
Abstract
This paper investigated the degree to which legally-involved individuals’ criminal history was related to their responses on a validated screener for substance use. Using data from 56,000 people released from the Illinois Department of Corrections, this study examined whether prior arrests, arrests for violent crimes, and arrests for drug-law crimes were associated with substance use prior to prison, the identification of which drug caused the individual the most serious problems, and need for substance use treatment. Most of the relationships between criminal history indicators and self-reported substance use were weak. The exception to this trend was a moderate-to-strong correlation between methamphetamine arrests and methamphetamine use, which may reflect how rural jurisdictions in Illinois are using prison as a response to crime. This paper highlights the importance of drug screening to identify drug use problems and treatment need rather than relying solely on criminal history and drug law violations.
Introduction
At the end of 2021, 5.4 million people were under the supervision of the United States legal system (Carson & Kluckow, 2023). This includes approximately 1.5 million people—a national increase for the first time since 2005—in jail or prison (Sawyer & Wagner, 2024). Three hundred and sixty thousand people are incarcerated in the United States for a drug-related offense (e.g., possession, distribution; Sawyer & Wagner, 2024), and drug-related crimes account for about a quarter (26%) of all annual arrests (National Center for Drug Abuse Statistics, 2024). Substance use-related difficulties have been documented as a noteworthy behavioral health concern for incarcerated populations (see Staton-Tindall et al., 2011). The consequences of substance use in incarcerated samples includes, but is not limited to, higher rates of recidivism (Zgoba et al., 2020), a greater chance of drug overdose (Binswanger et al., 2016), and an increased all-cause mortality rate (Chang et al., 2015). Consequently, justice agencies provide substance use treatment for people in prison to improve both client and public safety outcomes (De Andrade et al., 2018).
Public health initiatives designed to improve the outcomes of incarcerated populations have led to the implementation of practices that identify, prevent, and treat substance use disorders (Belisle & Solano-Patricio, 2022; Chandler et al., 2009; Russell, 2019). Cascade of Care frameworks, in particular, have been used in prisons to ensure people showing a need for substance use treatment receive programming while incarcerated or following release (Ray et al., 2022). Commonly consisting of screening, assessment, treatment referrals, treatment initiation, and retention (Belenko et al., 2018; Mugavero et al., 2013; Williams et al., 2019), Cascade frameworks are intended to maximize service delivery within the target population. The use of Cascade models with legal samples has been related to improved treatment outcomes for both infectious disease and substance use (Grella et al., 2022; Hariri et al., 2020; Socías et al., 2018). Studies closely examining specific stages of the Cascade (e.g., screening) have the potential to inform practices that aid in the identification and treatment of substance use disorders.
Screening is a crucial step in the identification of people with a need for substance use treatment (Belenko, 2006; self-cite; Kubiak et al., 2005). The screening process can include, for example, justice agencies developing organizational policies that require all persons be screened for a substance use disorder upon admission. The results from a screener can then be used to make evidence-based treatment decisions (e.g., residential vs. outpatient; see Long et al., 2019 for an empirical example). The use of evidence-based screeners in legal settings, however, varies widely across the United States (e.g., Bunting et al., 2023; Ray et al., 2022; Scott et al., 2019; Taxman et al., 2007a, 2007b). Failing to properly screen for substance use may lead to a mismatch between a client's treatment needs and program intensity, which has been shown to impede progress in treatment (e.g., Bonta et al., 2000). In this way, identifying reliable indicators predicting someone's need for substance use treatment can maximize the efficiency and accuracy of the screening process.
Static and Dynamic Risk Factors: Predicting Treatment Need
Indicators warranting intervention is commonly conceptualized as either static or dynamic (see Wong et al., 2009, pp. 84–86). Static risk factors, including age, sex, and criminal history, are immutable characteristics that increase someone's risk for recidivism (Taxman & Smith, 2021, p. 101459). Conversely, dynamic risk/need factors are theoretically malleable (e.g., substance use, mental health, negative peer groups; Andrews & Bonta, 2010) processes that can be intervened upon to lessen one's risk for recidivism. Collectively, the impact of static and dynamic factors is frequently assessed with respect to their association with recidivism.
