
Abstract
Personal support workers (PSWs) provide a large proportion of in-home care services for Canadians. PSWs must negotiate with clients and their family on how prescribed care is delivered. How PSWs set and maintain professional and personal boundaries during care is poorly understood, and failure to manage boundaries can expose both PSWs and clients to risk. High-performing PSWs (n = 9) and supervisors (n = 4) within an Ontario, Canada, home care agency were engaged in workshops (n = 3) to identify field-tested strategies and tactics for identifying, managing, and supporting PSW boundaries. A boundary-management framework was generated, including types of boundary challenges; decision-making principles (e.g., consider the purpose of home care); response strategies (e.g., work with the client on an alternative solution); and tactics for action (e.g., use proactive reminders). Supervisory and organizational supports (e.g., enabling “shop-talk”) were identified. The framework can inform teaching and practice materials for PSWs in Canada and other countries.
Keywords
PSWs engage in a complex and largely implicit decision-making process when choosing to enforce or make an exception to a boundary between professional and unprofessional, or safe and unsafe, work during a boundary-challenging situation. In the absence of macro- (e.g., provincial) and meso-level (e.g., organizational) supports to guide boundary negotiation, high-performing PSWs engage in a nuanced, self-directed boundary-management process with multiple individualized tactics (often in combination) which leverage their interpersonal relationship with the client. In addition to developing materials to train PSWs’ individual boundary-management skills, organizations can support and encourage already existing/organic opportunities for PSWs to collectively manage boundaries. These opportunities are viewed positively by both supervisors and PSWs.
The strategies and tactics identified can be used in training programs to help PSWs become more adept at identifying and managing boundaries during care. The supervisor and organizational supports can be integrated by care organizations to facilitate PSWs’ successful boundary management. Future research can further investigate the role of collective decision-making in PSWs’ successful boundary management.What this paper adds
Applications of study findings
In 2021, approximately 6.1% of Canadians reported at least one person in their household received formal home care services in the year prior, and 52% of those households received home support services (Statistics Canada, 2022). Clients, families, and governments favor home care over institutional care because it typically yields better medical and social client outcomes while reducing system expenditures (Sinha & Nolan, 2020).
Over 80% of Canadian home care services are delivered by direct care providers (Sinn et al., 2022) variously called personal support workers (PSWs), home health aides, and personal care aides, depending on jurisdiction. In Ontario, Canada (i.e., the geographical location of this study), PSW is the term used, and thus the term applied throughout this paper. Although titles vary, work tasks are largely consistent, primarily including a) assisting clients with activities of daily living (ADLs; e.g., bathing and dressing assistance) and instrumental activities of daily living (IADLs) for independent community-living (e.g., meal preparation), and b) completing social support activities (e.g., respite services) (Saari et al., 2018). A small, but growing, proportion of PSWs are increasingly performing delegated care tasks (e.g., range of motion exercises, complex lifts, and transfers) as home care demand grows (Saari et al., 2018).
Ontarian PSWs are unregulated, with no predefined scope of practice, no standardized training/education, and job descriptions that vary across organizations (Saari et al., 2018). Home care sector PSWs frequently experience precarity, with the lowest rates of full-time hours, poorest rates of pay, more irregular schedules of work, and frequent workplace injuries (Zagrodney et al., 2023a). In Canada, they are primarily female, older aged, and a substantial proportion are immigrants (Zagrodney et al., 2023b). Ontario home care PSWs are employed by for-profit and not-for-profit care organizations. Clients obtain services 1) through Home and Community Care Support Services (HCCSS), the provincial agency responsible for coordinating publicly paid in-home and community-based services delivered by contracted provider organizations; or 2) by purchasing services directly from an organization on a private-pay basis (Brookman et al., 2022).
PSWs help clients continue living independently and are a vital component of high quality, person- and family-centered home care, to the point they are sometimes described as “members of the family” by clients and caregivers (Lee et al., 2020; Spring et al., 2024). Despite this importance, how and what is involved in delivering care is poorly understood and under-researched (Lam & Baxter, 2023). What we do know is PSWs encounter many situations requiring boundary-negotiation (Karlsson et al., 2020; Spring et al., 2024). Boundaries are “standards that include the rules, expectations and guidelines (technical and ethical) that govern a professional both at work and outside work to facilitate a safe and effective working environment” (Abrams et al., 2018, pp. 1976–1977). Boundaries exist for work tasks, emotional engagement, appropriate behavior (for clients and PSWs), and personal disclosure (Abrams et al., 2018; Karlsson et al., 2020). There are many reasons for boundary challenges (Karlsson et al., 2020), and a PSW may make an exception (e.g., by staying later than scheduled, or completing non-care plan tasks) (Franzosa et al., 2018; Spring et al., 2024) to benefit clients or avoid moral distress due to unmet client needs (Byrne et al., 2012).
Negotiating boundaries involves direct communication and managing formal (e.g., company policies and care plans), informal (e.g., client and family’s expressed needs and expectations), and interpersonal factors (e.g., relationships between PSW, client, and caregivers/family) (Martin-Matthews et al., 2013; Ris et al., 2019). These factors can, and do, conflict (Timonen & Lolich, 2019), forcing PSWs to decide what is “best,” often at some other expense (e.g., not staying for the “full time” and being seen as uncaring) (Karlsson et al., 2020). Successful boundary-management relies on intersecting macro-, meso-, and micro-level factors. In absence of standardized provincial training/education standards and guidelines (macro-level), or formalized workforce structures (meso-level), it is largely up to a PSW’s individual experience, skill, and personality (micro-level), to accomplish a satisfactory solution (Spring et al., 2024).
