
Abstract
Objectives
To identify correlates of hearing aid use in people with dementia and age-related hearing loss.
Methods
Bivariate and multivariate logistic regression analyses of predictor variables from 239 participants with dementia and hearing loss in the European SENSE-Cog Randomized Controlled Trial (Cyprus, England, France, Greece, and Ireland).
Results
In multivariate analysis, four variables were significantly associated with hearing aid use: greater self-perceived hearing difficulties (OR 2.61 [CI 1.04−6.55]), lower hearing acuity (OR .39 [CI .2−.56]), higher cognitive ability (OR 1.19 [CI 1.08−1.31]), and country of residence. Participants in England had significantly increased odds of use compared to Cyprus (OR .36 [CI .14−.96]), France (OR .12 [CI .04−.34]) or Ireland (OR .05 [CI .01−.56]) but not Greece (OR 1.13 [CI .42–3.00]).
Conclusions
Adapting interventions to account for cognitive ability, country of residence, self-perceived hearing difficulties, and hearing acuity may support hearing aid use in people with dementia.
Keywords
Introduction and Background Context
Hearing loss and dementia both increase in prevalence with age (Alzheimer’s Association, 2020; Quaranta et al., 2015). Both hearing loss and dementia are within the top ten causes of disability-related burden globally for people aged 75 and over (Vos et al., 2020). There is also high comorbidity between the two conditions: the prevalence of hearing loss is at least 60% in people with dementia or cognitive impairment that live in the community (Nirmalasari et al., 2017), and it has been suggested that hearing loss may be a risk factor for developing dementia (Brewster et al., 2022; Loughrey et al., 2018).
Hearing aids are the primary means of managing hearing loss among people with or without dementia (Dawes et al., 2022; Ray et al., 2019). Among people living with dementia and hearing loss, hearing aid use may increase their quality of life, mental health, and communication (Atef et al., 2023; Mamo et al., 2018). However, people with dementia or cognitive impairment are less likely to use hearing aids than people without dementia (Fisher et al., 2015; Lupsakko et al., 2005; Naylor et al., 2022; Powell et al., 2023). Lower levels of hearing aid use in people with dementia are likely due to both lower levels of uptake (Nirmalasari et al., 2017) and lower levels of sustained hearing aid use among those who obtain them (Allen et al., 2003; Naylor et al., 2022; Powell et al., 2023), highlighting a need to better understand, and then address, the factors that influence uptake and use in this population. One of the reasons that hearing aid uptake may be lower in people with dementia is because hearing loss may not always be recognized, or may be mistaken for symptoms of dementia (Hopper & Hinton, 2012; Pichora-Fuller et al., 2013) leading to lower referral rates. People with dementia may also be less likely to recognize and act on hearing problems (Batchy et al., 2011).
A recent systematic review reported that many of the correlates of hearing aid use in the general population also pertain to hearing aid use among people with dementia (Hooper et al., 2022). For instance, as with the general population (Hickson et al., 2014; Knoetze et al., 2023; McCormack & Fortnum, 2013; Ng & Loke, 2015), proficiency in handling hearing aids; experiencing positive consequences; the degree of hearing aid comfort or fit; the perceived demands of the listening situations; and receiving prompts or encouragement from others are all associated with hearing aid use among people with dementia (Hooper et al., 2022). Other research suggests that economic factors such as income-to-poverty ratio and level of health insurance may have an additive influence on hearing aid use in people with dementia compared to those without dementia (Powell et al., 2023), and that severity of hearing loss is associated with hearing aid use in people with dementia (Kim et al., 2021; Nirmalasari et al., 2017), as in the general population (Knoetze et al., 2023). Research in the general population suggests that age and gender are associated with hearing aid use, with a trend towards people of older age and male gender being more likely to adopt hearing aids (Knoetze et al., 2023). However, the effects of these demographic factors on hearing aid use in people with dementia are not known.
The main limitation with previous research identified by Hooper et al. (2022) was that there has been little research that has investigated correlates of hearing aid use in people with dementia, which limits understanding of factors that influence use. Furthermore, no studies to date have attempted to determine the relative importance of a range of factors associated with hearing aid use in people with dementia. Understanding this could inform the development of interventions to promote hearing aid use and improve hearing-related quality of life. For the present study, we therefore investigated correlates of hearing aid use in a cross-sectional sample of community-residing people with dementia and hearing loss.
