
Abstract
This study assessed the Stay Strong, Stay Healthy (SSSH) level two resistance training program in 406 older adults (69.3 ± 8.1 years). SSSH included 10 exercises completed during 60 minute sessions, which were offered twice weekly for eight weeks. 30-second sit-to-stand (30STS), timed-up-and-go (TUG), flexibility, and balance poses were completed pre/post-SSSH. Paired t-tests with Bonferroni corrections showed the whole group improved 30STS, TUG, flexibility, and total balance scores over time (p < .001). Repeated measures analyses of variance showed both geography and age groups improved 30STS, TUG, flexibility, and total balance scores over time (all time effects p ≤ .039). Independent t-tests showed rural participants improved to a similar or greater absolute extent than their urban neighbors for nearly all measures and all age groups improved to a similar absolute magnitude over time. This study demonstrates SSSH level two improves physical function in older adults and these benefits are similar across geography and age groups.
• Past research indicates rural populations experience more falls each year than their urban neighbors. SSSH level two, a progressive exercise program, may attenuate this gap by improving measurements associated with fall risk such as dynamic postural change, flexibility, and balance. • A well-designed, progressive exercise program may lead to continued adaptation to physical function in both rural and urban dwelling older adults and across age groups from the 60s, 70s, and 80s+.
• Fall prevention exercise programs should incorporate progressive levels because active older adults may continue improving measures associated with fall risk. • SSSH level two may be disseminated across varied geographic locations and among older adults of varying ages to improve factors associated with fall risk.What this paper adds
Applications of study findings
Introduction
Aging is a complex biological process that contributes to the degradation of physical function (Villareal et al., 2011). This loss in function often begins around the fifth decade of life and is a product of reduced muscular strength and cardiorespiratory fitness decrements, further diminishing balance, strength, and flexibility, all of which are important to maintain independence and combat fall risk (Casteel et al., 2018). Approximately one in four older adults aged 65 years and older will experience a fall, with up to 60% of these falls resulting in injury (Burns & Kakara, 2018). Unfortunately, those who reside in rural counties, defined as having a population of <50,000 (Ratcliffe et al., 2016), report a greater frequency of falls than their urban neighbors (Smith et al., 2018). This geography-related discrepancy in falls incidence is multifaceted. For instance, there is a lack of personalized education about falls in rural communities (Taylor et al., 2019). Furthermore, many exercise programs shown to reduce fall risk, such as those utilizing resistance training (RT), are often unavailable in rural areas (Boehm et al., 2013). Additionally, agricultural workers, many of whom reside in rural areas, experience one of the highest occupation-related fall rates, further contributing to this discrepancy (Rosecrance et al., 2006).
Exercise programs which include RT have been shown to be an effective way to reduce age-related loss of physical function, improving many factors associated with falls (Crowe & Ball, 2015) such as enhancing muscle capacity and bone health (Ball et al., 2013; Foster & Armstrong, 2018; Giangregorio et al., 2014; Guizelini et al., 2018), reducing cardiometabolic risk factors (Beavers et al., 2018), improving sleep quality (Baker et al., 2020; Yang et al., 2012), health-related quality of life (Wanderley et al., 2015), and self-confidence (Dionigi, 2007; Royse et al., 2023). Furthermore, community-based exercise programs allow for better socialization which may increase adherence (Farrance et al., 2016) and combats rates of mental health issues by reducing feelings of depression (Seino et al., 2019). Despite these benefits, most community-based exercise programs are not offered in rural locations, may only be efficacious for younger aging adults (e.g., 50–60 years of age instead of 70–80+ years), and do not include multiple progressive levels.
One community-based exercise program that addresses these shortcomings is the Stay Strong, Stay Healthy (SSSH) resistance training program. A vast body of literature demonstrates SSSH level one significantly improves muscular strength and flexibility, gait, static and dynamic balance, body composition, and sleep quality in older adults (Baker et al., 2020, 2021a, 2021b; Ball et al., 2013; Crowe & Ball, 2015; Syed-Abdul et al., 2022; Syed-Abdul & Ball, 2021). Furthermore, Baker et al., 2021a showed that in 388 participants the program improved dynamic postural control, lower body flexibility, and static balance similarly in adults across different geographic locations (urban vs. rural) and different age groups (50–59; 60–69; 70–79; 80–89). However, despite initial functional performance improvements in SSSH and other similar programs, participants engaging in any exercise program, older adults included, require progression to experience additional benefit. Exercise programs without multiple levels and specific progression schemes often result in participants’ experiencing training plateaus (Gelman et al., 2022). As such, SSSH has since developed a second level to ensure progression and has been successfully implemented to thousands of participants already, residing in both urban and rural areas. Despite this widespread dissemination and anecdotal evidence of the program’s success, it has yet to be evaluated for general efficacy, or if it works similarly in urban and rural communities and across age groups. This is especially important as advancing decades of life are often marked with reduced exercise capacity and SSSH level two might benefit certain age groups differently as not all exercise programs are efficacious in all age groups (Distefano & Goodpaster, 2018).
The three aims of this study were to: (1) assess if the 8-week SSSH level two program would improve functional health in older adults, (2) describe any divergent effects of the program based on rural or urban programming, and 3) determine if the program was efficacious across age groups. It was hypothesized that all participants would benefit from eight week SSSH level two participation. Additionally, it was hypothesized that the degree of improvement would be similar between rural and urban populations, and between age groups.
