
Abstract
Language-based strategies are recommended to improve coherence, clarity, reciprocity, and continuity of interactions with persons living with dementia. Person-centered care is the gold standard for caring for persons with dementia. Person-centered communication (PCC) strategies include facilitation, recognition, validation, and negotiation. Little is known about which language-based strategies support PCC in home care. Accordingly, this study investigated the overlap between language-based strategies and PCC in home care interactions. Analysis of conversation of 30 audio-recorded interactions between personal support workers (PSWs) and persons living with dementia was conducted. The overlap between PCC and language-based strategies was analyzed. Of 11,347 communication units, 2578 overlapped with PCC. For facilitation, 21% were yes/no questions. For recognition, 25% were yes/no questions and 22% were affirmations. For validation, 81% were affirmations and positive feedback. Finally, 60% were yes/no questions for negotiation. The findings highlight the person-centeredness of language-based strategies. PSWs should use diverse language-based strategies that are person-centered.
Keywords
• Language-based strategies that support the person-centered goals of facilitating, recognizing, validating, and negotiating with a person living with dementia are outlined. • Language-based strategies that may contribute to missed opportunities for person-centered communication are outlined. They highlight common pitfalls during communication with persons living with dementia and how to avoid them. • Naturalistic interactions between home care workers and persons living with dementia were analyzed, thus providing insight into the communication experiences observed during home care.
• Language-based strategies that support multiple goals related to effective communication and personhood can be integrated into communication training and education for caregivers. • Insights provided on language-based strategies that contribute to missed opportunities for person-centered communication can add helpful considerations to communication skills training. • Home care workers are encouraged to use a more diverse set of language-based strategies that support person-centered communication.What this paper adds
Applications of study findings
Introduction
Dementia is as a chronic, progressive major neurocognitive disorder that affects cognitive functioning and memory processes (5th ed.; DSM-5; American PsychiatricAssociation, 2013). Language functions deteriorate over time resulting in speech, language, and comprehension difficulties, including a possible decline in naming abilities, fluency issues, loss of creative language use, and difficulty understanding rapid or complex speech (Eggenberger et al., 2013; Santo Pietro & Ostuni, 2003).
Ensuring effective communication can be challenging for formal caregivers who enter an interaction without a nuanced understanding of the communication abilities of the person living with dementia. The Communication Predicament of Aging Model highlights that a reliance on age-associated stereotypes can result in communication behaviors that are detrimental to the well-being of older adults (Ryan et al., 1986). However, when communication opportunities are harnessed appropriately, the person living with dementia can partake in a reciprocal interaction that promotes meaningful expression (Acton et al., 2007; Morris et al., 2020). Accordingly, the Communication Enhancement Model stipulates that older adults can be supported when caregivers employ communication modifications rooted in a consideration of the person living with dementia, their communicative intentions, and the environment (Ryan et al., 1995).
Personal support workers (PSWs) provide the bulk of formal dementia care in long-term care and home care settings (Home Care Ontario, 2018). Older adults overwhelmingly want to age at home. For instance, 93% of Home Care Ontario survey respondents indicated their desire to stay at home with none identifying long-term care in their future housing plans (Home Care Ontario, 2020). Thus, it is essential that the home care workforce is skilled and trained effectively to meet the growing demands. Currently, there is inadequate dementia-specific and communication-related training in PSW formal education and training (Savundranayagam et al., 2020). Communication interactions can consequently become task-focused, directive, and patronizing (Vasse et al., 2010). Formal caregivers recognize the need for dementia-specific caregiver training (Breen et al., 2021; Flöjt et al., 2014; Morgan et al., 2016; Savundranayagam et al., 2021). Equipping PSWs with evidence-based communication practices that complement the communication abilities of the person living with dementia while accommodating for their communication challenges is necessary. A person-centered and language-based approach to communication can be the pathway to improved care and caregiver-client relationships.
The person-centered care approach was established by Tom Kitwood’s work highlighting the impact of interpersonal relationships on the behaviors associated with dementia (Downs & Collins, 2015; Kitwood, 1997; Savundranayagam & Moore-Nielsen, 2015). Its benefits are especially evident when communication is used as the mechanism to provide person-centered care (Young et al., 2011). Person-centered caregivers respond to individual needs, amplify abilities, and recognize their client as a unique individual, first and foremost (Downs & Collins, 2015; Kitwood, 1997; Savundranayagam & Moore-Nielsen, 2015).
Interactions that are essential to good dementia care and meet clients’ specific psychological needs are termed as “positive person work” (Kitwood, 1997). Indicators of positive person work most relevant to conversational interactions during care are recognition, negotiation, validation, and facilitation (Savundranayagam et al., 2007; Savundranayagam & Moore-Nielsen, 2015). Recognition includes acknowledging the person living with dementia as an individual, including calling them by name and integrating their life story into conversation. Negotiation includes communication that consults on needs, desires, and preferences. Validation includes communication that is feelings-oriented and affirms the person living with dementia. Facilitation includes communication used to initiate and sustain interactions. Missed opportunities for Person-centered communication (PCC) occur where one of the above indicators could have been used to support the client’s personhood, but were absent (Savundranayagam, 2014; Savundranayagam et al., 2007). A missed opportunity alternative occurs when a caregiver uses a non-person-centered alternative during an opportunity to be person-centered. A missed opportunity omission is when a nonresponse or minimal response, such as failing to greet the client or allowing enough time to respond, occurred in place of a person-centered response.
Effective language-based strategies are also recommended for communication with persons living with dementia. Verbatim and paraphrased repetitions, using nouns instead of pronouns, right-branching sentences, positive instructions, and allowing time to respond facilitate comprehension. For example, repetitions can lower demands on working memory capacity instead of limiting communicative opportunities by relying solely on simple sentences (Small et al., 1997). Persons living with dementia also often experience challenges with expressive communication (Acton et al., 2007; Dijkstra et al., 2002; O’Brien et al., 2020; Ramanathan, 1997; Savundranayagam & Orange, 2011, 2014; Tappen et al., 1997). Yes/no questions, unfinished sentence prompts, minimal turns, matching comments, and affirmations can improve expression. For example, yes/no questions accommodate difficulties generating additional information, especially during demanding tasks (Ripich et al., 1999; Small & Perry, 2005).
Language-based strategies can also address refusal of care and resolve communication breakdowns. To prompt collaboration, caregivers can announce activity/intent clearly, ask for permission, and use politeness and affirmations (Bourgeois et al., 2003; Medvene & Lann-Wolcott, 2010; O’Brien et al., 2020; Ramanathan, 1997; Santo Pietro & Ostuni, 2003; Savundranayagam & Moore-Nielsen, 2015; Weitzel et al., 2011; Wilson et al., 2012a, 2013). Verification questions and comments, giving more information, and filling in missing information can help resolve issues related to speech production, language structure/processing, cognition, or hearing (Savundranayagam & Moore-Nielsen, 2015; Savundranayagam & Orange, 2014; Wilson et al., 2012b, 2013) . Addressing the person living with dementia by name/title and using greetings is also recommended (Acton et al., 2007; Bourgeois et al., 2003; Kim & Bayles, 2007; Savundranayagam & Moore-Nielsen, 2015; Weitzel et al., 2011; Wilson et al., 2012a, 2013).
