
Abstract
Hearing loss is highly prevalent in dementia; however, people with dementia are less likely to use hearing aids consistently than people with intact cognition are. This qualitative study is the first of its kind to explore factors that influence hearing aid use from the perspective of community-living people with mild to moderate dementia and their care partners. Eleven UK-based dyads from the European SENSE-Cog Randomized Controlled Trial of a sensory intervention for people with dementia completed semi-structured interviews based on the Theoretical Domains Framework (TDF). Our findings suggest that the TDF domains environmental context and resources, behavioral regulation, reinforcement, and social influences are of greatest relevance to hearing aid use in dementia. Within these domains, we identified a range of factors that may influence the target behavior of hearing aid use. The findings suggest that adoption of multifaceted, flexible intervention approaches may support hearing aid use in dementia.
This study extends understanding about enablers and barriers to hearing aid use that people with dementia experience. Enablers include establishing routines for wear and care, quality hearing aids, experiential benefits, and responsive support. Barriers include difficulty with hearing aids and their maintenance, especially if support to troubleshoot is not timely.
Our findings suggest that interventions for supporting hearing aid use in dementia should include training, environmental restructuring, enablement, incentivization, and education. Our findings suggest that a need for enhanced service provision for people with dementia and concurrent sensory loss exists.What this paper adds
Applications of study findings
Introduction
Hearing loss is highly prevalent among people with dementia, with rates of 60%–94% being reported (Gold et al., 1996; Nirmalasari et al., 2017). Untreated hearing loss can lead to adverse consequences including increased social isolation, loneliness, and dependence upon others (Guthrie et al., 2018). Hearing aids are the recommended intervention for hearing loss (National Institute for Health and Care Excellence, 2019), including for people living with dementia (Ray et al., 2019). Many people living with dementia are able to use hearing aids (Dawes et al., 2022) with benefits including increased quality of life (Atef et al., 2023), and improved cognitive function (Bisogno et al., 2021). However, people with dementia are less likely to use hearing aids consistently than people with intact cognition are (Naylor et al., 2022).
A recent systematic review of enablers and barriers to hearing aid use in dementia identified a range of factors that influence use (Hooper et al., 2022). These included the person’s hearing aid handling skills, experiential consequences, aspects related to fit and comfort, social influences, and the demands of the listening environment. While this review goes some way to identifying influencing factors, none of the included studies addressed factors affecting hearing aid use as their primary research question. This may have restricted the range of influencing factors that were identified in the review and is a limitation of the existing evidence-base. Other factors that may influence hearing aid use could include challenges related to the impact of dementia, such as cognitive and functional difficulties (Lupsakko et al., 2005) and socio-economic barriers to accessing hearing care services and hearing aids (Willink et al., 2019).
The objective of the present study was to use a theory-informed approach, based on the Theoretical Domains Framework (TDF) (Cane et al., 2012), to gain insight into factors that influence hearing aid use from the perspective of people with mild to moderate dementia and their care partners. This is the first primary research study to adopt a theory-informed approach to investigate this with this population. The TDF is a comprehensive framework that integrates multiple theories of behavior change (Cane et al., 2012). Comprised of 14 domains of behavioral influence, the TDF links directly into the Behavior Change Wheel (Michie et al., 2014) and facilitates a “behavioral diagnosis” of factors that influence the target behavior. Michie and colleagues (2014) propose that this forms a key first step in the process of developing targeted, testable behavior change interventions. This is relevant to the present study because the current evidence base is insufficient to understand factors that influence the behavior of hearing aid use in dementia (Hooper et al., 2022). There is therefore a need for research to develop this understanding, prior to designing interventions that aim to address these influences to optimize hearing aid use in this population.
Methods
Sample
We enrolled a convenience sample of participants from the intervention arm of the European SENSE-Cog Randomized Controlled Trial, which evaluated the impact of an individualized sensory intervention for people with dementia on quality-of-life outcomes (Regan et al., 2019). To be eligible for inclusion in the parent study, participants had to be aged 60 or over, residing in the community, have a previously established clinical diagnosis of Alzheimer’s, Vascular or mixed dementia, and have age-acquired hearing and/or vision loss. Dementia needed to be at the mild-moderate stage, quantified by a Montreal Cognitive Assessment (MoCA) score of at least 10 (Nasreddine et al., 2005). Hearing loss was defined by hearing worse than 35 dB HL at 1000 Hz and above in the better ear, using the portable Siemens HearCheckTM device. Existing ownership of hearing aids did not preclude participation. Further detail is described elsewhere (Regan et al., 2019).
