
Abstract
Objective(s)
Patients with advanced head and neck cancer (AHNC) are susceptible to malnutrition due to disease progression and side effects of cancer treatments. Current evidence on the effectiveness of nutritional interventions is limited. This scoping review aims to identify the nutritional needs and experiences of patients with AHNC and provide an overview of nutritional interventions implemented to prevent malnutrition.
Methods
CINAHL via EBSCO, PubMed, EMBASE via OVID, Web of Science, Scopus and Google Scholar were searched from inception to August 2024, and articles were screened based on predefined inclusion criteria. The Joanne Briggs Institute Scoping Review Framework guided the review. The Patterns, Advances, Gaps, Evidence for Practice, and Research Recommendations (PAGER) framework was used to synthesise findings.
Results
Of 1703 articles identified, 32 met the inclusion criteria, including 13 retrospective studies, 9 prospective studies, 7 reviews and 3 guidelines. Using the PAGER pattern chart, 4 themes were identified: (1) the use of enteral tube feeding, (2) identification and treatment of malnutrition, (3) the effects of palliative treatment on nutrition and (4) the experiences of patients and carers. Enteral feeding was the most common intervention to manage malnutrition; however, other interventions such as dietary counselling, oral nutritional supplements and parenteral nutrition were also employed. These interventions should be tailored to specific needs of the patients.
Conclusions
Weight loss and impaired oral intake were associated with psychosocial distress affecting patients and carers. Future research is needed to explore the experiences of patients, carers and healthcare professionals regarding nutrition and evaluate the effectiveness of alternative nutritional strategies.
Introduction
Head and neck squamous cell carcinoma (HNSCC) and its related variations arise from several anatomical subsites within the oral cavity, oropharynx, hypopharynx and larynx. 1 Patients with head and neck cancer (HNC) often present late with stage III or IV or advanced disease and have a poorer prognosis.2,3 Overall, 5-year survival rates are poor (34-77%), with 59% of patients succumbing to disease progression 4 and 50% to 60% of patients with stage III or IV cancer developing recurrence or distant metastases. 3 Despite advances in medical and surgical oncology, patients diagnosed with advanced HNC (AHNC) or recurrent HNC often transition to palliative care due to poor prognoses and limited curative options. 5 Surgery or radiotherapy is often unsuitable for these patients, leaving anti-cancer treatments or palliative supportive care as options. 3 Palliation for patients with HNC is initiated following confirmation of an incurable diagnosis or when curative treatment has been declined. Palliative care for individuals with advanced cancer aims to improve the quality of life (QOL) of both patients and their families following a life-limiting diagnosis. This includes improving the physical, psychological, social and spiritual aspects of patients’ lives. Despite its significance, the palliative care needs and experiences of this patient population remain poorly understood.6,7
Patients with AHNC face a plethora of challenges affecting their QOL. These symptoms can be challenging to manage and include compromised airways, communication difficulties, dysphagia, fatigue, fistulas, bleeding, pain, feeding issues and psychological issues such as depression and anxiety.8,9 Early identification and management of physical symptoms caused by tumour progression can prevent and relieve suffering. 9
Malnutrition is prevalent among patients with HNSCC, with 35% to 60% of patients being malnourished at diagnosis. 10 The effects of previous HNC treatments (eg, surgery, chemoradiotherapy) and the onset of new symptoms caused by recurrence or a new incurable cancer diagnosis (eg, dysphagia, difficulty chewing, tumour obstruction, trismus, pain) contribute to nutritional deficits and malnutrition.11,12 Advanced cancer treatments can help with symptom control (eg, debulking surgery, radiotherapy, chemotherapy, immunotherapy) but also have side effects, potentially affecting nutritional management, such as colitis, mucositis or xerostomia, leading to weight loss and malnutrition.12–14
Feeding issues due to tumour position and progression into surrounding anatomical structures contribute to weight loss and sarcopenia, causing a decline in physical function and negatively affecting advanced cancer treatments. 15 Malnutrition is linked to an increase in treatment interruptions, reduced treatment tolerance, increased complications following surgery, longer hospital admissions and increased mortality.16–18 Additionally, malnutrition is associated with reduced QOL, fatigue, reduced performance status and psychological distress.13,19,20 To prevent malnutrition, nasogastric, gastrostomy or jejunostomy tubes are frequently placed in this group. 21 The tumour itself causes metabolic changes, increasing energy expenditure and fat breakdown, alongside muscle protein degradation caused by the release of tumour necrosis factor and interleukins 1 and 6, leading to anorexia (reduced appetite), muscle wasting and weight loss. 10 This metabolic syndrome, called cachexia, adds further complexity to an already intricate problem. Addressing the nutritional challenges faced by this patient population contributes to a holistic approach to advanced cancer care. 10
While the symptoms of AHNC, either due to previous treatment side effects and/or tumour locality and their contribution to malnutrition are documented, there is a lack of evidence regarding the impact and role of various nutritional interventions. Therefore, a scoping review was chosen to identify and map the breadth of evidence available on the nutritional needs and experiences of patients with AHNC undergoing noncurative cancer treatment or those with incurable disease receiving palliative and supportive care. The review will also provide a descriptive overview of the nutritional interventions implemented, the impact of malnutrition and the effects of any palliative care on nutrition, alongside seeking to understand the experiences of both patients and their carers. By examining the available evidence on nutrition, this scoping review will help to identify gaps in knowledge, identify challenges in nutritional management, guide clinical practice and improve the nutritional care of patients with AHNC.