Ontario’s vocational learning standards for PSW training courses (Ministry of Colleges and Universities, 2022) mention person-centered care delivery and professional boundaries, but a review of current training and education showed little time for care service negotiation (Grant, 2016). Some guidelines and manuals on professional conduct standards exist, but have largely been adapted from other models (e.g., medical, clinical, and therapeutic), and may not translate well to home-based settings (Shevellar & Barringham, 2015). Additionally, intimate and emotional personal care can be more difficult to navigate with rigid rule-based ethics (Abrams et al., 2018; England & Dyck, 2011; Shevellar & Barringham, 2015).
PSWs also receive little guidance from employers on managing non-task work (Franzosa et al., 2018). Structured care plans map “task”-related activities (i.e., direct care services like baths or medication reminders) but omit “non-task” work PSWs do to deliver care or address non-clinical care needs (e.g., providing social engagement) (Franzosa & Tsui, 2020). Despite providers’ lack of received support, this “social labor” (Lam & Baxter, 2023) involving person-centered, holistic, and “family-like” PSW care is frequently emphasized in organizational marketing to attract clients (Franzosa & Tsui, 2020).
Boundary management is an important skill because avoiding all exceptions is “in many situations neither advisable nor possible” (Zur, 2013, p. 254), and they can be safe and beneficial, especially in meeting person-centered care needs (England & Dyck, 2011). However, despite regularly encountering boundary challenges, many home care PSWs struggle with them. This can expose clients and PSWs to risks of injury, psychosocial stress, abuse, and being taken advantage of (Brouillette et al., 2023; King et al., 2018; Ruston & Backhouse, 2022), on top of the already physically demanding work (Ho et al., 2023), which aggravates ongoing health human resource challenges (Zagrodney et al., 2021). Therefore, identifying and leveraging boundary-management strategies is essential to protect the limited PSW workforce from burnout and psychosocial stress; reduce staff and client injury rates; and demonstrate organizational support to facilitate PSWs’ job satisfaction (Brouillette et al., 2023; Denton et al., 2002; Lee & Jang, 2016; Quinn et al., 2021; Yoon et al., 2015).
The study goals were to a) identify and expand on thought processes and tactics used by high-performing PSWs in care negotiations and b) identify supervisory and organizational supports necessary to enable and support PSW approaches. In this study, “high-performing” PSWs and supervisors are defined as positive deviants who “consistently demonstrate exceptionally high performance in an area of interest” (Bradley et al., 2009, p. 2) with the same resources and supports available to other similarly situated individuals. Leveraging positive deviants addresses complex health care issues effectively by (re)using solutions from populations who encounter them (Bradley et al., 2009), which can be further spread via co-designed educational materials (Lawton et al., 2014). While other professions’ boundary-management strategies might be adapted for PSWs, we believe highlighting and sharing already successful methods is a valuable first step which could later be supplemented by other sources.
As PSW work involves physical, social, and emotional labor activities (England & Dyck, 2011; Lam & Baxter, 2023; Saari et al., 2018, 2019), this paper uses “boundary challenges” to identify when any member of the care relationship (e.g., PSW, client, and caregiver) attempts to or does (whether implicitly or explicitly) re-negotiate, change, or newly establish some aspect of care. In this case, we use “care” in a holistic rather than task-based sense, so boundaries are not only limited to direct service provision but also incorporate other activities (e.g., gift-giving and attending clients’ funerals) that PSWs encounter. This diverges from other home care literature by a) characterizing boundary challenges and exceptions as neither inherently negative nor positive and b) framing boundaries to capture home care PSWs’ context more inclusively. We have opted not to use “boundary crossing” to reinforce the negotiation inherent in such boundaries.
Methods
A pragmatic approach guided workshops in southern Ontario, Canada, identifying boundary-management strategies with high-performing PSWs and supervisors (Kaushik & Walsh, 2019). Findings are reported using COREQ guidelines (Tong et al., 2007) (Supplemental Material 1). Ethical approval was obtained from the University of Waterloo Research Ethics Board (REB#40913).
Participants and Recruitment
With stratified purposeful sampling of extreme cases (Palinkas et al., 2015) participants were recruited for one of three workshops (n = 13, range 2–6 participants) from three geographically diverse regions within one home care organization. Each region’s director was emailed by the study team to introduce the project and asked to suggest potentially interested high-performing supervisors. Supervisors contacted ECK and were asked to share study information with high-performing PSWs on their teams, with guidance to contact ECK if interested. Although “high-performing” was not defined for directors or supervisors, we anticipated individuals would be readily identifiable by people they report to. Given the lack of “quality” metrics for home care service delivery and that many dimensions of care are not captured in existing documentation practices, we opted not to use administrative data to identify staff. Supervisors and PSWs were not separated into different workshops as one goal was to examine supervisory supports and understand how those supports affect PSWs.
Data Collection
Development of Workshop Scenarios
The workshops integrated 10 vignettes of common boundary-challenging situations (see Supplemental Material 2) developed from unpublished research ECK and PH conducted in 2017, with PSWs and supervisors who discussed commonly occurring care problems. To ensure relevance, vignettes were reviewed by a nurse researcher with extensive home care experience. Four or five regionally salient vignettes were presented in each workshop. Nine vignettes strongly resonated with participants across all three sites; the remaining vignette was not relevant to PSW-delivered care and was omitted after the first workshop.
Pre-Workshop Sensitizing Activity
Four days pre-workshop, ECK emailed participants sensitizing questions (Sanders & Stappers, 2012) about 1) strategies for setting reasonable boundaries, 2) strategies if clients forget or push boundaries, and 3) supports required for successful boundary management.