In the United Kingdom, recruitment to the parent study took place through the National Health Service and the Join Dementia Research registry (https://www.joindementiaresearch.nihr.ac.uk) from April 2018 to April 2021. Participants were recruited in dyads, comprising the person with dementia (PwD) and a care partner (CP). Participants were randomized to receive either a sensory intervention or care as usual. For participants with hearing loss, the sensory intervention comprised correction of their hearing through Starkey Muse i2400 behind-the-ear hearing aids and a multi-component program of home-based support delivered by a Sensory Support Therapist (SST). Although the intervention included hearing aid adherence support and training, no minimum requirement of hearing aid use was specified.
For the present study, we offered an invitation to participate in interviews to sequential UK-based participants with hearing loss and dementia in the intervention arm of the SENSE-Cog trial between the 18-week (intervention-end) and 36-week (trial-end) visits. All participants had provided written informed consent for inclusion at trial enrollment. Taking a process consent approach (Dewing, 2007), verbal consent for inclusion in the interviews was re-confirmed by the SST at the conclusion of their sensory intervention.
Interview Procedure
Qualitative Interview Schema—TDF Domains and Definitions (Cane et al., 2012) With Example Questions and Responses.
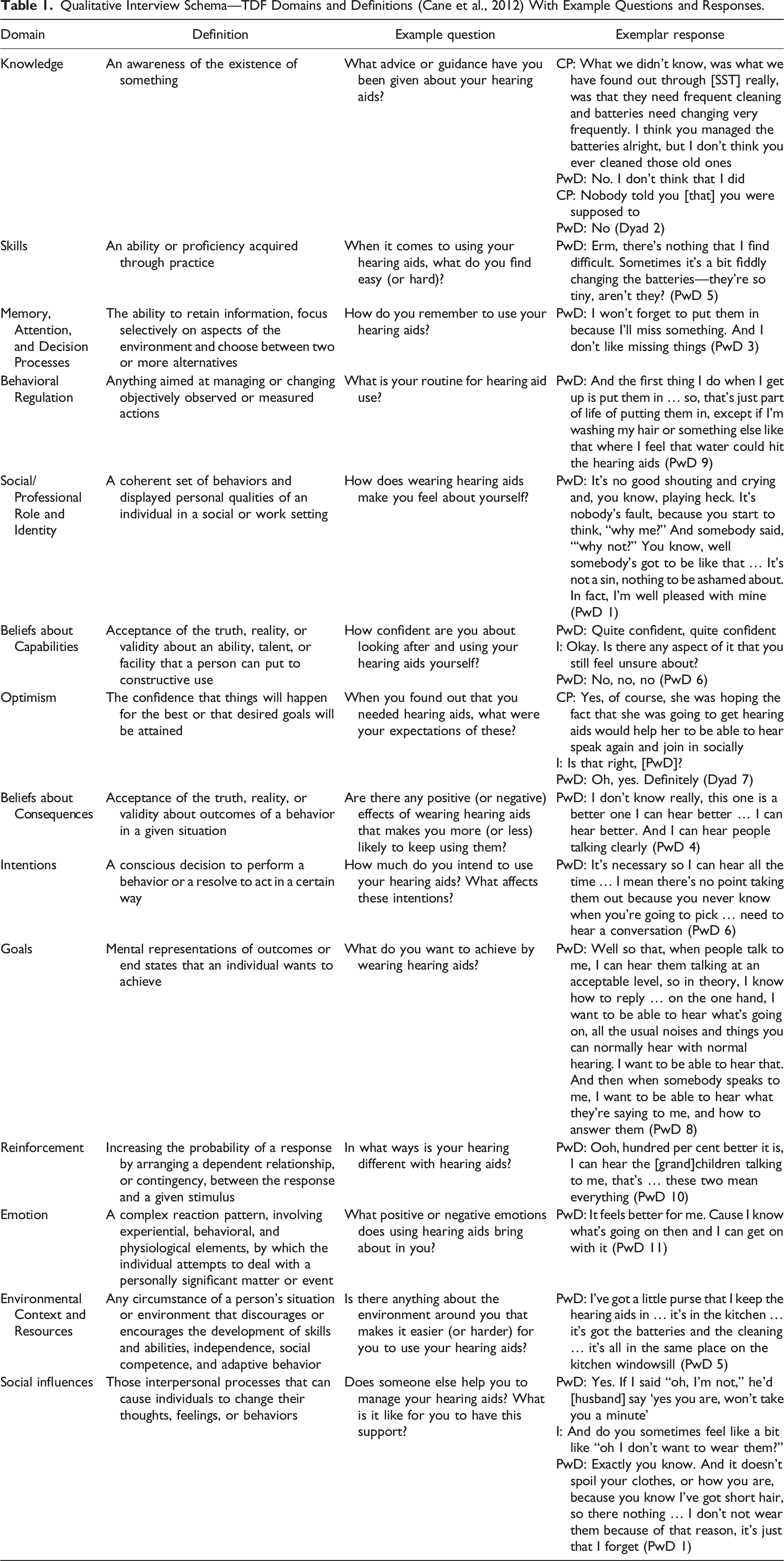
In qualitative research, the credibility of the report rests on the voices of the participants being revealed (Denzin & Lincoln, 2018). When interviewing people who are living with dementia, this can present challenges because responses may be short or difficult to interpret due to verbal communication difficulties. We therefore adopted guidance for interviewing people living with dementia (Murphy et al., 2015) alongside additional consideration about managing the sensory needs of this particular participant group.