Methods
Study Design
The Joanne Briggs Institute (JBI) Scoping Review Framework 22 was used to guide the design and conduct of this scoping review. The Preferred Reporting Items of Systematic Reviews and Meta-Analyses extension guidelines for Scoping Reviews (PRISMA-ScR) 23 were followed when reporting our findings. A review protocol was developed, peer reviewed and published in the Open Science Framework (https://osf.io/w6znk).
Search Strategy
The search strategy aimed to locate all relevant published literature. An initial, limited search was undertaken on Medline and CINAHL to identify keywords and phrases that were used as Medical Subject Headings (MeSH) terms and were discussed with a research librarian. The identified MeSH terms were used to search 5 databases, including PubMed, CINAHL, Scopus, Web of Science and Embase. Google Scholar was also searched to target grey literature sources (such as guidelines, institutional repositories and policy websites) and maximise the literature searched in line with JBI guidance. Screening in Google Scholar stopped following 10 consecutive ineligible results. The reference lists of all identified papers included in the review were screened for additional relevant studies. The databases were searched from inception until August 2024. The search terms and keywords that were used are presented in Table 1.
Search Terms and Keywords.
The eligibility criteria included all primary and secondary studies, including qualitative, quantitative, mixed-methods studies, systematic reviews, commentary articles, clinical guidelines, narrative reviews and expert opinions published in English and focused on nutrition or malnutrition in patients with AHNC. As per the JBI guidelines for scoping reviews, grey literature was included to ensure that the scoping review was as comprehensive and inclusive as possible. This included any nutritional interventions started before an advanced cancer diagnosis and continued or nutritional interventions implemented following an advanced cancer diagnosis. Nutritional interventions included were dietary modification, oral nutritional supplements (ONS), enteral feeding or parenteral feeding used alone or together. Nutritional interventions delivered in the acute, community or hospice settings and patients’ experiences of these interventions were also included. Additional outcomes including weight, body mass index (BMI) and any impact of the nutritional interventions on patient-reported outcome measures such as QOL, measured by a validated questionnaire, were included.
Data Extraction, Analysis and Synthesis
All identified papers (from databases, Google Scholar and grey literature) were merged into EndNote 2020 for de-duplication and manual verification. The papers were imported to Covidence for further de-duplication and screening. Grey literature sources were screened, and the quality was assessed using the Authority, Accuracy, Coverage, Objectivity, Date and Significance (AACODS) checklist. 24 Items failing this were excluded at the source of screening. Titles and abstracts were screened by 3 independent reviewers with relevant papers retrieved in full and imported into Covidence, a web-based collaboration software platform that streamlines the production of literature reviews. The full texts of selected papers were assessed by 2 or more independent reviewers. Any disagreements that arose between the reviewers were resolved through discussion or with an additional reviewer. Included papers were not appraised for their quality in line with scoping review guidelines. 22 Data were extracted using an extraction table developed by the authors, which was piloted before use. The extraction table included information about country of origin, aim, design, study population (if applicable), data collection and analysis methods, results and key implications. The extraction table is included in Table 2. Limitations within the current literature were identified and presented.
Data Extraction.

