
Abstract
Black older adults’ (BOAs) experience of loneliness differs from other ethnic groups because of the disproportionate disadvantages faced across their life course. This scoping review aimed to describe the range of research on loneliness or subjective social isolation among BOAs, identifying the contributing factors to loneliness in this population, based on Weiss’ Social provision Framework. Of the 15,345 initial retrieved citations from seven databases and corporate websites, we included 27 studies conducted in the USA, Nigeria, South Africa, Ghana, Canada, the United Kingdom, and Uganda. Studies reporting on BOAs’ experience of loneliness focused on the influence of attachment, social integration, opportunity for nurturance, reassurance of worth, guidance, socio-economic factors, health-related factors and behaviors, and technology, media device possession and usage. There is a need for future studies to identify which social provisions (when targeted) could reduce loneliness, allowing clinicians to develop relevant interventions.
What this paper adds
This is the first review to provide global evidence on loneliness among Black older adults (BOAs). This review highlights the unique experience of loneliness among Black older adults as a collective group from a global perspective and aspects requiring more research and practice attention. This review outlines the Social Provision Framework as a potential tool in understanding the trajectorial experience of loneliness among Black older adults and the significance of relational gains.
Applications of study findings
Understanding the unique ways loneliness affects BOAs would help program and service developers design interventions that adequately address the needs of such minority groups. The findings of this review mapped around the social provisions will enable clinicians, policymakers, and researchers to identify which of the social provisions (when targeted) could meaningfully reduce loneliness among older adults in general. The findings underline areas needing further research attention and the need for empirical studies of any design that will specifically explore or investigate how loneliness affects BOAs, particularly in countries like Canada, where very few studies have focused on this interest.
Introduction
Loneliness is a serious public health issue that affects many older adults globally. Loneliness is defined as a subjective negative feeling that is associated with the lack of a wider social network (social loneliness) or the absence of desired companionship (emotional loneliness) (Valtorta & Hanratty, 2012). Loneliness can be experienced at any age, but progresses non-linearly across middle and older age, with the highest prevalence among older adults aged 80 years and older (Dykstra, 2009). In the literature, loneliness has often been used interchangeably with social isolation; however, Wigfield et al. (2020) advocated examining the terms individually. They define social isolation as an objective measure of the quantity of social contact available to an individual, while loneliness is the subjective negative feeling because of a lack of meaningful relationships (Wigfield et al., 2020). Our paper focuses on loneliness or subjective social isolation, not objective social isolation.
Loneliness increases the risk of poor health outcomes, including poor quality of life, poor cognitive functioning, poor physical functioning, and increased mortality (Courtin & Knapp, 2017). Increased loneliness was positively associated with higher systolic blood pressure among older adults in the USA (Hawkley et al., 2010). Among older Nigerians in a qualitative study, loneliness was linked to suicidal thoughts (Ojembe & Kalu, 2018). Additionally, individuals experiencing loneliness are 26% more likely to die prematurely than those with healthy social relationships (Holt-Lunstad et al., 2015) and are more likely to experience hearing loss, living alone, chronic illness, and the loss of friends or family (Centers for Disease Control and Prevention, 2020).
Although the studies on loneliness in the older-adult population report findings on the general population of older adults, ethnic minority older adults experience this phenomenon in unique ways. While the term ethnic minority conceals significant heterogeneity, evidence suggests important patterning of loneliness by ethnicity among the older adult population (Salway et al., 2020; Victor et al., 2012), with Black older adults (henceforth BOAs) showing low levels of social connection and support (Taylor & Nguyen, 2020). A UK study by Hayanga et al. (2021) found that Black and Asian adults older than age 65 years are nearly twice as likely (9% and 7%, respectively) to report having no close friends compared to white and other ethnic older adults of the same age (4%). Another study in the US found that race significantly moderated the relationship between loneliness and depressive symptoms among BOAs (Taylor & Nguyen, 2020). These suggest that older ethnic minority adults may be more vulnerable to loneliness and social isolation due to their country of birth, socio-cultural and community contexts than older adults from other popular cultures or ethnic groups. Additionally, social support and relations as independent predictors of loneliness have shown larger health effects for Black than White older adults (Assari & Lankarani, 2018), further highlighting the importance of understanding loneliness and its contributory factors among BOAs.
