
Abstract
The rates of dementia are on the rise as populations age. Storytelling is commonly used in therapies for persons living with dementia and can be in the form of life review, and reminiscence therapy. A systematic literature review was conducted to examine the range and extent of the use of digital technologies for facilitating storytelling in older adults and their care partners, and to identify the processes and methods, the technologies used and their readiness levels, the evidence, and the associated outcomes. Eight electronic databases were searched: Medline, EMBASE, PsycINFO, CINAHL, Abstracts in Social Gerontology, ERIC, Web of Science, and Scopus. We included 34 studies. Mild cognitive impairment or dementia represented over half of medical conditions reported in the studies. Overall, our findings indicate that the most common use of digital storytelling was to support older adults’ memory, reminiscence, identity, and self-confidence; however, the level of evidence of its effectiveness was low.
Introduction
The rates of dementia are on the rise as populations age. In 2019, 50 million people were living with dementia globally and this number is expected to increase to 82 million in the next 11 years (World Health Organization [WHO], 2019). Challenges experienced by persons living with dementia include memory loss, difficulties with communication, and losing a sense of their identity (Alm et al., 2007). Storytelling is commonly used in therapies for dementia and can be in the form of reminiscence, life review, and reminiscence therapy (Damianakis et al., 2010).
When digital technology is used to create and tell stories, it is called digital storytelling. A digital story can be defined as a 3- to 5-min short clip with sequences of still images and photos, music, video clips, narration, or written text, selected and woven together to impart messages to various audiences such as family, friends, care providers, community members, and the general public (Stenhouse et al., 2013; Waycott et al., 2017). These messages and topics can range from personal experiences of a condition (e.g., illness, caregiving, being housebound) to major biographical events of a person’s life. Thus, digital storytelling can be a powerful tool that has been used with older adults to foster social interaction (Chonody & Wang, 2013), stimulate autobiographical memory and communication with family members (Smith et al., 2009), and facilitate self-expression and identity (Manchester & Facer, 2015). Potential benefits of digital storytelling for persons living with dementia, in particular, include increased confidence, connection with others, sense of purpose, communication, and improved well-being (Alm et al., 2007; Massimi et al., 2008).
Despite an increased interest in utilizing digital storytelling among older adults, including those living with mild cognitive impairment or dementia, scholarly literature on this topic remains limited, and the level of evidence as well as the procedures and technologies used for the creation of the stories are unknown. Thus, for this literature review, we posed the question, “How has digital storytelling been used with older adults with typical aging, and with mild cognitive impairment, or dementia?” This can inform how digital storytelling can be applied in practice and identify future research directions. To address the research question, the objectives of this systematic review were to (a) describe the purpose of digital storytelling studies; (b) identify the processes and methods utilized in the studies and development of the stories; (c) identify technologies used in digital storytelling and describe their readiness levels, that is, stages of precommercial development of a technology; (d) summarize the outcomes of using digital storytelling among persons with typical aging, and living with mild cognitive impairment or dementia; and (e) identify the clinical evidence of the digital storytelling interventions used.
Method
Design
In this systematic literature review, we (a) formulated the research questions based on the PICOS guidelines (Population, Intervention, Comparison, Outcome, Study type; Portney & Watkins, 2015), (b) identified relevant studies, (c) selected the studies based on inclusion and exclusion criteria, (d) charted the data, and (e) collated, summarized, and reported the results.
Data Sources and Search Strategy
A health sciences librarian supervised and validated the search strategy. Our search was conducted in eight electronic databases: Medline, EMBASE, PsycINFO, CINAHL, Abstracts in Social Gerontology, ERIC, Web of Science, and Scopus. All databases were searched using the following MesH1 terms identified in the title, abstract, or key words: (dementia OR Alzheimer OR “cognitive impairment”) OR (elderly OR “older adults” OR aging) AND (reminiscence OR memories OR storytelling) AND (digital OR ICT OR “artificial intelligence” OR online OR media OR mobile) (see Table A.1 in Online Appendix A).
Inclusion criteria
1. Papers that report the use of digital storytelling that included:
(a) People age 50 years and older, including those with typical aging or living with mild cognitive impairment or dementia. This cutoff point allowed us to include papers from diverse countries where the life expectancy is shorter (WHO, 2001).
(b) Technology (ies) implemented or deployed at least in pilot form: Technology Readiness Level (TRL) 5 (Department of Energy [DOE], 2009), with one older adult at a minimum.
(c) Digital media production to create narrative forms of telling a story using nonphysical media such as video (with and without sound), animation, pictures, or audio and/or methods that employ any kind of data mining and artificial intelligence to create these narrative forms of telling a story.
2. Papers published between January 1, 2005, and June 4, 2019.
3. Studies published in any language and available in full-text in peer-reviewed journals or conference proceedings.
4. Papers that used any type of study design or methodology, with positive or negative results.
Exclusion criteria
Studies published in books, book chapters, doctoral, or master’s theses.
Conference lecture notes, seminal or theoretical papers, news, protocols, and any type of literature reviews.
Studies that used digital media only for gathering research data without producing a digital media story.
A complete book of conference proceedings.
Full papers that were not available.
Abstracts or papers that translation software was unable to translate.
Papers that did not provide enough information to categorize it (e.g., description of participants, technology readiness).
Studies Selection Process
Two members of the research team (C.D. and N.N.) exported identified studies into the reference manager (RefWorks) and removed duplicates. The team (A.M.R.R., C.D., N.N., A.M.C., L.L.) evaluated the titles and abstracts and compared them with the inclusion and exclusion criteria. Two pairs of researchers (Pair 1: C.D. and A.R.; Pair 2: N.N. and A.M.C.) evaluated the full texts of the selected studies. Any differences between the two pairs of the independent researchers were reviewed by a third reviewer (L.L.) to make the final decision.
Data Extraction Process
Two pairs of reviewers (Pair 1: A.R. and A.C.; Pair 2: C.D. and A.M.C.) extracted data in the included papers. Each pair met to reconcile any differences through discussion. For more details on the operationalization of each variable extracted from the studies, see Table B.1 in Online Appendix B.