Methods
Participants
This study utilized screening and baseline data from the European SENSE-Cog Randomized Controlled Trial of a sensory intervention for people with dementia and hearing and/or vision loss on quality-of-life outcomes (Regan et al., 2019). Participants of the SENSE-Cog trial were enrolled between April 2018 and April 2021 across five European sites (Cyprus, England, France, Greece, and Ireland). All met the following inclusion criteria: Aged ≥60 years old; clinically diagnosed with dementia (Alzheimer’s disease, Vascular dementia or mixed dementia), in the mild-moderate stage, as indicated by a MoCA score of ≥10 (Nasreddine et al., 2005); had adult-acquired hearing and/or vision impairment (hearing impairment was defined as bilateral hearing acuity worse than 35dBHL at 1000 Hz and above in the better ear); residing in the community; and had a study partner. Study partners were family members or close friends of the person with dementia, aged over 18 years, in regular contact with the participant, and willing to participate in the study. Site-specific ethical approval was in place for the trial, in accordance with the individual requirements of each country. Further details are available in Regan et al. (2019).
The sample for the present study was a pre-randomization subset of 239 participants with a diagnosis of dementia who met the eligibility criteria for inclusion in the main trial and screened positively for hearing loss at trial enrollment. This sample size was sufficient to test the fit of our regression model for an expected medium effect size (Field, 2018).
Study Design
We performed secondary analysis of cross-sectional data to evaluate potential correlates of hearing aid use in people with dementia. The data were collected during pre-randomization home visits by research assistants who were trained in the administration of the measures.
Theoretical Framework
We organized our data according to the Capabilities, Opportunities, and Motivations model of Behavior change (COM-B) (Michie et al., 2011, 2014). The COM-B model suggests that behavior (B) − in this case hearing aid use − is generated from interactions between the components capability (C), opportunity (O), and motivation (M). In accordance with Michie et al. (2011), capability denotes the person’s physical or psychological capacity to enact the behavior. Opportunity represents external factors that enable or prompt the behavior within the physical (environmental) or social (cultural) setting. Motivation refers to reflective and automatic processes that direct a person’s behavior. Analysis of influences on hearing aid use according to the framework of the COM-B model facilitates a ‘behavioral diagnosis’ of what needs to change for the target behavior to occur (Michie et al., 2014). We considered that use of this model would help to generate understanding to inform intervention design. Predictor variables that did not map to the COM-B model were included as control variables.
Outcome Variable (Behavior)
Hearing Aid Use
The outcome variable was hearing aid use, ascertained by responses of the study partner to the question ‘Does the person currently use a hearing aid?’ (Yes/No).
Predictor Variables (Capability, Opportunity, Motivation, Control)
Capability: Cognitive Ability, Vision Impairment, Health Status, and Functional Dependence
Cognitive ability was determined by the total score achieved on the Montreal Cognitive Assessment (MoCA) (Nasreddine et al., 2005). The MoCA is a clinician-/researcher-administered 30-point cognitive screening tool with high sensitivity and specificity. Higher scores denote better cognitive ability.
Vision impairment was ascertained through the PEEK acuity app (https://peekvision.org/en_GB/peek-solutions/peek-acuity/). This is a researcher-administered validated Android smartphone-based test that provides a measure of distance visual acuity (Bastawrous et al., 2015). We categorized participants with scores ≥0.2 LogMAR as visually impaired, and those with scores <0.2 LogMAR as not visually impaired (Regan et al., 2019).
Health status was evaluated by the study partner’s response to the question, ‘In general, would [person with dementia’s name] say his/her health is excellent, very good, good, fair, or poor?’ This question is taken from the proxy 12-item Short Form survey (SF-12) (Ware et al., 1996), which is a valid and reliable measure of health-related quality of life (Huo et al., 2018).
Functional dependence was measured by the Bristol Activities of Daily Living Scale (BADLS) (Bucks et al., 1996), which was completed by the study partner. The BADLS evaluates the person with dementia’s level of function across 20 activities of daily living (ADLs). We categorized scores of 0–14 as lower dependence and scores of 15–60 as higher dependence, using a categorization reported in previous research (Leroi et al., 2024).