Khan (2014) noted that despite the high rates of loneliness reported in older ethnic minority adults, they are frequently assumed to be protected from social isolation and loneliness since they are more likely to live in multigenerational families with traditional family customs and intergenerational supports. This stereotypical or taken-for-granted assumption may tend to stem from the association of ethnic minority populations within collectivist cultures that value interdependence and are oriented toward obligation, cohesion, and commitment (Burholt et al., 2018). These stereotypes are harmful because they fail to recognize the various experiences and needs of different ethnic minority older adults, elevating their risk of loneliness and social isolation. In addition, the stereotypes sometimes generate structural and institutional hindrances that lead to poverty, unemployment, poor housing, internalized racism, and interpersonal factors (Kissoon, 2010; Taylor & Nguyen, 2020). Moreover, processes and structures of exclusion linked to individuals with ethnic minority identities (e.g., cumulative exposure to racial discrimination) increase their risk of social isolation and loneliness (Wallace et al., 2016).
There has been considerable research and reviews, including scoping, systematic, and integrated reviews on loneliness among older adults, such that researchers now conduct “rapid review” of reviews on loneliness (Boulton et al., 2021). Recent reviews have primarily focused on interventions to reduce loneliness among older adults in the community (Fakoya et al., 2020; Gardiner et al., 2018; O’Rourke et al., 2018) and in long-term care facilities (Quan et al., 2020). Other reviews were concerned with defining the concepts of loneliness, health, and social isolation (Courtin & Knapp, 2017; Malcolm et al., 2019), identification of risk factors for loneliness among older adults (Dahlberg et al., 2021), and the public health consequences of loneliness (Leigh-Hunt et al., 2017). A few reviews (Johnson et al., 2019; Shorey & Chan, 2021) centered on loneliness among ethnic minorities. While Johnson and colleagues conducted a scoping review exploring social loneliness among older adult immigrants and refugees (e.g., South Asians) in Canada, Shorey and Chan (2021) conducted a systematic qualitative review exploring the experiences and needs of socially isolated lonely Asian older adults. Both reviews described similar themes, including association with older adults' well-being, dealing with social isolation and loneliness, loss of social support, wish lists of older adults, the unique experiences of Asian older adults in western countries (Shorey & Chan, 2021), and loss, living arrangement, dependency, barriers and challenges, and family conflict (Johnson et al., 2019). They highlighted the cultural and contextual factors influencing loneliness among minority ethnic groups. However, they used “social isolation” and “loneliness” interchangeably, which have different meanings and did not include older adults from other ethnic groups, thereby limiting the application of their findings to understanding loneliness among BOAs.
To the best of our knowledge, no reviews have focused on loneliness among BOAs globally. Because it is not clear what is generally available in the literature and what the gaps are in addressing loneliness among this group, the authors determined that a scoping review (instead of a systematic review) was more appropriate and critically needed to understand unique and accumulated factors predisposing this group to loneliness. Our review aims to describe the range of research on loneliness among BOAs, identifying the contributory factors to loneliness in this population as presented in the global literature. This will inform future research and practice that focuses on designing interventions that will address the specific needs of this group. This will also enhance their general differential experience of aging, health, and well-being, since loneliness is a growing concern among this population in many parts of the world, including Africa, the US, and the UK (Ojembe & Kalu, 2018; Taylor, 2019; Victor et al., 2021).
Methods
The protocol has been published elsewhere (Ojembe et al., 2021) and was registered at (https://doi.org/10.7565/SSP.V4.5748). Summarily, this scoping review was guided by the methodological framework proposed by Arksey and O’Malley (2005) and was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-Scr) (Tricco et al., 2018). The following research questions guided the review: a) What is the range of research on loneliness among Black older adults? b) What are the contributory factors for loneliness in this population as presented in the global literature?
Search Strategy and Study Selection
Comprehensive search strategy, study selection, and data extraction processes have been published in the protocol paper (Ojembe et al., 2021). The search strategy was developed in consultation with a social science librarian. Summarily, seven databases, including Ageline, PsychInFo, Cochrane library, PubMed, CINHAL, Web of Science, and SocIndex and Social Services Abstracts, were searched using the search strategy described in Online Appendix 1 with no year restriction.
