
Abstract
Individuals with a history of criminal legal system (CLS) involvement may experience additional challenges to their recovery from substance addiction. We compared recovery capital trajectories of individuals in recovery residences with and without the involvement of CLS and assessed predictors of their Overall Recovery Capital Score (ORCS). We employed a quasi-experimental approach using weighted repeated measures modeling to compare the ORCS on the REC-CAP measure between 1,933 residents from 101 recovery houses (RH), with (59.9%) and without (40.1%) CLS involvement. Residents with CLS involvement showed equally positive gains in recovery capital while in recovery residences (p < .0001), despite reporting greater unmet needs at baseline. Being man (p = .01) and older age (p = .04) predicted greater recovery capital gains regardless of CLS status. Our findings suggest that RH may be an effective setting for individuals with CLS involvement to build their recovery capital.
Problematic substance use is prevalent among individuals involved with the criminal legal system (CLS; Fazel et al., 2017). Studies have shown that over half of incarcerated individuals used illegal drugs in the month preceding their offenses (Maruschak et al., 2021; Mumola & Karberg, 2007), and that reoffending rates are higher among individuals with histories of substance use (Kelly et al., 2020; Smith & Trimboli, 2010). Moreover, a review of studies from multiple countries showed that 19% to 88% of individuals in prison, probation, and police custody settings met the criteria for alcohol use disorder, as measured using the Alcohol Use Disorders Identification Test (Newbury-Birch et al., 2022). As a result of the co-occurrence of substance use and involvement in the CLS, these individuals often face challenges in their daily lives, such as societal stigmatization and difficulties securing basic necessities, including safe and stable housing and employment (Henley, 2015).
Addiction recovery and desistance processes share several key similarities, with conceptual overlap present (Best et al., 2017; Van Roeyen et al., 2017). Both concepts are strength-based approaches that involve changes in cognition and behavior, social connections, and other recovery- and desistance-related outcomes, such as employment. Furthermore, both fields emphasize the significance of recovery and desistance as holistic processes of change. In this study, we define recovery as a “process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential” (SAMHSA, 2012, p. 3). In turn, we consider desistance “long-term abstinence from criminal behaviour among those for whom offending had become a pattern of behaviour” (McNeill et al., 2012, p. 3).
Although recovery and desistance are distinct processes of change, the theories and models of these processes cover many of the same domains (Best et al., 2017; Van Roeyen et al., 2017). Both phenomena are commonly regarded as gradual processes of change that encompass three stages and include the recurring risk of substance use and criminal behavior (Van Roeyen et al., 2017). Recovery can be viewed in three stages: early recovery (the first year), sustained recovery (1–5 years), and stable recovery (beyond 5 years), all characterized by improved biopsychosocial functioning and quality of life throughout these stages (The Betty Ford Institute Consensus Panel, 2007; Dennis et al., 2007). Desistance has been categorized into primary desistance (cessation of offending behavior), secondary desistance (involving changes in social networks and identity), and tertiary desistance (where an individual’s desistance is accepted and recognized by surrounding societal groups; Maruna & Farrall, 2004; McNeill, 2016). Importantly, recovery and desistance are not about the termination of problematic substance use and offending; they also involve moving beyond these behaviors toward personal and social flourishing, as well as active social contribution (Best et al., 2017; Eddie et al., 2021; Gutierrez et al., 2022).
A range of theories has been established to understand when and how individuals initiate and sustain desistance. Sampson and Laub’s (1992, 2003) work on the life course model (Laub & Sampson, 2006), focusing on ontogenic and developmental changes, highlights the relationship between age, criminal activity, and the influence of contextual factors. Key insights from this work suggest that age alone is not the primary factor underlying desistance; instead, it is the various life transitions and experiences that occur as people age. These life transitions and experiences, or “turning points” in life, such as acquiring and maintaining high-quality relationships and achieving stable employment, contribute to positive identity change and individual agency, which ultimately facilitates desistance (Best et al., 2017). Indeed, desistance does not occur in isolation; rather, it is closely linked to developing a pro-social identity through meaningful social experiences (Maruna, 2012; Shapland & Bottoms, 2011). Moreover, Shapland and Bottoms (2011) discuss the importance of individuals accepting the constraints of a non-offending life. This often involves, for instance, making conscious decisions to distance oneself from offending-related social connections while focusing on developing desistance-supportive connections. The life course model proposes that desistance is influenced by various overlapping factors, including personal decisions and agency, as well as social and contextual influences throughout an individual’s life (Best et al., 2017).