Studies on how static and dynamic risk factors influence recidivism have produced mixed results (e.g., Caudy et al., 2013; Eisenberg et al., 2019; Wiese, 2022). A recent systematic review, for example, reported that dynamic risk factors (e.g., substance use, employment problems, and marital problems) were comparable to static factors (e.g., age, gender, and criminal history) when predicting recidivism for people with community sentences (Yukhnenko et al., 2020). In contrast, a systematic review including people released from custody concluded that static risk factors were superior to dynamic factors when predicting recidivism (Goodley et al., 2022). Despite mixed findings, the literature is conclusive in that both static and dynamic factors are related to general, sexual, and violent recidivism (rs = 0.02–0.17; Katsiyannis et al., 2018), suggesting that people with more static and dynamic risk factors would benefit from some form of recidivism reduction program. Additional research is needed on how static and dynamic factors interact to predict risk, and by extension treatment need, so that clinical resources are allocated for those with the highest treatment needs.
Criminal history is an especially robust predictor of recidivism (United States Sentencing Commission, 2017) that could serve as an indicator of treatment need. People with a more extensive criminal history, for instance, have been found to report more physical health problems (Mateyoke-Scrivner et al., 2003) and substance use (Pierce et al., 2017). It may seem reasonable then to assume that someone with a drug-related offense would have a greater need for substance use treatment relative to someone without a drug-related offense. However, there remains limited research on the connection between criminal history, substance use patterns, and substance use treatment need.
Studies have noted differences in drug and alcohol use patterns between people with and without violent offenses (e.g., Håkansson & Jesionowska, 2018; Proctor et al., 2017). For example, people in prison for a violent offense (as compared to people with a drug-related offense) reported less illicit and injection drug use and more binge drinking and sedative drug use (Håkansson & Jesionowska, 2018). Another study found a lower incidence of cocaine dependence among people with a violent crime, but no difference in other drug-specific dependence (e.g., alcohol, marijuana, and heroin) when comparing people with more or less than 10 prior arrests (Proctor et al., 2017). These studies highlight important differences in drug use patterns between people with and without a history of violent crime yet fail to capture how these differences are related to treatment need. By further understanding the relationships among criminal history, substance use, and treatment, justice agencies may be better positioned to serve individuals involved with the justice system. If criminal history is related to substance use, and perhaps more importantly, treatment need, agencies can use this information to identify persons in need of treatment with greater acuity. Conversely, the absence of a relationship between criminal history and substance use behavior would further underscore the need for all people in the justice system to be screened using an evidence-based screener and not to conflate certain criminal history as a reliable indicator of treatment need.
Current Study
The current study sought to examine the extent to which criminal history—a static risk factor for recidivism—served as an indicator of substance use in the year prior to incarceration and current substance use treatment need using a sample of individuals released from prison in the United States. Within the Illinois Department of Corrections, a validated screener for substance use disorders (i.e., Texas Christian University Drug Screen II [TCUDS-II]) assists in the identification of individuals that may need treatment. Without such a screening instrument, identification of who may need treatment would be based solely on current conviction offense or an individual's criminal history. Therefore, this study gauged the degree to which there was a correlation between the extent and nature of a person's criminal history and self-reported substance use behaviors. Overall, the current paper was guided by the following three research questions:
To what degree does a more extensive criminal history correspond to more problematic drug use as reported on the TCUDS-II? What is the relationship between the number of prior arrests for drug-law violations and self-reported drug use; and does this relationship generalize when examining drug-specific use and offenses? Does the magnitude of the relationship between criminal history and self-reported drug use vary by assigned sex and race?