We conducted the interviews with the participating dyad together so that the person with dementia was supported to recall their personal experiences, facilitating triangulation of data within the interview and enhancing credibility of the data (Knudsen et al., 2012). Adopting a dyadic approach to interviews in dementia research is not uncommon (Samsi & Manthorpe, 2020). As the purpose of the present study was to evaluate enablers and barriers to hearing aid use in dementia, rather than to explore relational aspects of dyadic hearing aid management, the role of the care partner within the interview was predominantly as a supporting and confirmatory respondent. We therefore directed questions to the person with dementia first before inviting their care partner to share their experiences. We endeavored to ensure that the participant with dementia had heard and understood the questions through repeating, rephrasing, and inviting the care partner to reframe questions where necessary.
The first author undertook the interviews. She is an occupational therapist and postgraduate researcher with experience of dementia and in-depth knowledge of the parent trial. The remaining authors are from psychology, psychiatry, and audiology backgrounds, with a range of expertise including behavior change theory.
The authors had not met with any of the participants prior to the interviews. Each participant was interviewed once between March 2020 and September 2021. Interviews were conducted face-to-face (n = 6) or remotely, via telephone (n = 2) or video conferencing (n = 3), according to national COVID guidelines at the time of the interviews. Mean interview duration was 61 minutes (range 26–89 minutes).
Analysis
Interviews were audio-recorded, transcribed verbatim, and anonymized. Field notes were made following each interview. The account from each dyad was considered a distinct unit and the data were analyzed accordingly. Informed by guidance for conducting qualitative TDF-based research (Atkins et al., 2017), we approached the data analysis in two phases. Firstly, we used the TDF as a framework for deductive content analysis. For this, the first author and another researcher independently coded the transcripts of three interviews into TDF domains. The percentage agreement between the two coders was 84%, which was above the 60% threshold of acceptability outlined by Atkins et al. (2017). The first author then coded the remaining interviews independently. In the second phase, we completed an inductive analysis of the mapped data to generate themes for responses with similar underlying ideas that related to the target behavior of hearing aid use. Throughout this process, an expert in the TDF provided input when necessary. We did not return transcripts to participants for comment or feedback. However, we sent a summary of the findings to the participants following completion of the analysis.
