
Abstract
Several interventions for care partners of persons living with dementia target the negative effects of behavioral symptoms. Evidence suggests that actively engaging care partners improves outcomes. However, there is little information on the best approaches to optimize active engagement. Enhancing Active Caregiver Training (EnACT) is an arts-based intervention designed to help care partners address the behavioral symptoms of dementia. The purpose of this study is to describe the process of partnering with care partners of persons living with dementia (n = 9) to refine EnACT. We conducted a series of three iterative focus groups to (1) identify video vignettes, (2) test intervention activities, and (3) gather feedback. Focus groups were analyzed in three cycles using structural, descriptive, and pattern coding. Intervention revisions focused on narrowing vignette topics, removing confusing components, enhancing accessibility, and adding facilitator training. Partnering with care partners improved intervention feasibility in preparation for future testing.
• This paper provides an example of how partnering with community-based care partners of persons living with dementia can help optimize interventions to address care partner specific needs. • This paper illustrates that combining video vignettes and tailored activities through the Enhancing Active Caregiver Training (EnACT) intervention is a useful way to engage care partners in a discussion of dementia-related symptoms. • Care partners thought EnACT was relatable to them and would be applicable to caring for persons at different stages of dementia.
• Findings from this study can be used as a guide for other researchers interested in utilizing focus groups to iteratively revise an early-stage intervention. • Care partners’ recommendations for refining EnACT were used to develop a facilitator guide, which will be incorporated into the intervention moving forward.What this paper adds
Application of study findings
Introduction
Behavioral symptoms associated with Alzheimer’s disease and related dementias (ADRD), including aggression, apathy, agitation, and disinhibition (Cheng, 2017), are associated with increased stress for informal care partners (Gilhooly et al., 2016). Care partners, most often family members, experience negative effects due to this stress (Lee et al., 2017). Greater levels of burden, depression, poor health, and decreased quality of life impede the ability to provide the type of care that persons living with dementia require (Laver et al., 2017).
Many interventions developed to support the needs of care partners of persons living with dementia demonstrate some level of benefit (Walter & Pinquart, 2020). A recent meta-analysis of describes weak to moderate effect sizes on outcomes such as burden, functional independence, behavioral symptoms, and institutionalization (Walter & Pinquart, 2020). Intervention approaches include counseling/psychotherapy, self-care/relaxation training, psychoeducation, professional support, and behavioral management/skills training (Gaugler et al., 2017). Interventions with the greatest outcomes actively engage care partners by delivering both education and skills. However, strategies involved in the transfer of education and skills are not clearly defined nor evaluated (Walter & Pinquart, 2020).
Actively engaging care partners during an intervention is one area that holds potential for improving care partner outcomes (Walter & Pinquart, 2020). Active engagement is defined as care partners applying both knowledge and skills gained during an intervention. This may occur using a variety of strategies, such as role-play, discussion, and problem-solving (Gaugler et al., 2017; Walter & Pinquart, 2020). Studies have found that caregiving interventions are less effective if they focus solely on didactic teaching when compared with interventions that combine teaching with practice (Witlatch & Orsulic-Jeras, 2018). General efficacy of interventions has been a major focus, which has reduced research focused on the intervention process. The process of engagement, a component of intervention delivery, has not been tested in a systematic way, reducing knowledge about the mechanisms underlying active engagement (Gaugler et al., 2017).
In an effort to optimize active engagement, we developed the EnACT intervention for informal care partners of persons living with dementia. Our goal was to develop a systematic process by which care partners might actively engage in training using techniques from communication, the arts, and education to better prepare to address the behavioral symptoms associated with dementia. EnACT uses care partner informed videos (Eaton & Madsen-Wilkerson, 2020) to represent dementia caregiving scenarios such as repetition, confusion, and hallucinations. Care partners then work through engagement activities that promote exploring choices, outcomes, and practice to address the behaviors within each scenario. Cognitive processing, making choices, and verbalizing are skills explored through active engagement with the intervention. EnACT may serve as a stand-alone intervention or be incorporated into care partner support groups and pre-existing interventions to augment active engagement. The process of initial development is reported elsewhere (Eaton et al., 2023).