Abbreviations: ANH, artificial nutrition and hydration; BMI, body mass index; BOR, best overall response; DCR, disease control rate; DT, distress thermometer; ECOG, Eastern Cooperative Oncology Group; EORTC, European Organisation for Research and Treatment of Cancer; ESAS-r, revised Edmonton Symptom Assessment System; ETF, enteral tube feeding; FACIT, Functional Assessment of Chronic Illness Therapy; GNRI, Geriatric Nutritional Risk Index; HEN, home enteral feeding; HNC, head and neck cancer; HNSCC, head and neck squamous cell carcinoma; HR, hazard ratio; ICD-10, International Classification of Diseases, 10th revision; ICI, immune checkpoint inhibitor; JIPMER, Jawaharlal Institute of Postgraduate Medical Education and Research; KPS, Karnofsky Performance Status; NCCN, National Comprehensive Cancer Network; NGT, nasogastric tube; OTSSC, oropharyngeal tonsillar squamous cell carcinoma; PC, palliative care; PEG, percutaneous endoscopic gastrostomy; PFG, percutaneous fluoroscopic gastrostomy; PHQ, Patient Health Questionnaire; PNH, parenteral nutrition at home; QOL, quality of life; RCC, Regional Cancer Center; RECIST, Response Evaluation Criteria in Solid Tumors; RIG, radiological inserted gastrostomy; RPMI, Roswell Park Memorial Institute; SEIQoL, Schedule for the Evaluation of Individual Quality of Life; SPC, specialised palliative care; TNM, tumour, node, metastasis.
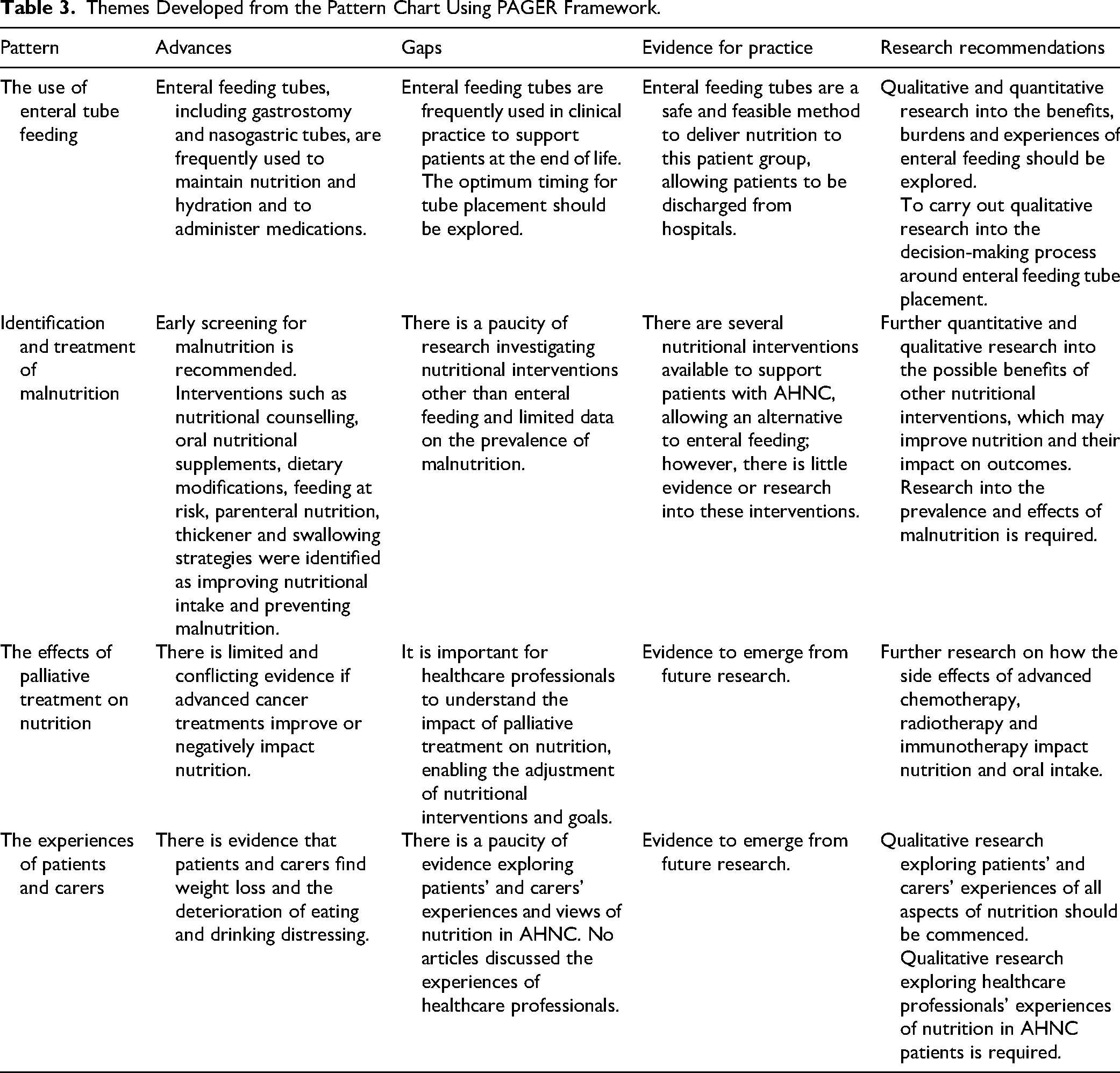
The Patterns, Advances, Gaps, Evidence for practice and Research Recommendations (PAGER) framework 25 was used to analyse the data. The PAGER framework focuses on the identification of patterns and advances in current literature, helping to map and describe the literature, while highlighting areas for future research. A pattern chart was developed in line with the PAGER framework using the descriptors ‘Patterns’, ‘Advances’, ‘Gaps’, ‘Evidence for practice’ and ‘Research recommendations’. From this chart, themes were developed, extracted and analysed (Table 3).