Results
Participant Characteristics (Person With Dementia and Care Partner).
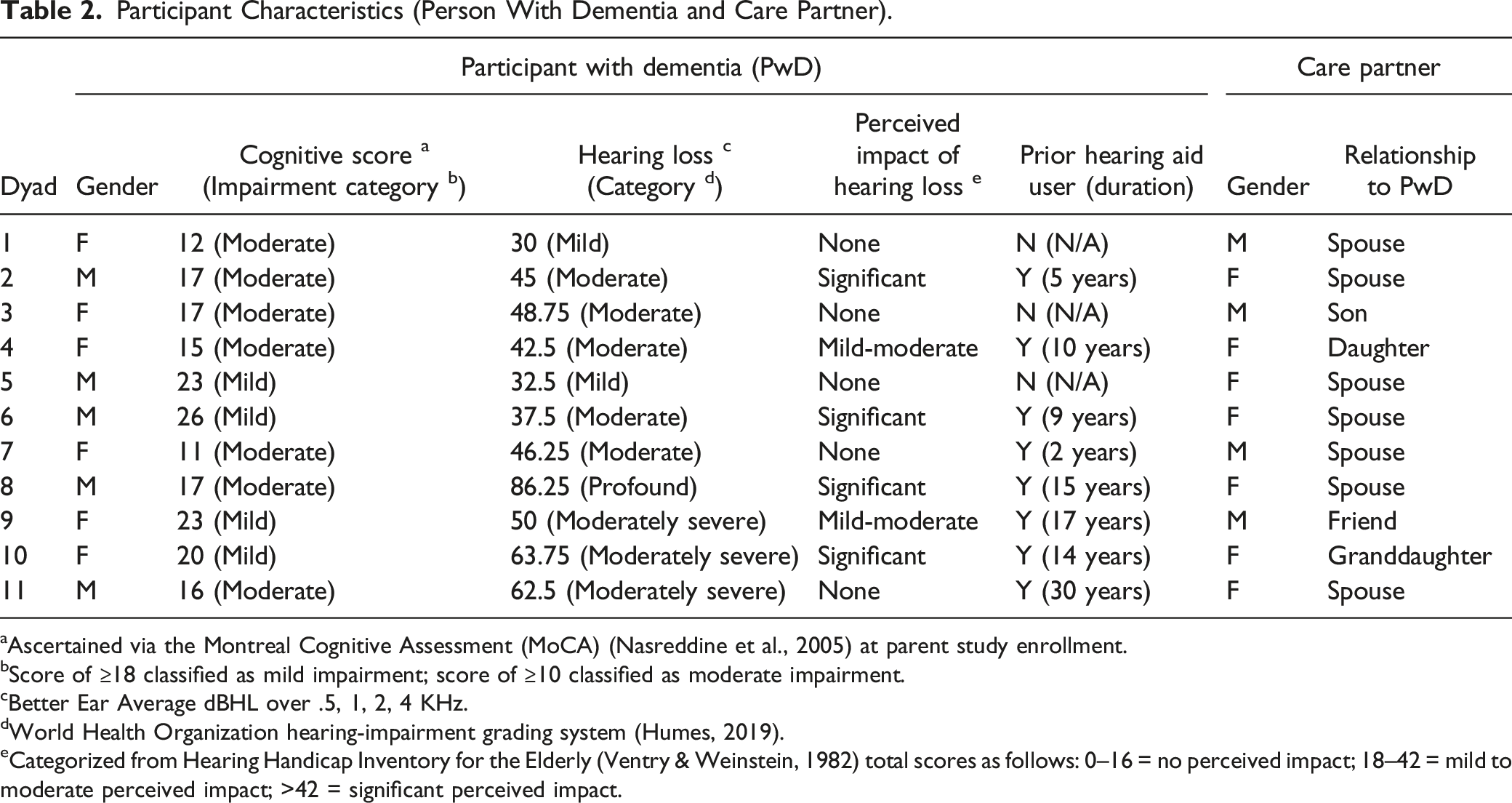
aAscertained via the Montreal Cognitive Assessment (MoCA) (Nasreddine et al., 2005) at parent study enrollment.
bScore of ≥18 classified as mild impairment; score of ≥10 classified as moderate impairment.
cBetter Ear Average dBHL over .5, 1, 2, 4 KHz.
dWorld Health Organization hearing-impairment grading system (Humes, 2019).
eCategorized from Hearing Handicap Inventory for the Elderly (Ventry & Weinstein, 1982) total scores as follows: 0–16 = no perceived impact; 18–42 = mild to moderate perceived impact; >42 = significant perceived impact.
Data mapped into all the TDF domains. The domains that featured most prominently in the data were “environmental context and resources,” “behavioral regulation,” “reinforcement,” and “social influences.” The themes that we identified within these domains are presented in Figure 1. Enablers and barriers to hearing aid use in people living with dementia.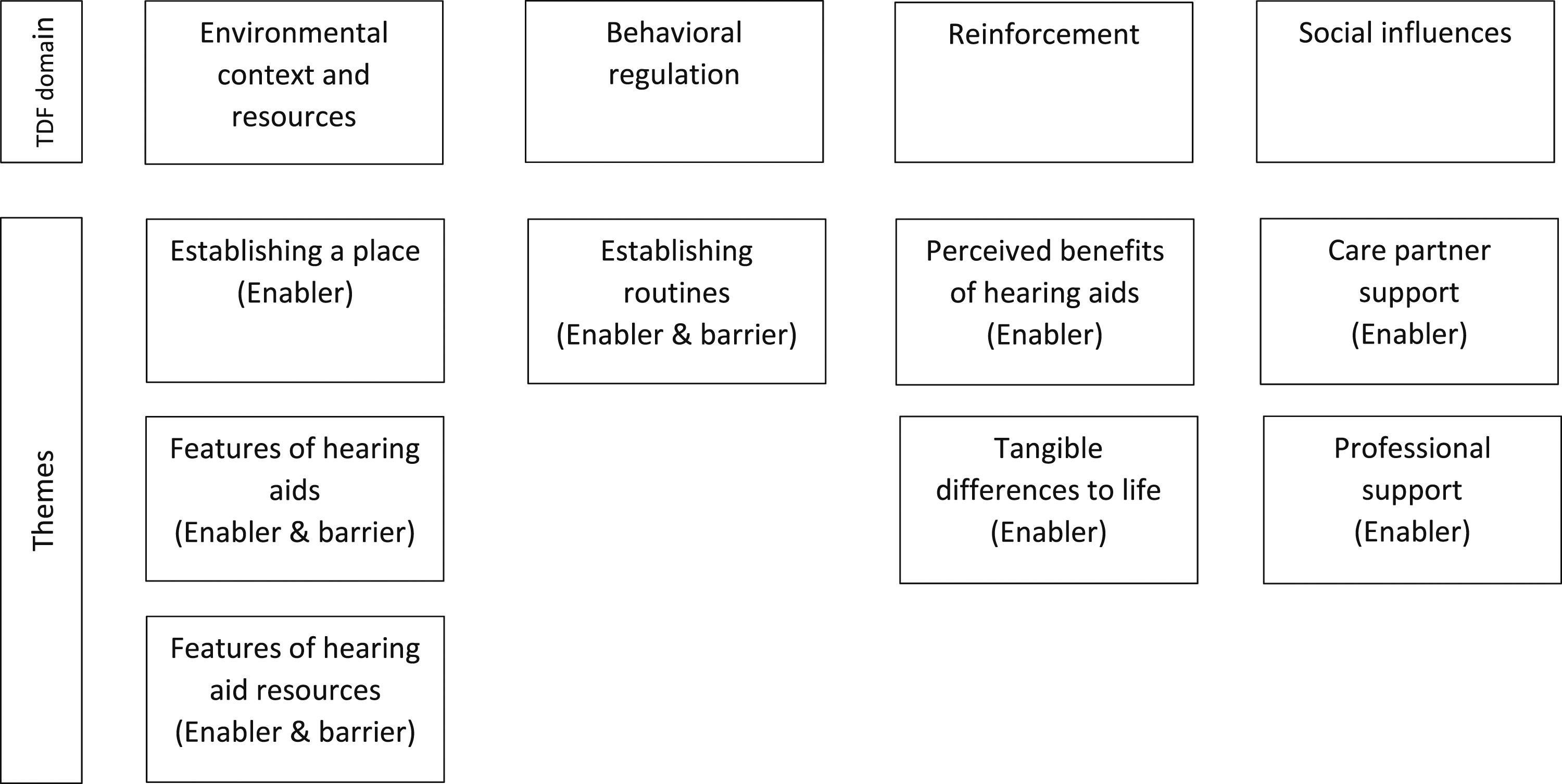
Domain 1: Environmental Context and Resources
Three themes were generated in the domain environmental context and resources, representing both enablers and barriers to hearing aid use.
Establishing a Place (Enabler)
Participants described the benefit of establishing a set place to keep their hearing aids and to care for them. This helped them to keep track of their hearing aids and the resources that they needed to keep them in working order. I have them in a little box … the hearing aid case, batteries, cleaning (PwD 9)
Although participants predominantly described the establishment of a place for storing hearing aids as a successful strategy, some identified occasional difficulties with misplacement. The majority of the time she puts them in the box, although sometimes we'll have to go searching the next day for them (CP 4)
Typically, participants reported that routinely using a solid surface, such as a specific table, during maintenance tasks such as cleaning the aids was beneficial. They also described the benefit of optimizing the environmental conditions during these tasks, including ensuring that lighting was adequate or using colored card to enhance contrast. When [the SST] was here, she gave us a couple of cards … You put the card on the table, and you put your hearing aid on top of the card so you can distinguish where the hearing aid is from everything else (CP 7)
Features of Hearing Aids (Enabler and Barrier)
This theme relates to visual, auditory, or physical features of the hearing aids. These represented both enablers and barriers to their use.