Although PCC and language-based strategies are independently effective, there is little knowledge about which language-based strategies support PCC. This study is a timely follow-up to the research by Savundranayagam and Moore-Nielsen (2015) who investigated language-based strategies used by nursing assistants in the United States of America during interactions with persons living with dementia in long-term care. To bridge present gaps in the literature, the purpose of this study is to investigate the overlap between PCC strategies, missed opportunities for PCC, and effective language-based strategies used in a Canadian home care setting with persons living with dementia.
Method
Participants and Procedure
This study was approved (107789) by the Research Ethics Board at Western University. Routine in-home care interactions between 11 PSWs and their 12 clients living with dementia were audio-recorded in 2018 in London, Ontario in Canada. All participants or their legal substitute decision makers provided written consent to audio-recording of home care interactions. Interactions were recorded at three time points over 15 weeks, resulting in 30 conversations (11 dyads at time 1, 10 dyads at time 2, 9 dyads at time 3). One client moved to long-term care after time 1. Home care interactions between the corresponding PSW and another of their clients with dementia were audio-recorded for time 2 and 3.
All PSW participants were female. 10 participants self-identified as White and one as Black or African-Canadian. PSW participants ranged in age from 21 to 62 years, with a mean age of 47.2 years. The average amount of time spent working in home care was 4.5 years. Most participants (n = 8, 72.7%) provided home care to more than 10 clients. Seven participants living with dementia were female (58.3%) and five were male (41.7%). All 12 participants living with dementia were White. They ranged in age from 77 to 97 years, with a mean age of 87.8 years. Two-thirds of participants were diagnosed with dementia and had probable Alzheimer’s Disease (n = 8, 66.6%). Other participants had suspected Alzheimer’s Disease (n = 2, 18.2%), mild cognitive impairment (n = 1, 8.3%), or vascular dementia secondary to stroke (n = 1, 8.3%).
Data Preparation and Coding
The analysis of conversations following a social psychological approach to the study of interpersonal communication was conducted (Roger & Bull, 1989). Audio-recorded interactions were orthographically transcribed and segmented into communication units or c-units (main clause + subordinate clause) following the Systematic Analysis of Language Transcripts SALT (Miller et al., 2012) conventions.
Through reflexive notes on the nature of each interaction, we determined that half (n = 15) were routine care and half (n = 15) were leisure-based. Interactions focused on routine care activities were classified as routine care interactions. Conversation-based interactions involving activities beyond routine care, such as playing games, taking a walk, or going on a drive, were classified as leisure-based. The duration of interactions ranged from approximately 5 minutes to 3 hours, with leisure-based interactions among the longest. The average number of c-units produced by PSW was approximately 378. The average number of c-units produced by persons living with dementia was approximately 367.