All citations were exported into Rayyan QCRi(c) for removing duplicates and study screening. Study selections were conducted in two stages: title/abstract and full-text screening, with predefined inclusion and exclusion criteria in Box 1. Six raters (CD, CP, TO, OO, AI, and MJ) independently performed pilot testing of the title/abstract and full-text screening at each stage to determine inter-rater reliability. Raters' kappa scores for both title/abstract and full-text screening were 0.92 and 0.94, respectively, indicating strong agreement (Landis & Koch, 1977). Retrieved articles were divided among the six raters. Disagreements were resolved in research meetings. An article was included if: a. It investigated the experiences/risk factors of social and/or emotional loneliness among Black older adults (Africa and the Caribbean) or some aspect of loneliness (e.g., feeling alone, reduced, or no social support or contact). We define loneliness as a subjective negative feeling resulting from a lack of a meaningful or intimate social and/or emotional relationship. This definition differs from social isolation, an objective measure of social contact available to an individual. b. It utilized qualitative, quantitative, or mixed-method methodologies. Qualitative studies were included if they focused on loneliness among BOAs, and we were able to extract the data on the specific experience of loneliness of Blacks that participated in the study, even if it is just one person. Quantitative studies were included if they described risk factors for loneliness among BOAs, specific interventions to reducing loneliness among BOAs, conducted (a) sub-analysis for BOAs or use race (black) as a risk factor or predictor in their loneliness studies, and (b) BOAs constituted 70% of the study population. Authors were contacted three times requesting specific data (qualitative or quantitative) for BOAs, and articles whose author(s) did not respond after the third attempt were excluded. c. The mean age of the study population was 55 years and above. d. Published in the English language. e. Peer-reviewed and gray literature articles (e.g., organizational reports, theses, etc.) Articles were excluded if (a) they explored objective social isolation, as defined above, or factors related to social isolation—for example, depression or social isolation as synonymous with loneliness, and (b) they are opinion papers with no empirical data. There was no year restriction on both during database searches [i.e., each database will be searched from inception till 2021] and in selecting the included articles provided they meet the criteria.BOX 1: Inclusion & Exclusion Criteria
Data Extraction
Data extraction was done using an adapted form from a previous review by Kalu et al. (2021) but was modified to suit the research questions. The following information was extracted: authors name(s), year of publication, the country study was conducted, study aims/research questions/hypothesis, the study settings, type of study (qualitative, quantitative, or mixed-method), study design, sampling method, participants characteristics (e.g., the number of participants, mean age of the participants, sex/gender), study themes (if qualitative), study findings (if quantitative or mixed-method), policy statements, clinical implication statements, and future research statement. For quantitative findings, we extracted the mean (SD) scores and prevalence (%) of loneliness, the odds ratio, beta and the 95% confidence interval highlighting the association between loneliness and other variables (e.g., age, gender) reported in the included studies. For a more extensive description of the method, see the protocol paper—Ojembe et al. (2021), (p. 5). The six raters independently pilot tested the data extraction sheet, and any disagreements were resolved by discussions during research meetings.
Data Synthesis
Social provisions and other emerging aspects across included studies.