Theoretical Framework
Imagined interactions theory (Honeycutt, 2010) and the Consequences of Dementia Caregivers’ Stress Process Model (Campbell et al., 2011) guided the development of EnACT (Figure 1). Imagined interactions theory (Honeycutt, 2010) explains the cognitive process by which individuals imagine encounters with others. Imagining future interactions is one method of preparing through cognitive rehearsal. Research on using imagined interactions to rehearse for the future demonstrates a reduction in the difference between imagination and reality (decreased discrepancy), promotes preparation in advance (increased preparation), and enhances the level of detail of an encounter (increased multisensory detail). Outcomes from this process include reduced conflict, greater relationship quality, and increased preparation. This allows individuals the opportunity to make mistakes, anticipate outcomes, and personalize future tasks (Bodie et al., 2013). Theoretical framework: Theoretical framework using the EnACT intervention to improve the caregiver stress process (Campbell et al., 2011) through the mechanisms of Imagined Interactions (Honeycutt, 2010).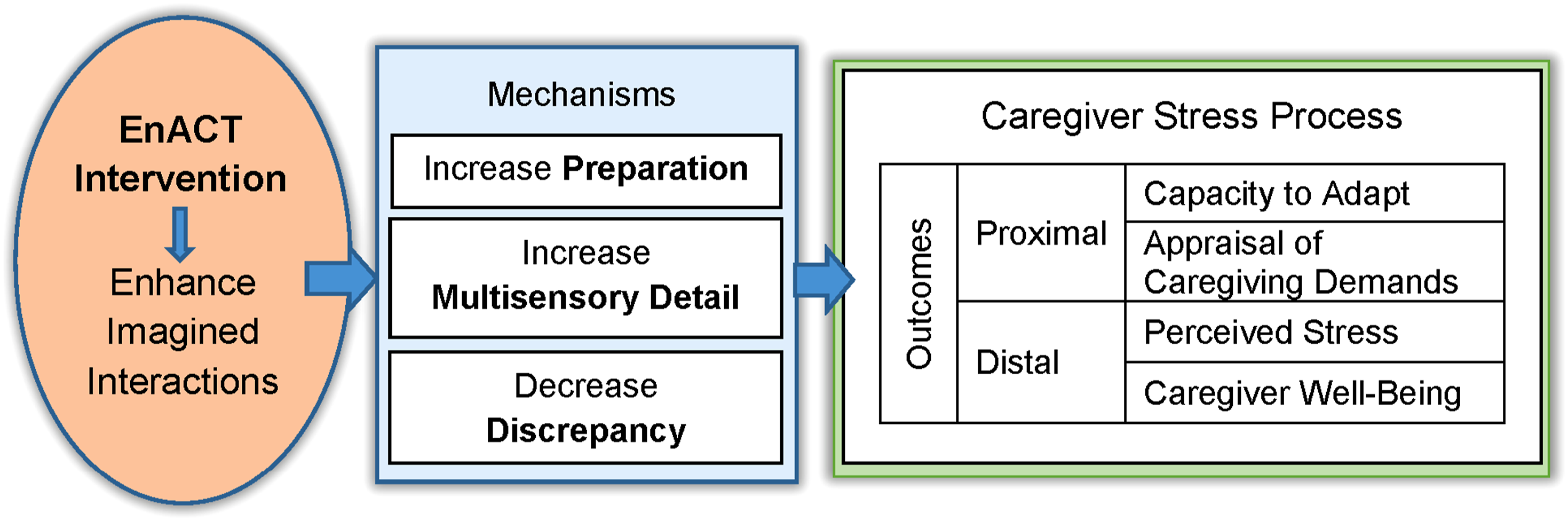
The Consequences of Dementia Caregivers’ Stress Process Model (Campbell et al., 2011), adapted from Schulz and Martire’s (2004) Stress-Health Model, demonstrates the consequences of the stress process for care partners of persons living with dementia. Stressors influence a care partner’s assessment of demands and capacity to adapt, which leads to the perception of stress and behavioral/emotional responses. A series of studies found that the way care partners respond to perceived stress has consequences, including care partner morbidity/mortality (Schulz & Martire, 2004) and behavioral symptoms of persons with ADRD (Campbell et al., 2011). This intervention targets the link between stressors and care partners’ assessments of demands and capacity to adapt. These theories form the foundation of the EnACT intervention, which aims to address stressors—specifically disruptive behaviors in ADRD—by improving care partners’ imagined interactions. This enhancement is designed to strengthen their ability to assess demands and adapt effectively.
Grounded in a robust theoretical framework and extensive research that underscores care partner stress as a significant and well-documented concern, we propose that active engagement in the EnACT intervention will help care partners anticipate and rehearse challenging scenarios using realistic examples. This process is expected to result in (a) improved management of behavioral challenges and (b) reduced stress through enhanced adaptive capacity and better appraisal of caregiving demands.