Participants used cues from the hearing aids themselves to help keep them in working order and use them effectively. Visual cues related to colored markings on the aids helped the participants to distinguish between their hearing aids. Auditory cues related to recognizing when the batteries needed to be changed or checking that the hearing aids were working. You check they’re working when you just tap them a bit … just tap it like that and a bit of a song comes on. So, I thought, oh entertainment here! (PwD 1)
Participants who were established hearing aid users spoke of differences between hearing aids. The quality of the sound, auditory comfort related to less whistling, and simplicity of use seemed to be of importance, and in some cases influenced hearing aid use. Of these features, the quality of sound was identified as being the most important aspect by some participants. The other hearing aids were simple because you didn’t have to clean them as much as these … I prefer these now ‘cause they’re better, well, they’re not only a better quality, you’re getting a better sound … You can put up with [fiddly bits] because you’re getting a better-quality sound (PwD 11)
Some participants found certain features of their hearing aids to be suboptimal, however. This related to aspects of size, fit, or volume (reported by some participants with more severe hearing loss). This led to frustration in a few, affected use in others, and sometimes led to increased dependence upon support. The content of this theme was predominantly generated from established hearing aid users. On the one hand, the bigger ones were easier for her to handle … and she used to clean the others, pull them apart and clean them herself whereas these she can't (CP 4)
Features of Hearing aid Resources (Enabler and Barrier)
Participants described ways in which having access to maintenance resources, including batteries and cleaning tools, helped them to keep their hearing aids in working order. However, some participants reported that aspects of handling these resources were difficult for them. For example, removing the labels from batteries and managing the size of batteries was problematic for some, leading to increased dependence on support or provoking feelings of frustration. You know, I get the batteries and they have a little stick-on label on them. I find it difficult enough first of all trying to pick it up. They are so small. And then getting the label off, the label doesn’t come off easily, you know, so that can be a bit of a problem (PwD 2)
As these relate to the nature of the resources themselves, such as size or packaging, we mapped these here rather than to the skills domain of the TDF.