Opportunity: Living Situation, Country of Residence, and Access to Subsidized Hearing Aid Provision
Living situation was dichotomized as living with someone versus living alone. Country of residence was categorized according to which of the five European trial sites the participant lived (Cyprus, England, France, Greece, and Ireland). Access to subsidized hearing aid provision was categorized as low-medium or high-full subsidy for each country using information from the ‘State of provision of hearing aids in Europe’ report for England, France, and Greece (EFHOH, 2022), publicly available information for Ireland (Hearing aids - HSE.ie), and information from an audiologist in Cyprus (Thodi, 2023). Subsidy levels were lower (maximum €900 stereo subsidy) and/or subject to means testing in Cyprus, Greece, and Ireland. We therefore categorized these countries as low-medium subsidy. Subsidy levels were higher (€1900 stereo subsidy) or fully subsidized without means testing in England and France, and so we categorized these countries as high-full subsidy.
Motivation: Hearing Acuity, Self-Perceived Hearing Difficulty, Engagement in Social Activities, and Depression
Hearing acuity was measured using the researcher-administered Siemens HearCheckTM Screener. This validated device screens hearing acuity at the 1 kHz and 3 kHz frequencies at decreasing fixed intensities (75, 55 and 35 dBHL at 3 kHz and 55, 35 and 20 dBHL at 1 kHz) (Parving et al., 2008) and has good sensitivity and specificity (Abes et al., 2011). The score represents the number of tones heard from a possible maximum of 6 tones. Higher numbers represent better hearing acuity. For our analysis we used the total better ear score.
Self-perceived hearing difficulty was evaluated by the researcher-administered Hearing Handicap Inventory for the Elderly (HHIE) (Ventry & Weinstein, 1982). This assesses self-perceived emotional and situational impact of hearing loss in older adults. Following comparison of self- and study partner-reported outcomes for the HHIE, the self-report from the person with dementia was included in the analysis as this relates more closely into the motivation component of the COM-B model and was significantly correlated with the study partner score (r (4) = .51, p < .001). In alignment with previous studies (Kawata et al., 2021; Leroi et al., 2024), we categorized total scores of 0–16 as no or minimal perceived difficulty, 18−42 as mild to moderate perceived difficulty, and >42 as significant perceived difficulty.
Frequency of engagement in social activities was established from the person with dementia and their study partner’s report of engagement in the following health and social care activities: cognitive rehabilitation, cognitive stimulation therapy, dementia café or memory café, music therapy, befriending service, exercise/mobility class, animal assisted therapy, day center, lunch club, education group, other. We assigned a binary value of 1 (yes) if they participated in any of the listed activities at least monthly, or 0 (no) if they did not engage in any activities.
Depression was evaluated according to the Neuropsychiatric Inventory (NPI) (Cummings et al., 1994). This is a validated study partner-rated measure that assesses the presence, frequency, and severity of neuropsychiatric symptoms across ten different domains of behavior. For our analysis, we calculated a composite total from the frequency x severity scores of the depression domain. In alignment with previous studies (Zhang et al., 2012), we categorized composite scores of ≥4 as being indicative of clinically significant depression.
Control Variables: Age and Gender
Age (in years) was added as a continuous variable. Self-reported gender (man or woman) was added as a categorical variable.
Analysis
We undertook our analysis using IBM SPSS Version 29. Descriptive statistics were examined for dispersion and central tendencies. To determine which variables to include in a multivariate logistic regression model, we first evaluated associations between each predictor variable and hearing aid use through a series of bivariate logistic regression analyses. Using a significance level of p = ≤ .05, we identified the predictor variables that were independently associated with hearing aid use and included these in a multivariate logistic regression analysis model. We took this approach to guard against model instability due to the sample size and number of variables included (Stoltzfus, 2011).
Results
Participant Characteristics
Characteristics of the Sample.