The language-based strategy coding framework and the PCC coding framework guided transcript coding. Only PSW c-units were coded as this study focused on effective communication employed by caregivers. C-units were first coded according to the updated language-based framework (Savundranayagam & Moore-Nielsen, 2015) comprising of 32 effective strategies (please see Supplementary Appendix for complete list). Transcripts were then analyzed for PCC and missed opportunities using an existing codebook (Savundranayagam, 2014; Savundranayagam et al., 2007). C-units that did not receive a code were marked as “Uncoded.” This permitted the representation of PSW c-units that were uncoded under both frameworks or coded under one but not the other.
Reliability of the coding frameworks was established through independent coding of a subset of conversational data (20%) by two trained coders to derive Scott’s pi measure of inter-rater reliability. Scott’s Pi was .97 for the language-based strategy framework and .99 for the PCC framework constituting “almost perfect” agreement between coders (Intercoder Reliability Techniques, 2017).
Data Analysis
Overlap analysis followed protocols established by Savundranayagam and Moore-Nielsen (2015). Language-based strategies corresponding with PCC indicators and missed opportunities were analyzed. This allowed us to investigate the relationship between both sets of communication strategies and whether certain language-based strategies may be implicated in missed opportunities for PCC.
Results
The overlap of language-based strategies with PCC indicators and missed opportunities were analyzed. Figure 1 shows that of 11,347 PSW c-units analyzed, 2578 c-units overlapped with PCC and 433 c-units overlapped with missed opportunities. Language-based strategies overlapped with 39% of all c-units coded as recognition, 95% of all c-units coded as negotiation, 64% of all c-units coded as validation, and 49% of all c-units coded as facilitation. Summary of Results for Overlap Analysis.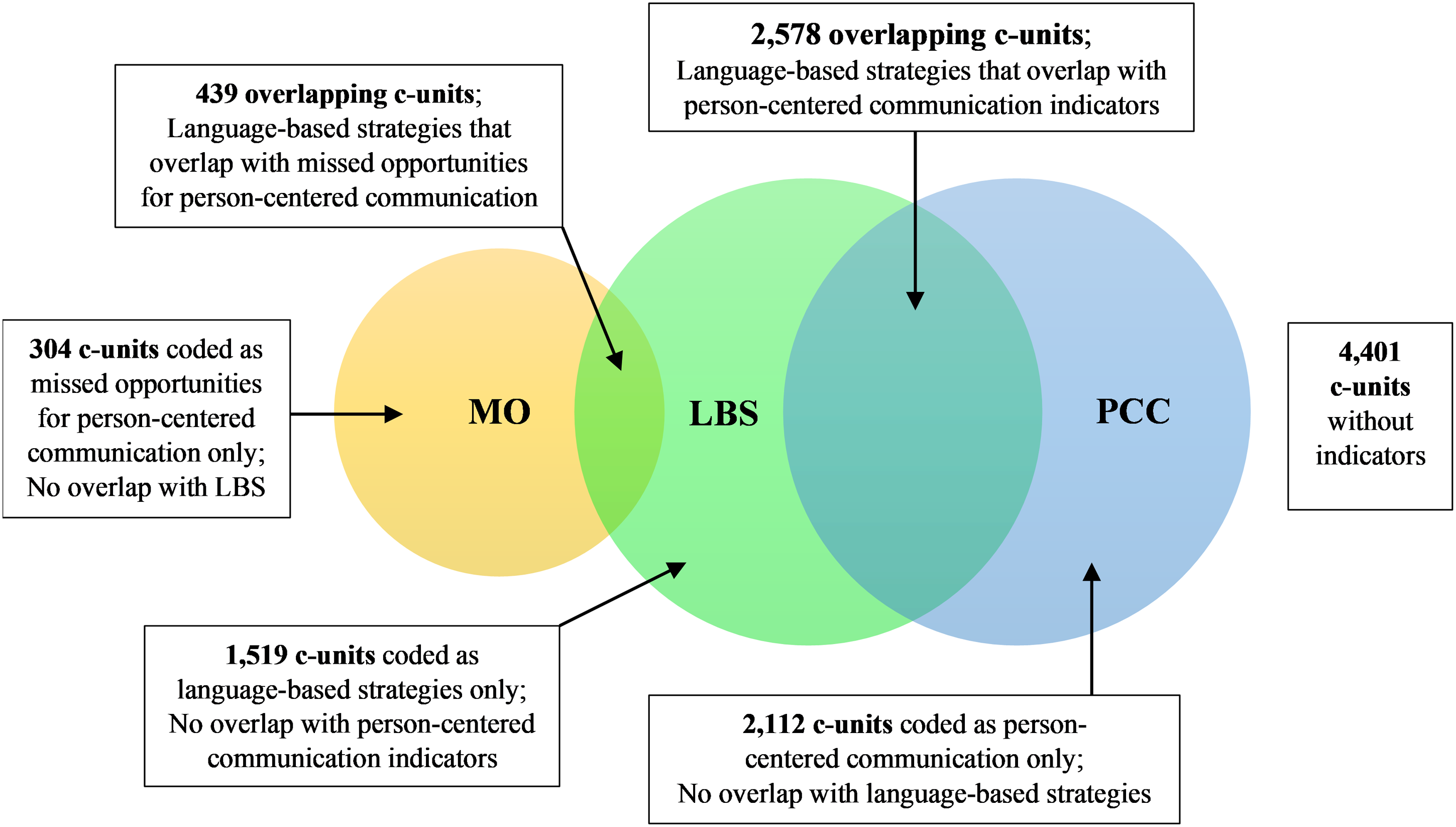
Recognition
Language-based strategies overlapping with recognition at a frequency greater than or equal to 1% are displayed in Figure 2. Frequency of Language-based Strategies Coded as Recognition. Note. YNQ = Yes/no questions; Aff = Affirmations; AddName = Address by name and/or title; Greet; AddName = Greetings and address by name and/or title combination; VerQ; YNQ = Verification questions and yes/no questions combination; MatchC = Matching comments; AnnounceAI = Announcement of action/intent; Greet = Greetings; FLead; YNQ = Focused leads and yes/no questions combination.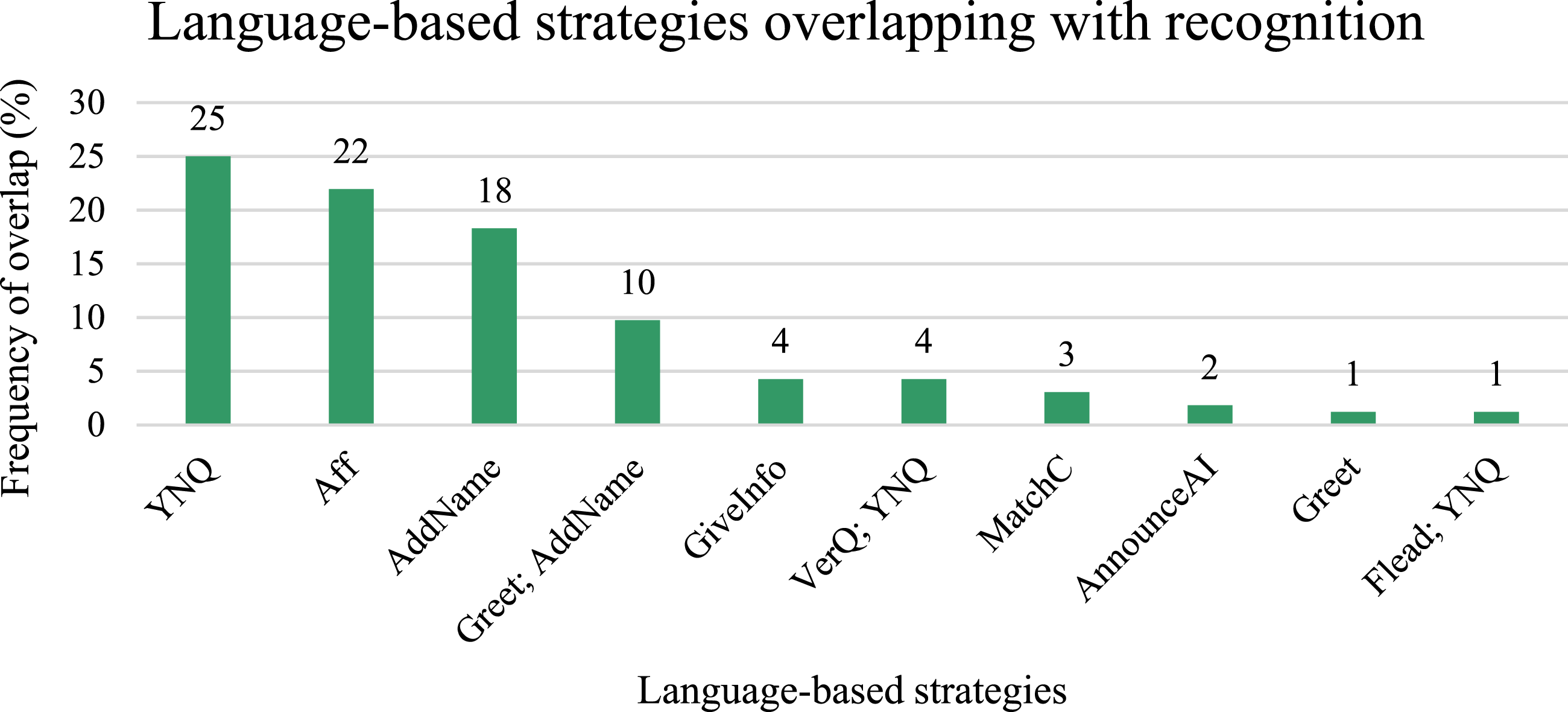
In the excerpt below, the PSW demonstrates recognition by asking a yes/no question that highlights the PSW-client relationship and integrates the client’s life story into the conversation. Client with dementia: But my daughter and her husband likes the way> Client with dementia: She likes camping. [...] Client with dementia: Everyday he wanted to come home to sleep.
Client with dementia: Huh? Personal Support Worker: Lucy’s husband? [Recognition] [Paraphrased Repetition; Yes/No Question] Client with dementia: Yah.