Data Analysis and Synthesis
One member of the team (A.C.) conducted the data analysis under the supervision of the experienced authors who met with him in a weekly basis to guide and review data analysis. The studies were categorized into nine groups according to the main purpose of the story. All studies were analyzed in terms of population characteristics, study designs, processes, and methods for creating the digital storytelling, and the new technologies that have been used and its readiness levels. We used descriptive statistics to characterize the studies included in our literature review. In some cases, we allowed data such as diagnoses to be counted manifold.
Risk of Bias (Quality) Assessment
By including a variety of source, databases were able to achieve greater levels of sensitivity to avoid reducing source publication bias and to guarantee a more thorough search. The inclusion of papers with positive and negative results reduced the possibility of publication bias. The inclusion of papers registered in electronic abstract systems was the first “quality filter,” thus ensuring a certain scientific level of conceptual and methodological rigor. The inclusion of non-English papers also avoided the Tower of Babel bias. For reducing rater bias, we included two pairs of raters during the selection process for relevant articles (i.e., abstract and full paper reading) and a third reviewer in the case of disagreement. We extracted information from both outcomes and on how they were measured, which allowed us to reduce bias of overestimated conclusions in the analyzed papers.
To control for bias in individual studies, for randomized controlled trial (RCT) studies, the risk of bias was measured using the Physiotherapy Evidence Database (PEDro) Scale (Portney & Watkins, 2015). We assessed the strength of the evidence using an adaptation of the modified Sackett criteria (Teasell et al., 2020) in which evidence is assessed on levels ranging from conflicting evidence to Level 1a (the highest level; Online Appendix B, Table B.2). We assessed the quality of qualitative studies using the clinical appraisal assessment tools (Critical Appraisal Skills Programme [CASP] Checklist; CASP, 2018).
Results
Study Selection
Figure 1 shows the results of the review process. We identified 4,548 studies; after removing duplicates, a total of 3,890 (85.5%, 3,890/4,548) studies remained for the title and abstract screening phase. In total, we included 34 studies for data extraction.
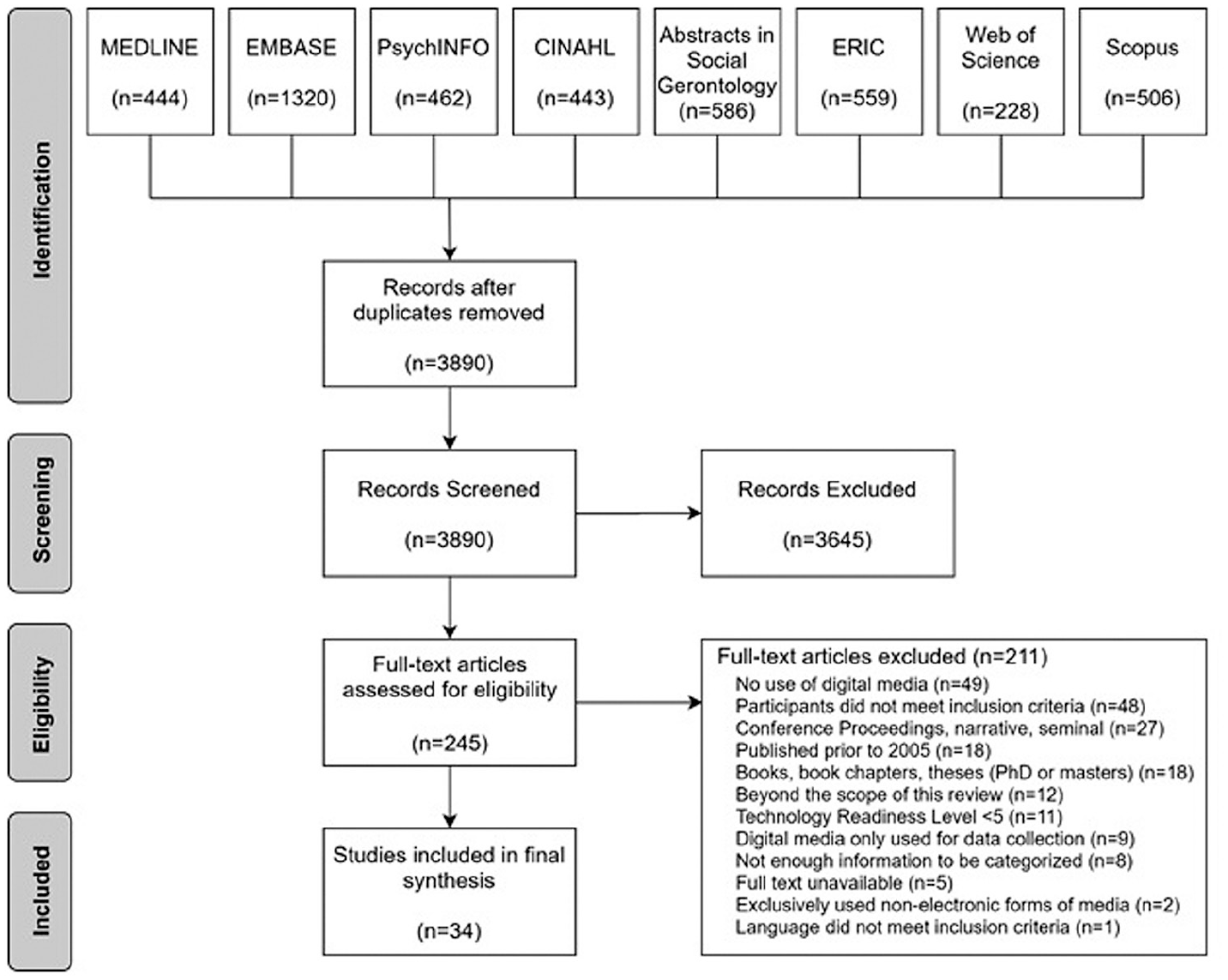
Scholarly literature search results.
Population
Older adults involved in digital storytelling studies
Overall, the studies included 510 participants in total. The majority or 70.2% of participants were female. Participants were older adults with a mean age of 72.90 (SD = 6.74) years. Mild cognitive impairment or dementia represented over half (52%, 13/25) of medical conditions; less common conditions each account for 4% to 8%, including diabetes, chronic conditions, cancer or at risk of getting cancer, visual impairment, depression, intellectual disability, Parkinson’s, and communication problems (see Table 1 for a detailed characterization of the population).