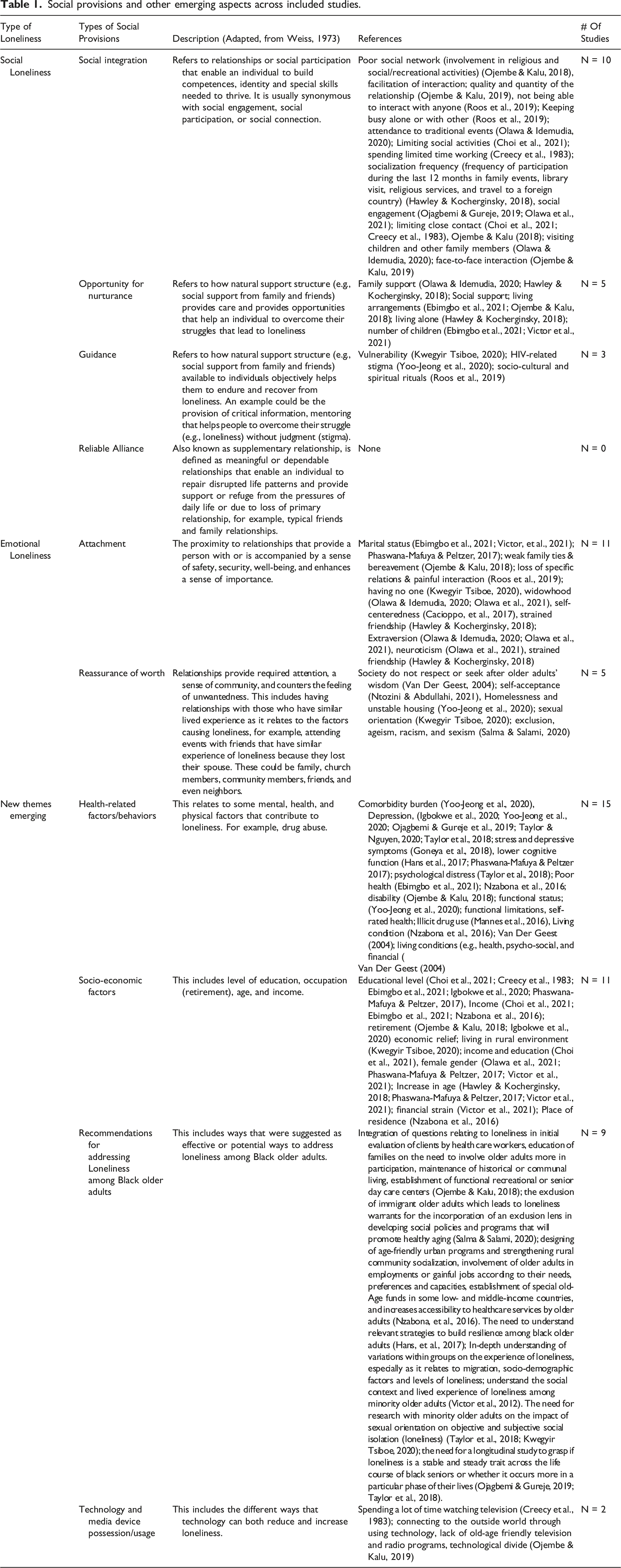
Two authors (BO and MK) independently reviewed the included studies’ findings and mapped their findings across Weiss’s six provisions stated above. For instance, a qualitative study, Roos et al. (2019) provided several themes as conditions for loneliness among South African women. Such themes include but are not limited to “loss of specific relationships,” “inability to interact with anyone,” and “the impact of painful social interactions.” Using the above qualitative example, (BO and MK), each mapped the themes, “inability to interact with anyone” on social integration, while “loss of specific relations” and “painful social interaction” were mapped across attachment. Similarly, a quantitative study by Olawa and Idemudia (2020) reported that widowhood and extraversion were significant predictors of loneliness among men, while family support significantly lowers the risk of loneliness among women. BO and MK independently mapped widowhood, extraversion, and family support across attachment, social integration, and opportunity for nurturance using this quantitative example. These processes were repeated for all articles. Afterward, they both met to compare their mapping, and any disagreement was discussed with the most senior author. Extraneous data were formulated into a new theme, undergoing iterative interpretation using inductive and thematic analysis techniques.