Materials and Methods
Participants
From 2018 to 2021 the SSSH program was offered throughout Kansas and Missouri. These geographical areas were located across 22 urban counties and 56 rural. These rural counties have <50,000 residents but were often considered agricultural hubs in both states (Ratcliffe et al., 2016). Retrospective access to these data was approved by the University of Missouri Institutional Review Board (#2031903) in 2022. SSSH instructors used flyers, word of mouth, and multimedia advertisements throughout the 78 counties to recruit participants. In total, 406 participants aged 60–91 years old completed all testing for pre- and post-SSSH level two and were grouped based on geographical location (urban, n = 225; rural, n = 179) and age groups (60–69 yrs, n = 188; 70–79 yrs, n = 140; 80 + yrs, n = 42) as shown in Figure 1. For the geographic location analyses, two participants were excluded for missing county data. For the age group analyses, 36 participants were excluded for missing data or being younger than 60 years old. Study design and participant flowchart.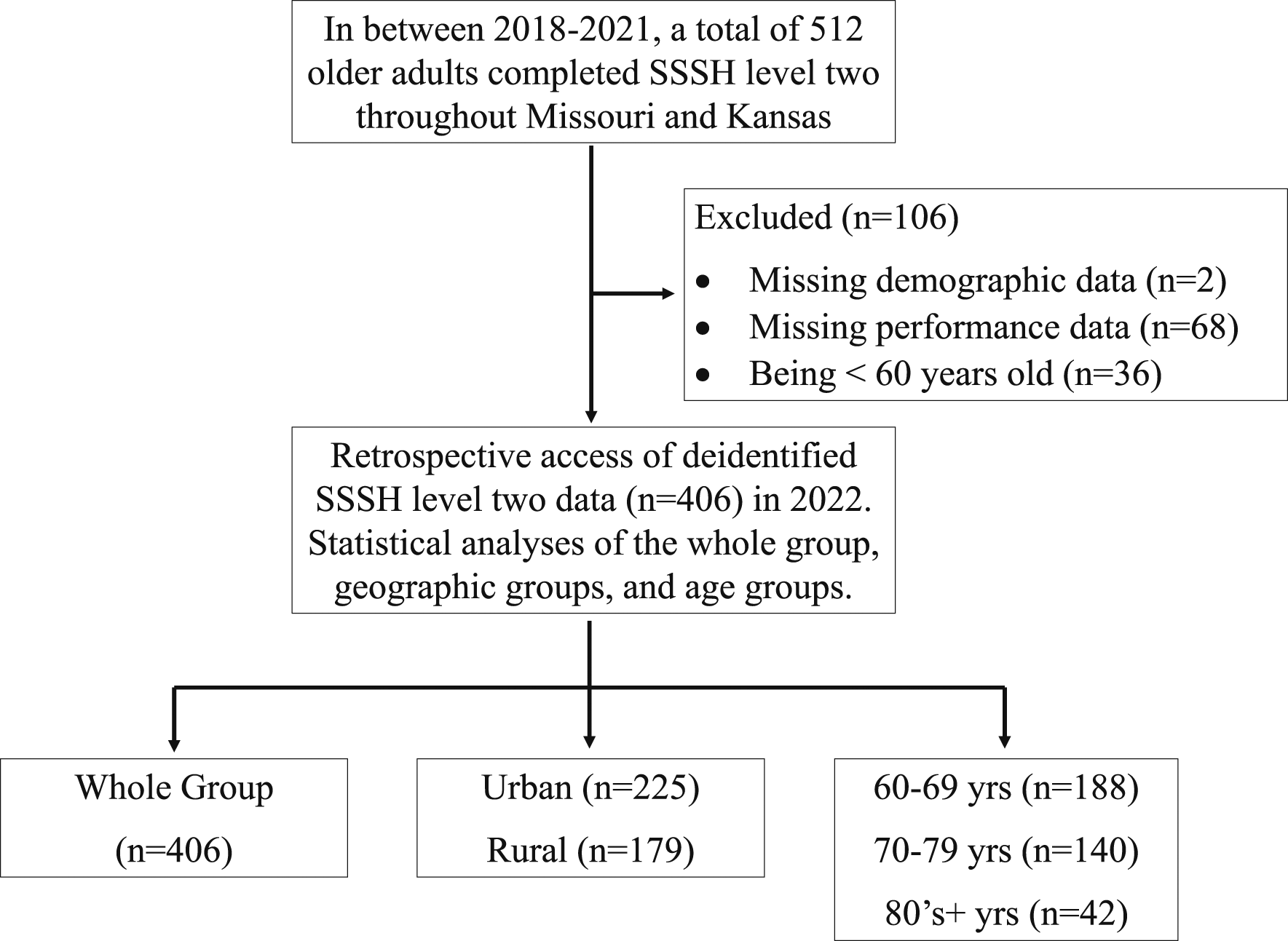
Stay Strong, Stay Healthy Programming
SSSH level two included participants meeting in-person two times per week for 60 minutes for eight weeks, with each session beginning with a warm-up and ending with a cool-down. The warm-up period lasted eight to nine minutes and included aerobic activities like marching, walking, side-steps, quarter squats, and dynamic and static stretching of the major muscle groups. Next, one seated exercise, three lying exercises, and six standing exercises were performed using a 2:4 second tempo. The exercises included the hovering wide leg squat, lying hip bridge, lying side leg raise, small hops, triceps pushup, biceps curl, side arm raise and upright row combination, standing bent-over row, lying opposite arm and leg raise, and seated oblique crunch as shown in Figure 2. If participants could not initially complete exercises on the ground, a standing option was provided. For example, the laying side leg raise would be replaced with a standing side leg raise using the chair for stability. All classes ended with a five to six-minute cool-down period which included light stretching and breathing exercises. All instructors completed formal training from the SSSH program and followed the progression chart detailed in Figure 2. All 10 exercises used throughout the eight week level two SSSH classes are on the left. The progression chart used during the 8 week level two SSSH classes is on the right.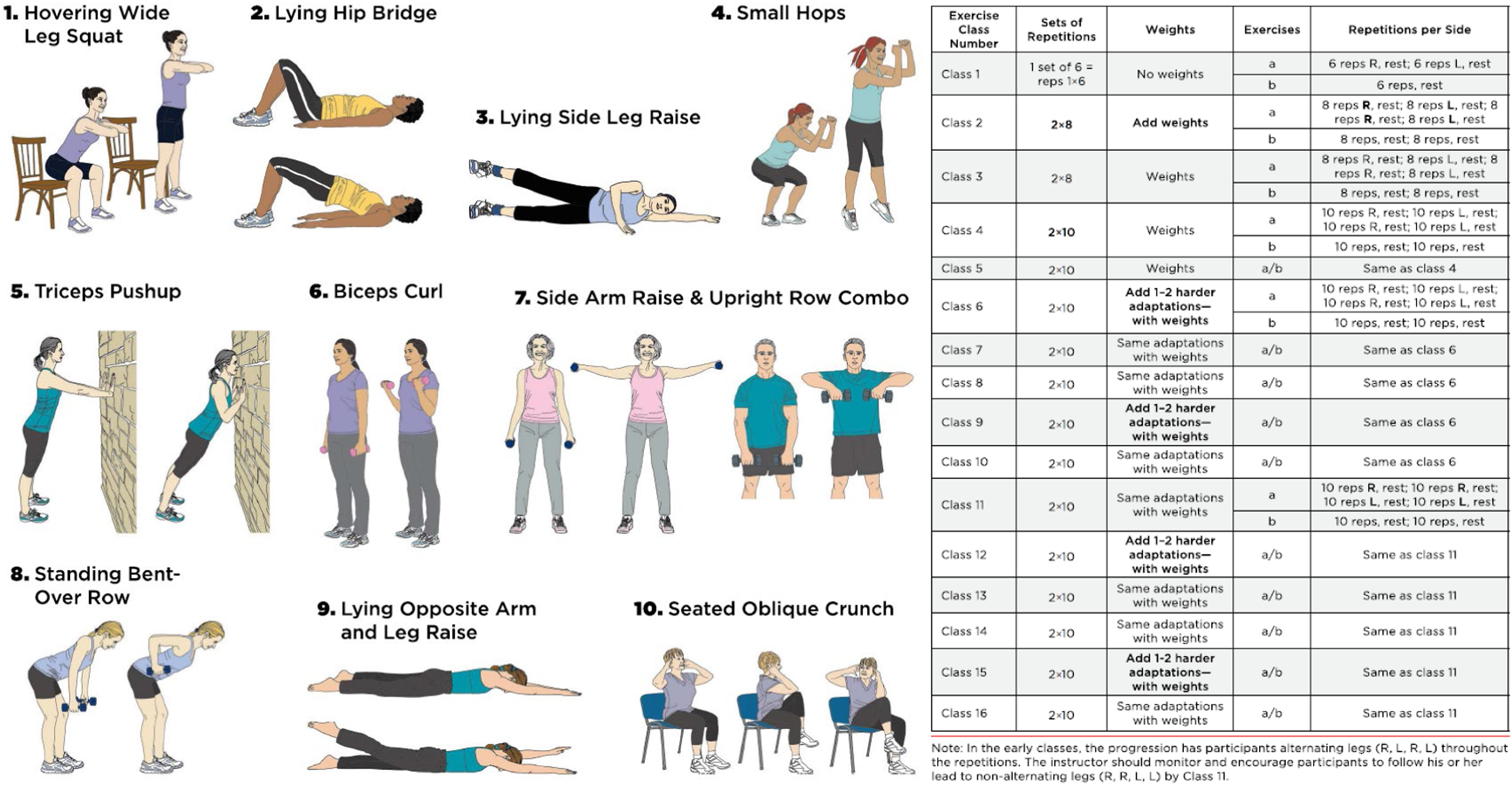