Domain 2: Behavioral Regulation
One theme was generated within this domain, representing an enabling factor for hearing aid use.
Establishing Routines (Enabler)
Participants described how the routines that they had established for the care and wear of hearing aids supported their use. In relation to hearing aid care, they described their routines for changing batteries and cleaning their aids. Most participants changed both batteries at the same time, in response either to an auditory cue or on a set day of the week. In the latter case, the auditory cue was unnecessary due to the routine that had been established. If participants had a set day for changing their batteries, they generally combined this with other hearing aid maintenance tasks. I clean them on a Sunday, once a week … usually my batteries run out on a Sunday, so while I'm changing my batteries, I usually get all the cleaning stuff and clean them at the same time, so it saves me a lot of hassle. (PwD 11)
For some of the participants, including a few established hearing aid users, the development of these routines arose from the sensory intervention that they had received. For others, it was well established and automatic. Most of the established hearing aid users did not feel that the onset of dementia had affected their hearing aid care routines. Some, however, reflected that they were more intentional about certain aspects of their routines now. When I take them off at night, I put them in very … carefully, so it doesn’t turn round, and I bring it out very carefully. So, they're formed right for the correct ear, you see? (PwD 6)
In relation to hearing aid wear, participants had predominantly established routines of wearing their hearing aids from morning until evening. They described this as being part of their daily routines, and typically linked with other self-care routines. It’s part and parcel of getting dressed … Give them a polish, get them in, give them a – well, when they come out, they get a wipe, but they still get another one when they’re going back in (PwD 3)
Domain 3: Reinforcement
Two themes were generated in the domain reinforcement. These both described enablers for hearing aid use.
Perceived benefits of hearing aids (enabler)
Participants reported finding hearing aids to be beneficial. The language that they used in relation to this ranged from expressing that the positives outweighed the negatives to using emotive language that indicated they find them to be essential. If I took them out, I’d be dead without it … They’re the best thing that ever happened to me, you know (PwD 10)
The sentiment that life was better with hearing aids was the case even for participants who had expressed dissatisfaction with aspects of their aids. It was evident that this was a motivating factor for these participants to persevere with hearing aid use. I mean, they’re a long way better than nothing really (PwD 8)
Tangible differences to life (enabler)
Participants relayed the way hearing aids made a tangible difference within many aspects of their life, including their ability to engage in leisure activities such as watching the television, or feeling more connected to the external environment such as increased traffic awareness or hearing the birds singing. I can hear the birds singing outside, so that’s the main thing … and hear the cat when he cries at the door (PwD 4)
The most frequently reported difference related to connection with other people. Participants with dementia and their care partners spoke of the way in which they not only found communication to be easier with hearing aids, but also of increased participation and confidence as an outcome of hearing aid use. Since I’ve got these, they’ve been marvellous and I can have a proper conversation, you know? [Before] I was saying ‘yes’ when I should have said ‘no’ and different things … [Now] I don’t hold myself back … when I used to think ‘I’ll say this and say that’, well I thought, ‘well it’s not important, I’ll not bother saying’. But now I say everything to ‘em (PwD 10)
Some of the participants with dementia indicated that when hearing is clearer, and communication is less effortful, that it supported their cognition. They portrayed this as a motivating factor for using hearing aids. Hearing is important, then you can hear - formulate it. But if you're not getting a good hearing then it will affect your memory even more because you can't put the sentence together. When I can hear clearly, like now, I can understand what people are saying better (PwD 6)
Domain 4: Social influences
Two themes were generated in the domain social influences, comprising enablers and barriers to hearing aid use.