Method
Procedure and Sample
The sample used for the analyses included all individuals released from prison in Illinois from January 2018 through December 2022, excluding those who had been admitted to prison for a technical violation of their mandatory supervised release (i.e., “parole”). During that sampling period, there were a total of 68,643 unique individuals released from prison. All people who are admitted to prison in the state of Illinois are required to be administered the TCUDS-II to screen for substance use problems and inform treatment recommendations. This information was used to quantify participants’ self-reported substance use, the substance causing them the most issues in the past 12 months, and treatment need. Using the available inmate ID numbers, we requested participants’ criminal history information through the state's Criminal History Record Information (CHRI). Inconsistencies in reporting resulted in 12,030 people having incomplete records. Only individuals with complete data were included in this study, resulting in a final sample of 56,613 people who had a TCUDS-II score and a complete criminal history record.
Measures
Demographic Information
It is standard practice for prisons in the state of Illinois to collect the demographic information of new residents at intake. This information was used in the current study and included participants’ age, sex, and race/ethnicity.
Criminal History
The current study collected detailed information about participants’ criminal history using the Illinois State Police's CHRI system. Criminal history was recorded as the number of arrests prior to incarceration (i.e., count data), categorized-based on whether these offenses were general, violent, or drug-law violations, and grouped into drug-specific offenses (e.g., alcohol, cannabis, methamphetamine) when possible. Analyses involving offense type relied on the charge listed as the primary charge given individuals could have been sentenced for multiple charges.
Substance Use and Substance Use Treatment Need
Drug use in the year prior to prison, including the substance causing respondents the largest problem, and current treatment need were measured using the TCUDS-II (Institute of Behavioral Research, 2018). The TCUDS-II is a validated screener for substance use that was developed based on the DSM-IV diagnostic criteria for substance use dependence. This screening assessment includes 15 items asking respondents to report on their substance use behavior in the 12 months prior to incarceration. The nine items used to quantify treatment need are presented on a dichotomous scale (No = 0, Yes = 1) Supplementary items that are not included in the scoring of treatment need are included to provide additional information that may inform programing. Of particular interest, participants were asked to indicate the drug that caused them the most serious problems in the past 12 months. Total scores on the TCUDS-II were scored by taking the sum of all items, ranging on a continuous scale from 0 to 9. Scores greater than 3 were used as an indicator of need for a treatment referral and/or treatment services. Using this cut off, we created a dichotomous variable representing treatment (Treatment Need vs. No Treatment Need).
Analytic Plan
Bivariate analyses (e.g., chi-square tests) were performed to examine the relationship between various measures of criminal history (i.e., prior arrests for various offenses) and self-reported drug use from the TCUDS-II. The analyses progressed from examining the relationship between general measures of criminal history—total arrests and total arrests for violent crimes—to measures that were more specific to possession or distribution of drugs.
Similar analyses were performed to determine the relationship between prior arrests on drug charges and whether each specific drug was reported on the TCUDS-II as the drug causing the individual the most serious problems. Due to how Illinois’ drug laws are categorized, it was only possible to isolate arrests involving a few specific substances. For example, prior arrests for offenses that involved alcohol included driving under the influence (DUI), minor in possession, or a violation of Illinois’ Liquor Control Act. It was also possible to isolate prior arrests specifically for methamphetamine offenses (e.g., possession, manufacture, delivery as defined in Illinois’ Methamphetamine Control and Community Protection Act) and prior arrests for offenses involving cannabis (as defined in the Illinois Cannabis Control Act). It is important to note that Illinois legalized recreational cannabis in 2020, and thus arrests for cannabis possession were less likely after that law went into effect. Further, criminal records involving cannabis possession were expunged if they involved 30 grams or less and likely effected the data used in these analyses. Still, one in five of the cases included in the analyses had a prior arrest for a cannabis offense. Most other substances (e.g., cocaine, crack cocaine, and opiates/heroin), however, are all combined into one broad category—the Illinois Controlled Substances Act, and therefore it was not possible to isolate prior arrests involving heroin, for example. Only when relatively large amounts of drugs were involved (e.g., possession) for these Illinois Controlled Substance Act offenses was it possible to distinguish the drug type.