Themes Developed from the Pattern Chart Using PAGER Framework.
Results
Of 1703 articles identified, 32 met the eligibility criteria and were selected for the scoping review (Figure 1). The studies had varying methodologies, including 13 retrospective studies, 9 prospective studies, 7 reviews and 3 guidelines. All the articles discussed nutritional interventions for patients with AHNC. The review articles were narrative or based on expert opinion. The prospective and retrospective studies took place in acute hospitals, hospices and the community. These 32 articles came from across the globe, including some countries in Europe (eg, Netherlands, UK, Italy, Germany), India, Philippines and the United States. The articles were published between 1980 and 2024, and the sample size of the prospective and retrospective studies ranged from 3 to 175 patients (Table 2).
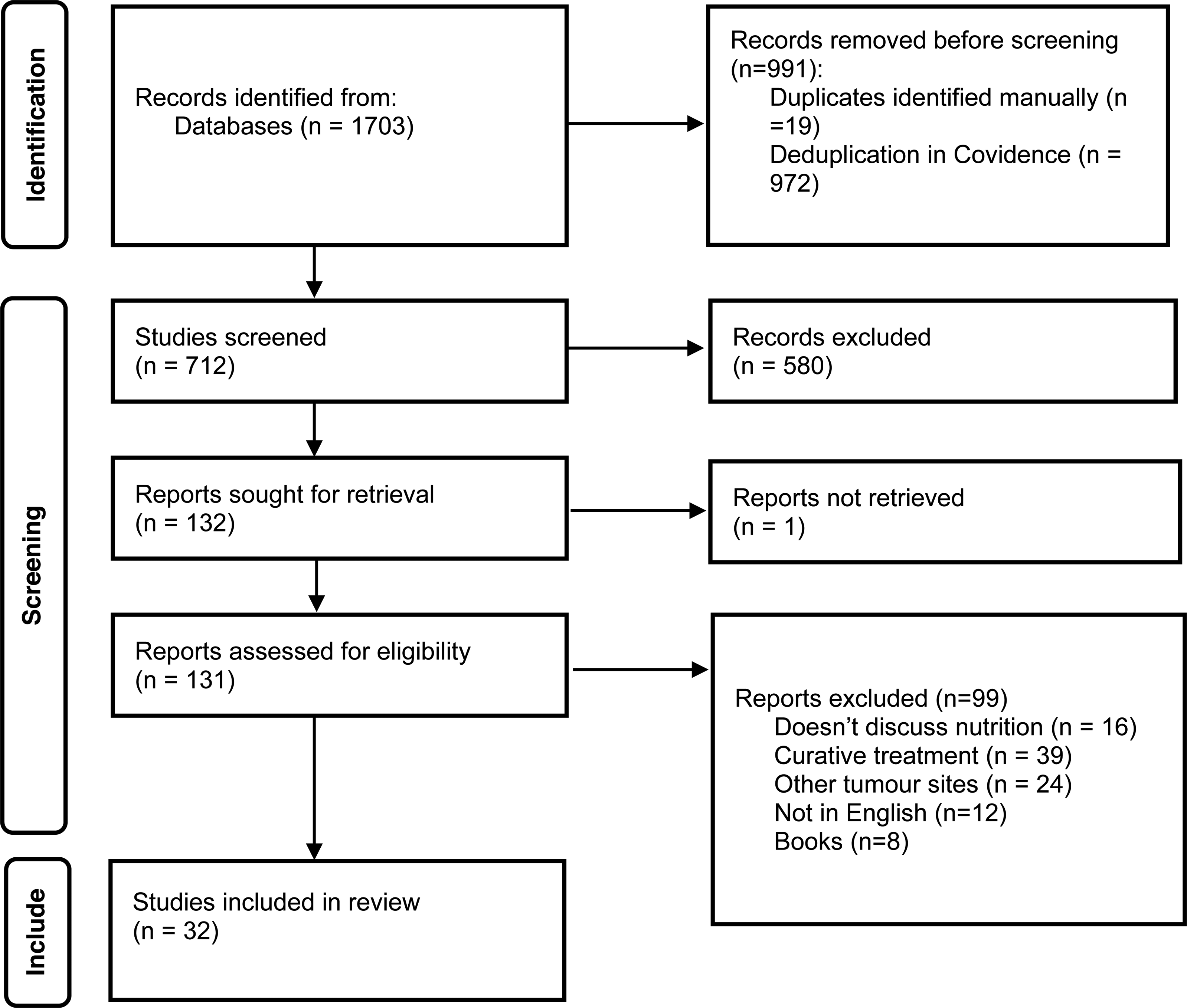
PRISMA Flow Diagram Identifying Studies Used in the Scoping Review.
Four themes were identified: (1) the use of enteral tube feeding, (2) identification and treatment of malnutrition, (3) the effects of palliative treatment on nutrition, (4) the experiences of patients and carers (Table 3).
Theme 1. The Use of Enteral Feeding
Enteral feeding was the most common nutritional intervention implemented for patients with AHNC (n = 26). Various feeding tubes were used, including gastrostomy, jejunostomy and nasogastric tubes (NGTs) 26 or Ryle’s tubes.26,27 The early insertion of enteral feeding tubes (EFTs) was recommended28,29 alongside discussions with patients on the benefits and potential risks of EFT insertion.30–32 Following these discussions, patients could decline EFT insertion, choosing to eat and drink orally as able.27,33 Reasons for EFT insertion included dysphagia, aspiration and impaired oral intake for longer than 30 days. 28 34–36
EFT selection also depended on patients’ prognosis, with gastrostomy tubes preferred for longer-term feeding compared to NGTs.28,36 NGTs were perceived as a safety risk in the community and were identified as being difficult to insert past the tumour, requiring multiple replacements, being prone to blocking and requiring additional ‘out of hours’ care.30,3336–38 There were also issues with gastrostomy tubes. One case study highlighted issues with a leaking gastrostomy, causing excoriation to the abdominal skin and becoming blocked, causing discomfort and distress to the patient. The gastrostomy was removed as a result. 39
Perceived benefits of enteral feeding were identified, including providing a route for nutrition, hydration and medications when patients were unable to swallow, reducing the risk of aspiration, improving QOL and length of life and improving biochemistry and weight.29,33,35,36,40 Sironi et al showed a statistical improvement in biochemistry and an increase in body weight (P = 0.03) following 3 months of home enteral feeding. Three studies reported that EFT enabled patients to be discharged home or to a hospice from the hospital, allowing patients to be better supported in the community.41–43