Negotiation
Language-based strategies overlapping with negotiation at a frequency greater than or equal to 1% are displayed in Figure 3. Frequency of Language-based Strategies Coded as Negotiation. Note. YNQ = Yes/no questions; OpenQ = Open-ended questions; ChQ = Choice questions; YNQ; Time = Yes/no questions and allow time to respond combination; ClosedQ = Closed-ended questions; PRep; YNQ = Paraphrased repetition of yes/no questions; VerQ; YNQ = Verification question and yes/no question combination; PerQ; YNQ = Permission question and yes/no question combination; PosIns = Positive instructions; Aff = Affirmations; AnnounceAI = Announcements of action/intent.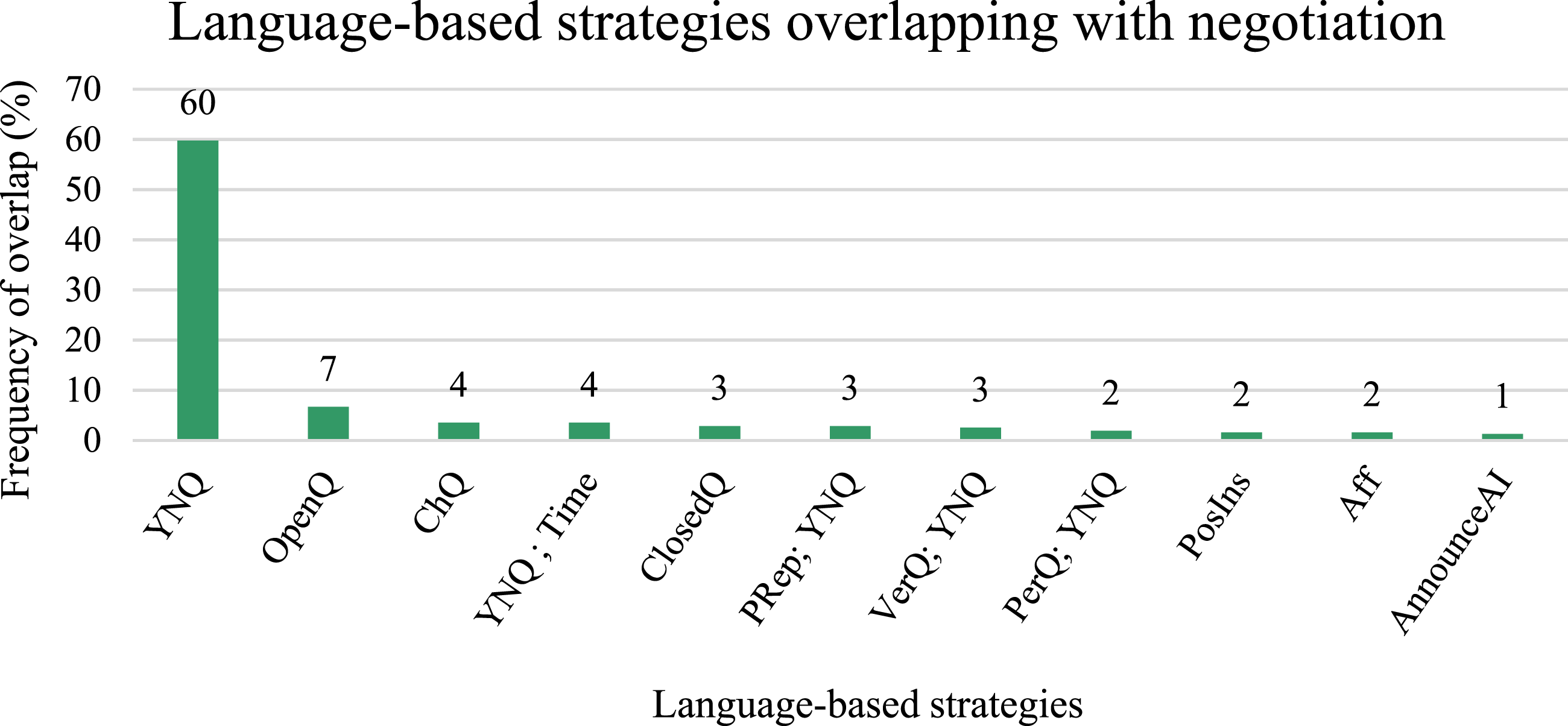
In this excerpt, the PSW negotiates by consulting with the client with dementia on meal preferences and mealtimes using open-ended and yes/no questions.
Client with dementia: Nothing right now.
Client with dementia: No. Personal Support Worker: Okay. Personal Support Worker: Well, I’m back for lunch today. Client with dementia: Okay.
Client with dementia: No, I’ll try to be up. Personal Support Worker: Okay.
Validation
Language-based strategies overlapping with validation at a frequency greater than or equal to 1% are displayed in Figure 4. Frequency of Language-based Strategies Coded as Validation. Note. Aff = Affirmations; PosFB = Positive feedback; MatchC = Matching comments; YNQ = Yes/no questions; Aff; AddName = Affirmations and address by name and/or title combination; AnnounceAI = Announcements of action/intent; PosIns = Positive instructions; News = Newsmarks.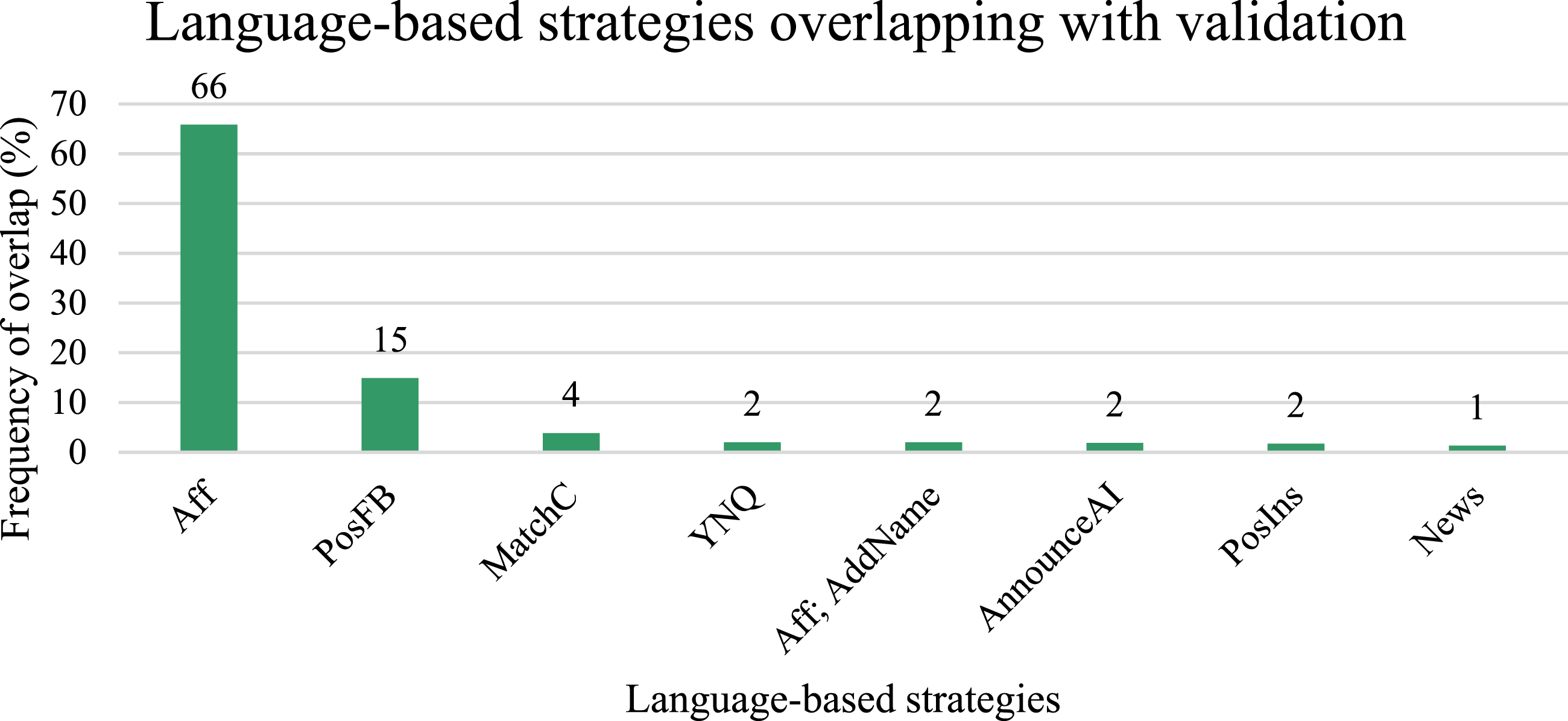