Population Characteristics: Older Adults Involved in Digital Storytelling Intervention.
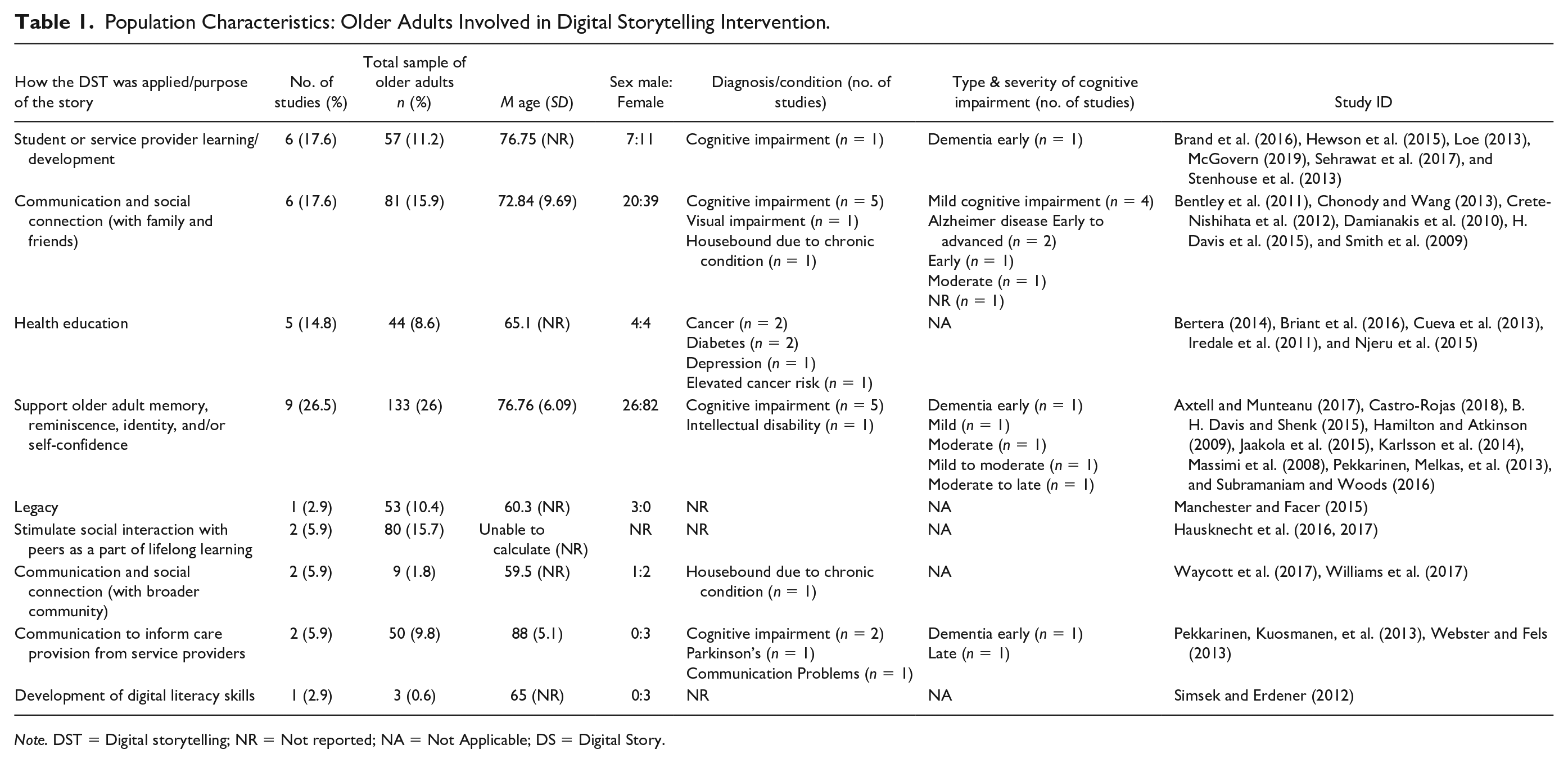
Note. DST = Digital storytelling; NR = Not reported; NA = Not Applicable; DS = Digital Story.
People involved in digital storytelling studies
In some studies, the process of creating and delivering digital storytelling involved people other than the older adults. Table 2 shows the characteristics of these individuals. Overall, their roles were characterized as (a) helping with the nontechnical development of the digital stories, (b) providing technical support to the older adult participants (e.g., in the digital story production process), and (c) receiving or observing the stories. In the first group, family members were the most commonly involved (25%, 11/44), followed by research team members who conducted the study, and formal care partners each accounted for 11.3% to 13.6%. In the second group, the research team members were the most commonly involved (36.4%, 12/33), followed by the participants themselves and media/digital storytelling specialists each accounted for 9.1% to 15.2%. In the third group, family members were the most commonly recipients of the digital stories (26.2%, 17/65), followed by the general public, formal carers, and friends each accounted for 7.7% to 16.9%.
Population Characteristics: People Involved in Digital Storytelling Studies.