Care Partner Support (Enabler)
Most of the care partners within the study reported ways in which they supported hearing aid use. This ranged from offering light-touch verbal prompting to providing full assistance with donning the aids and attending to maintenance tasks such as changing batteries and cleaning the hearing aid tubing. Sometimes, maybe he’s not pushed the tube far enough in his ear, so in that case it’s not really working, is it? So, I will say ‘you’ve not pushed that far enough down’, so he will then sort of fiddle and push it down (CP 5)
There were three participants that were fully reliant upon assistance with donning their hearing aids, and receiving care partner support made it possible for them to use them. These participants had moderate dementia and two were new hearing aid users, although for one new and one established hearing aid user their dependence was, in part, due to difficulties with manual dexterity from arthritis. She'd [PwD] never wear hearing aids if I didn't get them out and put them in for her. She struggles to put them in. She has arthritis (CP1)
The participants with dementia generally expressed that they were accepting and appreciative of this support, although some were motivated to retain as much independence as possible in the tasks surrounding hearing aid use to reduce burden on their partners. My dear wife works hard enough. You know, she’s always doing something and, if I can do it myself, it’s, you know, takes something off her (PwD 2)
Professional support (barrier and enabler)
All participants had received a sensory support intervention through the parent study. Participants described how the nature of this support was an important factor in enabling successful hearing aid use, including established hearing aid users. Key aspects related to aiding the development of skills, building routines around hearing aid use, and timely troubleshooting of any problems. But [SST] … used to talk about it like you're talking about it and any problems, you know, iron them out. And she used to send me sheets through the post, and that, to fill in, you know, these worksheets, and things. So, yeah, it's been very helpful … they’ve got me … into a routine, you see? (PwD 6)
The perceived accessibility and responsiveness of professional support was also important. This became a barrier when participants’ expectations were not met, leading to disappointment, frustration, or lack of trust in services. This aspect was only raised by established hearing aid users. That’s the thing that upsets her [PwD] more than anything because … her left ear is a problem because it keeps falling out … so the hearing people suggested that we had these molds made they said that that would be a lot better for us. So we’ve had the molds made and the molds have come but when the lady came to fit them, she hadn’t got the right pieces to piece them together with the hearing aid that fits at the back of the ear … it was a big disappointment and the fact that it was over two weeks ago is a bigger disappointment because we’re still struggling with the ones that we’ve got now (CP 7)
Discussion
This qualitative research used a theory-informed approach to explore influences on hearing aid use in a sample of people with dementia and their care partners that had received hearing aids and a sensory intervention aimed at supporting their use. To the best of our knowledge, this is the first study of its kind to adopt a theory-informed approach to explore this, and we suggest that the findings represent a best-case scenario due to the enhanced support that the participants received. In relation to a “behavioral diagnosis” (Michie et al., 2014), our findings suggest that the TDF domains environmental context and resources, behavioral regulation, reinforcement, and social influences are of greatest relevance to hearing aid use in dementia. Within these domains, we identified a range of factors that may influence the target behavior of hearing aid use. There were some differences according to whether the participants were new or experienced hearing aid users, and minor differences in relation to severity of hearing loss and cognitive impairment. However, no clear influences were noted regarding self-perceived impact of hearing loss.
Several of our findings align with previous research with this population. The establishment of routines to minimize the risk of misplacing hearing aids, the motivating impact of experiencing positive outcomes, and the importance of care partner support have previously been identified as enablers (Gregory et al., 2020; Hooper et al., 2022). Likewise, difficulties with handling of aids or resources and difficulties with fit have been reported as barriers in previous research (Hooper et al., 2022). This strengthens the credibility of the existing evidence-base.
Several novel findings within our study extend understanding. Our finding that optimizing environmental conditions such as lighting and contrast during hearing aid maintenance tasks acts as an enabler is novel. This may be of particular relevance to this population due to the impact of dementia on visuospatial function (Rizzo et al., 2000), and aligns with environmental modification approaches to enhance functioning in dementia (Woodbridge et al., 2018). Furthermore, the motivation to retain active roles in the care and use of hearing aids within the framework of care partner support, and the minimal impact that the onset of dementia had on previously established hearing aid care and use routines, have not been reported in previous research. These findings highlight the importance of support being person-centered with this population, aligning with practice recommendations (Dawes et al., 2022; Littlejohn et al., 2022).
Our findings suggest that several key intervention functions (Michie et al., 2014) may be relevant for hearing care professionals and others supporting people with dementia and hearing loss. First, interventions should develop the person with dementia’s routines for hearing aid care and wear, optimizing environmental conditions such as lighting and contrast during maintenance tasks. This is a training intervention approach that includes environmental restructuring (Michie et al., 2014).
Second, the type of hearing aid should optimize hearing ability and include dementia-friendly features that support use, such as a clear battery-warning alert and visual prompts to aid differentiation between left and right aids. The hearing aids and associated resources should also be suitable for the person to handle. In this regard, offering trials of differing hearing aids may be advantageous (Dawes et al., 2022). This is an enablement intervention approach (Michie et al., 2014).
Third, an incentivization intervention approach (Michie et al., 2014) could enable people with dementia to recognize positive consequences of hearing aid use, fostering motivation for their use. In this regard, receiving ongoing reminders about tangible ways in which hearing aids enable communication and connection with other people may be beneficial. This may be particularly relevant for this population as hearing aid use in dementia has been shown to reduce over time (Powell et al., 2023).