Here, the PSW validates the confusion experienced by the client with dementia using empathy and responding on the feelings level with an affirmation. Client with dementia: I got to go to the Dutch store. Personal Support Worker: Oh today? [Negotiation] [Verification Question; Yes/No Question] Client with dementia: I need cookies. ; :02 second pause Personal Support Worker: Oh but today is Tuesday. [Facilitation] Client with dementia: Yah I know. Client with dementia: It’s not open today? Personal Support Worker: No. […] Client with dementia: Good thing you came in here <because> I was sure that it was today. Personal Support Worker: <Yah!> [Affirmation – Minimal Turn] Personal Support Worker: Yup! [Affirmation – Minimal Turn]
Client with dementia: <Okay.> Client with dementia: Yah.
Facilitation
Language-based strategies overlapping with facilitation at a frequency greater than or equal to 1% are displayed in Figure 5. Frequency of Language-based Strategies Coded as Facilitation. Note. YNQ = Yes/no questions; AnnounceAI = Announcements of action/intent; PosIns = Positive instructions; Aff = Affirmations; MatchC = Matching comments; OpenQ = Open-ended questions; GiveInfo = Give more information; VerQ; YNQ = Verification questions and yes/no questions combination; ClosedQ = Closed-ended questions; Greet = Greetings; News = Newsmarks; PRep = Paraphrased repetitions; VRep = Verbatim repetitions; FLead; YNQ = Focused leads and yes/no questions combination.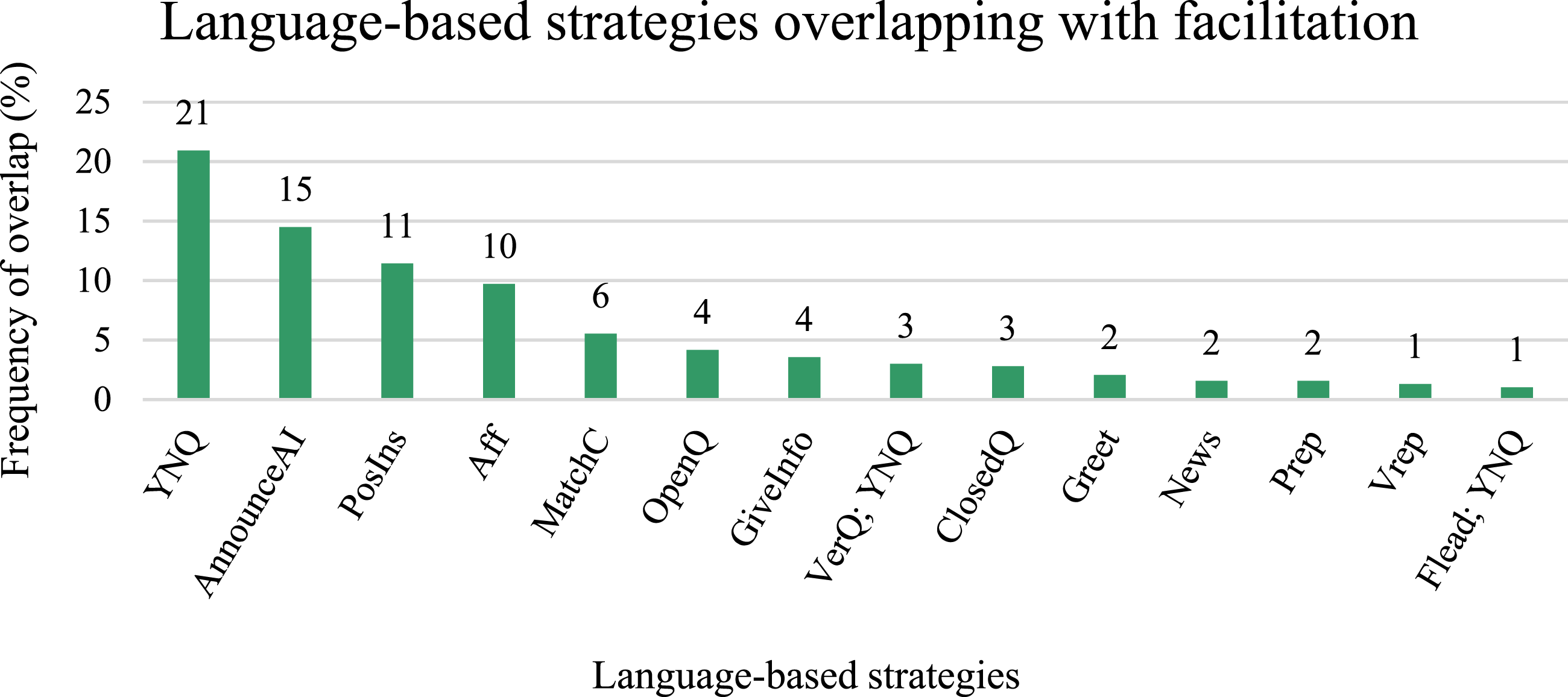
In the excerpt below, the PSW provides a positive instruction to facilitate the client’s completion of a task and to enable the client with dementia to sustain their action. Client with dementia: And what do I do next?