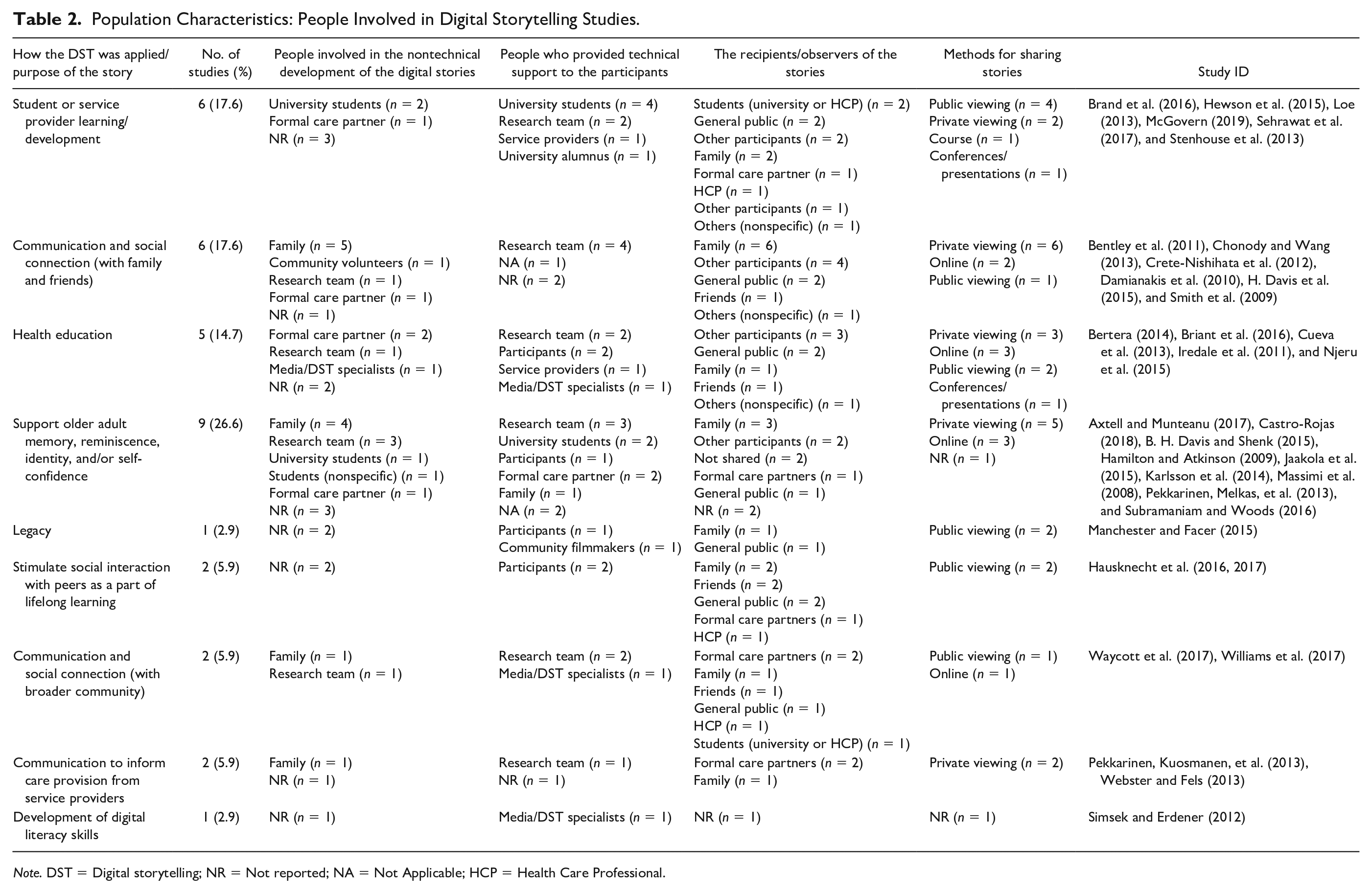
Note. DST = Digital storytelling; NR = Not reported; NA = Not Applicable; HCP = Health Care Professional.
Digital Storytelling: The Purpose of Stories and the Study Designs
Table 3 shows the purpose of digital stories and study designs. We found nine different categories of the purpose of stories. With respect to study designs, qualitative and mixed were the most common research designs used, accounting 1 for 81% (30/37). Case study (20.6%, 7/37) was the most common strategies of inquiry of quantitative design. We found no RCT so we did not assess any study with the PEDro Scale. Most of the qualitative studies seemed to use generic qualitative description (64.8%, 24/37), although not clearly stated in the manuscripts. Overall, the qualitative papers met 9.6% of the CASP criteria (ranging between 0% and 37.5%). Twelve studies were clinical oriented (32.4%, 12/37) and 13 aimed to determine the usability (35.1%, 13/37) of the technology used to create the digital stories.
Digital Storytelling: The Purpose of Stories and the Study Designs.
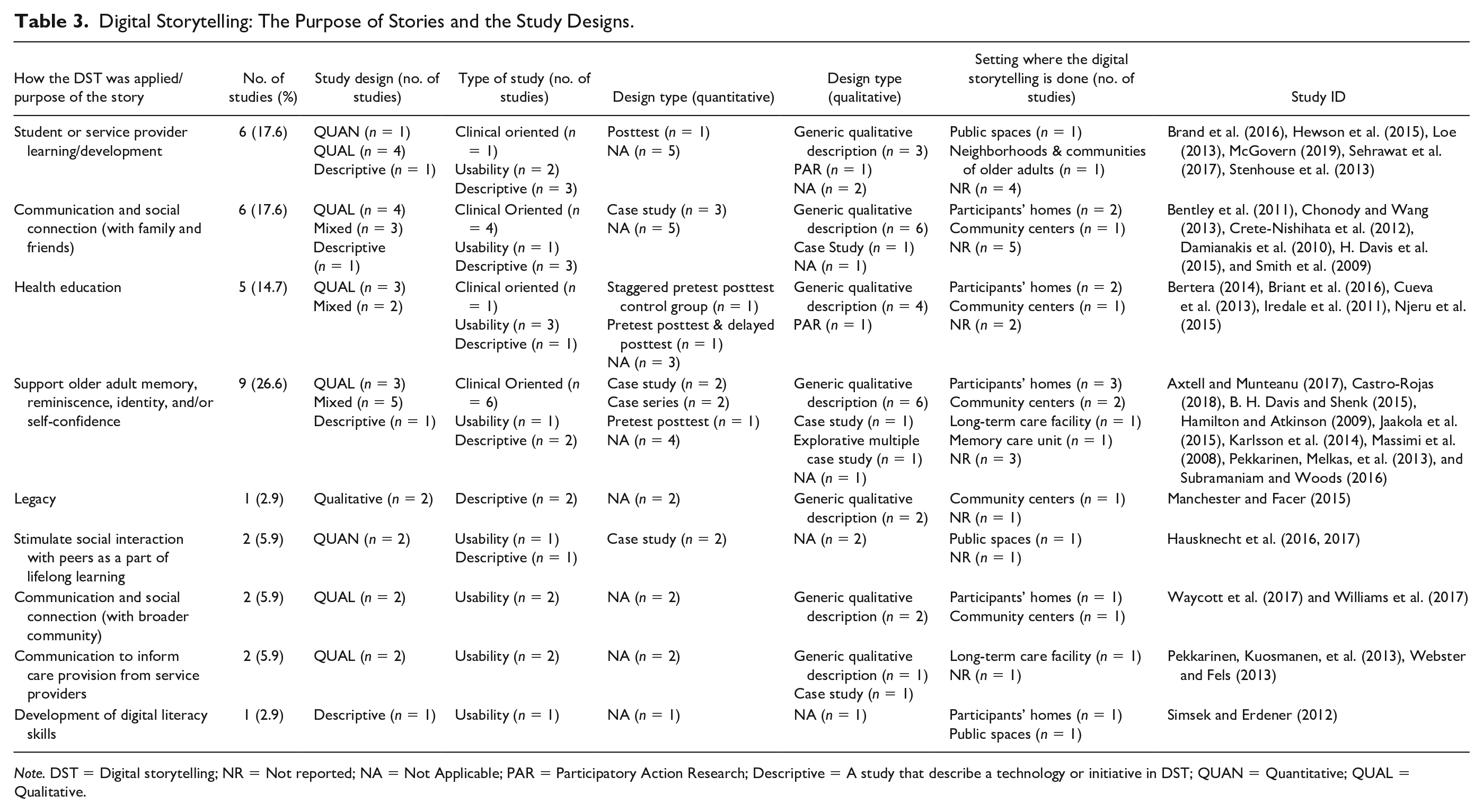
Note. DST = Digital storytelling; NR = Not reported; NA = Not Applicable; PAR = Participatory Action Research; Descriptive = A study that describe a technology or initiative in DST; QUAN = Quantitative; QUAL = Qualitative.