Similarly, theories have been developed to understand how individuals initiate and sustain recovery from alcohol and drug addiction. The Betty Ford Institute Consensus Panel’s (2007) conceptualization of recovery identifies three main components: sobriety, personal health, and citizenship, which can be divided based on time (i.e., early, sustained, and stable recovery). The Recovery Capital framework (Granfield & Cloud, 1999, reviewed in more detail in the next section) also views recovery as a holistic process of change across various life domains, with a particular emphasis on the strengths and resources essential for the initiation and maintenance of recovery. This includes addressing barriers and unmet needs that may impede behavior change. One key component of the model is social recovery capital, which refers to the influence of friends, peers, and family on recovery processes. Relatedly, the Social Identity Model of Recovery (SIMOR, Best et al., 2016) focuses on the shift in self-concept from an addiction-based identity to a recovery-oriented identity (Best et al., 2016). This model specifies that recovery should not be understood as solely a personal journey of change but rather as a socially embedded process where changes in social networks are crucial. Recovery is also described as socially contagious, with individuals adopting recovery-oriented attitudes, beliefs, and behaviors by witnessing recovery within their social networks and communities (Best et al., 2015; Best & Ivers, 2021; White, 2010). Various models have also been proposed regarding stages in recovery (White & Kurtz, 2006), such as the Stages of Change model, which comprises six stages (i.e., pre-contemplation, contemplation, planning, action, maintenance, and termination; Prochaska & DiClemente, 1983). These models suggest that the recovery process begins before observable behavioral changes occur in substance use and that change can happen linearly or non-linearly as individuals may cycle through stages of change (Vilela et al., 2009; White & Kurtz, 2006).
Recovery Capital as the Basis for Understanding the Addiction Recovery Process
Recovery capital has been described as “the sum of one’s total resources that can be brought to bear in an effort to overcome alcohol and drug dependency” (Granfield & Cloud, 1999, p. 179). This framework adopts a strengths-based approach to recovery, seen as a contextually shaped journey to improved overall well-being. In this journey, external factors such as recovery-supportive relationships and access to recovery-supportive spaces and services within the community matter. Recovery barriers and unmet needs are also integral to this framework, referring to all the personal, social, and community-related aspects that hinder or prevent individuals from achieving or maintaining recovery (Best et al., 2020; Cloud & Granfield, 2008). Incarceration, in particular, has been described as an experience that can act as a major barrier to developing recovery capital (Cloud & Granfield, 2008). Prison environments are associated with social norms and values that are not supportive of recovery (e.g., the “convict code”), and these often become internalized when adapting to prison life. The resulting social identity persists even after incarceration ends and can strongly influence how the incarcerated person interacts with the external community, including the social groups they can engage with. In this way, the experience of incarceration can be understood as a direct assault on social and cultural recovery capital (Cloud & Granfield, 2008), meaning that recovery journeys may be more challenging for those with CLS exposure. Therefore, while recovery is a challenging process of change on its own, simultaneously desisting from crime may lead to greater obstacles in obtaining recovery capital.
Fortunately, a range of addiction recovery interventions can serve as pathways to increased recovery capital. For example, one study found that participating in a clinic that prioritized engagement and promoted patient-centered treatment improved recovery capital in a cohort of individuals within 1 year post-incarceration and reduced self-reported alcohol and drug use as well as crimes committed (Bormann et al., 2023). The authors stated that these improvements were not medication-related but rather an outcome of the support provided, which focused on enhancing recovery capital. Furthermore, in another study, living in recovery housing was associated with improvements in recovery capital, and intensive recovery support intervention resulted in even greater improvements for those who were deemed vulnerable because of low recovery capital upon admission to recovery housing (Belanger et al., 2024).
Dual Challenges of Being in Recovery and Desistance
Given the challenges of both recovery and desistance, individuals experiencing both simultaneously form a unique subgroup facing additional difficulties in their journeys toward improved well-being (Best et al., 2017; Van Roeyen et al., 2017). Both processes of change are linked to societal responses that can impede progress and daily life, such as intersecting stigmas (experienced and internalized) related to addiction and CLS involvement (Avery, 2019; Best et al., 2017; Maruna et al., 2013). For instance, a higher level of anticipated stigma during incarceration is associated with challenges to community reintegration post-release, including greater levels of social withdrawal (Moore et al., 2016; Moore & Tangney, 2017). The barriers to everyday life for individuals in recovery and desistance are diverse, including difficulties in securing housing and obtaining mortgages, limited stable employment prospects, and increased challenges in obtaining insurance (Henley, 2015; Neale et al., 2016). Importantly, these barriers may not operate independently but rather intersect, compounding exclusion from potential opportunities to develop personal, social, and community capital. This could influence the capabilities individuals have for progressing toward holistic well-being.
Living in Recovery Housing as a Pathway to Recovery and Desistance
Living in stable housing is a core component of initiating and maintaining recovery and desistance. Therefore, recovery houses (RH) serve as ideal accommodation for individuals in recovery, both with and without CLS involvement (Polcin, 2018; Reif et al., 2014). These services are typically provided as a form of continuing care following in-patient or residential treatment (or after release from prison) during the early stages of recovery, and they help support individuals to become independent in their daily lives (Reif et al., 2014). RHs play an important role in continuing care since a major issue with acute care interventions for substance use is their often short-lived impact on individuals who lack access to substance-free living and positive social environments (Polcin et al., 2016).