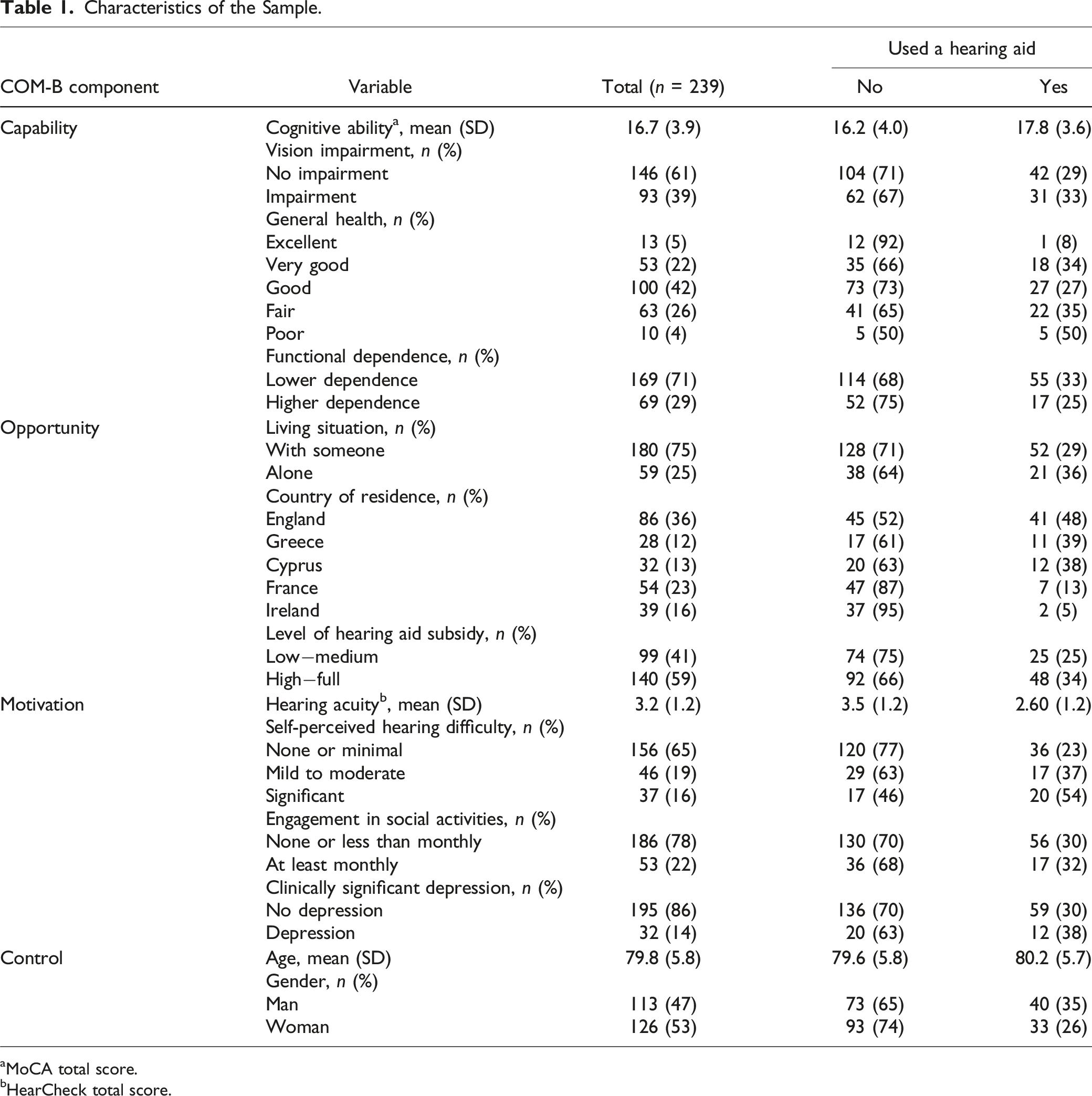
aMoCA total score.
bHearCheck total score.
Correlates of Hearing Aid Use
Bivariate and Multivariate Associations With Hearing Aid Use.