Result
Of the 15,345 retrieved citations from databases and corporate websites, 1854 were duplicates. After removing duplicates, 13,474 citations underwent title/abstract screening, 13,341 were excluded leaving 150 articles that underwent full-text screening, and finally, 27 articles were included (See Figure 1). PRISMA Flowchart of included articles. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/.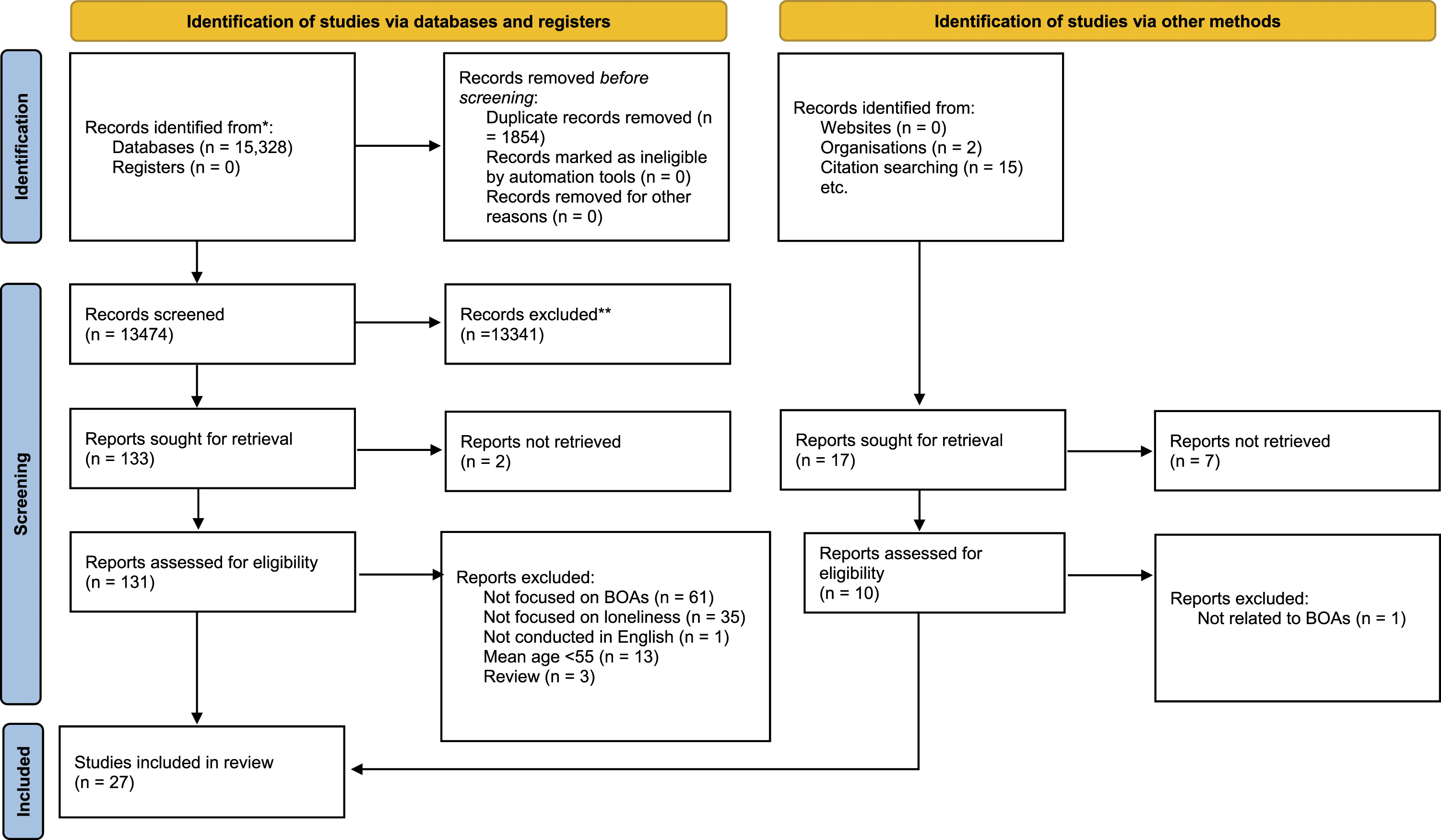
Characteristics of the Articles Included
The 27 included articles were peer-reviewed and published in the USA (n = 11), Nigeria (n = 7), South Africa (n = 3), Ghana (n = 2), Canada (n = 1), the United Kingdom (n = 2), Uganda (n = 1) (See Online Appendix 2a, 2b and 2c). Reported mean age ranged from 55.8 years (Mannes et al., 2016) to 77.3 years (Abedini et al., 2020).
Recruitment
Most of the articles (n = 23, 88.9%) recruited participants from the community; the remaining four papers recruited participants from hospitals (n = 3) (Han et al., 2017; Mannes et al., 2016; Yoo-Jeong et al., 2020) and care home (n = 1) (Roos et al., 2019). Most studies (n = 17, 63.0%) were conducted in both rural and urban settings; eight studies were conducted in the urban setting only (Han et al., 2017; Ntozini & Abdullahi, 2021; Ojembe & Kalu, 2018, 2019; Phaswana-Mafuya & Peltzer, 2017; Roos et al., 2019; Salma & Salami, 2020) and two studies were conducted in a rural setting (Kwegyir Tsiboe, 2020; Van Der Geest, 2004). Among the qualitative studies, the sample size ranged from 10 (Kwegyir Tsiboe, 2020) to 67 (Salma & Salami, 2020). The sample size of the quantitative and mixed-method studies ranged from 96 (Mannes et al., 2016) to 6884 (Nzabona et al., 2016).