Among RH residents, higher overall levels of recovery capital have been associated with greater quality of life, recovery group participation, and perceived social support, full-time employment, and longer durations in an RH (Best et al., 2023; Cano et al., 2017; Härd et al., 2022). Conversely, recovery barriers, such as CLS involvement and unmet health and housing needs, have been associated with lower levels of overall recovery capital (Best et al., 2023; Härd et al., 2022). While these studies suggest that RHs provide suitable environments for supporting the development of recovery capital among individuals with and without CLS involvement, the existing literature is limited on whether recovery capital trajectories differ between RH residents with and without CLS exposure.
Study Aims
This study compared recovery capital trajectories between individuals with and without CLS exposure and examined the predictors of recovery capital development. The research aims were as follows: (a) to assess differences in personal, social, and community recovery capital, recovery barriers, and unmet needs at baseline among CLS clients compared with non-CLS clients among new admissions to RHs in Virginia, USA, (b) to assess the predictors and trajectory of the Overall Recovery Capital Score (ORCS) as measured by the REC-CAP, and (c) to assess the importance of CLS status in the observed changes. We hypothesized that those with CLS involvement would report lower levels of recovery capital and a higher number of barriers and unmet needs at baseline. Moreover, we expected a slower rate of growth in the ORCS among individuals involved with CLS.
Method
Setting and Participants
The study accessed data from 101 RHs within the Virginia Association of Recovery Residences (VARR) network, which has approximately 1,000 to 1,150 residents at any given time. The residences are predominantly single-gender housing for individuals recovering from substance use disorders. All residents, including those with a CLS background, can access recovery housing support through direct applications, or via family or friends, the jail or prison if incarcerated, a court order, or parole or probation boards. The residences offer differing approaches to recovery support, including varying medication policies, drug testing, behavioral rules, community service and recovery group attendance requirements, and services particularly tailored for groups such as pregnant or postpartum women or LGBTQIA+ populations (VARR, n.d.). All VARR-certified RHs are certified in accordance with the National Alliance for Recovery Residences (NARR, 2018) Standard 3.0. On average, a VARR RH accommodates nine residents, ranging from 3 to 21. VARR currently (i.e., in 2025) has 113 certified RHs, of which 85 are Level II and 24 are Level III. Level II RHs are run by residents with a recovering peer as an on-site manager, whereas Level III facilities offer on-site services and paid staff (Polcin, 2018). 1 Individuals with a history of CLS involvement may access VARR-certified residences in several ways. They can enter an RH directly after incarceration or with assistance from a Discharge Coordinator, Case Manager, or a Recovery Navigator. 2 Placement is the result of a joint decision between the recovering individual and RH characteristics such as location, age, and gender.
We report assessment data on 1,933 clients who accessed VARR-certified residences between February 2020 and August 2022. Everyone entering the RHs completed the REC-CAP as part of their stay at the residence unless they chose otherwise. Figure 1 presents detailed information on the number of individuals per assessment time. This research includes data only from those who chose to consent to use their data for research purposes. Ethical approval for this study was granted by Leeds Trinity University, UK.