This research is an initial step in addressing a larger research objective, how best to use active engagement to reduce dementia care partner stress. Here, we address the research question—How can we revise EnACT to effectively engage care partners of persons living with dementia? We conducted focus groups with care partners to identify strategies for iteratively refining the intervention, with the goal of improving its feasibility and acceptability for future pilot testing.
Methods
Guided by the NIH Stage Model for Behavioral Intervention Development (Stage 1a) (Onken et al., 2014), this qualitative component is part of a sequential qualitative to quantitative mixed-methods study to develop and iteratively refine the EnACT intervention. The University of Utah’s Institutional Review Board approved study procedures (#00135515).
Sample
We sought 10 informal care partners of persons living with dementia to participate in this study using purposive sampling. Excluded from participation were formal care partners, persons under the age of 18, and individuals with non-English language preferences. We collaborated with community-based services, such as the Utah Caregiver Support Program and the Utah Alzheimer’s Association, to distribute flyers and emails to listservs and support groups of care partners of persons living with dementia. Additionally, we partnered with the ongoing Time for Living and Caring research study to contact potential participants who indicated an interest in future research opportunities. After 2 weeks, a research assistant contacted them by phone to describe the study, confirm participant eligibility, and subsequently obtain verbal and written informed consent (Sparks et al., 2024). Enrollees received $50 for each focus group attended with the potential of receiving $150 total in compensation.