In addition to examining the relationship between self-reported drug use and prior arrests for drug-law violations, we also examined the association between an individual's TCUDS-II score and the number of prior arrests for all crimes and violent crimes. Because of the large sample size (∼56,000 cases), almost all chi-square tests were statistically significant. To measure the strength of the relationship; Kendall's tau-c, Phi, or Spearman's Rho was calculated for each set of bivariate analyses; depending on which was most appropriate given the data structure.
Results
Sample Characteristics
Table 1 summarizes the demographic, current offense and criminal history, and TCUDS-II results for the entire sample. Most individuals in this study were males, Black, and sentenced to prison for a non-violent crime. Over 40% reported at least monthly use of alcohol and cannabis prior to incarceration, while roughly 20% reported monthly use of cocaine, opiates and methamphetamine. The screening portion of the TCUDS-II includes nine questions designed to identify different clusters of substance use symptoms (e.g., physical dependence, substance use interfering with responsibilities, etc.). A score of three or higher on this screener suggests the need for substance use treatment or at least a more thorough diagnostic assessment. Overall, 55% of the sample was considered in need of a treatment referral and/or substance use programing.
Characteristics of Sample of 2018–2022 Illinois Prison Exits (N = 56,613).
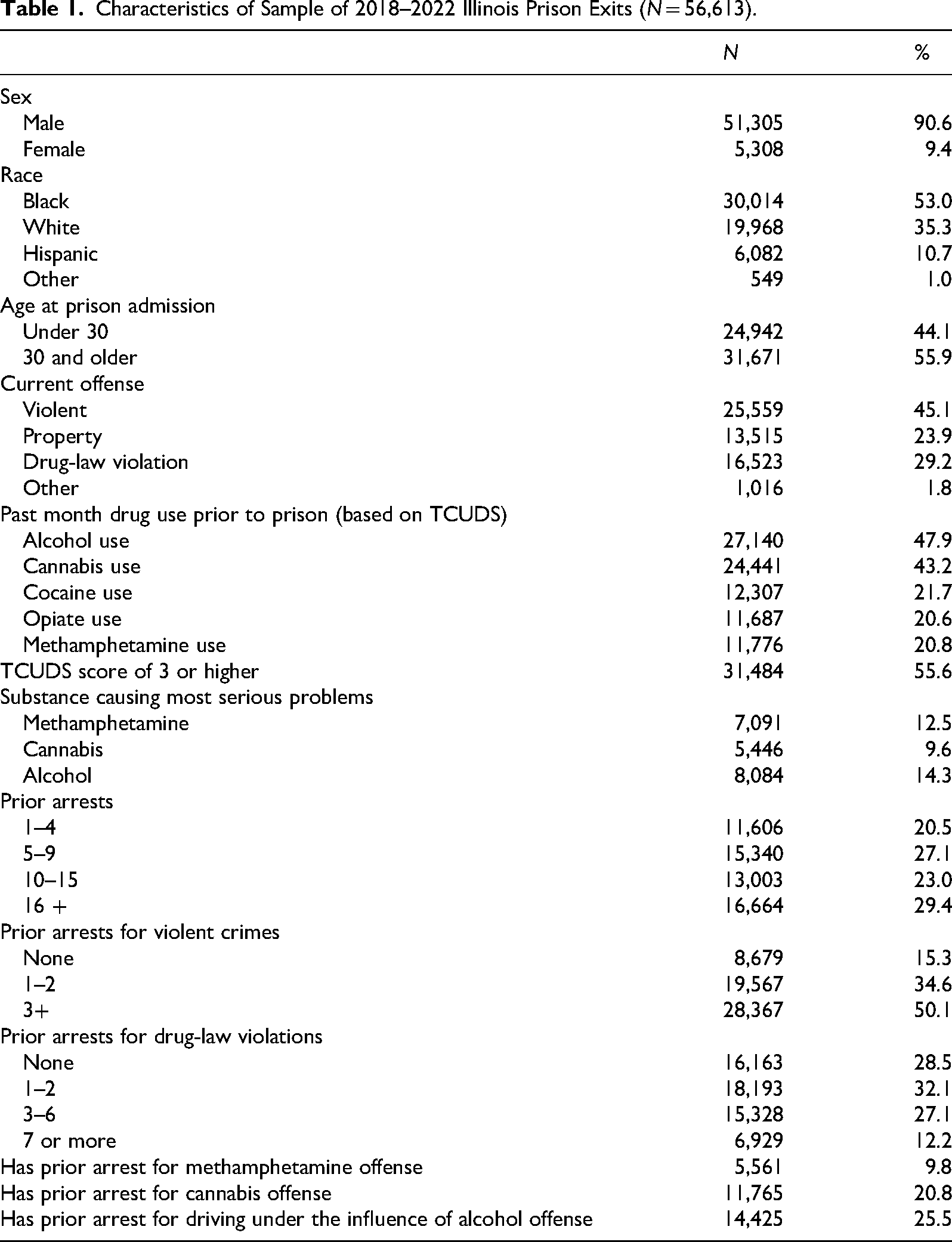
The average number of total prior arrests was 12.9, with 29% having 16 or more prior arrests. Most (85%) had prior arrests for violent crimes, with roughly 50% having three or more prior arrests for crimes of violence. Additionally, almost 70% had a prior arrest for a drug-law violation. When arrests involving specific drugs were examined, relatively few (9.8%) had a prior arrest for methamphetamine, while 20% had a prior arrest involving cannabis, and 25% had at least 1 prior arrest for DUI of alcohol.
Criminal History, Substance Use, and Treatment Need
When analyses were performed to measure the correlation between general measures of prior arrests (total prior arrests and prior arrests specifically for violent crimes) and whether the individual showed a substance use treatment need, the strength of the relationships were extremely weak (τc = 0.02, p < .001). Similar patterns of low correlation were seen when the interval-level measures of prior arrests and ratio-level TCU scores were compared (rss ≤ 0.04).