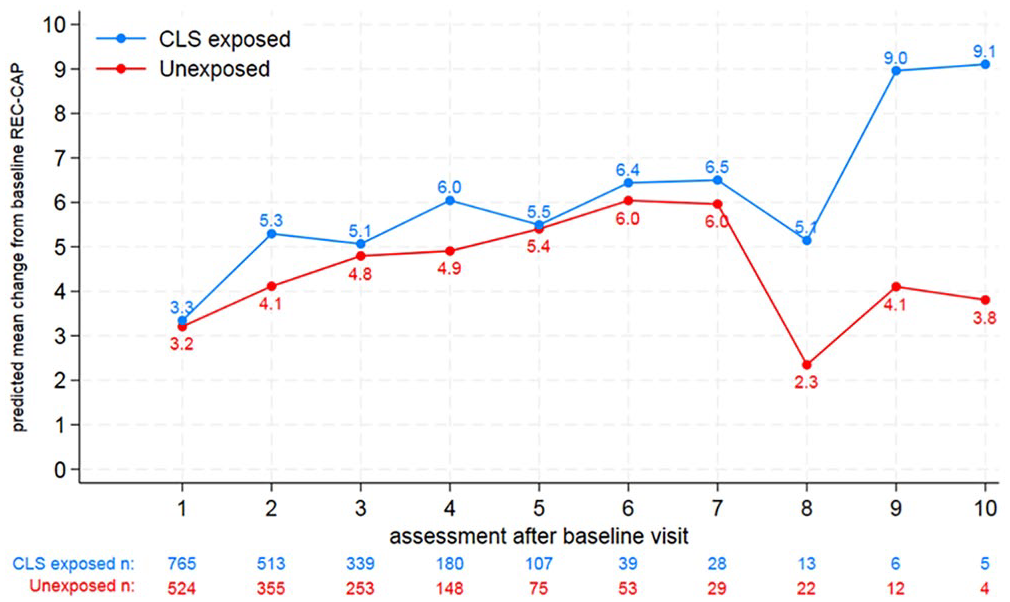
Predicted Mean Change From Baseline REC-CAP Score Comparing Recovery Residents From the CLS and Those Not From the CLS
Instrument and Procedure
The REC-CAP questionnaire (Cano et al., 2017) measures recovery capital, barriers, and unmet needs among those in recovery. It comprises validated questionnaires, including the Assessment of Recovery Capital (ARC, Groshkova et al., 2013a), the Recovery Group Participation Scale (RGPS, Groshkova et al., 2013b), the Commitment to Sobriety Scale (CSS, Kelly & Greene, 2014), and well-being measures and the Barriers to Treatment Scale from the Treatment Outcomes Profile (Delgadillo et al., 2013). The ARC (Groshkova et al., 2013a) consists of the Personal and Social Recovery Capital scales, with dichotomous yes/no questions yielding a total score ranging from 0 to 50. The RGPS (Groshkova et al., 2013b) has 14 dichotomous yes/no questions, resulting in a total score from 0 to 14. The CSS (Kelly & Greene, 2014) contains five questions on a 6-point Likert-type scale from 1 (strongly disagree) to 6 (strongly agree), yielding a total score from 5 to 30. The well-being measures include five questions regarding psychological health, physical health, quality of life, accommodation, and social network, each scored from 0 (poor) to 20 (good), resulting in a total score from 0 to 100. The barriers to recovery score ranges from 0 to 5, based on five dichotomous yes/no questions related to accommodation, non-prescribed substance use, current involvement in offending, recent risk-taking behaviors, and lack of meaningful activities (i.e., not being in work, education, or volunteering). Moreover, the REC-CAP assesses unmet needs for drug treatment, alcohol treatment, mental health services, housing support, primary health care, family relationships, and other services using dichotomous yes/no questions, resulting in a total score from 0 to 8. Demographic questions include gender identity (multiple answer options; however, our analysis focused on comparing outcomes for men and women, as these were the most prevalent responses in our sample), age, and ethnicity (Alaska Native, American Indian, Asian, Black or American African, Caucasian, Hispanic, Native Hawaiian or Other Pacific Islander, Other; however, our analysis focused on comparing outcomes for White vs. Non-White). The psychometric properties of the entire REC-CAP have not been assessed. In this study, the ORCS was calculated only for positive recovery capital (which includes well-being measures, personal, social, and community recovery capital, as well as a commitment to sobriety, with each scaled to contribute 20% of the total score), yielding a score that ranges between 0 and 100, with a higher score indicating more recovery capital.
The REC-CAP was designed to be completed electronically with the support of RH staff trained to administer the REC-CAP at baseline, at 45 days, 90 days, and then at 90-day intervals thereafter. The REC-CAPs are completed as part of routine recovery support service delivery at the RHs; therefore, this data was not primarily collected by researchers for research purposes. We do not have information on the specific number of individuals who chose not to complete the REC-CAP at baseline. However, the research team works in close collaboration with the VARR team, and there have been no reports of a cohort of individuals choosing not to complete the REC-CAP. Although the primary purpose of the REC-CAP is to guide and measure recovery progression at RHs, the structured completion pattern makes the REC-CAP data also ideal for research purposes. Due to the secondary data nature of this analysis, there was no pre-determined number of REC-CAP completions that residents included in this study were expected to complete.
Study Design and Analysis
A CLS-exposed person in recovery was defined as any individual who had answered “yes” to any of the following questions in the previous 90 days: (a) any involvement with the police (n = 388, 20.10%); (b) on probation (n = 941, 48.70%); (c) on parole (n = 48, 2.50%); (d) any other CLS involvement (n = 340, 17.60%). Individuals who were criminally active but not involved in the CLS were excluded from the analysis (i.e., answered “yes” for being involved in crime but not any of the other questions regarding justice involvement). Since an individual can be exposed to several CLS agencies at the point of assessment (e.g., involved with the police, on probation, on parole, or any other type of CLS exposure), it was determined that 1,158 people were CLS-exposed (59.90%) compared with 775 non-CLS exposed individuals (40.10%).