; :03 second pause Client with dementia: Run some water. Personal Support Worker: To wash your upper body. [Facilitation] [Give More Information]
Missed Opportunity Alternative
Language-based strategies overlapping with missed opportunity alternative at a frequency greater than or equal to 1% are displayed in Figure 6. Frequency of Language-based Strategies Coded as Missed opportunity Alternative. Note. AnnounceAI = Announcements of action/intent; PosIns = Positive instructions; YNQ = Yes/no questions; MinCue = Minimal cue; News = Newsmarks; AddName = Address by name and/or title; OpenQ = Open-ended questions; ClosedQ = Closed-ended questions; Aff = Affirmations; PosIns; YNQ = Positive instructions and yes/no questions combination; VerQ = Verification questions.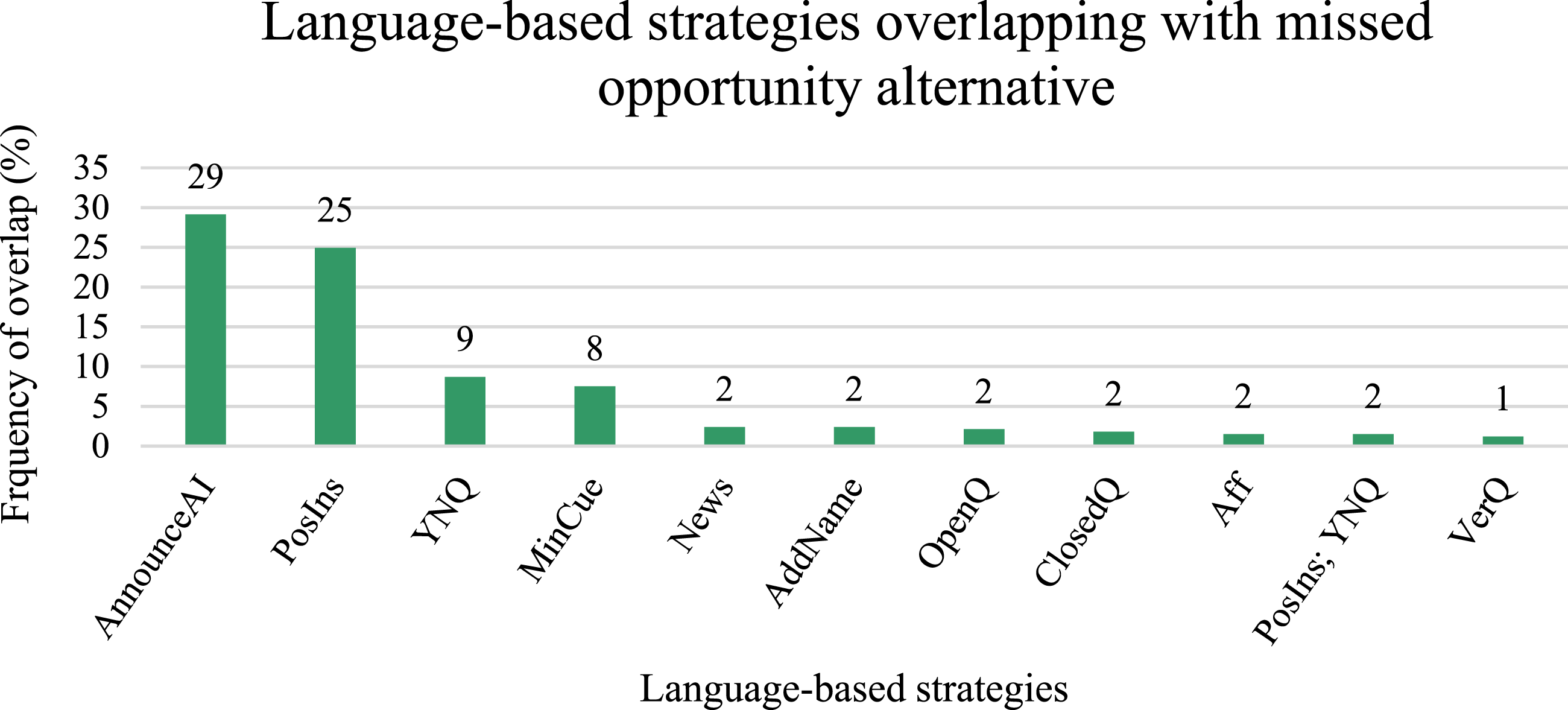
The PSW in this example uses a positive instruction that is overly directive rather than first enquiring about the client’s desires. Another missed opportunity alternative is exhibited when the PSW uses the collective pronoun “we” while presenting a task that is not collaborative. Personal Support Worker: Did you sleep okay? [Facilitation] [Yes/No Question] Client with dementia: Yup. Personal Support Worker: Good. Client with dementia: (I) I>
Missed Opportunity Omission
Language-based strategies overlapping with facilitation at a frequency greater than or equal to 1% are displayed in Figure 7. Frequency of Language-based Strategies Coded as Missed opportunity Omission. Note. YNQ = Yes/no questions; ClosedQ = Closed-ended questions; OpenQ = Open-ended questions; VerQ = Verification questions and yes/no questions combination; ChQ = Choice questions; Flead; YNQ = Focused leads and yes/no questions combination; PosIns; YNQ = Positive instructions and yes/no questions combination; RepQ = Repetition-seeking question; MinCue = Minimal cues; PRep; YNQ = Paraphrased repetitions of yes/no questions.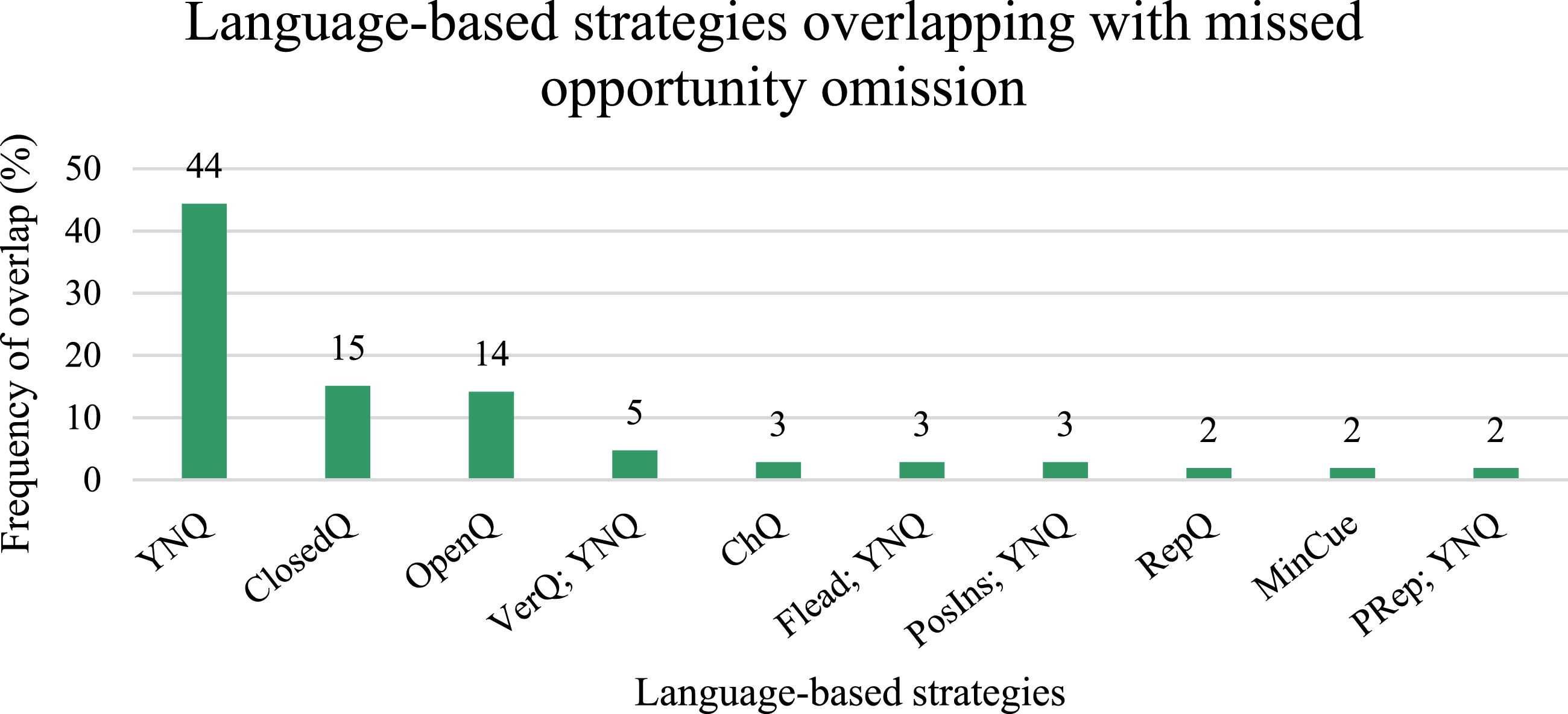
Below is displayed one of many instances where the PSW asks a yes/no question without giving the person living with dementia enough time to respond.
