews may be the best form of safety net to support assessment of individual needs and adjustment.
In addition, recognising that service-led contact, referrals and/or grief-focussed interventions provide a safety net can inspire other services to establish their own service-initiated contact processes if none already exist. While it is well known that not all bereaved individuals require grief counselling, there is a recognised need to provide information and support in the early period following a death. Specialist palliative services have a higher standard to meet regarding supporting grieving individuals due to the bonds that are formed with staff during end-of-life care in anticipated deaths. At minimum, specialist palliative services should be guiding bereaved family members to understand grief, how it may impact their functioning, and how support can be accessed.
Implications for future research
Our scoping review provides a starting point in articulating the purpose of palliative bereavement service models, though much more is required. Firstly, there is a need for present-day palliative bereavement services to clearly articulate the purpose of their service-initiated contact and how they assess need for grief counselling. This requires bereavement services to be clear about their purpose and intent. Such clarity could be shared through publications and when surveys are conducted. Without such clarity in describing the aim and intent of service-initiated contact, assessment and grief counselling interventions, concerns like the one expressed by some literature22 –28 will continue due to lack of detailed information. Aligning with this scoping review, an insightful description can be found in Kobel et al. 6 survey of Australian palliative bereavement services which appears to be in-step with the published service descriptions included in this scoping review. They acknowledged that ‘access for all’ (which reflects our concept of a safety net) differs from ‘provision to all’. Secondly, more research is needed to examine how current palliative bereavement services define their work, to help validate the investment made, all be it a typically small investment. Bereavement services may in fact view their primary purpose as providing information and pathways to support, thus acting as a safety net, though they have yet to adopt this term. Services may also define an equally important purpose of completing an assessment of needs with the bereaved person and providing time-limited grief counselling when indicated, available and requested. Palliative bereavement services may find a natural ally in the compassionate community movement, where they could form a partnership in helping families transition from formal health services back into community networks. Adopting this process would be like a recently proposed model, 67 with a similar approach described in one review article. 48
In the future, policy approaches and funding bodies may need to measure models of bereavement care from specialist palliative services. Examining bereavement service models and activity against healthcare accreditation standards, for example, will further add to emerging evidence. Obtaining such evidence about current service models and how this is experienced by the bereaved individual should be considered a priority, due to the known risk of declines in health and potential for loss of life. Inclusive research about service models, meaning research undertaken with providers of bereavement support, will improve the understanding of what palliative bereavement services offer. Research in conjunction with bereavement service providers and those it is aimed at plays a key role in obtaining much-needed clarity of models of care, their effectiveness and impact. Co-constructed research will identify what bereaved individuals seek and how services meet or fail to meet that demand. Consideration also needs to be given to how current models of bereavement care best meet varying cultural needs, across different age groups and in various settings. Research on access to bereavement support is generally from high-income countries, where personal choice and responsibility is emphasised and highly valued, and personal income and public health access may influence models of care. We acknowledge that as our research was conducted before the COVID-19 pandemic literature emerged, some palliative care services may have revised their model of bereavement support. Recent literature indicates an increased focus on bereavement support.68,69
Conclusion
Our findings show palliative bereavement services aim to provide support according to identified and expressed needs. The findings of this scoping review indicate bereavement service models have an overall common purpose when considered as an accessible and recognisable safety net. Such service models can guide newly bereaved individuals to understand their responses and support decision-making about the need for formal interventions for complex needs. Further, this study offers a start to shared terminology regarding service-initiated bereavement contact and grief counselling processes. If the literature is to move on from its concerns about specialist palliative bereavement service models, then bereavement services have some work to do. Further, in the face of increasing pressure on resources, palliative bereavement services need to articulate their approach clearly to be better understood and specific in how their practices meet national standards to better understand their purpose and impact.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251326947 – Supplemental material for What functions do palliative care bereavement services deliver? A scoping review
Supplemental material, sj-docx-1-pcr-10.1177_26323524251326947 for What functions do palliative care bereavement services deliver? A scoping review by Kathleen E. Jurgens, David C. Currow and Jennifer Tieman in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251326947 – Supplemental material for What functions do palliative care bereavement services deliver? A scoping review
Supplemental material, sj-docx-2-pcr-10.1177_26323524251326947 for What functions do palliative care bereavement services deliver? A scoping review by Kathleen E. Jurgens, David C. Currow and Jennifer Tieman in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524251326947 – Supplemental material for What functions do palliative care bereavement services deliver? A scoping review
Supplemental material, sj-docx-3-pcr-10.1177_26323524251326947 for What functions do palliative care bereavement services deliver? A scoping review by Kathleen E. Jurgens, David C. Currow and Jennifer Tieman in Palliative Care and Social Practice
Footnotes
Acknowledgements
The lead author (KJ) acknowledges the support received by co-researcher’s clinical psychologist, Mr. Michael Baraniec and Dr. Mary Hood for their contributions to this study in her PhD research. KJ also acknowledges support from Specialist Librarian, Ms. Shannon Brown (Flinders University, South Australia) in designing and testing the search strategy.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.