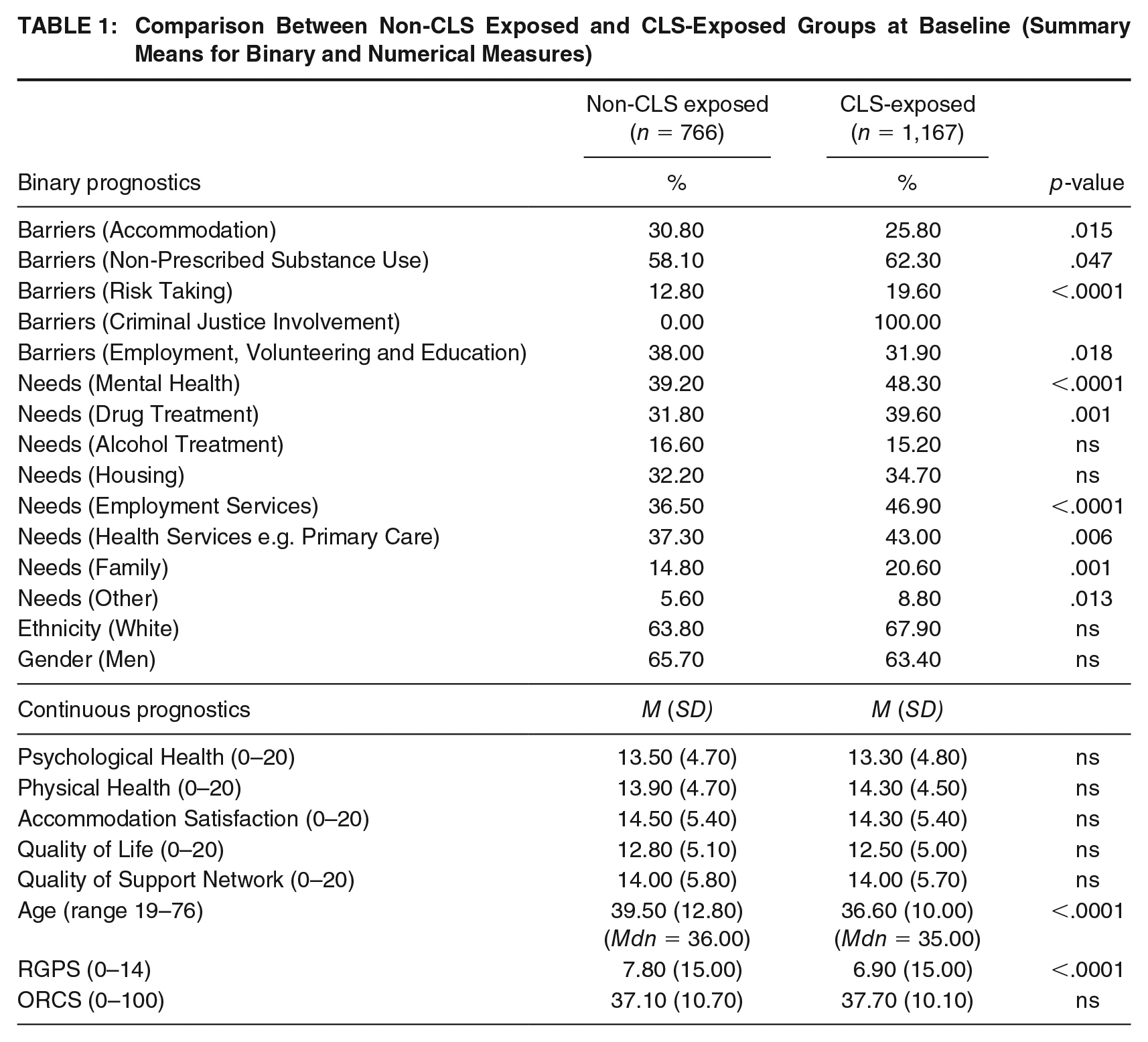
A quasi-experimental method was employed to derive a treatment effect by weighting the characteristics of individuals exposed to the CLS (CLS-exposed) to create a pseudo-population of individuals without exposure to the CLS (non-CLS exposed). The 25 potential measures are presented in Table 1, including means (formatted as a percentage) for 15 binary variables (five barriers, eight unmet needs, ethnicity, and gender). Numerical measures assessing perceptions of psychological and physical health, satisfaction with accommodation, quality of life, support networks, engagement with recovery groups (RGPS), and baseline ORCS revealed broadly similar results for clients in the CLS group. The exception was age; on average, clients exposed to CLS were 3 years younger than those not exposed.