Digital stories created were predominantly related to past event (64%) although a few also focused on current (28%) and future events (2%). Regarding life events recalled, stories were related to personal experiences, general content, or era/time in a person’s life; the majority were about personal experiences (79%). Most common topics were life biography, important life moments, or events related to history (67%, 23/34). Other topics included the experience of having a health condition or caring for someone with a health condition (dementia, cancer; 9%, 3/34), and health information (screening, health promotion, disease management; 9%, 3/34).
Digital Storytelling Processes
The processes used to create digital storytelling are shown in Tables 2 and 4. The most common approach to create digital stories was one-on-one, that is, not in a group format (45.9%, 17/37), and the stories were mostly co-created (72.9%, 27/37) between older adults and the other people involved in the digital storytelling studies. Nearly 65% of the digital stories were stored as film, movie, video, or motion picture. Participants’ homes (24.3%, 9/37) and community centers (16.2, 6/37) were the most common settings. It took on average of 4.5 weeks, ranging from 1.62 to 4.57 weeks, to create a digital story and just over 8 months to assess the impact of digital stories.
Digital Storytelling Processes.
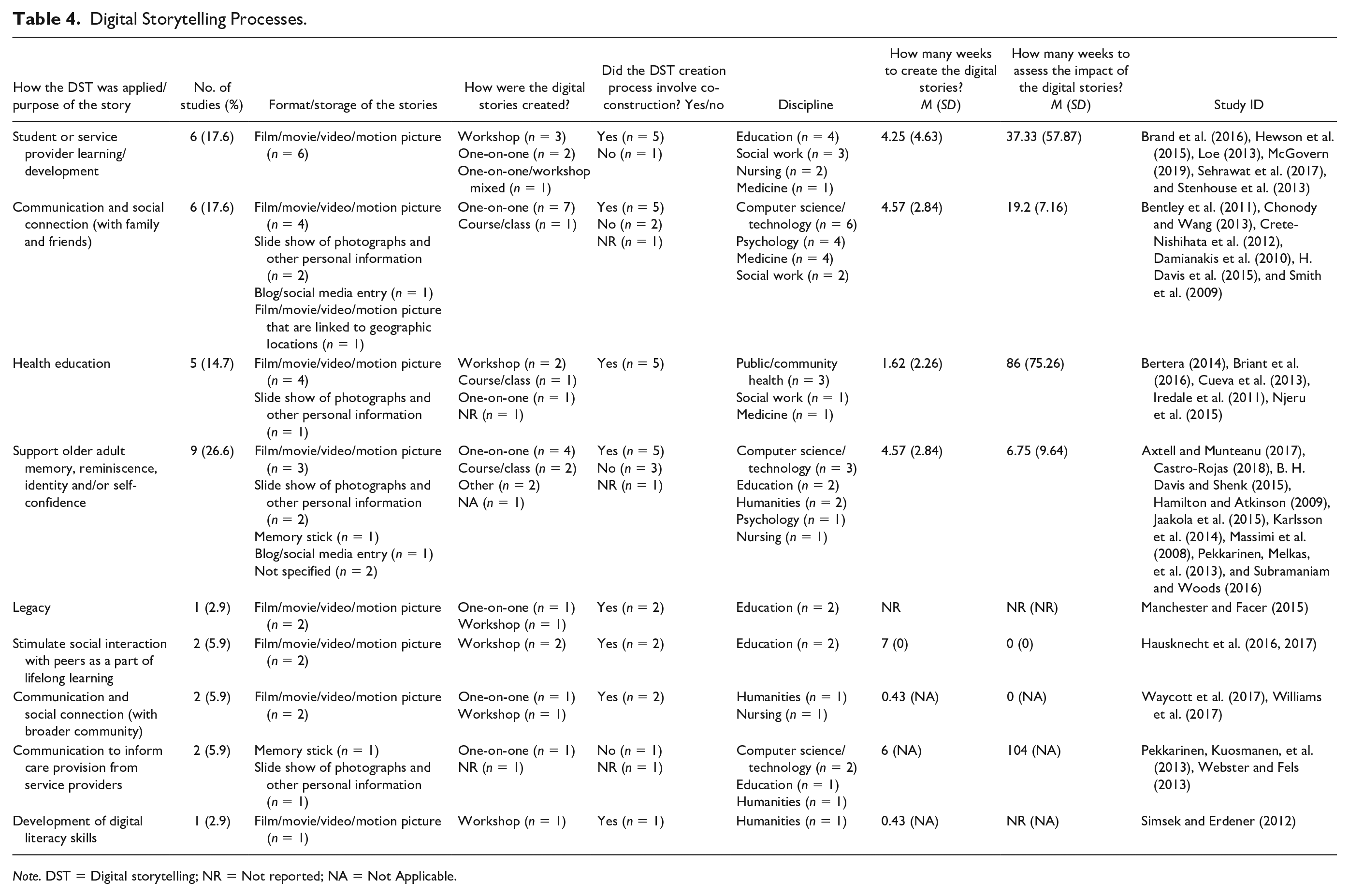
Note. DST = Digital storytelling; NR = Not reported; NA = Not Applicable.