Functional Assessments
Participants completed pre/post-SSSH level two program functional assessments that tested lower body strength, gait, flexibility, and balance as previously described (Baker et al., 2020; Ball et al., 2013; Crowe & Ball, 2015). The 30 second sit-to-stand (30STS) was measured as the number of full chair-stands a participant completed in 30 seconds. The 30STS assesses lower body power, strength, dynamic balance, and coordination and was only attempted once. The eight-foot timed-up-and-go (TUG) was measured as the time in seconds it took a participant to rise from a chair, walk around a marker eight feet away at a self-selected pace, and return to the seated position. The TUG measured balance, gait speed, and coordination and was only attempted once. Both of these validated dynamic postural change tasks were included due to their strong clinical and statistical relationships with fall risk in older adults (Kahraman et al., 2020; Rose et al., 2002). Upper and lower body flexibility was tested using the back-scratch test (BS) and the seated Sit-n-Reach (SnR) test. Both BS and SnR were measured three times for each limb, averaged across limbs, and were measured in inches. Lastly, six balance tasks were completed for up to 10 seconds each. These poses included (1) mountain; (2) tandem without challenge; (3) tandem with eyes closed (EC); (4) tandem with eyes closed and with a head turn (EC + HT); (5) single leg stance without challenge; and (6) single leg stance with EC. Static balance tests have long been used as a proxy for fall risk (Dominguez, 2020) but dual-tasks have been shown to be stronger predictors of fall risk (Commandeur et al., 2018). As such, the current study incorporated both single- and dual-task balance tests. Participants’ total balance scores could range from 0 to 60, with a 60 indicating they successfully held all six poses for the full 10 seconds. Each SSSH instructor was trained on the correct methodology for collecting these pre/post measures by certified SSSH master trainers. They also completed quarterly check-ups with master trainers both virtually and in-person. Per Baker et al., 2020, the interclass coefficient ranges from 0.948 to 0.967 over separate days of testing by SSSH instructors, demonstrating effective training and a high degree of reliability.