Comparison Between Non-CLS Exposed and CLS-Exposed Groups at Baseline (Summary Means for Binary and Numerical Measures)
Analytical Approach
Standard regression methods for observational studies are known to yield biased results due to the lack of a random treatment allocation mechanism; therefore, a quasi-experimental model of repeated measures for the same person was deployed instead (Hernán et al., 2002; Hernán & Robins, 2020). Marginal structural modeling (MSM) is a weighted repeated measures approach that uses exposure (e.g., CLS or non-CLS) as a time-varying covariate. Stabilized weights control for any time-varying confounders by creating a counterfactual pseudo-population that balances both time-invariant and time-varying confounders. Longitudinal studies can become biased if people who drop out differ meaningfully from those who remain, primarily based on their offense history or other life events. MSM addresses this by applying censoring weights, ensuring that the analysis accounts for missing individuals. This creates adjusted samples for each resident type, removing biases using a weighting method (Kennedy et al., 2023; Seaman & Keogh, 2024). This enables causal inference comparisons using standard repeated measures models.
We derived stabilized inverse propensity weights for use in weighted structural marginal models (Hernán & Robins, 2020) aimed at predicting the probability of exposure (propensity scores), deploying a binary regression model on CLS-exposed/non-CLS exposed groups as an outcome with two different sets of prognostics. The first set comprised time-independent variables (age, ethnicity, gender, assessment, and baseline values for all time-dependent variables). Next, the ratio between the two propensity scores was computed to derive the stabilized inverse propensity score. The following step involved fitting a marginal model for repeated measures by modeling the mean change from the baseline ORCS. This is a Generalized Estimating Equation model (GEE) that focuses on the fixed effects of time, exposure, and their interactions. GEE models the average response to draw inferences about the study population while accounting for within-subject correlations. A final GEE model included the stabilized weights in the modeling process, creating a structural marginal model. Our goal was to model changes in the ORCS over time from baseline to evaluate the impact of each assessment point. These points were categorized into sets for CLS-exposed and non-CLS exposed groups, recognizing that an individual’s exposure to CLS may vary at different assessment points. In addition, we aimed to assess how group exposure modified the effects at each assessment. All computations and modeling were conducted in SAS On Demand for Academics.
Results
The CLS-exposed group at baseline had significantly higher unmet needs (see Table 1 for specific p-values) for mental health, drug treatment, employment, health services, family-based services, and other services. Barriers to recovery were significantly higher in the CLS-exposed group for substance use and risk behaviors but significantly lower for accommodation and lack of meaningful activities (i.e., employment, volunteering, and education). The CLS group was also more likely to be White (67.90% compared with 63.80% of the non-CLS exposed group) and less likely to be women (63.40% compared with 65.70% of the non-CLS exposed group), although these differences were not statistically significant. In comparison, the non-CLS exposed group was significantly more likely to be older (mean age 39.50) than the CLS-exposed group (mean age 36.60).
To derive the propensity score for the numerator of the stabilized weights to ensure counterfactuals across all assessment points, we included 23 time-invariant measures in a binary model for intervention selection (e.g., whether CLS-exposed or non-CLS exposed), such as age, gender (men vs. women), ethnicity (White vs. Non-White), and 20 indicators of time-varying variables measured at baseline (psychological health, physical health, quality of life, accommodation, support network, RGPS, ORCS, five barriers, and eight unmet needs), along with the categorical effect of the assessment time, resulting in a total of 24 prognostics (Faries & Kadziola, 2010).
In creating the stabilized weights to assess change over time, we found that the mean ORCS was statistically different across the multiple assessments (p < .0001) when averaged over the group. The change in ORCS was not dependent on exposure to the CLS, nor was the group effect statistically different when averaged across assessments. However, being older (p = .04) and being man (p = .01) were factors related to changes in the ORCS from baseline, regardless of exposure to the CLS. Consequently, we adjusted for the effects of baseline characteristics, including the ORCS, age, gender (men), and ethnicity (White). The resulting GEE model predicted the mean change in ORCS from baseline, as shown in Figure 1. The changes in average ORCS from baseline are higher for the CLS-exposed group at all assessment points and continue to increase in subsequent assessments. The increase in the ORCS is broadly similar across groups until assessment seven (no statistically significant differences between CLS-exposed and non-CLS exposed groups). There is a drop in the rate of increase in ORCS at assessment eight. Thereafter, the mean changes are notably higher for the CLS-exposed group.
Discussion
This study compared the progress in recovery capital between individuals with and without CLS involvement living in recovery housing across Virginia, USA, and sought to identify predictors of recovery capital change. The findings partially supported the hypotheses. Although both groups had similar recovery capital profiles upon entering recovery housing with regard to mental and physical health, quality of life, and quality of support networks, individuals with CLS involvement reported more barriers related to substance use and injection-related risk-taking, as well as more unmet needs concerning mental health, drug treatment, employment, volunteering and education, family, health (e.g., primary healthcare services) and other services. The key finding of this study showed that, despite these obstacles among individuals with CLS involvement and adjusting for these barriers using quasi-experimental methodologies to create balanced groups, there were no statistically significant differences in the mean change in ORCS between the two groups at baseline or over time. Although further research is needed, this positive finding may suggests that, for residents with CLS involvement, the support provided by the CLS and RHs may lead to improvements in recovery-supportive factors that are also associated with desistance (such as meaningful activities and housing stability).