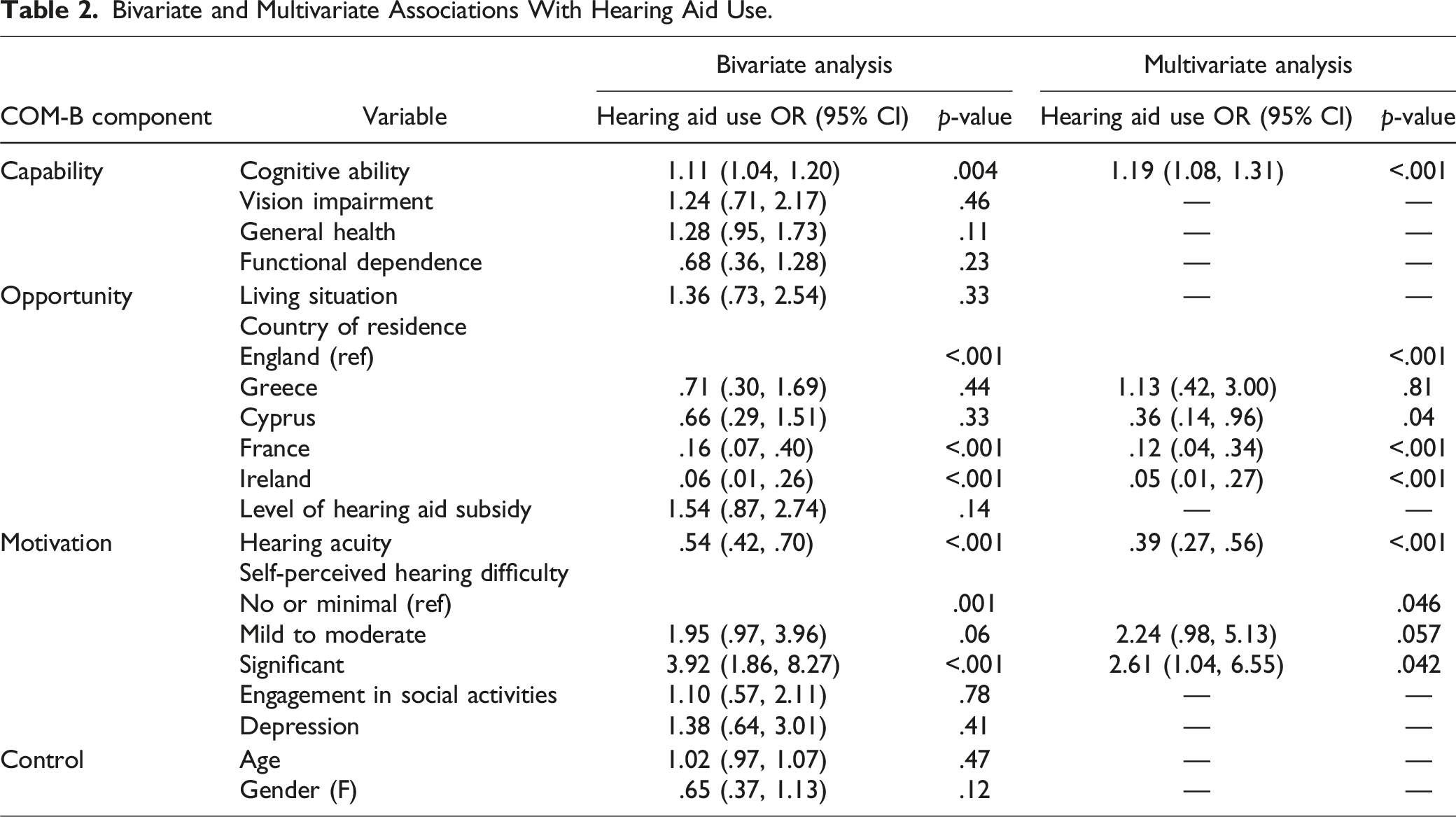
The multivariate logistic regression model was statistically significant: Chi squared (DF, n = 8) = 86.731, p = < .001, explaining between 30% (Cox and Snell R square) and 43% (Nagelkerke R square) of the variance in the dependent variable, and correctly classifying 78.2% of cases.
In the multivariate logistic regression analysis, cognitive ability, country of residence, hearing acuity, and self-perceived hearing difficulty remained significantly associated with the likelihood of hearing aid use. This represents one variable in each of the capability and opportunity components, and two variables in the motivation component of the COM-B model (Table 2).
Self-perceived hearing difficulty was the strongest correlate of hearing aid use. The odds of hearing aid use for participants with significant self-perceived difficulty were 72% greater than for those who reported no or minimal self-perceived difficulty (OR 2.61 [CI = 1.04–6.55]). There was no significant difference in odds of hearing aid use between those with mild-moderate and no or minimal self-perceived difficulty. For cognitive ability, the odds of hearing aid use were greater in participants with higher cognitive ability. Every unit increase in the MoCA assessment score was associated with a 19% increase in the odds of using a hearing aid (OR 1.19 [CI = 1.08–1.31]). For hearing acuity, the odds of hearing aid use decreased in participants with better hearing, corresponding to a 61% decrease in the odds of using a hearing aid with every ∼20 dB improvement in hearing acuity (OR .39 [CI = .27–.56]).