Statistical Analyses
All statistical procedures were performed using IBM SPSS (v26, Armonk, New York). When considering how all participants changed over time, paired t-tests with a Bonferroni correction for multiple comparisons was used. The newly adjusted α = .004 was calculated by dividing the original alpha (.05) by the number of comparisons (11). When considering specific grouping based on geographic location, age group, or sex, unique statistical methods were used. First, rural and urban groups were compared at baseline using an independent t-test framework with α = .05. A 2 × 2 repeated measures analyses of variance (ANOVA) was used to analyze geographic location × time interactions and main effects for group or time. Second, baseline comparisons of age groups (60s, 70s, and 80s+) were completed using one-way ANOVA with Bonferroni post-hoc procedures, α = .05. Next, a 3 × 2 repeated measures ANOVA was used to analyze age group × time interactions and main effects for age group or time. Significant interaction models were further decomposed using one-way ANOVA and Bonferroni post-hoc procedures. Two of the balance tasks (tandem + EC + HT and single leg + EC) were rarely attempted by those in the 80s+ age range with sample sizes being less than five. For these measures a 2 × 2 repeated measures ANOVA was used to analyze age group (60s vs. 70s) × time interactions and main effects for group or time. Absolute change scores were also compared between geography groups using an independent t-test framework and one-way ANOVA for age groups. Lastly, baseline and absolute changes for all measures were compared between sexes (females; n = 375 and males; n = 31) using an independent t-test framework with α = .05; however, due to the disproportionate sample size, these analyses are only exploratory and should be interpreted with caution.
Results
Performance Comparisons for the Whole Group and Males and Females Over Time.
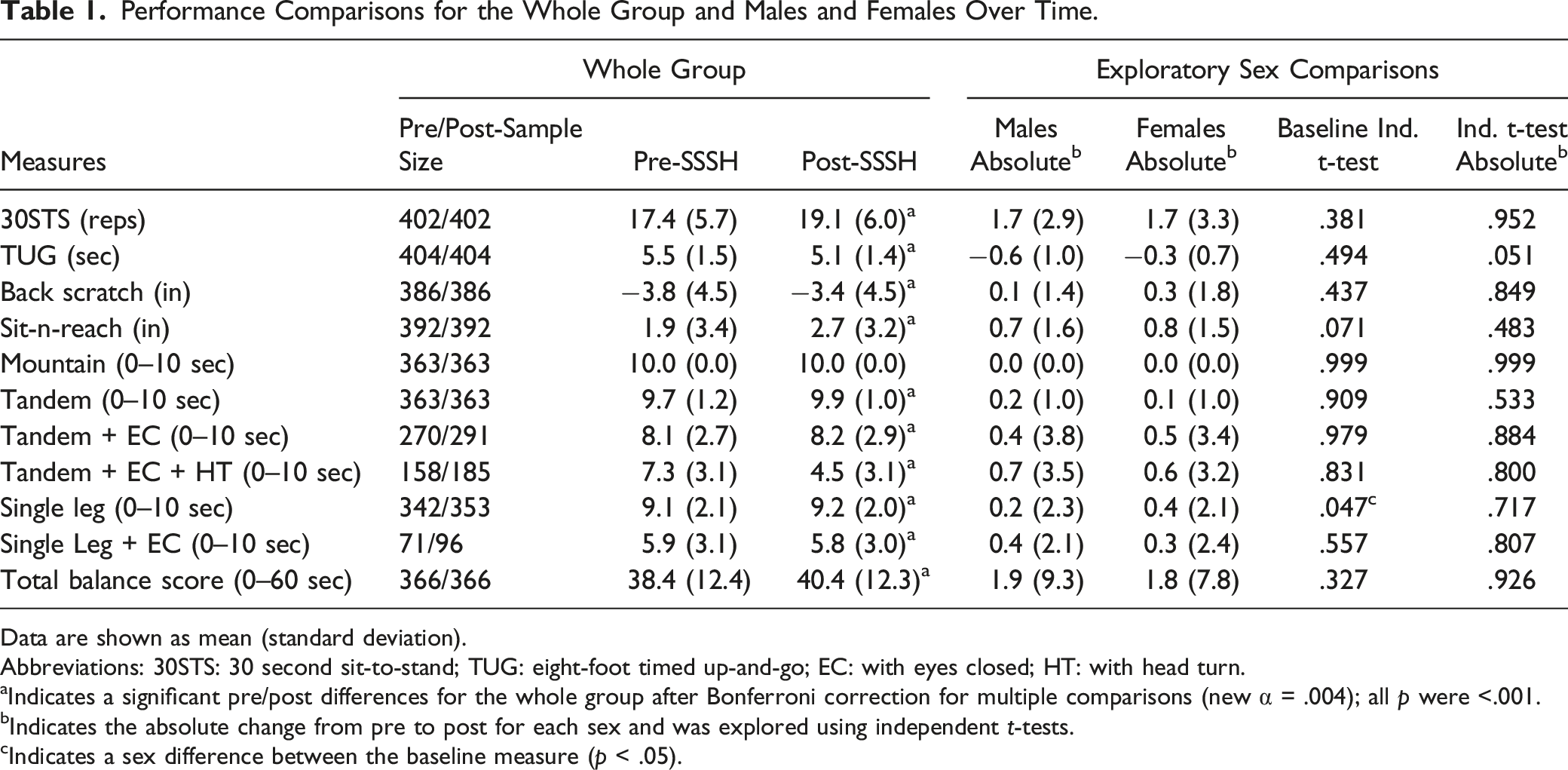
Data are shown as mean (standard deviation).