Data Collection
A series of three iterative focus groups were conducted in partnership with care partners of persons living with dementia. Focus groups aligned with established guidelines which emphasized that 4 to 12 participants with a minimum of three focus groups were needed (Tong et al., 2007). A series of three online focus groups were conducted with two groups, one group of four meeting in the evening (Group A) and a group of five meeting during the day (Group B), across 4 weeks. Each meeting was held every 2 weeks for approximately 90 minutes and was conducted by the principal investigator (JE) who has experience leading focus groups and a trained research assistant (SN). Meetings were scheduled based on participants’ availability and conducted via Zoom, a secure online platform. During Focus Group 1, participants were introduced to the research team and viewed the previously developed research-based performance called Portrait of a Caregiver. Taking place in a support group, actors portray the experience of caregiving for persons living with dementia using the direct words from in-depth research conducted with care partners (Eaton & Madsen-Wilkerson, 2020). A filmed version was viewed in order to gather feedback on the vignettes most relevant for EnACT inclusion. Focus Group 2 involved testing previously developed practice activities (Eaton et al., 2023) for refinement and improvement. In Focus Group 3, participants provided feedback on the facilitator guide developed during this process (Figure 2). All focus groups were audio recorded, professionally transcribed, and reviewed for accuracy. Field notes of participant observations during the focus groups were taken by research assistants (MFC, SN). Participants completed a demographic questionnaire to allow us to describe those participating in the study. Iterative revision of EnACT: Focus group process to revise the EnACT intervention in collaboration with care partners of persons living with dementia.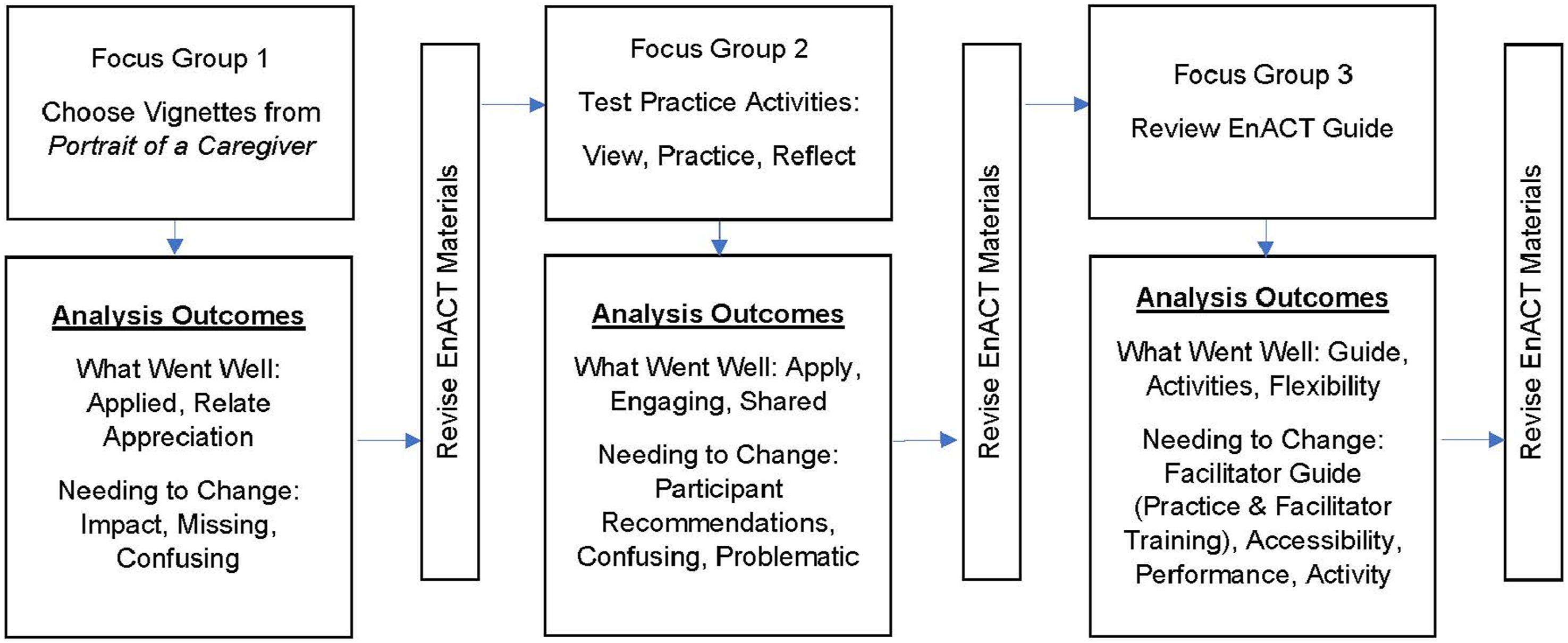
Data Analysis
Univariate statistics were used to describe participants. Focus groups and field notes were analyzed in three cycles of coding: structural, descriptive, and pattern (Saldaña, 2015). First, structural coding was used to organize information into groups to help identify what went well and what needed to change. Second, descriptive coding was used to describe concepts and feedback within each structural code. Finally, a third round of coding was used to organize similar descriptive codes into patterns. Coding was managed using Microsoft Word and Excel. Three research team members coded data (JE, SN, and MFC) and met to resolve conflicts, refine definitions, identify how to code ambiguous segments, and decide how best to group descriptive codes into patterns. Member checks were incorporated into all three focus groups, and peer debriefing occurred after each focus group to facilitate iterative revision and triangulation throughout the process with the goal of increasing trustworthiness.
Results
Demographic Characteristics.
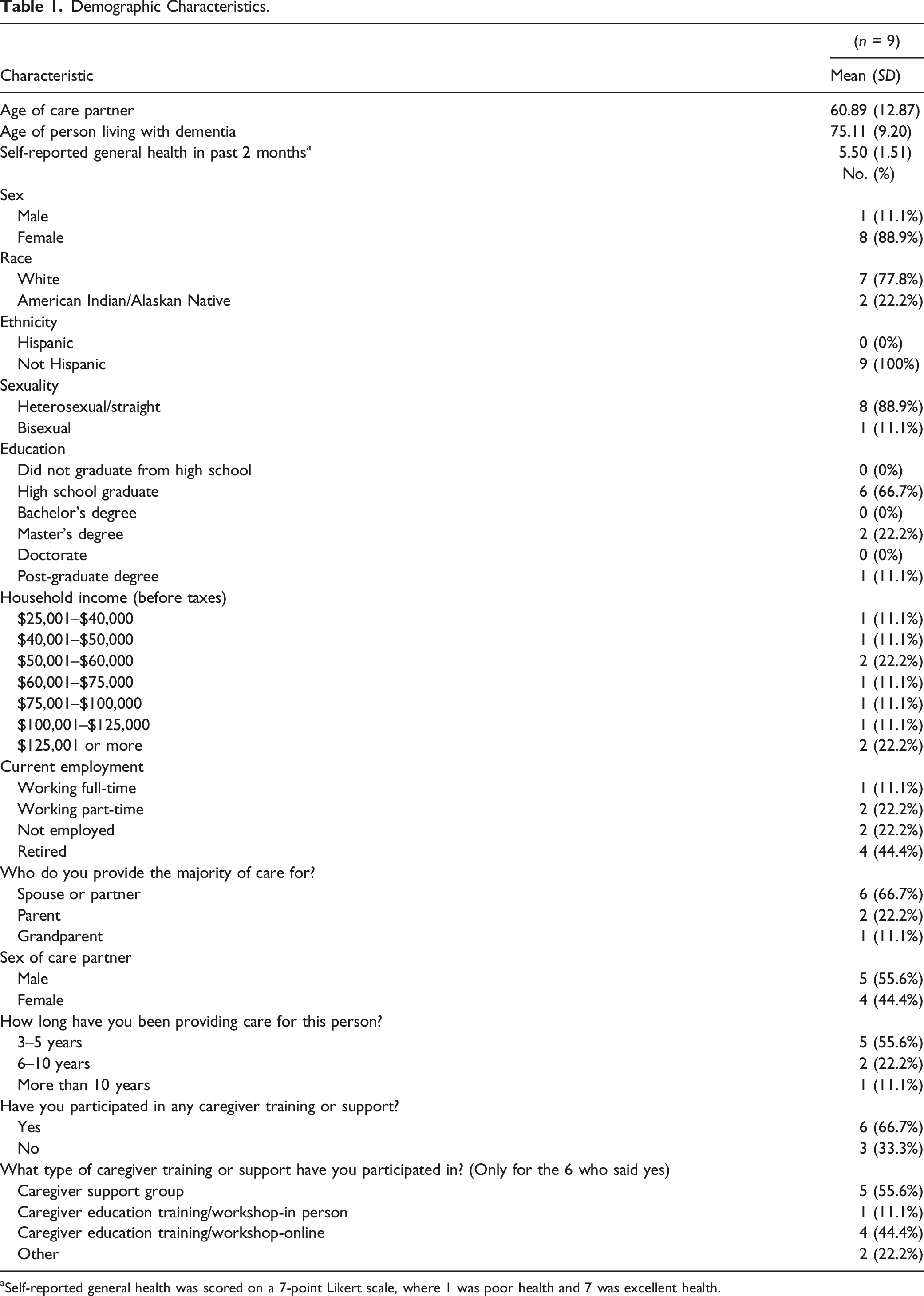
aSelf-reported general health was scored on a 7-point Likert scale, where 1 was poor health and 7 was excellent health.
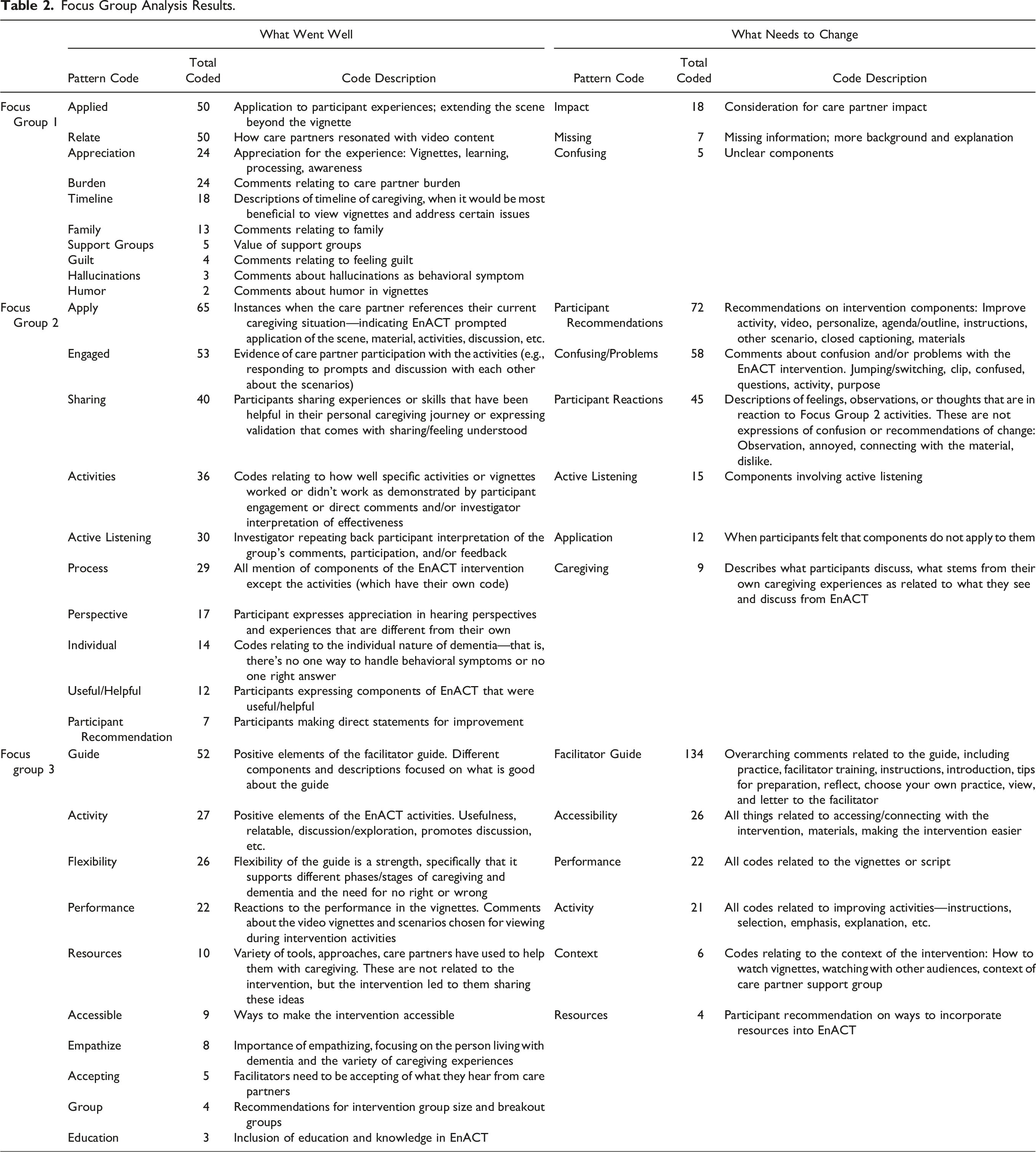
Focus Group Analysis Results.