In relation to country of residence, the odds of hearing aid use were significantly lower for participants living in Cyprus, France, or Ireland relative to those living in England. Those living in England had 72% increased odds of using a hearing aid compared to Cyprus (OR .36 [CI = .14–.96]), 89% increased odds of using a hearing aid compared to France (OR .12 [CI = .04–.34]), and 95% increased odds of hearing aid use compared to Ireland (OR .05 [CI = .01–.56]). The odds of hearing aid use in Greece were not significantly different to those in England.
Discussion
This study investigated correlates of hearing aid use in a cross-section of community-residing people with dementia and hearing loss within the framework of the COM-B model. This is the first study of this nature to investigate multiple correlates concurrently, and thus to give an indication of their relative importance.
Capability and hearing aid use
Cognitive ability was the only variable within the capability component that was associated with hearing aid use. This adds to existing research that has shown a correlation between cognition and hearing impairment in a general population sample of people aged over 75 (Lupsakko et al., 2005) by demonstrating that level of cognitive functioning is also associated with hearing aid use among people with clinically diagnosed dementia. Although investigation into explanatory causes for this was beyond the scope of the present research, lower levels of use in those with more advanced cognitive impairment could be influenced by functional decline associated with progression of dementia. Previous research has reported that deterioration in executive functioning (such as planning and executing actions) predicts impairment in ability to perform activities of daily living (Cipriani et al., 2020); thus, evaluation of the influence of executive functioning on hearing aid use could provide a starting point for further empirical investigation with this population.
Opportunity and Hearing Aid Use
Within the opportunity component country of residence, but not level of hearing aid subsidy, was associated with hearing aid use. For example, participants in our study living in England had significantly higher odds of hearing aid use than those in France, despite both countries being classified as having a high level of hearing aid subsidy. A possible explanation for this is that access to fully subsidized hearing aids through the public National Health Service has been long-established in England, whereas in France the level of reimbursement increased markedly during the recruitment period for our study under the French government’s ‘100% Sante’ reforms, now covering the full cost of basic hearing aids (EFHOH, 2022; Légifrance, 2019). A recent European Hearing Instrument Manufacturers Association (EHIMA) Euro Trak survey reported that hearing aid uptake in France increased to 45.7% in 2022 from 41% in 2018 following the introduction of the reforms (EHIMA/ANOVUM, 2022), suggesting that they may be having a positive effect. Re-evaluation of hearing aid uptake among people with dementia in France may therefore be advantageous in time. Nevertheless, despite Greece being identified as having a ‘worryingly low’ level of subsidy by the European Federation of Hard of Hearing People (EFHOH) (2022, p. 2) the odds of hearing aid use there were not significantly different to those in England, suggesting that cultural factors beyond the economics of hearing aid provision may be influencing use (Zhao et al., 2015).
Motivation and Hearing Aid Use
Hearing acuity was negatively associated with hearing aid use in our study, suggesting that people with more severe hearing loss are more likely to use hearing aids. This aligns with findings for both the general population (Knoetze et al., 2023) and people with dementia (Kim et al., 2021; Nirmalasari et al., 2017). Given that people with mild-moderate hearing loss also benefit from using hearing aids (Ferguson et al., 2017), it is concerning that we found that the odds of hearing aid use decreased by 61% with every ∼20 dB improvement in hearing acuity.
Further, and in line with findings for the general population (Knoetze et al., 2023), greater self-perceived hearing difficulty was the strongest correlate of hearing aid use among people with dementia. To our knowledge, the association between self-perceived hearing difficulties and hearing aid use has not previously been investigated among people with dementia. We had postulated that self-recognition of hearing difficulties may be particularly important among people with dementia due to the lower self-awareness and insight associated with dementia (Mograbi et al., 2021). However, as there was no comparison group of people with healthy cognition in the present study, we were not able to investigate whether lower levels of insight might result in less likelihood of reporting hearing difficulties among people with dementia.