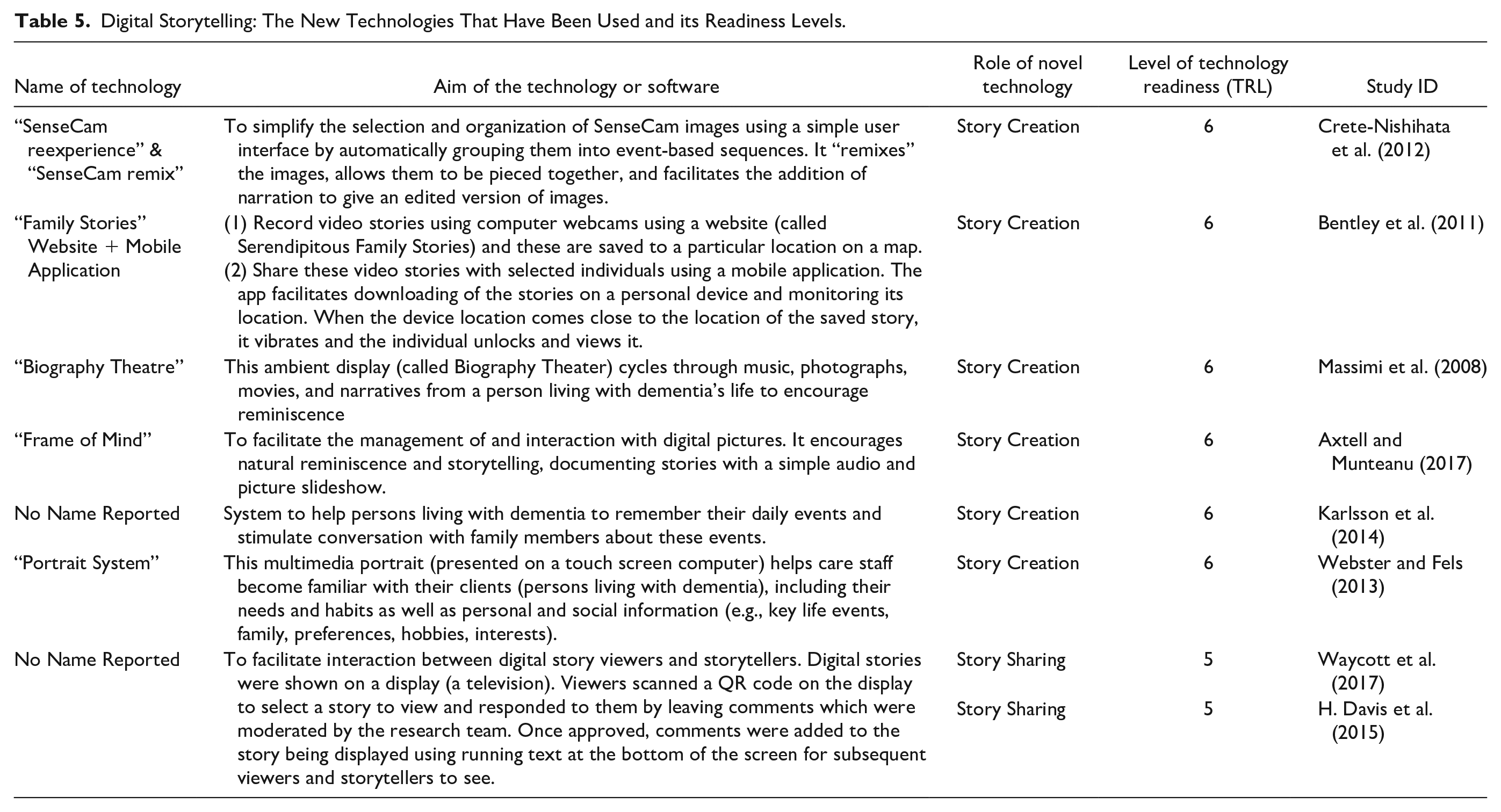
Digital Storytelling Technologies
Technologies used to create digital storytelling employed an amalgamation of commercial off-the-shelf 2 traditional video-editing tools (44.1%, 15/34) with new technologies for editing video tools (23.5%, 8/34). In the first group, the software used was Final Cut Pro (first developed by Macromedia Inc. and later Apple Inc), WeVideo (WeVideo, Inc.), Windows Movie Maker (Microsoft), iMovie (Apple Inc.), Sony Movie Studio (Sony Creative Software), and Adobe Premiere (Adobe Inc.). Table 5 shows the new technologies that have been developed to create digital stories, including the name of technology, the aim, the role, and the level of technology readiness. Overall, the technology readiness level of the new technologies for editing video tools in digital storytelling was 5.75 (0.46), meaning these technologies are at the “Technology Development” level (DOE, 2009, p. 9). In other words, the new technologies that have been used to create digital storytelling are at the laboratory scale.
Digital Storytelling: The New Technologies That Have Been Used and its Readiness Levels.
Outcomes of Digital Storytelling and Level of Evidence
Twelve studies reported clinical research (e.g., using digital storytelling as an intervention); only five of these studies reported outcome variables:
Bertera’s (2014) study evaluated a health education intervention using storytelling slide shows designed to impact diabetes and hypertension knowledge, attitudes, and practices among African American older adults. The Eating Decisions, the Diabetes Self-Efficacy Index, and the High Blood Pressure Self-Efficacy Index were outcome variables in this staggered pretest posttest control group study design. Findings suggest that when digital storytelling was used through an education program designed for behavioral change, all outcome variables significantly improved, at postintervention (Level 2 evidence).