Similarly, low levels of correlation were seen when the number of total prior arrests and prior arrests for violent crimes were compared with whether the individual reported past-month use of specific substances, and these patterns remained when using interval/ratio level measures of prior arrests (rss ≤ 0.08). Interestingly, there was a slight inverse correlation between total prior arrests and use of cannabis and methamphetamine (rs ≤ −0.08); as well as a slight inverse correlation between prior arrests for a violent crime and past month use of cannabis, heroin/opiates and methamphetamine (rs ≤ −0.08).
Similar analyses were performed separately for males and females to determine if the magnitude of correlations were sensitive to the sex of the individual. In several instances, the strength of the correlation was slightly higher when the analyses only included females (note by correlation coefficients in parentheses in Table 2). For example, the correlation between methamphetamine use and prior arrests for violent crimes was −.16 (p < .001) for females, compared to 0.07 for the whole sample (which is 90% male). Separate analyses were also performed to determine if the correlations differed between Black (differences noted by correlation coefficients in [ ]) and White individuals (differences noted by { }). For the most part there were few differences in the correlations when analyses were performed separately for Black and White individuals. A couple notable differences included a stronger inverse correlation among people who were Black between prior arrests for violent crimes and cannabis use, no significant correlation between heroin/opiate and methamphetamine use versus prior arrests for violent crimes. Among people who were White, there was a stronger correlation between TCUDS-II scores and prior arrests for drug-law violations, and treatment need and methamphetamine use.
Correlations (Kendal's Tau-c & Phi) Between Criminal History Measures, TCUDS, and Specific Problem Drug.

Note. *Correlations are statistically significant at an alpha of .05 (females); [black]; {white}. For ease of interpretation, correlation coefficients for subsamples were only reported if larger than that using the full sample.