Personal Support Worker: Try sit here a little bit? [Validation] [Positive Instruction; Yes/No Question] ; :05 second pause Personal Support Worker: You can sit here. [Validation] [Positive Instruction]
Discussion
Research on communication with persons living with dementia has not explored whether the PCC and language-based frameworks complement each other, with the exception of one study by Savundranayagam and Moore-Nielsen (2015). They examined interactions with persons living with dementia in long-term care to determine whether language-based strategies support PCC. The present study analyzed the overlap between the language-based and person-centered approaches to communication during naturalistic home care interactions with persons living with dementia. This study also extended to assessing language-based strategies that may inadvertently contribute to missed opportunities for PCC.
Our findings highlight the person-centeredness of language-based strategies. More c-units were coded as a language-based strategy overlapping with PCC than PCC alone or a language-based strategy alone. In other words, several language-based strategies support the PCC goals. Yes/no questions, affirmations, and addressing the person by name/title can show recognition of the person living with dementia. Yes/no questions can exhibit negotiation while consulting with the client. Affirmations and positive feedback demonstrate validation. Finally, when used appropriately, yes/no questions and announcements of action/intent support facilitation.
Yes/no questions overlapped at a frequency greater than 10% with three of the four PCC indicators: recognition, negotiation, and facilitation. Home care PSWs frequently used yes/no questions to demonstrate recognition of the client’s life story. In contrast, Savundranayagam and Moore Nielson (2015) found that greetings overlapped most frequently with recognition in long-term care interactions between staff and residents with dementia. In comparison to long-term care, where constraints like staffing issues limit one-on-one time between PSW-client dyads (McGilton & Boscart, 2007), numerous home care interactions were enriched with opportunities for conversation. This may have motivated PSWs’ use of questions demonstrating recognition during active conversation about the client’s family, interests, and life events. Yes/no questions can facilitate the comprehension and expression of persons living with dementia (Ripich et al., 1999; Savundranayagam & Lee, 2017; Savundranayagam & Moore-Nielsen, 2015; Small et al., 2003; Small & Perry, 2005; Tappen et al., 1997; Wilson et al., 2012a). Yet, the literature also recommends them for specific purposes, namely, to accommodate communication difficulties, generate necessary additional information, or during collaboration on demanding tasks (Ripich et al., 1999; Small & Perry, 2005). It is notable that these functions seem more task-focused. Caregivers should be encouraged to use other question types, such as open-ended questions, if yes/no questions do not in fact yield further contributions from the person living with dementia. Yes/no questions overlapping with negotiation were posed in the current study to consult with the person living with dementia, rather than assuming their decisions (Kitwood, 1997). However, there is discussion that the use of yes/no questions in such situations should be limited to avoid inhibiting the free expression of persons living with dementia (Small et al., 2003). The present study displayed a similar pattern of frequent overlap between yes/no questions and negotiation as was observed in long-term care (Savundranayagam & Moore-Nielsen, 2015). This could indicate a shared task-focused nature of care across settings or rather the effectiveness of yes/no questions in facilitating successful responses thus prompting continued use. Unlike yes/no questions and choice questions, open-ended questions do not restrict the client’s responses. Contrarily, they may preserve the autonomy of the person living with dementia (Tappen et al., 1997). However, in practice, they overlapped with negotiation at a low frequency. Still, home care PSWs used open-ended questions to consult with persons living with dementia at a frequency more than double that observed in long-term care (Savundranayagam & Moore-Nielsen, 2015). Ultimately, caregivers should find a balance between modifying messages to improve comprehension/expression and providing opportunities for meaningful participation. Yes/no questions, overlapping with facilitation, that intend to learn more about a client are an example of formal caregivers striking this balance. They first prompted a confirmation/denial response to an information-seeking question, which often led to further talk from the client.
A majority of missed opportunities for PCC overlapped with language-based strategies. This indicates that language-based strategies are not always person-centered. Language-based strategies contributing to missed opportunities included announcements of action/intent, positive instructions, and various question types. For example, announcements of action/intent were missed opportunities when the PSW could have consulted with the client prior to announcing a new care activity or next steps. Instead, they prescribed what was going to happen next, failing to take consideration of individual preferences. Although announcements of action/intent can prepare the client for an upcoming activity, they should not hinder autonomy and free expression. Further, PSWs often missed opportunities to be person-centered when providing positive instructions. Positive instructions, which instruct what to do, can encourage collaborative behaviors (Belzil & Vézina, 2015; Bourgeois et al., 2003). However, when used inappropriately they can become overly directive and patronizing. Also, the common inclusion of collective pronouns in positive instructions, as in the previous missed opportunity alternative excerpt, feed into the perception that older adults cannot be independent (Williams et al., 2017). Understanding these pitfalls causing effective and well-intended language-based strategies to produce non-person-centered interactions can encourage caregivers to be mindful communicators.