Subramaniam and Woods’s (2016) study studied the acceptability and efficacy of using multimedia digital life storybooks with people living with dementia in care homes. Outcome measures included the Quality-of-Life Alzheimer’s Disease (QOL-AD) Scale, the Autobiographical Memory Interview (AMI), the Geriatric Depression Scale (Residential) (GDS-12R), and the Quality of the Caregiving Relationship Questionnaire (QCPR). Based on the findings from this pretest posttest study design (no control group), when digital storytelling was used with people living with dementia, the QOL-AD, AMI, GDS-12R, and the QCPR improved at postintervention (Level 4 evidence).
Karlsson et al.’s (2014) study explored the process of acceptance and integration of a digital photograph diary as a tool for remembering and conversing about daily life events among individuals living with dementia and their family members. The outcome variables were the Mini-Mental State Examination (MMSE), Computer-Based Verbal Episodic Memory Test (two-word lists with random words), and the Philadelphia Geriatric Center Morale Scale (PGCMS). Based on the findings from this explorative multiple case study design, the use of DPD has no effect on cognitive function, well-being, and memory function of older adults living with dementia (Level 4 evidence).
Davis and Shenk’s (2015) study explored digital storytelling to increase engagement and support the retention of identity in older adults living with dementia. The outcome variable was engagement with the digital stories measured through physiological data (e.g., heart rate), time spent viewing each video, preferences between videos with personal or general content, and language patterns. Based on this case study’s findings, participants were engaged in digital storytelling activities and that the videos with generic content elicited more diverse language in participants than those with personal content (Level 5 evidence). Authors did not report how identity was measured nor results associated with this construct.
Massimi et al.’s (2008) study examined how the novel “off the desktop” technologies to aid in memory and conversation may help remediate identity. Authors used the Geriatric Depression Scale-30 (GDS-30), the Goldberg Anxiety Scale (GAS), the Apathy Evaluation Scale–Informant (AES-I), the Self-Image Profile–Adult (SIP-AD), the Autobiographical Memory Interview (AMI), the Mini-Mental State Exam (MMSE), the Informant Questionnaire of Cognitive Decline in the Elderly (IQCODE), and the Modified Caregiver Strain Index (CSI) as outcome variables. Based on this exploratory case study with a single participant, the use of digital storytelling improved sense of identity (SIP-AD), reduced apathy (GDS-30, GAS, AES-I), and changed the participant relationships and communication with the care partner (CSI; Level 5 evidence). No change in general cognition or autobiographical memory was observed.
Discussion
Our systematic review addressed the question how has digital storytelling been used with older adults with typical aging, and with mild cognitive impairment, or dementia? We examined the range and extent of the use of digital storytelling in older adults and their care partners, described the processes and technologies used and their readiness level, and identified the evidence and the associated outcomes. We included 34 studies, and overall, our findings indicate that there are nine purposes of digital storytelling, the most common of which was to support memory, reminiscence, identity, or self-confidence. The majority of stories focused on personal experiences that occurred in the past and were co-created on a one-on-one basis in participants’ homes. The stories were mostly in the form of film, movie, video, or motion picture and were developed over approximately 4.5 weeks, and the technologies used to create digital stories employed commercial off-the-shelf traditional video-editing tools and novel video-editing tools. Overall, the technology readiness level of the novel technologies was medium-low. The level of evidence for effectiveness was low for the use of digital storytelling as intervention to support older adults and their care partners.
Purpose of Digital Storytelling Studies
There is a general interest in research exploring the use of digital storytelling as a therapeutic means to improve cognitive, emotional, or affective skills in older adults living with mild cognitive impairment or dementia, followed by its use to facilitate conversation and social connection between individuals living with dementia and their families. This is aligned with the finding that the majority of the content was personal (e.g., life biography, an important moment in life, or events related to history) and related to past events in the participants’ lives, which is commonly used in reminiscence therapy. Although the evidence was low, some findings suggest avenues for future research. Damianakis and colleagues (2010) found that the use of digital storytelling triggered memories in older adults living with mild cognitive impairment or dementia, which provided the family with new insights about the participant’s life story, which in turn, eased the interaction with the loved one living with dementia. Participants living with mild cognitive impairment were less likely view the triggers as early or lost memories than those living with dementia. Davis and Shenk (2015) reported that older adults living with dementia preferred to develop digital stories in the form of videos with personal content rather than with generic content. However, the videos with generic content elicited more diverse language patterns than the personalized video. Crete-Nishihata and colleagues (2012) found both positive and negative psychosocial outcomes when SenseCam technology facilitated review of images of daily life events. Personal stories based on personal life experiences may involve re-elicitation and consideration of sometimes painful memories (Lazar et al., 2014). Reminiscing can potentially cause emotional distress when older adults living with dementia fail to recognize themselves, others, or personal events in personal photographs (Gowans et al., 2004). On the contrary, when only generic material is used, older adults living with dementia preferred personal materials to be used in reminiscence therapy (Alm et al., 2004). Thus, whether personal or generic content is more effective for reminiscence therapy, including when digital technologies are utilized, remains unknown.