Correlations (Phi) Between Prior Drug Arrests, Monthly Use and Treatment Need (TCUDS Scores of 3 or Higher).
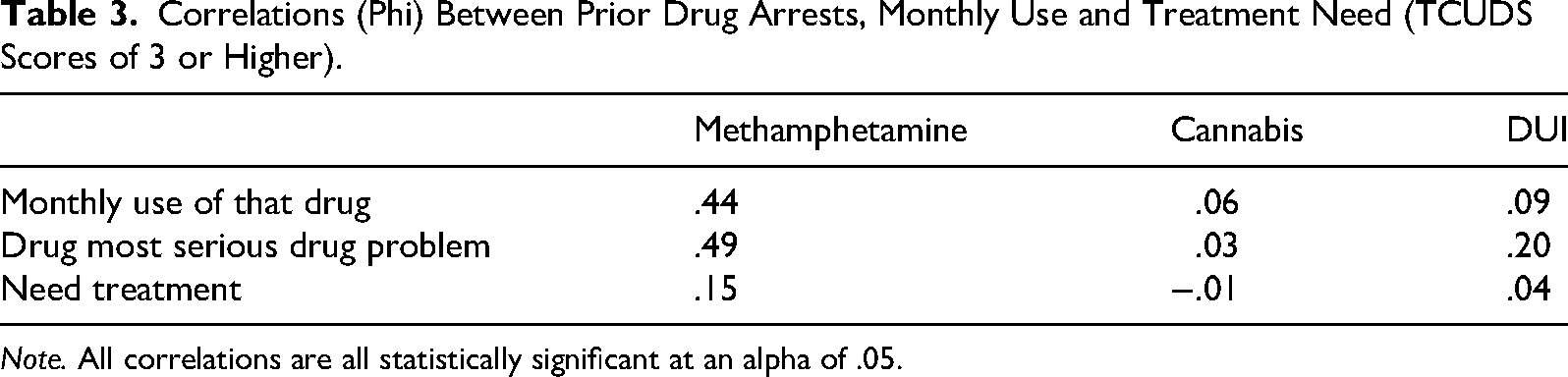
Note. All correlations are all statistically significant at an alpha of .05.
Drug-Related Offenses, Drug-Specific Offenses, and Drug Screening Scores
When the relationship between prior arrests for drug-law violations and measures of treatment need and drug use was examined, similarly low-levels of correlation were found. For example, the highest correlations were seen between prior arrests for drug offenses and treatment need (τc = 0.11, p < .001), and prior drug arrests and heroin/opiate use (τc = 0.12, p < .001). Finally, the relationship between the offense that resulted in the sentence to prison (i.e., a drug-law violation or some other offense) and treatment need was weak. For example, the strongest correlation was only 0.13 (i.e., rφ = 0.13, p < .001) between whether the current prison sentence was for a drug offense and the TCUDS-II score.
The structure of Illinois’ drug laws did not allow for the determination of all specific drugs involved in prior arrests. The exceptions are cannabis and methamphetamine—both of which have separate legal classifications allowing for the identification of arrests specifically for offenses involving these substances (e.g., possession, delivery, and manufacture). In addition, the one alcohol offense which can be easily identified in state law and arrest records is DUI of alcohol. Thus, for these three substances—cannabis, methamphetamine, and alcohol—it was possible to examine the correlation between prior arrests for offenses involving these drugs and reported monthly use using the TCUDS-II, whether that drug was identified by the individual as causing them the most problems, and if they showed a need for substance use treatment.