The second key finding is the broad, continuous increase in recovery capital over time. Our findings align with previous research showing that recovery capital tends to grow among RH residents over time (Belanger et al., 2024; Best et al., 2023; Bormann et al., 2023; Cano et al., 2017; Härd et al., 2022; Lynch et al., 2021). Our results align with findings from Bormann et al. (2023) and Lynch and colleagues (2021), who found that recovery capital increased among individuals with CLS involvement when they received targeted recovery supports, including those who were post-incarceration (Bormann et al., 2023) or on probation or parole (Lynch et al., 2021). Alongside improved recovery capital, these studies reported decreased engagement in criminal activity (Bormann et al., 2023) and illegal drug use (Lynch et al., 2021). The relationship between recovery capital and illegal behavioral outcomes was not analyzed in this current study; however, it may be possible that while RHs can provide different levels of drug recovery services or linkages to a range of specialist services, the overall improvement in recovery capital might function as a protective factor against resuming criminal activity. It might also support desistance from illegal activities through strength-based factors such as positive social networks, meaningful activities, and engagement in mutual aid groups. Although further research is needed to ascertain the exact mechanisms through which recovery housing may play a role in improving recovery capital among those with and without CLS involvement, aspects such as a structured sober living environment, accountability, enforcement of abstinence-focused rules, social support, and shared recovery goals have been suggested as mechanisms by which staying in recovery homes may enhance recovery outcomes (DeGuzman et al., 2019; Mericle et al., 2022), along with mentoring and one-to-one support from house managers and recovery peer specialists. Similarly, these factors could also play a role in improving desistance outcomes. Overall, the importance of accessing and remaining in RHs is crucial in the context of CLS, especially since a significant proportion of incarcerated individuals who could benefit from drug treatment do not receive it in prison, a factor linked to high levels of re-incarceration (Chandler et al., 2009).
Furthermore, although the ORCS trajectories of those with and without CLS involvement did not significantly differ, several key differences were reported by the groups at baseline. The CLS-involved group reported greater recovery barriers, including higher levels of unmet needs in mental health, drug treatment, employment, health services, family relationship services, and other services, as well as greater substance use, and risky injecting drug practices. This suggests that, despite similar ORCS trajectories, CLS involvement is associated with distinct barriers at the onset of recovery housing. In addition, CLS involvement may present complications such as legal and financial obligations, including probation or parole requirements, which can hinder reintegration into society post-release (Harding et al., 2022). These obligations, such as monetary sanctions, supervision fees, or employment and housing restrictions, may affect recovery by limiting access to resources and adding stressors for CLS-involved individuals.
An analysis of retention outcomes among recovery house residents, both with and without CLS involvement, showed that CLS-exposed individuals were more likely to complete their program than those without CLS involvement (Sondhi et al., 2024). However, after 6 months, CLS involvement was associated with a higher likelihood of leaving an RH due to a negative reason, such as disciplinary release. Addressing these baseline challenges around unmet needs and recovery barriers reported by CLS-exposed individuals through targeted resources and support is crucial and could help encourage their continued stay in RHs and avoid early discharges.
Research on RHs has that the development of recovery capital is influenced by gender (Best et al., 2023; Härd et al., 2022). Our findings align with this, showing that the average growth in the ORCS was higher for men than for women, regardless of CLS exposure. Some underlying reasons for these findings may be linked to challenges commonly faced by women in recovery, such as a higher prevalence of mental health difficulties and a corresponding lower quality of life compared with men (Grella & Lovinger, 2012; Tuchman, 2010). Women also tend to report significant histories of traumatic experiences, often more than men do regarding various forms of abuse such as neglect and sexual abuse (Bodkin et al., 2019; Stanton et al., 2016). Moreover, women’s recovery and desistance journeys are affected by systemic inequalities, including societal and cultural expectations that disproportionately assign caregiving and child-related responsibilities to them (Stanton et al., 2016; Swavola et al., 2016). These challenges can make recovery and desistance journeys more difficult for women and are particularly relevant for those involved with CLS, as traditional CLS settings often fail to provide adequate support to address the acute needs of women in this group (Arditti & Few, 2008; Wright et al., 2012). The value of gender-responsive and intersectional approaches must be considered to create equitable pathways to recovery and desistance.
In addition, older individuals experienced greater increases in the ORCS. This finding is important as it indicates that age may play a role in recovery capital development that may also be relevant for desistance. According to the life course model of desistance (Sampson & Laub, 2003), older individuals may be more capable of distancing themselves from offending behavior and substance use due to their life transitions and experiences, which may have facilitated the accumulation of recovery capital and reductions of recovery barriers in our sample. Overall, although more research is needed to understand how age may impact the development of recovery capital across populations, our findings suggest that RHs may wish to consider responses to support younger residents with CLS involvement in helping them develop recovery capital, and this should be explored in future research specifically focused on age-related trajectories for co-occurring desistance and recovery.