Abbreviations: 30STS: 30 second sit-to-stand; TUG: eight-foot timed up-and-go; EC: with eyes closed; HT: with head turn.
aIndicates a significant pre/post differences for the whole group after Bonferroni correction for multiple comparisons (new α = .004); all p were <.001.
bIndicates the absolute change from pre to post for each sex and was explored using independent t-tests.
cIndicates a sex difference between the baseline measure (p < .05).
Comparison of Functional Measures Between Geography Groups.
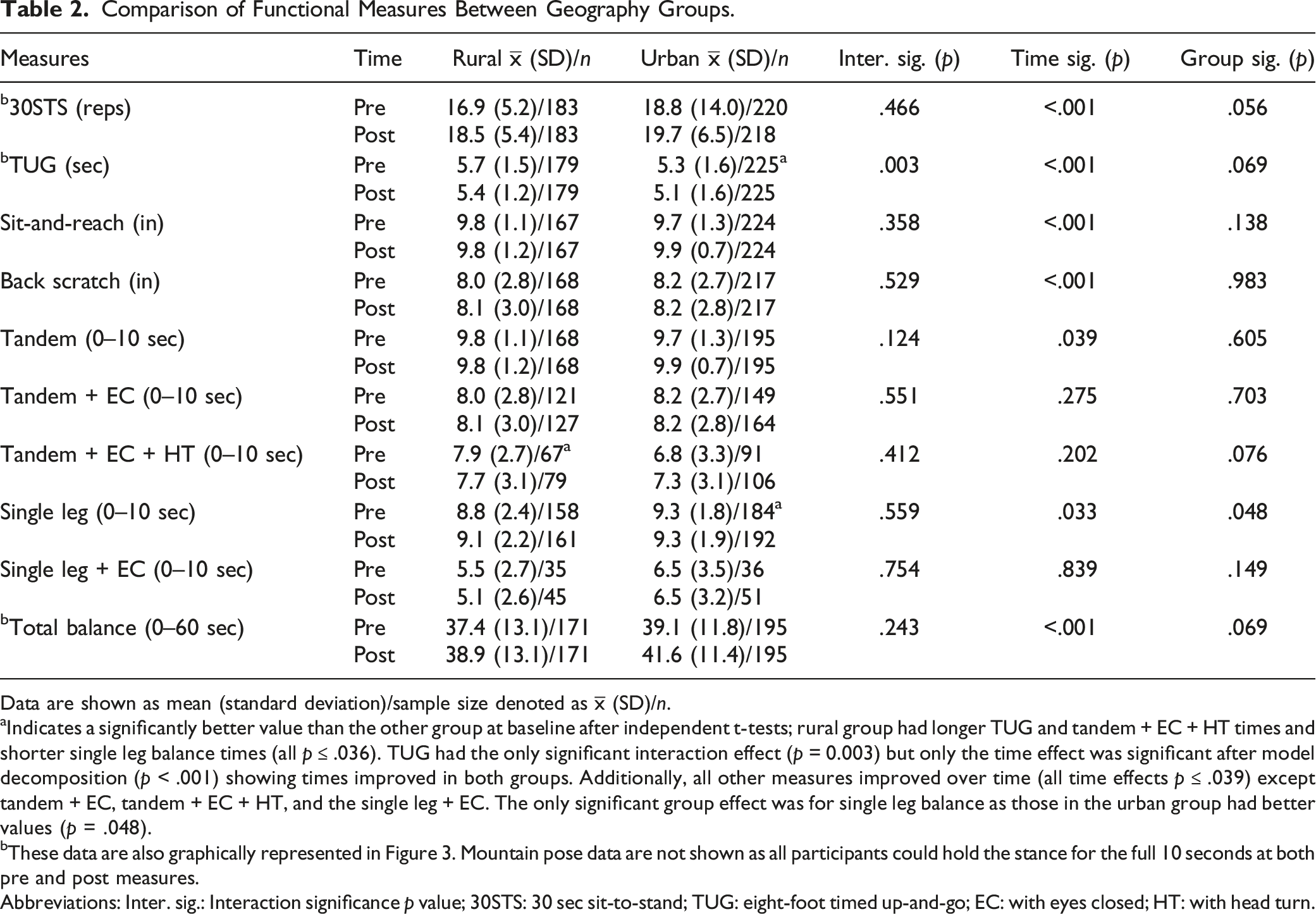
Data are shown as mean (standard deviation)/sample size denoted as
aIndicates a significantly better value than the other group at baseline after independent t-tests; rural group had longer TUG and tandem + EC + HT times and shorter single leg balance times (all p ≤ .036). TUG had the only significant interaction effect (p = 0.003) but only the time effect was significant after model decomposition (p < .001) showing times improved in both groups. Additionally, all other measures improved over time (all time effects p ≤ .039) except tandem + EC, tandem + EC + HT, and the single leg + EC. The only significant group effect was for single leg balance as those in the urban group had better values (p = .048).
bThese data are also graphically represented in Figure 3. Mountain pose data are not shown as all participants could hold the stance for the full 10 seconds at both pre and post measures.
Abbreviations: Inter. sig.: Interaction significance p value; 30STS: 30 sec sit-to-stand; TUG: eight-foot timed up-and-go; EC: with eyes closed; HT: with head turn.