Five articles discussed ethical dilemmas surrounding enteral feeding, regarding prognosis and appropriateness of EFT insertion and withdrawal of EFT.31,33,42,44,45 Seven studies concluded that enteral feeding should be tapered or not used in the last weeks of life, with EFT not advocated in the final days of life.30,31,33,41,44,46,47
Theme 2. The Effects of Advanced Cancer Treatment on Nutrition
Three articles reported on nutritional interventions employed during advanced cancer treatment, with 2 studies focusing on the effects of different hypofractionated radiotherapy regimes27,48 and 1 on immunotherapy. 49 All 3 articles identified weight loss and impaired oral intake before treatment started, with patients requiring ONS and EFT to maintain nutrition throughout treatment. Al-Magami et al reported that patients experienced acute toxicity during radiotherapy, including grade 3 mucositis, impacting nutrition, with some patients requiring EFT throughout treatment. Long term, this radiotherapy regimen led to a reduction in pain and an improvement in trismus, leading to weight gain and a reduced dependency on EFT. However, this radiotherapy regimen is not commonly used for patients with AHNC. Al-Magami et al's results were contradicted by Veluthattil et al's study, which reported impaired oral intake due to radiotherapy side effects, with patients requiring EFT and ONS post radiotherapy, with xerostomia impairing oral intake. This may be due to varying endpoints for follow-up post radiotherapy. Scholes and Mayer also noted weight loss during radiotherapy caused by anorexia. Some studies observed that despite aggressive nutritional support, including enteral feeding, no weight gain was observed following treatment. 41
Malnourished patients treated with immunotherapy reportedly had a worse progression-free survival (PFS) and worse overall survival (OS) compared to patients without malnutrition. Enteral nutrition and parenteral nutrition (PN) were also linked to reduced PFS and OS but were not statistically significant in multivariable analysis. 49
Theme 3. Identification and Treatment of Malnutrition
Early screening for malnutrition was highlighted as a critical component of care.30,45,50,51 Haas et al recommended the Geriatric Nutrition Risk Index (GNRI) to screen patients treated with immunotherapy. 49 This tool focuses on ideal weight and albumin as opposed to BMI, and predicted survival and immunotherapy response in patients. Just over a quarter of the included articles in this review discussed weight loss as a symptom of AHNC.28,29,31,3335–3741,50,52–54 Del Rosario-Ocampo identified weight loss as the third most common symptom in hospice admissions, and Sesterhenn et al observed severe weight loss (16.2% + 10.9% body weight) in the last 6 months of life.29,35 Malnutrition was the cause of death for 6% (n = 6) of patients in 1 study, 26 and another reported dehydration as the cause of death for 2 patients. 52