Group Workshop
Workshops employed a layering approach to elicit both latent and tacit knowledge (Sanders & Stappers, 2012). Vignettes were introduced one-by-one, and participants were asked 1) to identify boundary challenges and how they could be managed and 2) to discuss principles underlying their responses. ECK facilitated workshops with support from EAK.
The 3-hour long workshops were held in private conference rooms and were audio- and video-recorded, with paper worksheets completed by EAK. Participants were provided with refreshments and a midpoint break. Audio recordings were professionally transcribed and reviewed by EAK and ECK prior to data analysis.
Follow-Up Interview
Follow-up calls were completed by ECK (average = 18 minutes duration, 4.1 days post-workshop; range = 1–14 days; 3 participants unreachable) to give participants an opportunity to share additional reflections, including ones they were not comfortable sharing in group settings. ECK audio-recorded and took notes and then shared aggregated results with EAK and PH during analysis.
Data Analysis
To increase rigor and reduce bias, EAK and ECK made independent post-workshop notes and reviewed data individually before coding began (Lincoln & Guba, 1986). Reflexive thematic analysis (Braun & Clarke, 2019) was used to generate themes that formed the boundary-management framework. EAK and ECK developed the initial framework, and PH assisted with data analysis and framework refinement. Original recordings were referenced where necessary to identify body language and tonal cues. During early analysis stages, both EAK and ECK challenged assumptions about the emerging framework and contributed notes to the data audit trail. PH acted as a peer debriefer removed from immediate data gathering but familiar with qualitative home care research.
Coding and framework development took place on paper before a digital version of the framework was created in Microsoft Word. An early draft was presented to one PSW and one supervisor for member-checking. Where necessary, the framework was revised to be more reflective of members’ experiences.
Results
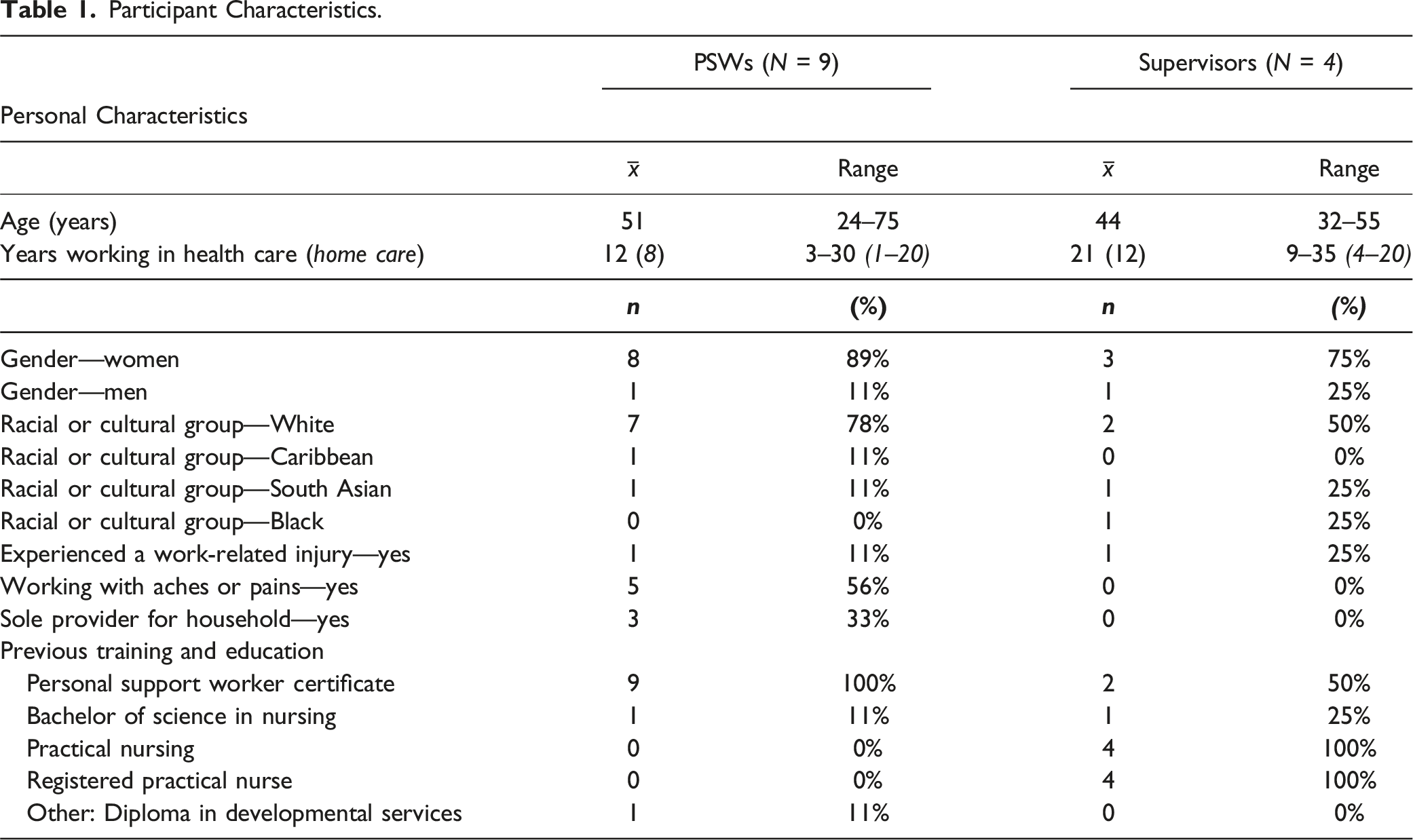
Participant Characteristics.