Fourth, hearing care professionals should also work in partnership with care partners to build their skills and understanding in supporting the person with dementia’s hearing aid use. This is an education intervention approach that would aim to foster enablement within the care partner—care recipient relationship (Michie et al., 2014), and may be particularly important for first-time hearing aid users with dementia.
Lastly, follow-up should be available and responsive to needs as they arise to troubleshoot difficulties and maintain motivation for continued use. This service provision (Michie et al., 2014) aspect presents a challenge because research suggests that a lack of time and resources impacts negatively on hearing care professionals’ potential to support people with dementia who have more complex needs (Wright et al., 2014). In light of this, developing pathways for dementia-specific hearing clinics, such as the clinic outlined in NHS England’s guide for hearing loss and healthy aging, (NHS England, 2017) may be beneficial.
Strengths
This study has built upon the emerging understanding that exists regarding enablers and barriers to hearing aid use in dementia, drawing this together within the theoretical framework of the TDF. We consider that the implementation of this framework is a strength of this study. Furthermore, use of the TDF has enabled a “behavioral diagnosis” (Michie et al., 2014) of factors that influence hearing aid use in dementia, and structured consideration of intervention functions to address these influences.
Limitations
The participants within this study were a convenience sample drawn from a parent research trial. Participants in dementia research are generally younger, more highly educated, healthier and from a majority ethnic background than the wider population with dementia (Cooper et al., 2014), influencing the applicability of results. Furthermore, in our study all the participants had received new hearing aids and an intervention that was designed to foster hearing aid use, they were all actively using their hearing aids, and all had a care partner that was actively involved in the research intervention. These factors may have positively influenced the target behavior of hearing aid use in our sample. Therefore, whilst this study has generated understanding of influencing factors for hearing aid use in dementia, it has not investigated how enablers and barriers to hearing aid use might differ for people with dementia who reject hearing aids, access standard audiology pathways, do not have care partner support, or have a greater severity of cognitive impairment. We suggest that our findings should be considered reflective of the best possible scenario.
Additionally, although the researchers adjusted their approach to optimize participation, it was more challenging to maintain effective communication with the participants with dementia in the five interviews that were conducted remotely due to national COVID restrictions. These interviews were shorter overall (mean duration 51 minutes, compared with a mean of 69 minutes for the face-to-face interviews) and the proportion of responses made by care partners was greater, suggesting that the method of data collection influenced the quality of interaction. This is a known limitation of remote interviewing (Davies et al., 2020).
Future Research
Michie et al. (2014) highlight that through collecting and triangulating data about a target behavior from multiple sources, a stronger understanding of influencing factors emerges. While the present study has started to build on an existing, fragmented, evidence base, confidence would increase by researching influencing factors on hearing aid use in dementia from an increased variety of methods, including through quantitative investigation of a larger population group. Additionally, we have suggested intervention functions that may support hearing aid use in this population. Further research to develop and evaluate interventions that adopt these functions is warranted.
Conclusions and Implications
Our study has developed understanding of factors that influence the behavior of hearing aid use in people living with mild-moderate dementia and age-acquired hearing loss. To the best of our knowledge, this is the first primary research study that has used a theory-informed approach to investigate this. Our findings suggest that hearing aid use in dementia is enabled through (i) establishment of routines that support hearing aid wear and care; (ii) provision of hearing aids that optimize hearing ability with features and resources that facilitate their use; (iii) experiencing benefits in daily life; and (iv) provision of formal and informal support that is responsive to the person with dementia’s abilities. Our findings suggest that hearing aid use in dementia is hindered if the person has difficulty with aspects of either their hearing aids or maintenance resources, especially if support to troubleshoot these difficulties is not timely or responsive. We have suggested a variety of intervention functions that may support hearing aid use in dementia from our findings, which would benefit from further research to establish their efficacy.
Supplemental Material
Supplemental Material - Enablers and Barriers to Hearing aid Use in People Living With Dementia
Supplemental Material for Enablers and Barriers to Hearing aid Use in People Living With Dementia by Emma Hooper, Laura J.E. Brown, Hannah Cross, Piers Dawes, Iracema Leroi, Iracema Leroi in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Constance Owens Charitable Trust; the National Institute of Health Research Manchester Biomedical Centre [BRC-1215–20,007]; the National Institute for Health Research Greater Manchester Patient Safety Research Collaboration; the European Union’s Horizon 2020 research and innovation program [Grant 668,648]; the Global Brain Health Institute; and the Alzheimer’s Society [Grant 403, AS-PhD-17b-006].
Ethical Approval
We gained ethical approval for the study from the Haydock NHS Research Ethics Committee (IRAS ID213875; SENSE-Cog protocol version 6.0).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.