Focus Group 1
During the first focus group, participants viewed filmed vignettes. Participants used the thumbs-up reaction in Zoom to identify content that related to their experience with ADRD caregiving. A total of 43 moments were identified from the video. These moments covered 22 topics related to the realities of caregiving including need for respite, guilt and burnout, validation, family help, and boundaries. After viewing, participants shared their reactions to the viewing by answering questions focused on ease of understanding, relevance, and which components might be most useful in illustrating behavioral issues in persons living with dementia.
What Went Well: Applied, Relate, Appreciation
Participants described 182 items that worked well, with the most common codes bolded and explained below. Participants discussed the many ways the content I saw [Portrait of a Caregiver] live about six years ago, and I laughed through the whole thing. It was so funny…and as I watch it today, it’s my life day to day. I mean minute to minute, everything that goes on, and you just think—it’s amazing how you can change from “That’s so funny” to “I got to live with this. I got to do this and it’s hard.” (Eva)
Many comments focused on how much each participant could
Components of …they don’t see the whole 24-hour thing, and I think that for care partners, it’s validating…. As care partners, we all get it. Nobody sees all the behind the scenes, and I thought that was one of the things that stood out, and I appreciated that. (Lena)
Needing to Change: Impact, Missing, Confusing
Forty-two items were coded as needing improvement. Participants recommended that care partners not watch the entire film. They described the That was really hard for me to watch. I’ll just put it that way, and I would rather see something that would be maybe one of the things and say, “Hey, how do you deal with this? Or how do you deal with the clogging of the toilet every day? Or how do you deal with--” instead of seeing a whole gamut, like everything. Does that make sense? (Lena)
In addition, at least two participants had interruptions watching in a home environment. Some participants felt information was
Revisions Based on Focus Group 1 Feedback
Revisions to the intervention were made based on focus group feedback, including (1) selecting relevant vignettes for intervention use and (2) creating an index of vignette topics to facilitate multiple discussion pathways to align with care partner training and support groups. Participants confirmed that vignettes provide a catalyst for discussion and sharing and would be useful for training and support groups. Plans to have individuals view the entire film were modified, and we developed a list of 16 vignettes, organized into 22 content topics that would help facilitators easily identify clips that may align with support group and training topics. Closed captioning was added as a constant and not just for those with a need.
Focus Group 2
A total of six activities were tested across the two groups, using four vignettes. Testing involved viewing a brief vignette chosen in Focus Group 1, reading the vignette script to better understand the caregiving interaction, practicing for caregiving using an interactive activity, and reflecting on the experience. Coding identified 331 items, organized into 10 patterns to describe what went well and 223 items coded as needing to change, which were organized into six patterns. The most prominent codes are described below.
What Went Well: Apply, Engaging, Shared
Instances when the care partner referenced their current situation, indicating EnACT prompted application of the scene, material, activities, or discussion, were organized within the code of I think that also in that first sentence I thought, you know, that’s a typical caregiver in my understanding is that it’s so fragmented. It’s like, oh I want to tell you this I want to tell you that, but I need to hurry through this. I want to get to a point. And that’s what I thought when I first-- we first came across that I thought that's the way I sound sometimes. (Florence)
Care partners also showed evidence of
In addition to applying EnACT content to their personal caregiving situations and engaging with the care partners within the vignettes, participants also
Needing to Change: Participant Recommendations, Confusing, Problematic
Participants also provided feedback on what elements needed to change.