As shown in Table 3, the results of these analyses revealed stronger correlations specifically for methamphetamine arrests, monthly use, and problems. Specifically, the correlation between whether the individual had at least 1 prior arrest involving methamphetamine and if they reported using methamphetamine monthly prior to prison was 0.44, p < .001. Similarly, having a methamphetamine arrest was also strongly correlated (0.49, p < .001) with the individual identifying methamphetamine as causing them the most problems. However, despite these strong correlations, prior arrests for methamphetamine offenses were weakly related to TCUDS-II scores greater than 3 (i.e., treatment need; 0.15, p < .001). Further, it is important to note that those with an arrest for a methamphetamine offense accounted for less than 10% of the total sample. The correlations between cannabis arrests, monthly cannabis use, cannabis causing serious problems, or need for treatment were all weak (0.06 or lower), but could be due to the issue described above regarding the expungement of cannabis possession offenses following the legalization of recreational cannabis in Illinois. Similar weak correlations were seen between arrests for DUI of alcohol and alcohol use and treatment need; a slightly higher correlation (0.20, p < .01) was seen between having a prior DUI arrest and alcohol being identified as the drug causing the individual the most problems.
Discussion
Individuals in jail or prison are negatively affected by substance use-related concerns (Baranyi et al., 2019; Butler et al., 2022; Fazel et al., 2017). Having a diagnosis for a substance use disorder, for instance, has been related to higher rates of recidivism (Zgoba et al., 2020) and drug overdose deaths following release (Binswanger et al., 2016). In this way, there remains a need for jails and prisons to provide substance use programing. The purpose of this paper was to investigate whether criminal history—a static risk factor associated with recidivism outcomes (United States Sentencing Commission, 2017)—was correlated with substance use in the year prior to incarceration and substance use treatment need. This included examining various offense categories, such as general, violent, drug-related, and if people with drug-specific offenses (e.g., methamphetamine, cannabis) were more likely to report substance use and have a substance use treatment need.
The relationship between criminal history—when assessed as the number of total prior arrests and prior violent arrests—and substance use during the past month was weak. These findings contribute to a nascent literature highlighting differences in drug and alcohol use patterns among people with varying criminal histories (Håkansson & Jesionowska, 2018; Proctor et al., 2017). Although differences have been noted, this study found the correlation between criminal history and offense type (general vs. violent) with substance use patterns to be modest in a large representative sample of people in prison. A similar effect was observed when assessing the relationship between criminal history and substance use treatment need. Overall, these analyses suggest that, despite the purported differences in drug and alcohol use patterns, these differences may lack practical significance—indicating that this information should have minimal impact on case management decisions and program assignment.
When examining drug-related charges, the relationships among criminal history, substance use, and treatment need were similarly weak. This pattern of results remained consistent when examining the number of previous drug-related offenses as well as sentencing offenses that involved drug violations. The absence of a notable association among these variables underscores the importance of using evidence-based screeners for substance use rather than a client's history of drug-related violations, especially considering national reports documenting the inconsistent use of screeners in legal settings (e.g., Bunting et al., 2023) Failing to screen people at intake may hinder the identification of treatment needs, prevent service delivery to those in need of care, and cause a mismatch between treatment need and program intensity.
The largest relationship observed in the current study was that between methamphetamine-related violations and self-report methamphetamine use before prison, and between methamphetamine-related violations and methamphetamine being endorsed as the substance causing participants the most difficulties. The strength of the association between methamphetamine offenses, methamphetamine use, and problems with methamphetamine could be a byproduct of how rural communities tend to provide harsher sentences for drug-related crimes when compared to urban communities (e.g., Ruhland & Holmes, 2023). Indeed, 40% of all those in the current study sentenced to prison from rural counties were for drug-law violations, compared to 26% of those sentenced from urban counties. This interpretation of the data suggests that these relationships may be overestimated and is further supported by the strength, or lack thereof, of the associations among arrests, monthly use, and substance use problems for alcohol and cannabis—two substances that are generally considered less “serious” when compared to methamphetamine.