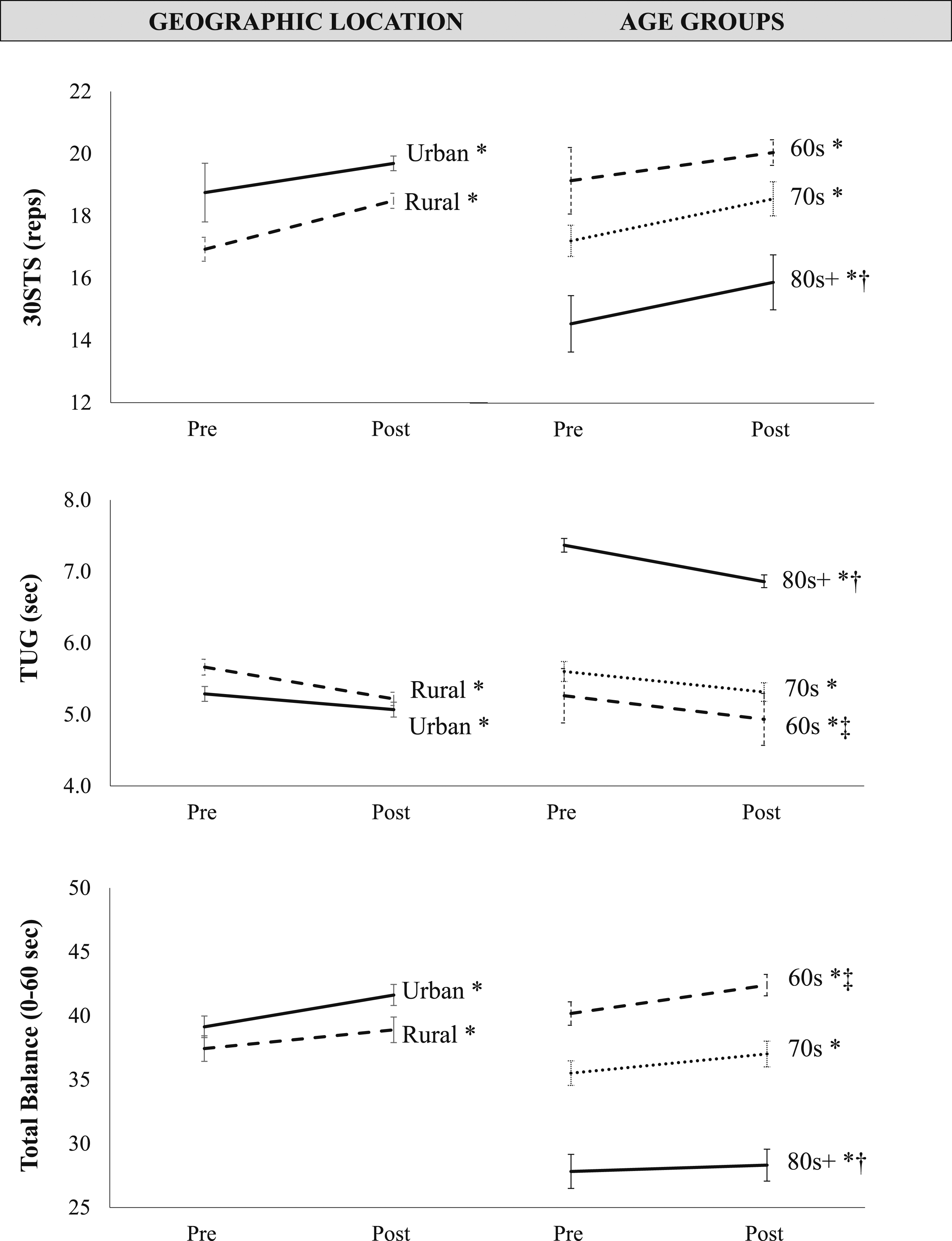
The left panels show rural and urban group differences for the 30STS (top), TUG (middle), and total balance scores (bottom). All three measures improved over time (* all time effects p < .001) and were similar between those who lived in urban or rural counties (all group effects p ≥ .056). The right panels show age group differences for the 30STS (top), TUG (middle), and total balance scores (bottom). All three measures improved over time (* all time effects p ≤ .008) and those in their 80 s + had worse scores than those in their 60 s and 70 s († all post-hoc p ≤ .006). Additionally, those in their 60 s had better TUG and total balance scores than those in their 70 s (‡ both post-hoc p ≤ .029).
Comparison of Functional Measures Between The Age Groups.