Limitations and Future Directions
The use of a novel quasi-experimental methodology that creates pseudo populations by balancing the characteristics of CLS-exposed and non-CLS-exposed individuals across all assessment points over time is a key strength in this study. However, several limitations should also be considered. Our definition of CLS involvement encompassed various types of involvement, as we relied on the phrasing within REC-CAP that asked about “any involvement” rather than a specific question on arrests. This approach aimed to avoid stigmatizing study participants; however, the resulting questions could be interpreted in multiple ways by respondents. Future studies could explore recovery capital trajectories for each type of CLS exposure separately. The literature suggests that CLS exposure of different types (e.g., arrest, violent conviction, non-violent conviction) and at different magnitudes (e.g., never incarcerated, incarcerated once, incarcerated multiple times) may have differing levels of impact on well-being, including physical and mental health and thriving in life (Fernandes, 2020; Sundaresh et al., 2020). For example, non-violent convictions have been associated with poorer physical and mental health, whereas prison exposure has been linked to improved physical health but poorer mental health (Fernandes, 2020). Moreover, individuals who were stopped and searched by the police reported lower levels of thriving compared with those who were stopped without searching, similar to those incarcerated multiple times compared with those incarcerated only once (Sundaresh et al., 2020). Furthermore, recent research by Bormann et al. (2023) demonstrated that changes in recovery capital were associated with reduced criminal activity among individuals with a recent history of incarceration, and future research should aim to analyze CLS-related outcomes such as recidivism and re-incarceration in the context of RH residents. Since our sample was based in Virginia, USA, further research is warranted across areas with different CLS structures and public health systems. One limitation of our study is the opt-in model used, where participants had to formally consent to the use of their data for research purposes; therefore, due to the nature of our research, we do not know how many people were missing assessments. Moreover, we could not assess how those who consented to their data for research may have differed from those who did not, but we hope to investigate this aspect in future research. We acknowledge that repeated REC-CAP completions may raise the possibility of response fatigue. However, the tool was designed to be completed collaboratively with a staff member trained to administer the questionnaire, and it is a part of the standard recovery service delivery at the RHs, helping recovering individuals track and plan their recovery progress. This approach may enhance engagement and mitigate the potential burden of repeated assessments. That said, there is a possibility that demand characteristics may influence the REC-CAP completion process. Although we do not have direct evidence of such bias and have little control over it, this is recognized as a limitation of the study. Finally, future research should establish the practical significance of the predictors of ORCS change.
Conclusion
These findings provide evidence for the development of recovery capital among RH residents. Importantly, the results demonstrated that CLS involvement does not impede the accrual of recovery capital during time spent in RH. Recovery capital increased over time, highlighting the importance of supporting individuals with CLS involvement to encourage their stay in RHs and particularly to overcome recovery barriers and unmet needs, which were more frequently reported by CLS-involved individuals at baseline. Although further research is needed to better understand the development of recovery capital among individuals from various backgrounds and stages of life, the current findings suggest that younger individuals and those identifying as women may benefit from additional support in developing recovery capital through their experience in an RH. Overall, RHs may provide an effective pathway to recovery capital improvement among individuals with CLS involvement. Nevertheless, the potential impact of RHs on reducing illegal activities remains to be explored. We propose that future research should expand to assess the effects of RHs on illegal activities, thus advancing the field’s understanding of the impact of recovery housing on desistance.
Footnotes
Authors’ Note:
The authors declare no conflict of interest. Emily A. Hennessy is supported by a grant from the NIAAA [K01 AA028536]. This funding source had no role in the decision to submit the manuscript. The authors of this article would like to thank the anonymous reviewers for their comments on this article.
Author Contributions
Adela Bunaciu (Writing—Original Draft, Writing—Review & Editing), Arun Sondhi (Conceptualization, Methodology, Software, Validation, Formal Analysis, Resources, Writing—Original Draft, Writing—Review & Editing, Visualization), David Best (Conceptualization, Writing—Original Draft, Writing—Review & Editing, Supervision, Funding Acquisition), Emily A. Hennessy (Writing—Original Draft, Writing—Review & Editing), Jessica Best (Conceptualization, Data Curation, Project Administration), Matthew J. Belanger (Writing—Original Draft, Writing—Review & Editing), Alessandro Leidi (Methodology, Software, Formal Analysis, Resources, Writing—Original Draft, Writing—Review & Editing, Visualization), Anthony Grimes (Investigation), Matthew Conner (Investigation), Robert De Triquet (Investigation), William White (Writing—Original Draft, Writing—Review & Editing).