Comments about
Revisions Between Focus Groups 2A and 2B
Many of the comments from Group A that related to confusing or problematic elements of the intervention were a result of concurrently testing activities of the intervention and requesting feedback on how those activities were perceived. Therefore, we recognized the need to adjust the protocol before meeting with Group B to clarify the purpose and improve activity delivery. Revisions included summarizing the previous focus group meeting and reiterating how the vignettes were created and their purpose as a tool to facilitate discussion and preparation. We also emphasized that the behavioral symptoms highlighted in the selected clips had been chosen by the participants during Focus Group 1.
It was also imperative to develop a clear delineation between testing and evaluating the intervention. Participants in focus group 2B were told that there were two goals: (1) test activities and (2) evaluate participant experience with each activity. We asked them to hold their feedback until we were through testing each activity. We also told them we would identify when the evaluation of the experience would begin by stating, “Now we are going to switch into evaluation of this story experience. The questions we ask now are to better understand your experience participating in [vignette] activities.” As a result, during Group B, we had a 50% reduction in the number of comments related to confusing or problematic elements of the intervention.
Revisions in Preparation for Focus Group 3
To prepare for Focus Group 3, revisions included adjusting instructions to reduce confusion and improve feedback. Vignettes were edited to simplify the story lines represented in each clip. Participants requested hard copies of the vignette scripts, to view them on or off screen. Thus, we mailed them physical copies of each vignette script. A facilitator guide was developed and revised based on Focus Group 2 testing. This guide included a table of contents, an introductory letter to the facilitator, the Introduction (background, purpose, and explanation as to why storytelling is useful in care partner training), Preparation to begin (EnACT structure, setting up, and tips for preparation), and Instructions for each intervention section. We also reviewed specific intervention activities to identify which worked best for inclusion within the facilitator guide.
Focus Group 3
Based on Focus Group 2 outcomes, we adjusted our plans for Focus Group 3. Our revisions between group 2A and 2B led to positive outcomes and improved processes. Thus, we adjusted our plans for Focus Group 3A to make sure these revisions worked across both groups. This meant a slight difference in Focus Group 3A and 3B agendas. Group 3A reviewed five intervention activities and the Letter to the Facilitator (which was part of the facilitator guide), and Group 3B reviewed the entire facilitator guide to provide feedback specific to acceptability of the materials and the logistics of incorporating the content into training and support groups.
What Went Well: Guide, Activities, Flexibility
Ten patterns describe what went well from a total of 166 codes. Positive components of the facilitator guide were coded as …some of them probably will not resonate with some people. But I think, you know, everybody’s going to find one of those clips that resonates. And then I think the ones that don't resonate initially they'll at least be able to learn from the discussion. (John)
Needing to Change: Facilitator Guide (Practice and Facilitator Training), Accessibility, Performance, Activity
Feedback specific to recommendations for change were organized into six pattern codes. The recommendations for the
The word
Codes relating to things facilitators need to learn before delivering the intervention, how they are trained, tips for preparing facilitators, or the selection of appropriate facilitators fall within the subcode of … I do think the presenter makes a big difference in how the people will respond to it. If you get…someone that knows the facts and just tells you the facts, you lose the people. But if you get someone that can engage you, then it works really well. I think what you’ve written here, what you have here is really good, but you need to have a presenter that can engage the people and get them to feel- to feel what’s going on. (Eva)
Participants also noted facilitator qualities of importance, such as “the facilitator isn’t responsible for fixing us” (Florence), “be accepting of the comments in the group” (Bessie), and the training should include “…some scripted comments for facilitators to support caregivers…” (Mabel).
The
Discussion
The EnACT intervention was created to allow care partners to practice imagined scenarios and prepare for future interactions with the behavioral symptoms of dementia to reduce stress and improve well-being. To optimize engagement in EnACT, we partnered with care partners and identified which intervention components were useful and which needed revision to ensure an appropriate, low burden EnACT protocol for pilot testing. Actively engaging care partners in intervention review and revision allowed us to prioritize care partner needs and preferences and aligned with our goal of enhancing active engagement (National Academies of Sciences, Engineering, and Medicine, 2016). Participants communicated that they felt the EnACT activities helped promote discussion and the vignette topics applied to caring for persons at different stages of dementia. Participants appreciated the opportunity to apply their caregiving experiences during the activities and learn how other care partners were addressing behavioral symptoms, which is similar to findings of other studies (Nehrig et al., 2019).
When conducting the focus groups, we recognized the need to alter our agenda between focus groups to incorporate participant feedback in real time. We learned that asking participants to try intervention components while they were also expecting to evaluate the intervention within the same focus group led to multiple interruptions, confusion, and challenging conversations before the intervention activity was fully tested. Adjusting the focus group agendas, we identified the purpose of each agenda item as testing or evaluation. This greatly improved the experience, the type of feedback we received, and our understanding of the experience of each care partner.