Nine interventions, other than EFT, were used to prevent malnutrition. This included PN,45,49 ONS,27,33,45,50,53,54 dietary modifications,33,41,46 nutritional counselling, 55 a high-energy diet, 54 swallowing strategies,26,41 thickener 50 and medications such as dexamethasone or megestrol acetate, used to improve patients’ appetite.26,32,40,54 Feeding at risk was used in patients to improve QOL.33,40 While these interventions are described, the timing of these interventions was ambiguous, and the articles did not state whether a combination of the interventions was used. Some articles named the nutritional intervention as an outcome, for example, 42 patients using an EFT. 44 Other articles linked nutritional interventions to more specific outcomes such as weight changes (n = 13 studies), QOL (n = 4), distress (n = 7), survival (n = 5), BMI (n = 3), hospital admissions (n = 3) and biochemistry (n = 2).
Five studies identified that PN was used to prevent malnutrition and dehydration30,41,45,46,49,56 caused by dysphagia and tumour obstruction. Yokota et al reported no advantage in using PN over ONS or EFT, 45 with Hass et al reporting that PN reduced PFS when using the GNRI (P = 0.015; P = 0.023).49 Three articles discussed using parenteral fluids for hydration; however, they concluded that it has little effect and should be used if necessary.41,46,56
Theme 4. The Experiences of Patients and Family Carers
Frustration and distress caused by impaired eating and drinking, loss of appetite and weight loss were reported by patients. 31 A prospective study by Ostwal et al highlighted that loss of appetite was a recurring source of distress for patients across 4 different time points during advanced cancer care follow-up. 57 Carers described feeling helpless and distressed when witnessing patients struggling with oral intake and weight loss.29,37 EFT placement resulted in psychological distress for both patients and carers, with EFT impacting QOL.44,58 The emotional, cultural and symbolic significance of food was highlighted by 3 studies,30,44,56 underscoring the need for psychosocial support alongside nutritional interventions. The majority of studies discussed the experiences of patients and carers; however, the experiences of healthcare professionals in relation to nutrition were not discussed in any depth, highlighting a gap in the literature. Exploring the experiences of healthcare professionals would provide valuable insights into the emotional and ethical dimensions of clinical practice. These perspectives would provide a more holistic understanding of managing nutrition and the nuances of ethical dilemmas and implementing nutrition interventions in this patient group.
Discussion
Four main themes were identified in this scoping review. Enteral feeding was frequently used to address malnutrition, providing a route for nutrition and medications. Some studies report associations with survival or QOL, although evidence is largely retrospective. However, other nutritional interventions such as ONS, nutritional counselling, altered textured diet, and feeding at risk are discussed but not explored in detail. Patients are selected on an individual basis for feeding tube insertion, with some patients declining EFT placement. Patients should be involved in the decision-making process regarding EFT placement and the ethical considerations regarding feeding at the end of life. Evidence on patients’ and carers’ experiences of nutrition and its impact on QOL is limited. The scoping review identified that the side effects of AHNC treatments affect oral intake; however, regimens and treatments vary, altering the severity of the symptoms.