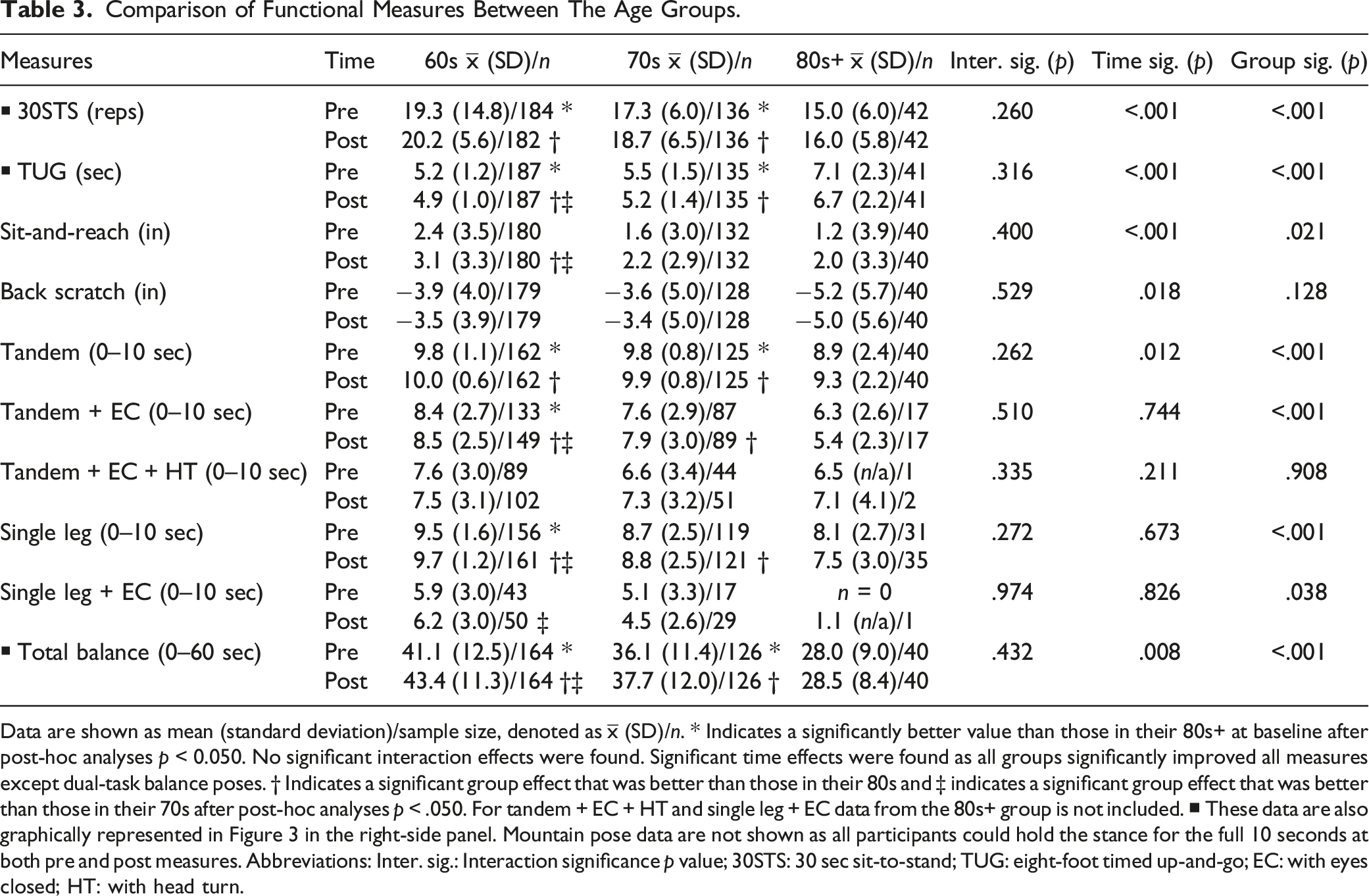
Data are shown as mean (standard deviation)/sample size, denoted as
Number of Participants in High-Risk Categories for Falls Over Time.
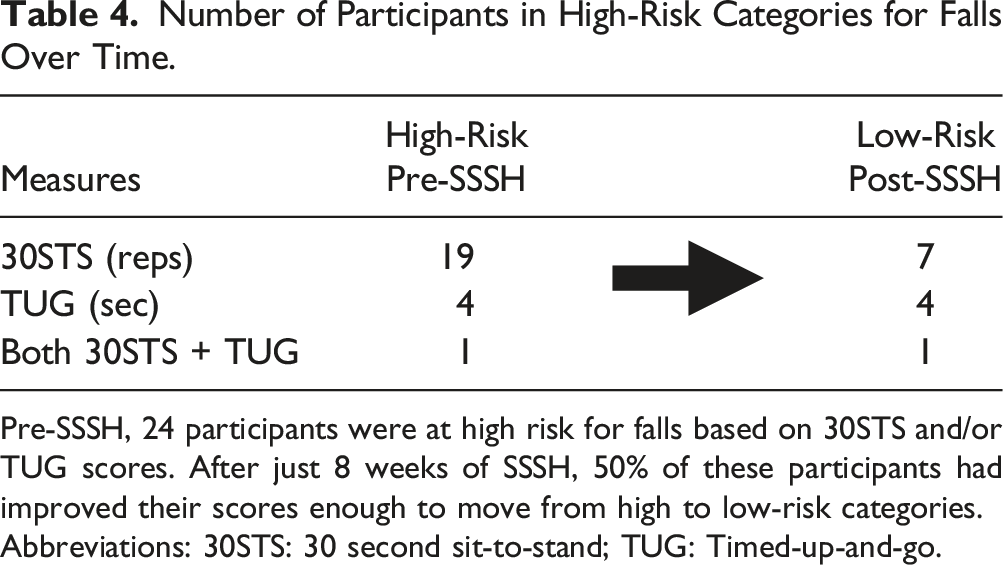
Pre-SSSH, 24 participants were at high risk for falls based on 30STS and/or TUG scores. After just 8 weeks of SSSH, 50% of these participants had improved their scores enough to move from high to low-risk categories.
Abbreviations: 30STS: 30 second sit-to-stand; TUG: Timed-up-and-go.
Discussion
This study demonstrated that the progressive SSSH level two program improved physical function measures associated with a reduction in fall risk in older adults. This was made evident by the enhanced ability to perform dynamic postural change movements, single- and dual-task balance tests, and flexibility post-SSSH level two participation. Furthermore, the degree of improvement was similar between rural and urban populations and between age groups, indicating the SSSH level two program may be well-suited for wider dissemination.