A boundary-management framework (Figure 1) was constructed to depict how PSWs recognize a boundary challenge, principles they consider in selecting a response, strategies for responding in the moment, and tactics used to implement their chosen response. Supervisory and organizational supports that enable these responses were identified. Home Care PSW Boundary-Management Framework.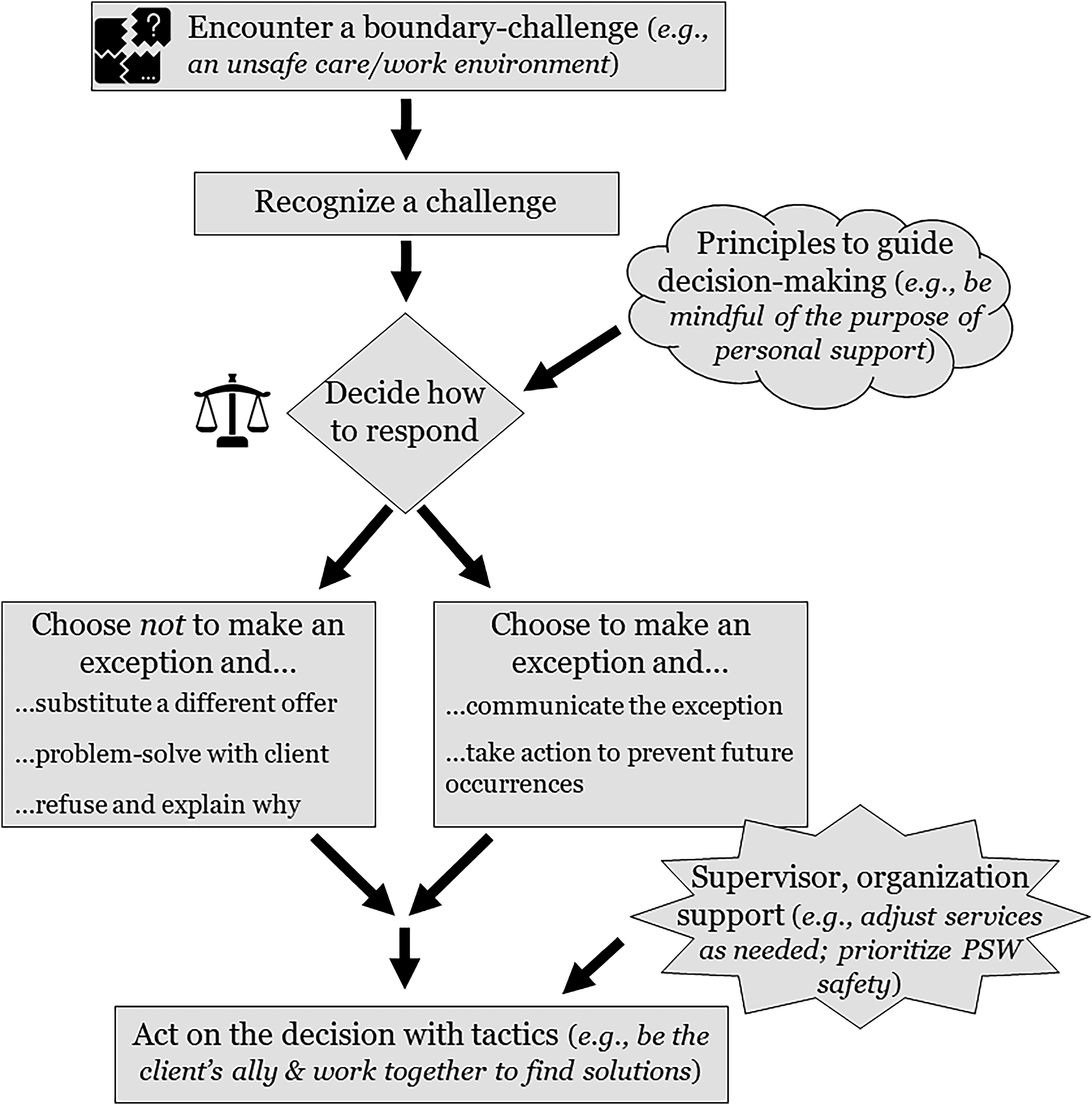
Encounter a Boundary Challenge and Recognize a Challenge
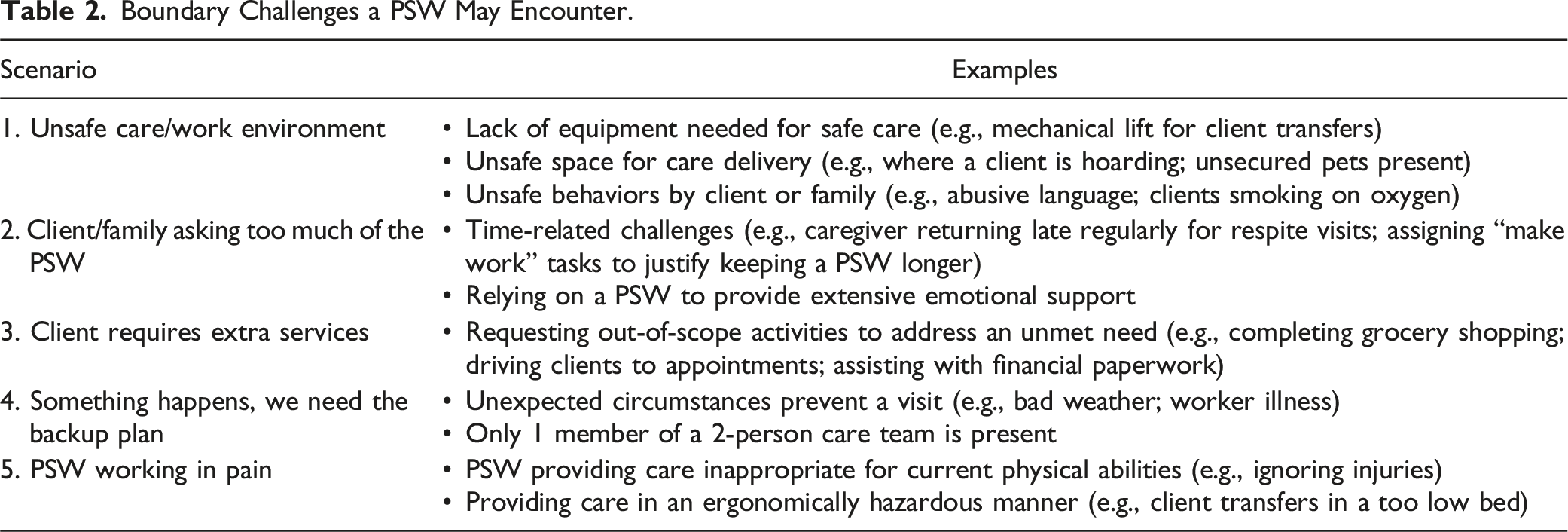
Boundary Challenges a PSW May Encounter.