Processes and Methods Utilized to Develop the Stories
A co-creation approach was used when participants lived with dementia or mild cognitive impairment (Crete-Nishihata et al., 2012; Damianakis et al., 2010; Pekkarinen, Melkas, et al., 2013; Smith et al., 2009; Stenhouse et al., 2013; Subramaniam & Woods, 2016), other chronic diseases (Briant et al., 2016; H. Davis et al., 2015; Njeru et al., 2015; Waycott et al., 2017), or an intellectual disability (Hamilton & Atkinson, 2009). Co-creation is a “sophisticated, value-based, context-driven, collaborative effort to develop new paradigms, products, and services to satisfy human wants” (Akhilesh, 2017, p. 2). Co-creation was observed in several ways: (a) support given by facilitators to the older adults to create the digital story (Crete-Nishihata et al., 2012; H. Davis et al., 2015; Hamilton & Atkinson, 2009; Pekkarinen, Melkas, et al., 2013; Stenhouse et al., 2013); (b) participatory design (Damianakis et al., 2010; Njeru et al., 2015; Smith et al., 2009; Subramaniam & Woods, 2016); and (c) active engagement of older adults during the digital storytelling process (Briant et al., 2016; Waycott et al., 2017). Stenhouse et al. (2013) proposed that digital storytelling is an arts-based method of representing experience of a person living with dementia. Waycott et al. (2017) suggested that co-creation is not so much about ensuring that participants are involved in every aspect of the digital storytelling creation process, but that participant find meaning in their participation, regardless of the extent of their involvement. It is more important how participants see themselves in the co-creation process than the amount of time they spend toward the overall product or the technical aspects of it.
Technologies Used in Digital Storytelling
Mainly commercial off-the-shelf technologies were used in digital storytelling. Only seven papers reported novel technologies. All but one were developed to assist with story creation. Most are at a laboratory scale of technology readiness (i.e., reported results are from test in a laboratory environment and technologies are not commercially available). Such notable technologies include software that automatically creates an animated slideshow of the pictures older adults selected while looking at their stored pictures on a mobile device synchronized with an older adult’s voice (Axtell & Munteanu, 2017). Another example is an algorithm that uses recent first-person perspective photos automatically captured using SenseCam (a lifelogging device) to create a digital story. This algorithm automatically selects 24 relevant pictures, synchronizes them with the event’s narration by the older adult’s partner, and thus holds promise not only for digital storytelling but also for an autobiographical memory assistive technology for people with mild cognitive impairment or dementia (Crete-Nishihata et al., 2012). Such technologies are promising as they may enable older adults with cognitive or motor impairments to easily create a digital story, requiring less support from others with technical skills.
Evidence and the Associated Outcomes of Digital Storytelling
The level of evidence provided in the quantitative clinical studies was low. Only five studies reported outcome variables, among which only one study had a control condition. The low level of evidence seems to be associated with the research designs selected rather than to the technologies used in the studies. Interestingly, the study providing the highest level of evidence (Hewson et al., 2015) used a prolonged amount of time to assess the impact of digital storytelling (i.e., 156 weeks or around 3 years). More rigorous research able to demonstrate effectiveness of using digital storytelling interventions on outcome variables in a shorter time span is also beneficial with older adults whose chronic conditions decline rapidly.
Qualitative studies are mainly devoted to exploring aspects of the use of digital storytelling such as (a) the topic or content of the stories (Castro-Rojas, 2018; H. Davis et al., 2015), (b) strategies used by older adults to gather and choose data and the ethical issues related to dependence on others for support in the processes of digital curation (Manchester & Facer,015), (c) whether of or not the stories were shared (Cueva et al., 2013), (d) the experience with the process of creating the stories (Williams et al., 2017), and (e) the role and functions of the technologies (Pekkarinen, Kuosmanen, et al., 2013). There was minimal detail on the methods used for collecting and analyzing the data; this compromises the credibility, dependability, confirmability, and transferability in most of the papers. Thus, results from these studies are mainly anecdotal.
Finally, although the literature has shown promise for storytelling activities as interventions for promoting positive psychosocial outcomes in older adults living with dementia, little is known about the best format for using storytelling interventions (e.g., paper-based or digital; Smith et al., 2009), and no study in this literature review addressed such comparison.
Limitations
Despite our efforts to conduct an exhaustive search of health databases, expand the timeframes of the published studies, and be as inclusive as possible when selecting the target population, we may have missed papers that were not published nor indexed in these databases.
Conclusions and Clinical Practice Implications
The highest level of evidence for digital storytelling was as a tool to improve knowledge, attitudes, and practices related to diabetes and high blood pressure in healthy older adults (Bertera, 2014). The positive results found in that study may be in part because the digital stories were produced using only photos and recorded voices of community members that represent the target population, that is, low-income African American older adults. Thus, digital storytelling may be a way of creating materials for health education and behavioral change to reach specific populations. The level of evidence is low for digital storytelling as a therapeutic means to improve cognitive, emotional, or affective skills in older adults living with mild cognitive impairment or dementia. Thus, clinicians need to consider this level of evidence if the goal is to improve certain abilities in clients living with dementia.
Co-creation of digital stories emerged as a common strategy that could be implemented in clinical practice. Digital storytelling can be used as a tangible way to uphold personhood among persons living with dementia (McKeown et al., 2017). Communication and relational skills inherent in co-creation approaches to digital storytelling can build a therapeutic relationship, bond, rapport, comfort, and trust between professionals and clients. More research would help support digital storytelling as a practice widely used by rehabilitation professionals to facilitate communication and interaction between persons living with dementia and their loved ones.
One barrier that may prevent the widespread use of digital storytelling in clinical and home settings is the need for video editing to produce digital stories. New technologies that reduce the need for video editing would support therapists and clients in the technical aspect of the digital story editing process. This would allow the therapist to focus in the communication and relationship with the client, which may be more useful for achieving therapeutic goals. Similarly, new technologies would support family and care partners in using digital storytelling to facilitate communication with older adults living with dementia.
Supplemental Material
sj-pdf-1-jag-10.1177_07334648211015456 – Supplemental material for Digital Storytelling in Older Adults With Typical Aging, and With Mild Cognitive Impairment or Dementia: A Systematic Literature Review
Supplemental material, sj-pdf-1-jag-10.1177_07334648211015456 for Digital Storytelling in Older Adults With Typical Aging, and With Mild Cognitive Impairment or Dementia: A Systematic Literature Review by Adriana Maria Rios Rincon, Antonio Miguel Cruz, Christine Daum, Noelannah Neubauer, Aidan Comeau and Lili Liu in Journal of Applied Gerontology
Footnotes
Acknowledgements
We thank Maria Tan, Librarian at the John W. Scott Health Sciences Library at the University of Alberta for her guidance. We also thank research assistants for their help in conducting this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Consortium on Neurodegeneration in Aging (CCNA).
Ethical Approval
Ethics approval was not required for conducting this literature review.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.