Implications for Practice
Although our results are not able to demonstrate causal relationships, they suggest that the COM-B components psychological capability (cognitive ability), physical opportunity (country of residence), and reflective motivation (hearing acuity and self-perceived hearing difficulty) are potential areas that could be targeted to support hearing aid use among people with dementia.
To address psychological capability, firstly it is important to increase understanding of why lower cognitive ability might be associated with reduced hearing aid use, and then to address these factors through interventions. Cognitive rehabilitation is an intervention approach that has been demonstrated to improve ability to complete targeted activities among people with mild to moderate dementia (Kudlicka et al., 2023), and could therefore provide an evidence-based way to improve capability in hearing aid use. According to Kudlicka et al. (2023), cognitive rehabilitation interventions may include a focus on developing habits and routines (such as designating a place to store hearing aids and their maintenance equipment) and implementation of compensation strategies (such as external prompts to use hearing aids) as part of the approach. Research suggests that structured support is key in enabling successful outcomes in cognitive rehabilitation (Clare et al., 2019). Implementation of this approach may therefore necessitate increased frequency of input from hearing health professionals.
To address physical opportunity, it is important to understand what factors might influence use by country. Further research to increase understanding of national differences in hearing aid use among people with dementia is therefore warranted. Zhao et al.’s (2015) paper on the influence of culture on hearing aid uptake and use provides a helpful starting point, through suggesting that cross-cultural psychological factors including stigmatization and social representation of hearing disability may be relevant factors to consider and investigate.
To address reflective motivation, consideration of ways in which hearing interventions could be targeted towards people with milder hearing loss who may not recognize the need for hearing aids may be warranted. Universal screening for hearing loss may therefore be advantageous. In this regard, implementation of Littlejohn et al.’s (2022) international practice recommendation to include hearing screening within the specialist diagnostic evaluation for dementia may be beneficial, alongside regular screening following a diagnosis of dementia, such as at two-yearly intervals as recommended by the United Kingdom’s National Institute for Health and Care Excellence (2018). Evaluation of whether such measures are (a) implemented, and (b) effective in increasing hearing aid uptake and use, is warranted.
It is also important to consider how to address any evident lack of insight that impacts on reduced recognition of hearing difficulties. In this regard, facilitating a trial of hearing aids so that the person experiences aided and unaided hearing may aid acceptance. If it is not possible to address this successfully, alternative interventions such as communication training for people with dementia and their care partners may be worth pursuing as an alternative to hearing aids (Mamo et al., 2017; Meyer et al., 2020).
Limitations
This study has several limitations. First, the sample for this study was recruited for a study of hearing and/or vision loss in people with dementia. Our sample may therefore be biased towards people who recognized that they have hearing difficulties. In this respect, our prevalence estimate of 30.5% hearing aid use should be treated with caution as it probably overestimates the level of hearing aid use within the wider population of people with dementia. However, because the sample included a range of people across key variables, correlational analyses are likely to be reliable. Second, through our use of logistic regression analysis we have identified associations between predictor variables and hearing aid use among people with dementia. We have not investigated causal relationships. Experimental research is warranted in this respect. Third, our use of a cross-sectional design precluded evaluation of the factors that influence hearing aid use over time. Longitudinal studies are therefore warranted. Fourth, our study involved secondary analysis of data that had been collected. This precluded investigation of additional variables that may be associated with hearing aid use in people with dementia, such as perceived hearing aid benefit and level of support. Fifth, our use of a screening measure for hearing aid use limited our understanding of the full audiological profile of the participants. Lastly, it was not possible for us to differentiate between hearing aid uptake and use or to evaluate the frequency of hearing aid use in our study.
Conclusion
For the first time, this study has used a theory-informed framework to investigate predictors of hearing aid use in a sample of people with dementia and hearing loss. Our study revealed that greater self-perceived hearing difficulty, higher cognitive ability, and more severe hearing loss increase likelihood of hearing aid use among people with dementia. Adapting interventions to account for psychological capability, physical opportunity, and reflective motivation may better support hearing aid use in people with dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Constance Owens Charitable Trust; the National Institute of Health and Care Research Manchester Biomedical Centre [BRC-1215-20007]; the National Institute for Health and Care Research Greater Manchester Patient Safety Research Collaboration; the European Union’s Horizon 2020 research and innovation program [Grant 668648]; and the Global Brain Health Institute.