Principles to Guide Decision-Making
Principles a PSW May Use to Decide on Their Response to a Boundary Challenge.
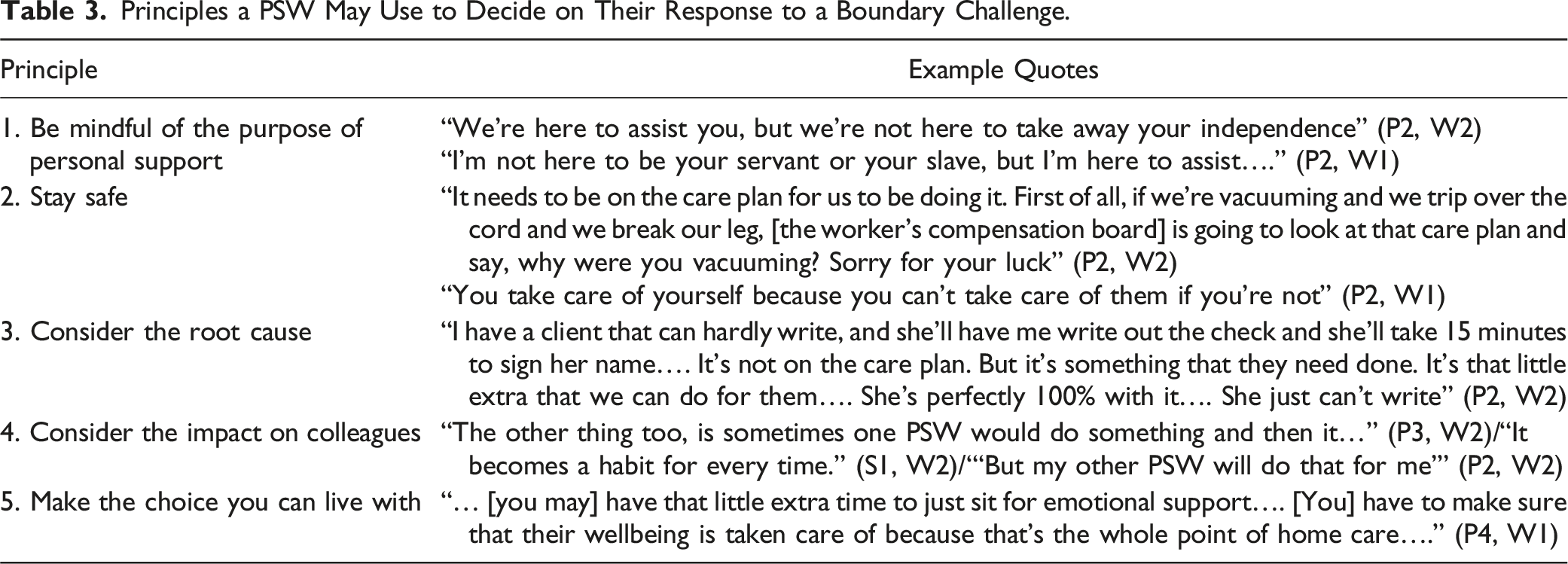
Workshop participants felt it was important to consider the impact decisions would have on colleagues (Principle 4). One PSW making an exception can create expectations that negatively impact other PSWs or perceptions that following the care plan is “slacking off.” Ultimately, a PSW must make a choice that they can live with (Principle 5). In some cases, knowing a client would otherwise go hungry, a PSW might bring food when they visit. After all, “you don’t just dismiss their issue. You try and help. That falls on all of us, not just the supervisor” (P4, W1).
Decide How to Respond
Once a boundary challenge is identified, a PSW must decide their response (Figure 1). This may involve individual or collective decision-making, and multiple factors are considered: perceived client need, degree of risk, work schedules, any pre-existing team boundaries, how frequently the challenge (re)occurs, and the PSW’s moral principles. PSWs may be more inclined to make an exception if the situation is a “one-off” that is unlikely to re-occur; relatively low risk; important to a client; or requiring modest effort or time.
Collective decision-making occurs when PSWs establish a boundary they all maintain. “Shop talk” was crucial for collective boundary-setting since it provides an opportunity to problem-solve and mentor. “We will sit down collectively and discuss how each of us are taking care of [a shared client]. So that if one person’s approach isn’t working, maybe another person’s is… We always make sure that we find 20 minutes at the end of our day… and discuss anything like that” (P2, W1).