Several different hypofractionated radiotherapy regimens have been studied 59 with symptom relief related to pain, dysphagia, trismus and hoarseness,60,61 with some studies observing longer PFS and OS, 61 warranting cautious interpretation. Alleviation of pain and dysphagia will improve nutritional intake for some patients; however, for others, the benefits may be minimal. Treatment-related toxicities, including mucositis, xerostomia, and pain, can impair further oral intake. These patients may require enteral feeding and/or ONS to support them while on treatment. In a review of published regimens, Finnegan et al noted late effects of hypofractionated radiotherapy such as mucositis and xerostomia, which can compromise nutritional intake longer term, contributing to weight loss, compounded by tumour progression.
The nutritional needs of patients with HNC are complex and pose significant challenges for healthcare professionals and carers. Patients experience several physical symptoms, including dysphagia, anorexia, pain, trismus and tumour obstruction, exacerbating the risk of malnutrition, impacting patients’ overall treatment and QOL.62,63 Malnutrition in this patient population is multifactorial, driven by the effects of the tumour on oral and pharyngeal structures, as well as the side effects of prior cancer treatments such as surgery or chemoradiotherapy.11,64 The impact of malnutrition can lead to increased complications, hospital readmissions and a decline in QOL.16,65 To mitigate these risks and help maintain QOL, patients diagnosed with AHNC should be screened regularly throughout advanced cancer treatment. 63
Despite initiating nutritional interventions, including enteral feeding, weight loss often persists in this population; however, this does not mean it should be overlooked. Food holds a psychosocial significance for patients, beyond sustenance, holding cultural, emotional and symbolic importance, and the loss of this can be distressing. 66 For carers, watching loved ones waste away or relying on EFT can cause distress, leading to feelings of helplessness. 67 Malnutrition is linked to distress, anxiety and depression and contributes to distress independently of other psychosocial outcomes. 68 For example, some patients withdraw from social situations due to difficulty swallowing or eating in front of family. This underscores the implications of malnutrition on emotional well-being and highlights the need for psychosocial support in the form of nutritional counselling from healthcare professionals to support both patients and carers.
Enteral feeding was commonly used to prevent malnutrition, particularly through gastrostomy and NGTs. These tubes provide an alternative route for administering nutrition, hydration and medications when oral intake is not possible. 69 Current literature suggests that early placement of EFT is used with the intention of preventing malnutrition and may support treatment outcomes, particularly in patients with AHNC 11 ; most evidence, however, is descriptive. EFT may not always align with patients’ wishes at the end of life, with some patients prioritising QOL and comfort over EFT insertion. 70 There can be challenges with enteral feeding, with some studies reporting patients decline EFT due to the psychological burden and discomfort associated with tube placement, highlighting the need for patient-centred care and shared decison making when deciding on EFT placement. 62
In patients undergoing curative treatment, some studies have documented the didactic nature of having an EFT, with patients describing positive and negative feelings. While the EFT provided easy access to nutrition, fluids and medications, and helped maintain weight, they also recognised the psychological benefits the EFT provided, feeling relieved from the burden and pain of eating and the reassurance that they were being nourished. 71 Patients also described the feeding regimens as being time-consuming, disturbing them when they slept and restricting hobbies and physical activity. 72 Socially, gastrostomy tubes were perceived to be more acceptable than NGTs, with patients reporting being stared at in public, leading to patients opting to stay at home and withdrawing from social situations. 71
Investigating alternative nutritional interventions, including ONS, dietary counselling, modified texture diets and various feeding strategies, is crucial. While these options are highlighted as nutritional interventions to prevent malnutrition in AHNC, they remain under-researched, and their potential to enhance QOL remains unknown. 64 While enteral feeding is regularly used, there are few studies investigating patients who decline or are not offered feeding tubes. The current lack of rigorous studies evaluating alternative nutritional interventions prevents healthcare professionals from making evidence-based recommendations, which could provide more tailored advice for individual patient preferences, reducing reliance on EFT.