This study can be used to inform how screening practices are used to identify people who could benefit from substance use treatment. An overarching theme of this paper was to evaluate the interaction between a static risk factor for recidivism (i.e., criminal history) and a dynamic treatment need (i.e., substance use). Across analyses, the association between these criminal history and drug-related outcomes was small—suggesting that criminal history should not be used as an indicator of substance use or substance use treatment need. Said differently, having arrests for drug-law violations does not necessarily imply a need for substance use treatment and the absence of arrests for drug-law violations does not indicate the absence of a treatment need. Failing to treat these risk/need factors as independent sources of information may misrepresent someone's risk and needs. Thus, despite the differing use of evidence-based substance use screeners in legal settings (Bunting et al., 2023; Ray et al., 2022; Scott et al., 2019; Taxman et al., 2007a, 2007b), screeners specifically for substance use should be part of the recommended approach for identifying candidates for substance use treatment.
Strengths, Limitations, and Future Directions
There are strengths and limitations of this paper that should be considered when interpreting its’ results. This study used a sample of more than 56,000 people in prison to evaluate the relationship between criminal history, self-reported substance use, and substance use treatment need. This relatively large sample size is an analytic strength in that the magnitude of the associations reported are likely to generalize to that of the population of interest. This analysis, however, involved data collected at a single timepoint and therefore does not represent causal linkages. A more advanced analytic procedure may be useful for simultaneously modeling the relationships among criminal history, substance use, and treatment need, potentially lending itself to a more accurate representation of how these variables are related. With this research, researchers should consider the effect of additional grouping variables not assessed in this investigation. For example, future research may consider using a multilevel framework to answer questions related to how community- (e.g., socioeconomic status) and state-level (e.g., state-specific drug laws) characteristics impact on the associations among criminal history, substance use, and treatment need.
Substance use behavior was collected using the TCUDS-II—a validated screening tool for substance use behavior. This approach could be viewed as a limitation in that it introduces a potential for response bias. Individuals completing the TCUDS-II could have felt pressured to underreport their substance use behavior given this screener was administered while in a custodial setting. Additional research may consider using behavioral (e.g., Timeline Follow Back) or biological (e.g., urinalysis) measures to determine the extent to which these approaches compare to that of self-reported substance use. Another strength of this study was the inclusion of drug-specific charges when comparing the relationship between criminal history and substance-specific use prior to incarceration. This allowed for the evaluation of the relationship between drug-specific offenses (e.g., prior arrests involving methamphetamine) and substance use treatment need for a particular substance. Alternatively, this could also be seen as a shortcoming in that information related to drug-specific offenses were limited to cannabis, methamphetamine, and alcohol. Analyses involving offense category were limited in that we relied exclusively on participating primary sentencing offense. This ignores the fact that individuals could have been sentenced for multiple charges. Participants’ charges were categorized into general, violent, and drug-law violations for ease of interpretation and based on previous work examining criminal history as an independent variable (e.g., Håkansson & Jesionowska, 2018; Proctor et al., 2017). However, this approach oversimplifies criminal history to some extent in that it does not account for their underlying motivations, such as drug use being a motivating factor for some other crime.
Conclusions
In conclusion, people involved with the legal system are adversely affected by substance use, and it is therefore imperative for the legal system to provide evidence-based programs that address substance use treatment needs. These efforts are dependent upon effective screening procedures that accurately pinpoint people in jail or prison in need of substance use treatment. The present study found that criminal history—a static risk factor associated with recidivism—was weakly associated with substance use behavior and need for substance use treatment. The exception to this trend was the moderate association between drug-specific offenses for methamphetamine. The results of this study support screening and assessment protocols that treat criminal history and substance use severity as independent risk/need factors that can be used to inform case management and assignment to substance use treatment.
Footnotes
Author Note
The authors of this paper declare no conflict of interest. This research was supported by the National Institute on Drug Abuse under grant UG1 DA050074. The de-identified data associated with this project is available upon request. Correspondence concerning this article should be addressed to Thomas B. Sease, 2800 S University Drive, Fort Worth, TX 76129, USA. E-mail: thomas.b.sease@tcu.edu
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant number UG1 DA050074).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.