Collaboration allowed PSWs to reduce individual-level burden, since no single PSW had to “be the heavy person and say, well I can’t do this, because it’s not on your care plan” (P3, W2).
There are some circumstances where “exceptions” to usual care rules have been formalized in the care plan. One supervisor observed that if a client has become accustomed to care activities excluded under new legislation/practice directives, “to try and take [back] or… scale them back, [is] next to impossible” (S1, W2), so an exception could be made.
Potential Responses to Boundary Challenges
When PSWs identify a boundary challenge, they choose whether to make an exception and what strategy to use (Figure 1). When making an exception, a PSW communicates this is not usual care by explaining what exception is being made and why (e.g., bringing bread so a client has food) (Strategy A), or communicates the exception and takes action to prevent future occurrences (e.g., notifying the supervisor that alternative/additional services may be needed) (Strategy B). If a PSW chooses not to make an exception, they may offer an alternative solution (e.g., staying late tomorrow) (Strategy C), work with the client/family to find solutions (e.g., calling the supervisor together to arrange alternative services) (Strategy D), or refuse and explain why (Strategy E). Strategy E may include situations prohibited by employers; well outside safe practice scope; presenting undue risk; or dubiously legal (e.g., client housing an illegal and potentially dangerous animal).
Act on the Decision With Tactics
Tactics PSWs Can Use to Manage Boundaries.
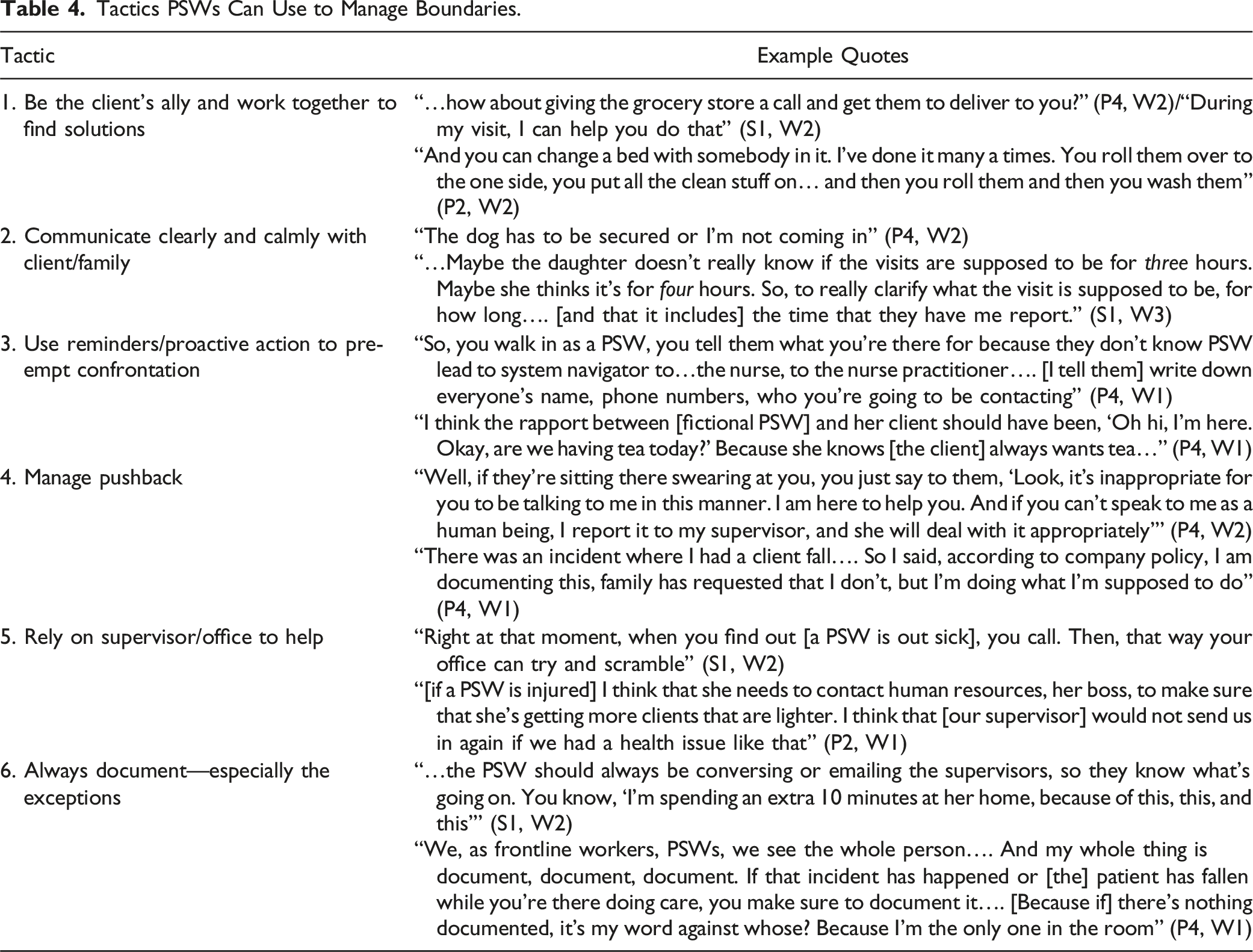
When experiencing pushback from a client or family member who feels their needs are not being met, PSWs can address the situation themselves (Tactic 4) (e.g., by reminding clients abusive behavior is inappropriate). If needed, PSWs may leverage their supervisor’s help (Tactic 5). The supervisor is not limited to just addressing upset clients; all PSWs felt their supervisor(s) were available for support and advice on a range of topics. As one PSW said, “[a] supervisor needs to be someone that’s willing to listen to their employees and be understanding and not just be all boss” (P3, W2). Even if a supervisor cannot directly help a situation, they are often the gatekeeper to further services/solutions (e.g., arranging care reassessments). Participants emphasized PSWs must always document what is happening (Tactic 6), which provides protection for all parties involved.