Many participants were in good physical condition before SSSH level two participation due to prior completion of the effective SSSH level one program. Despite the well documented improvements participants experienced from SSSH level one, participants in the current study continued to improve physical function measures which are associated with fall risk. For instance, at baseline 24 participants were considered at high-risk for falls based on their 30STS and/or TUG scores (CDC, 2018; Rose et al., 2002); however, after just eight weeks of SSSH level two participation, half of these participants had moved into a low-risk category, including the one participant who was at the greatest risk of falls. Additionally, the degree of instability during balance tasks is another indicator for fall risk (Crenshaw et al., 2018; Dominguez, 2020). In the present study, participants improved both single- and dual-task balance test performance for nearly all measures. Lastly, total balance scores, which were an aggregate of the six standing balance tasks, improved by 5.3%. These findings demonstrate SSSH level two participation might continue enhancing dynamic postural change and standing balance performance further decreasing fall risk.
Participation in the SSSH level two program also led to continued improvements in upper and lower body flexibility. These increases in flexibility may reduce fall risk because there is an inverse relationship between increasing joint mobility which reduces fall risk in older adults (Geremia et al., 2015). For instance, Emilio et al. (2014) found that focusing the flexibility training on the lower body musculature that surrounds the hips may offer even more protection against falls, so the 0.76 inch increase in SnR performance is statistically significant but may also have clinical significance.
There are many health discrepancies and/or barriers that exist between rural and urban older adults which can impact their physical function. For instance, both Baker et al. (2021a) and Smith et al. (2012) compared rural and urban participants before and after eight week fall prevention programs. Both found that rural participants started and ended the interventions with scores that were significantly below their urban neighbors. However, Baker et al. (2021a) specifically, observed that despite the lower scores, rural participants improved to a greater extent in many categories suggesting the physical function gap was narrowed with SSSH level one participation. In the current study, rural participants had reduced TUG and single leg balance, but better tandem + EC + HT than their urban neighbors at the pre-testing session. Despite these baseline differences, both groups were similar for all other measures at the pre-testing session suggesting the physical function gap may have been reduced from SSSH level one to SSSH level two. Support for this hypothesis comes from Miller et al. (2022) who completed a 12-month follow-up study with 388 SSSH level one participants. They found that previously sedentary older adults who completed their first SSSH level one program were able to create and sustain highly active exercise habits despite COVID-19 restrictions even one year later. Perhaps, those in rural communities were able to maintain the positive momentum they gained during SSSH level one and continued engaging in more exercise and physical activity prior to enrollment in the current study. These data suggest SSSH may be an effective tool to reduce fall risk in rural areas. More follow-up studies investigating how older adults respond after SSSH participation are needed to understand if there is a difference between participants who reside in rural and urban locations and if those who have high occupational fall risk, such as those in rural agriculture, can benefit from SSSH participation.
Another factor to consider is age, as older adults of advanced age have significantly more health disparities than younger populations, often reducing exercise capacity (Distefano & Goodpaster, 2018). In the present study, those in the 80s+ group had worse pre/post 30STS, TUG, tandem, and total balance performance, while those in their 60s had better pre/post single leg and tandem + EC. These findings support the well-established age-related declines in physical function that have been previously documented. For instance, Milanović et al. (2013) who found in 1288 participants (60–69, n = 703; 70–80, n = 585) that the reductions in BS and SnR, TUG, 30STS, arm curl, and two-minute step test performance were the result of the aging process. Despite the aging process reducing performance values, all age groups in the present study improved 30STS and TUG, upper and lower body flexibility, tandem and total balance to a similar extent, demonstrating SSSH level two’s ability to continue improving active older adults’ physical function. As physical activity is one of the best ways to combat age-related declines, SSSH and other evidence-based community exercise programs should be utilized.
There are a few key limitations to consider for future research. The lack of a control group makes it difficult to distinguish selection effects from treatment effects. Past efforts have utilized a randomized controlled trial design for SSSH level I, which will also be repeated for SSSH level II now that its efficacy has been suggested in this study. Also, the more challenging dual-task balance tests such as tandem + EC, tandem + EC + HT and single leg + EC may be better at predicting those who are at fall risk and more participants felt confident enough to attempt these tasks after SSSH level two participation, but those in the 80s+ group rarely attempted these tasks. This indicates these tests may not be suitable for this advanced age group and other tests are needed to assess if dual-task balance improves after SSSH level two. Another limitation is the findings reveal significant improvements in measures that are correlated with fall risk; however, fall incidence was not directly assessed and no long-term follow-up was conducted. Our team has recently published 12-month follow-up data with other SSSH level one participants (Miller et al., 2022) and are working on doing the same in SSSH level two participants. Next, at the time these data were generated the SSSH program did not collect any demographic data such as ethnicity, anthropometrics, or other factors that may be associated with the magnitude of improvement. All current investigations now collect these data to address this limitation. Lastly, the principle of progressive overload suggests that a SSSH level three is required in order to mitigate training plateaus. Our team has begun research on new programming, which will include highly scalable movements incorporating new speeds, resistance levels, and movement patterns to ensure older adults continue to benefit from SSSH participation.
Conclusion
In conclusion, the progressive SSSH level two program significantly improves dynamic postural change, balance task, and flexibility performance over time and similarly between rural and urban populations and various age groups. These data support SSSH level two’s widespread implementation.
Footnotes
Acknowledgments
The authors would like to specifically thank the following team members who were instrumental in program offering and data collection: Elena Doctor, Leslie Bertsch, Emily Barbee, Melissa Cotton, Denise Sullivan, Bethany Bachmann, Linda Zimmerman, and Debbie Bennett. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.