Iterative revision across focus groups was vital for strengthening the intervention and our evaluation process. Our methods incorporating care partner feedback align with the person-based approach to intervention development and evaluation of acceptability and feasibility (Yardley et al., 2015). This approach emphasizes the need to elicit and analyze user reactions to intervention elements using think-aloud techniques and iteratively modify the intervention to optimize it from the user perspective (Yardley et al., 2015).
Additionally, we noted that the way the vignettes were portrayed impacted the participants’ abilities to engage with the intervention activities. For example, we watched the full 60-minute performance that included all vignettes, thinking this was important context for engaging with the vignettes. However, watching via Zoom, participants did not have a shared sense of others’ reactions as they were not in the same in-person space. Participants were muted, meaning that they could not hear laughter, crying, audience movement, and reactions; this limited a shared understanding of how others were feeling or thinking. Additionally, confusion was increased when a vignette included multiple topics which led to frustration and comments on how the scene should be changed, rather than focusing on the behavioral symptoms highlighted for the intervention activity. Thus, vignette topics were narrowed to reduce the number of topics represented within one vignette. Confusing components of vignettes and intervention activities were carefully documented and helped us refine the intervention protocol.
Consistent with prior literature describing preparation for successful implementation, participants indicated that facilitators of the EnACT intervention must be appropriately trained to deliver active engagement activities and adapt to the needs of the care partners (Nehrig et al., 2019; Teresi et al., 2022). Care partners emphasized the importance of the facilitator communicating the purpose of the intervention, which is to practice imagined scenarios to help them prepare for future interactions, rather than expecting specific answers and ways to address each behavioral symptom. The facilitator guide developed during this process was adapted to address participant recommendations, aligning with recommendations for incorporating participant feedback (Yardley et al., 2015). Additionally, it became apparent that the guide alone would not provide enough training to support the flexibility participants felt was required to support the variety of caregiving situations and needs. Thus, a plan was developed to include facilitator training which would also enhance future fidelity testing (Teresi et al., 2022).
Revisions were used to prepare for a future Stage 1b randomized controlled trial (ClinicalTrials.gov #NCT04920006) led by interventionists to test the feasibility and acceptability of the revised EnACT intervention. At that time, we will conduct initial testing on care partner outcomes linked to the theoretical model to answer the research question, does enhancing active engagement through imagined interactions reduce stress by improving capacity to adapt and better appraise caregiving demands? We are currently conducting analyses to identify and define the ways care partners actively engage with intervention components and characterize levels of engagement, to better identify measurement of active engagement. Future work will examine how active engagement during EnACT impacts care partner outcomes.
Limitations
There are certain limitations to this study that we must consider. First, our sample was small and the demographic characteristics were homogenous; however, the sample size and our qualitative approach allowed us to gather in-depth iterative feedback to revise the EnACT intervention with small groups of care partners. The sample did include diversity in age, relationship to care partner, and length of caregiving. In addition, the focus groups were held over Zoom which contributed to challenges such as distractions from family and the home environment. However, attendance was high and attrition was low because participants could easily join online meetings.
Conclusion
This study describes our process for refining an intervention to actively engage care partners of persons living with dementia to anticipate and practice for the challenges associated with caregiving, which will lead to improved ability to manage behaviors, thus reducing stress, improving capacity to adapt, and better appraise caregiving demands. Here, we document the process of revising the EnACT intervention to increase relevance and acceptability in preparation for future testing in a randomized controlled trial. Partnering with community-based care partners improved our ability to enhance this process. Our next steps include testing EnACT in a Stage 1B randomized controlled trial which will evaluate the feasibility, acceptability, and potential mechanisms of change in a larger sample of care partners of persons living with dementia. It is our goal that EnACT may serve as both a stand-alone intervention and a resource to enhance existing interventions by improving protocols and processes to optimize active care partner engagement.
Footnotes
Acknowledgments
We are grateful to the Time for Living and Caring study for support with recruitment. We also acknowledge mentoring support from Drs. Rebecca Utz, Katherine Supiano, and Gary Donaldson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the National Institute on Aging [Eaton, K01AG065623; Ellington, K07AG068185] and the National Institute of Nursing Research [Neller, T32NR013456].
IRB Protocol
The University of Utah Institutional Review Board provided oversight and approved study procedures (IRB_00135515).
Data Availability Statement
The data that support the findings of this study are not publicly available due to small sample size.