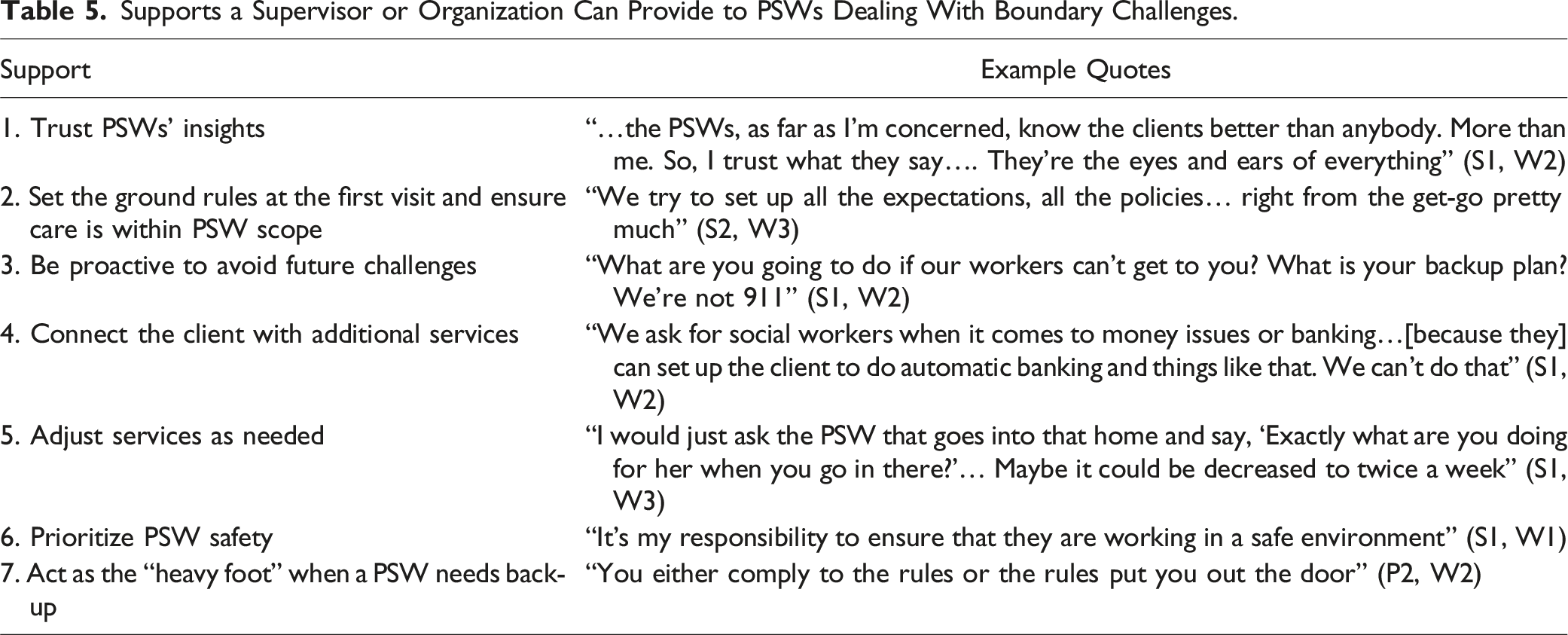
Supervisory and Organizational Support
Supports a Supervisor or Organization Can Provide to PSWs Dealing With Boundary Challenges.
Discussion
In absence of macro-level changes in Ontario (e.g., re-development of provincial education programs or regulation/management of ongoing PSW competencies), identifying micro-level PSW boundary-management practices and developing meso-level solutions like training packages to upskill point-of-care staff are essential to retain PSWs, provide high-quality care, and reduce risk of client or provider injury. This study provides novel insight into how high-performing PSWs set and maintain boundaries with clients, as well as supervisory and organizational supports necessary for this to be successful. It advances current literature by moving beyond “why” boundaries are challenging for PSWs to instead focus on “how” positive deviant providers are successful. We anticipate findings will be relevant for Canada and internationally as strategies can be implemented at the level of an individual or integrated into broader organizational training and practices.
Several boundary-challenging scenarios discussed by participants have been identified in prior literature, including hazardous client homes, extra care tasks, and PSWs working in pain (Brouillette et al., 2023; Karlsson et al., 2020; Zagrodney et al., 2023a). To our knowledge, this is the first study categorizing responses PSWs may have to a boundary challenge. Only one of the responses discussed (i.e., choose not to make an exception and explain why) does not involve action to help meet a client’s immediate or future needs. The implicit emphasis on meeting clients’ needs is aligned with published research as well as principles described by participants. Experiences of fulfilling client–provider relationships and supporting vulnerable clients are important motivation for PSWs to continue working in their job (Nizzer et al., 2023), and having the ability to provide care in a way a PSW believes best suits a client is associated with higher intrinsic job satisfaction (Barken et al., 2018; Morgan et al., 2013).
Decisions were predominantly made at an individual/micro-level, although some micro-level structures (e.g., “shop talk” with peers) took the place of absent organizational-level directives. Congruent with expectations, participants described a nuanced self-directed boundary-management process that accounts for personal factors, client characteristics, organizational requirements, work experience, and practical logistics. To our surprise, much of this knowledge is implicit, and participants had difficulty articulating how they recognize a boundary-challenging situation beyond “just knowing” when one occurs. Difficulty explicitly identifying boundary challenges has important implications for designing boundary-management training since before choosing a response, PSWs must first recognize a potential or actual challenge.