The ethics of tube feeding at the end of life adds another layer of complexity to nutritional support in AHNC care. In this context, the dilemma is whether to address malnutrition as a treatable condition or accept it as a consequence of disease progression. 73 The principles of autonomy, beneficence, nonmaleficence and justice must be balanced when making decisions regarding nutritional interventions at the end of life. Nutritional intake in this patient group is often restricted for anatomical reasons, leaving patients with the potential risk of death from malnutrition or dehydration. Enteral feeding is described as having the potential to support treatment tolerance, maintain nutrition and extend life, 70 but further evidence in this area is warranted. However, enteral feeding can be perceived as prolonging suffering in a group with an already diminished QOL and distressing symptoms.70,73 Cultural and religious concerns need to be addressed when initiating tube feeding, with values shaping patients’ and families’ perspectives on end-of-life care. 74 Muslims often believe that patient autonomy is secondary to the physician's authority over what benefits the patient, while the Taiwanese culture believes that an individual's soul will be restless if they die hungry. In Western culture, poor nutrition is associated with illness and death. 75 Ignoring these values can lead to reduced adherence, emotional distress and a poor death. Therefore, diverse dietary customs, beliefs and the wishes of the patient and carers are essential for making informed decisions regarding the placement of EFT.
The findings of this review recommend that effective communication is essential to ensure that patient goals and preferences are explored 73 and that enteral feeding in this patient group should be individualised, prioritising a patient-centred approach. 76 Shared decision-making facilitates a collaborative approach, allowing healthcare professionals to tailor decisions regarding the need for EFT, not only to patients’ clinical needs but also taking into account patient preferences and wishes, and how an EFT may impact their QOL. This shared decision-making is important in the final days or weeks of life when nutritional goals change from maintaining nutritional intake to comfort and dignity. The review also recommends that EFT should not be placed in the last weeks of life. If enteral feeding has already been commenced, consideration should be given to reducing or stopping the feed altogether if appropriate, providing an individualised approach.
Future research should focus on patient-centred approaches that consider both the physical and psychosocial impacts of nutritional interventions. Additionally, qualitative research exploring the experiences of patients and carers treated with various nutritional interventions could offer valuable insights into how these approaches align with patients’ holistic needs and contribute to QOL. These findings could aid the development of ethical guidelines and clinical recommendations that balance treatment efficacy with spiritual, physical, emotional and cultural dimensions of AHNC. 77
The studies analysed were not evaluated for the quality of their evidence nor critically appraised; therefore, the results are a summary of the current practice of nutritional interventions. To encapsulate as much evidence as possible, broad search terms were used. Many studies included in this review had small sample sizes and where retrospective in nature; therefore, caution is required when interpreting the results. The absence of clearly defined outcomes when employing nutritional interventions limits the interpretability and comparability of findings and therefore hinders the development of evidence-based guidelines. However, it may be difficult to interpret any benefits of nutritional interventions due to the heterogeneity of nutritional interventions, timings, individual patient needs and deterioration. The majority of the studies were European (n = 11), limiting the generalisability of findings across the world and between healthcare systems. Despite the inclusion of a wide range of articles, the experiences of healthcare professionals caring for these patients with complex needs and symptoms were overlooked. The absence of healthcare professionals’ perspectives within the existing literature restricts the understanding of how nutrition is managed in this patient group in practice and highlights opportunities for improving training to deliver patient-centred care. Exploring healthcare professionals’ experiences of nutritionally managing these patients may lead to improved patient care and provide better insights on how to support patients and their families.
Conclusions
The review highlights the complexity of nutrition in AHNC and the importance of developing a patient-centred approach to nutritional management. While enteral feeding is frequently used and reported, further studies evaluating the effectiveness of alternative nutritional strategies and interventions are required. All nutritional interventions should be tailored to individual needs and enable them to achieve their goals. Healthcare professionals often navigate uncertainty while trying to balance patient preferences and QOL with clinical indications for nutritional interventions, especially regarding EFT. The development of more structured guidance or tools to aid clinical decision-making would standardise pathways and support more equitable and patient-centred care while improving confidence among healthcare professionals. Further qualitative research is needed to explore the experiences of patients, carers and healthcare professionals regarding nutrition at the end of life, including patients who decline nutritional interventions.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank Lynn Harris, University of Birmingham Librarian, for her contribution to the research strategy.
Ethical Considerations
As this study is a scoping review, formal ethics approval was not required.
Author Contributions
RS, NE and PG conceived and designed the review. RS, SC and JO completed all the searches, conducted the initial screening and reviewed the full manuscript. RS, NE and PG analysed and interpreted the data. RS drafted the manuscript, and all authors contributed to its revision. All authors have approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Pre-Doctoral Clinical Academic Fellowship from the National Institute of Health Research (NIHR303494) awarded to RS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.