The overlap analysis with missed opportunities provided support for the effectiveness of other language-based strategies in supporting PCC. Although the language-based strategy, allow time to respond, did not overlap frequently with the PCC indicators, its absence resulted in the association of most question structures with missed opportunities. Caregivers are therefore urged to use pauses, with caution and when appropriate, to allow persons living with dementia time to respond. Some researchers suggest extensive pauses, such as Weitzel and colleagues (2011) who recommend waiting 15–20 seconds after asking a question prior to offering any repetitions. Other researchers, including Christenson and colleagues Christenson et al. (2011), suggest that shorter 5 second pauses suffice. However, it is also conveyed that the dynamic nature of conversing with persons living with dementia depends on the individual, their disease progression, and the context of care (Müller & Guendouzi, 2005; Sabat, 1991; Savundranayagam & Moore-Nielsen, 2015). Pauses must therefore be employed tactfully to avoid threatening conversational continuity, potentially being counterproductive to communicative success (Müller & Guendouzi, 2005; Ramanathan, 1997).
Savundranayagam and Moore-Nielsen (2015) identified minimal diversity in the language-based strategies supporting PCC in long-term care. Similarly, the present study uncovered that only between one and four of the 32 language-based strategies overlapped with at least 10% of utterances coded as each indicator of PCC. There was minimal diversity in home care PSWs’ use of language-based strategies supporting PCC, despite more effective strategies having been identified from the literature. For example, strategies like newsmarks, which promote conversational continuity and demonstrate engagement (Ramanathan, 1997), received evidence-based support in the literature, but in practice were rarely used by home care PSWs. This may have contributed to their minimal overlap with PCC indicators.
Finally, as the proportion of persons living with dementia receiving care at home increases, attention to home care practices should be intensified. PSWs who shared their communication experiences with persons living with dementia emphasized that time constraints and heavy workloads in long-term care hindered meaningful interactions; they preferred home care because of one-on-one interactions and more time allotted for care provision (Kamalraj et al., 2021). Consistent with this finding, home care PSWs in the present study used far more person-centered language than long-term care PSWs (Savundranayagam & Moore-Nielsen, 2015). Also, half of the home care interactions in this dataset were leisure-based involving a great deal of personal conversation. A sub-analysis looking at communication patterns within the routine care and leisure-based interactions demonstrated that PSWs used more PCC during the latter. These interactions were longer in duration and had more contributions from the client living with dementia.
Our findings could be limited by a potentially incomprehensive language-based strategy coding framework. Although best efforts were made to ensure it was representative of present research, language-based strategies that do not yet have evidence-based support were excluded. Although other established coding systems, such as the Roter Interaction Analysis System (RIAS; Roter & Larson, 2002), were available, they did not align with the research objectives of the present study. The RIAS, in particular, was not considered to address the research questions as it is better suited for the analysis of medical interactions and medical dialogue (Roter & Larson, 2002).
The paramount strength of this study is that it contributes important findings to research within the home care setting. This study is the first to examine naturalistic interactions with PSWs and persons living with dementia in a home care setting. A unique perspective was offered on the day-to-day interactions between PSWs and persons living with dementia during various contexts in the home care setting, including routine care and leisure activities. This study also emphasizes that PCC goes beyond using effective language by considering the potential overlap between missed opportunities for PCC and language-based strategies.
Future Directions
This sample of 11 female PSWs who self-selected to participate in this study was largely representative of the PSW workforce in Canada who are predominantly women (Ministry of Long-Term Care, 2020). The sample also reflected a broad age range (21–62 years), representing multiple career stages. However, future research should take into consideration the growing diversity within this workforce—be it in race, ethnicity, sex, or gender—through recruitment and data collection measures promoting the inclusion of multiple perspectives regarding dementia, older adults, and caregiving. This study uncovered language-based strategies that can support multiple facets of PCC. Especially for yes/no questions, with which there is some contention regarding their effectiveness (Ripich et al., 1999; Small et al., 2003), future research could examine how certain types of yes/no questions may be more effective for communicating with persons living with dementia and supporting their personhood across care contexts.
The impact of a client’s severity of cognitive impairment on the type of communication used by their formal caregivers should also be examined. In the Canadian context, 40% of persons living with dementia in long-term care have severe cognitive impairment compared to only 20% of persons living with dementia receiving home care (Canadian Institute for Health Information, 2018a, 2018b). A study by Savundranayagam and Orange Savundranayagam & Orange (2014) found that certain language-based strategies were used at different proportions with persons living with early, middle, and late Alzheimer’s disease. It is therefore plausible that the proportion of language-based strategies used by PSWs may vary depending on the client’s severity of cognitive impairment.
Clinical Recommendations
Our findings provide implications for the co-occurrence of language-based and person-centered approaches, PSW communication training/education, and the state of research on communication with persons living with dementia in the home care setting. The knowledge that language-based strategies can preserve the personhood of clients with dementia will strengthen care interactions in an informed and systematic manner. The lived experiences of home care PSWs reveal a lack of confidence in their communication skills and ability to facilitate successful communication interactions (Kamalraj et al., 2021). PSW education and training can be enhanced to better support PSWs through added insight into language-based strategies aligning with PCC. This would add to the limited focus on dementia-specific communication training in the current PSW curriculum. Yes/no questions, affirmations, positive feedback, addressing the person living with dementia by name/title, announcements of action/intent, and positive instructions are key. Several language-based strategies that exhibited overlap with PCC indicators are already integrated into person-centered communication training interventions (Savundranayagam et al., 2020). Further, knowing how the inappropriate use of certain language-based strategies lead to missed opportunities for PCC can train formal caregivers to be more attentive to their communication. Communication training interventions must share the nuances in the skills they teach by including a consideration of common pitfalls inadvertently tied to certain language-based strategies.
Conclusion
Language-based strategies that support PCC can produce a range of outcomes concerning communicative success and level of participation from the person living with dementia. Formal caregivers can thereby avoid reinforcing misconceptions about the needs and abilities of their client. Instead, as demonstrated by the Communication Enhancement Model, these positive communication modifications may enrich the resulting interaction due to the improved confidence and expectations of the person living with dementia to meaningfully contribute to conversation (Orange et al., 1995). Rather than modifying communication behavior based on certain perceptions related to the inabilities of the older adult and/or person living with dementia, such as the need for simplification, the outcomes of this study can provide formal caregivers with effective language-based strategies that support the personhood of their client.
Supplemental Material
Supplemental Material - Language-Based Strategies that Support Person-Centered Communication in Formal Home Care Interactions with Persons Living with Dementia
Supplemental Material for Language-Based Strategies that Support Person-Centered Communication in Formal Home Care Interactions with Persons Living with Dementia by Reanne G. Mundadan, Marie Y. Savundranayagam, J. B. Orange and Laura Murray in Journal of Applied Gerontology
Footnotes
Acknowledgments
We would like to thank all participants for their willingness and openness to be involved in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by a grant to the second author from the Center for Aging and Brain Health Innovation and an award to the first author from the Ontario Graduate Scholarship Program.
Ethical approval
This research has received Research Ethics Board approval from The Office of Human Research Ethics, Western University (IRB Approval Number 107789).
Supplemental Material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.