Aligned with Sims-Gould and Martin-Matthews (2010), many PSW tactics focus on maintaining positive rapport with clients while providing safe care. Participants described selecting tactics based on past experiences (i.e., what has worked for them before), knowing the client, intuition, and trial and error. It is possible that PSWs do engage in some form of systematic tactic-selection but are unaware of this.
In addition to developing training materials that build individual-level skills, organizations can encourage opportunities for “shop talk” and peer-support, which allows PSWs to collectively problem-solve and promotes consistent responses to boundary-challenging events (Denton et al., 2002). This is a comparatively resource-cheap approach that demonstrates organizational support, which reduces PSWs’ job stress while increasing intrinsic job satisfaction (Denton et al., 2002; Lee & Jang, 2016; Morgan et al., 2013; Yoon et al., 2015). These opportunities were very important to participants, which is echoed in other boundary-management research (Karlsson et al., 2020). Having a collective boundary all PSWs enforce helps staff better field stressful requests by diffusing responsibility across multiple providers (Karlsson et al., 2020).
In a departure from other literature (e.g., Franzosa et al. (2018)) PSWs in this study felt very supported by their supervisors, which included feeling their contributions were valued and that supervisors cared about, and worked to support, the well-being of “their” PSWs. It is beyond the scope of this study to attempt to determine the cause of this perception, for example, whether high-performing supervisors are better at supporting all PSWs or whether high-performing supervisor–PSW combinations build better rapport and support together. However, this finding does demonstrate that not all PSWs feel unsupported by their supervisor, which builds the case that effective organizational and supervisory supports (i.e., meso-level supports) can be implemented more widely within home care organizations, since they already exist in small pockets.
In our research, PSWs often leveraged supervisory support to reinforce a limit or obtain longer-term solutions. This supports other research which identified the value of supervisors in managing boundaries with clients (Karlsson et al., 2020) and demonstrated organizational structures can help or hinder PSWs’ management of boundaries (Cloutier et al., 1999). For supervisors in our study, their role enabled them to take actions that are unavailable to PSWs (e.g., arranging outside supports for a client, requesting re-assessment of client needs and service levels, or discontinuing care for a client whose behavior endangers staff). Although PSWs in our study were not concerned about relying on a supervisor for support, other PSWs may be reluctant to engage a supervisor for fear of endangering their relationship with a client (Sims-Gould & Martin-Matthews, 2010). This is something future training and support programs should consider.
Strengths and Limitations
Using pre-existing care scenarios provided participants with realistic situations for consideration, and pairing scenarios with a workshop format capitalized on the synergy and constructive ideas that can be generated by bringing together skilled individuals. Engaging positive deviants means strategies, tactics, and supports discussed have been tested “in the field” successfully, increasing the likelihood that they will be usable and effective for others (Bradley et al., 2009). Data were primarily generated through group workshops, but participants also had an opportunity to share additional thoughts privately with ECK during follow-up interviews.
However, the sample of participants is relatively small and drawn from a single home care organization. Additionally, strategies and tactics were self-identified, and actual application may vary. Further evaluation of the framework with supervisors and PSWs from other organizations paired with participant observation would provide an opportunity to assess transferability, robustness, and completeness. Client and family perceptions of the boundary-management framework should also be explored. Finally, it is possible that some strategies may not translate to other contexts, like directly funded (e.g., “gig”) PSWs.
Implications
The strategies and tactics identified can inform training programs to help PSWs become more adept at identifying and managing boundary challenges. Additionally, this work highlights how supervisors and organizations can support PSWs’ boundary management. Based on our findings, we would recommend that home care organizations foster opportunities for “organic” peer-support among PSWs, in addition to developing more formal training materials on boundary management. In absence of macro-system changes, developing PSW skills and organizational-level resources can help reduce PSW and client injury risks, improve staff satisfaction and retention, and ultimately improve client care.
Conclusion
While past research highlighted the importance of boundary management for PSWs working in home care, it has not addressed how PSWs should act to manage boundaries or how best to support them. This work presents a practical boundary-management framework with field-tested strategies and tactics that can be used by PSWs and the supervisors and organizations who support them, to manage boundaries with clients while ensuring needs are appropriately supported. Further research is needed to explore how PSWs recognize boundary challenges, beyond reliance on intuition and experience, and to understand the framework’s transferability as a basis for developing training for PSWs and supervisors, and organizational strategies to enhance support for PSWs.
Supplemental Material
Supplemental Material - How High-Performing Personal Support Workers Set and Maintain Boundaries When Providing Care: A Case Study in Ontario, Canada
Supplemental Material for How High-Performing Personal Support Workers Set and Maintain Boundaries When Providing Care: A Case Study in Ontario, Canada by Elizabeth A. Kalles, Emily C. King, and Paul Holyoke in Journal of Applied Gerontology.
Supplemental Material
Supplemental Material - How High-Performing Personal Support Workers Set and Maintain Boundaries When Providing Care: A Case Study in Ontario, Canada
Supplemental Material for How High-Performing Personal Support Workers Set and Maintain Boundaries When Providing Care: A Case Study in Ontario, Canada by Elizabeth A. Kalles, Emily C. King, and Paul Holyoke in Journal of Applied Gerontology.
Footnotes
Acknowledgments
The authors would like to thank all the staff and supervisors who contributed their time and expertise to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Women’s College Hospital – Women’s Xchange 15K Challenge; SE Health; MITACS (Grant #IT07204); and the Canadian Institutes of Health Research – Postdoctoral Fellowship (Grant #396160).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.