Study Population
Twenty-four studies included “apparently” healthy older adults. However, three studies included older adults with specific health conditions such as HIV/AIDS (Han et al., 2017; Mannes et al., 2016; Yoo-Jeong et al., 2020). Among studies conducted in the UK, South Africa, and the US, the % of BOAs ranged from 8.9% (Abedini et al., 2020) to 100% (Creecy et al., 1983; Mannes et al., 2016). In six articles, BOAs’ population was less than 50% of the study sample (Abedini et al., 2020; Choi et al., 2021; Hawkley & Kocherginsky, 2018; Taylor & Nguyen, 2020; Victor et al., 2012, 2021), and was 50% or more in nine articles (Creecy et al., 1983; Gonyea et al., 2018; Han et al., 2017; Mannes et al., 2016; Ntozini & Abdullahi, 2021; Phaswana-Mafuya & Peltzer, 2017; Savage et al., 2021; Taylor et al., 2018; Yoo-Jeong et al., 2020). A qualitative study conducted with immigrant Muslim older adults in Canada noted that the study population was predominantly from the Middle East/North Africa, South Asia, and East Africa (Salma & Salami, 2020). However, the exact sample of the population represented by each of the mentioned regions is unclear, but some of the quotes included were from older adults from Africa (Ethiopia). The older adults that participated in studies conducted in Ghana, Nigeria, Uganda and one study from South Africa (Roos et al., 2019) were 100% Black.
Study Design
Of the 27 articles included, 19 were quantitative studies, while six were qualitative and two were mixed-method studies. The quantitative studies employed either cross-sectional (n = 13) or longitudinal (n = 6), while the qualitative studies employed either phenomenology (n = 4; (Kwegyir Tsiboe, 2020; Ojembe & Kalu, 2019, 2018; Van Der Geest, 2004) or participatory action research designs (Salma & Salami, 2020). Roos et al. (2019) did not provide the qualitative study design but reported that a critical-realist ontology underpins their study. The two mixed-method studies did not state their specific design (Ebimgbo et al., 2021; Nzabona et al., 2016).
Instruments Used to Measure Loneliness
Among the 21 quantitative and mixed-method studies, 12 (57%) studies used original or modified UCLA in assessing loneliness (Abedini et al., 2020; Cacioppo et al., 2017; Ebimgbo et al., 2021; Gonyea et al., 2018; Hawkley & Kocherginsky, 2018; Igbokwe et al., 2020; Mannes et al., 2016; Ntozini & Abdullahi, 2021; Ojagbemi & Gureje, 2019; Olawa et al., 2019; Olawa & Idemudia, 2020; Taylor & Nguyen, 2020). The remaining eight studies used a modified version of the de Jong-Gierveld Loneliness Scale (Han et al., 2017), a 20-point index measuring social contact (Creecy et al., 1983), the Social Isolation component of a Patient-Reported Outcomes Measurement Information System (Yoo-Jeong et al., 2020), single-item question, for example, “did you feel lonely for much of the day yesterday or in the past seven days?” (Choi et al., 2021; Phaswana-Mafuya & Peltzer, 2017; Taylor et al., 2018; Victor et al., 2012), or two-item questions, for example, “are there times when you have a feeling of loneliness and what do you think needs to be done to reduce this loneliness?” (Nzabona et al., 2016). One study used a single-item question and the de Jong-Gierveld Loneliness Scale to measure loneliness (Victor et al., 2021).
Categorization of Articles Using the Social Provision Framework
When categorized into the six social provisions (see Table 1), focusing on social and emotional loneliness as stipulated by Weiss’ SPF, findings from the included papers were categorized under “attachment” (n = 11) and “social integration” (n = 10), followed by “Opportunity for Nurturance” (n = 5), “reassurance of worth” (n = 4), “Guidance” (n = 3), and “Reliable Alliance” (n = 0). Findings that could not fit into the categories listed above, were categorized under “New emerging themes,” comprising “health-related factors and behaviors” (n = 15), “socio-economic factors” (N =11), “recommendations” (n = 9), and “technology and media device possession and usage” (N = 2) (see figure 2). Conceptual figure depicting social provisions and other contributory factors for loneliness among BOAs.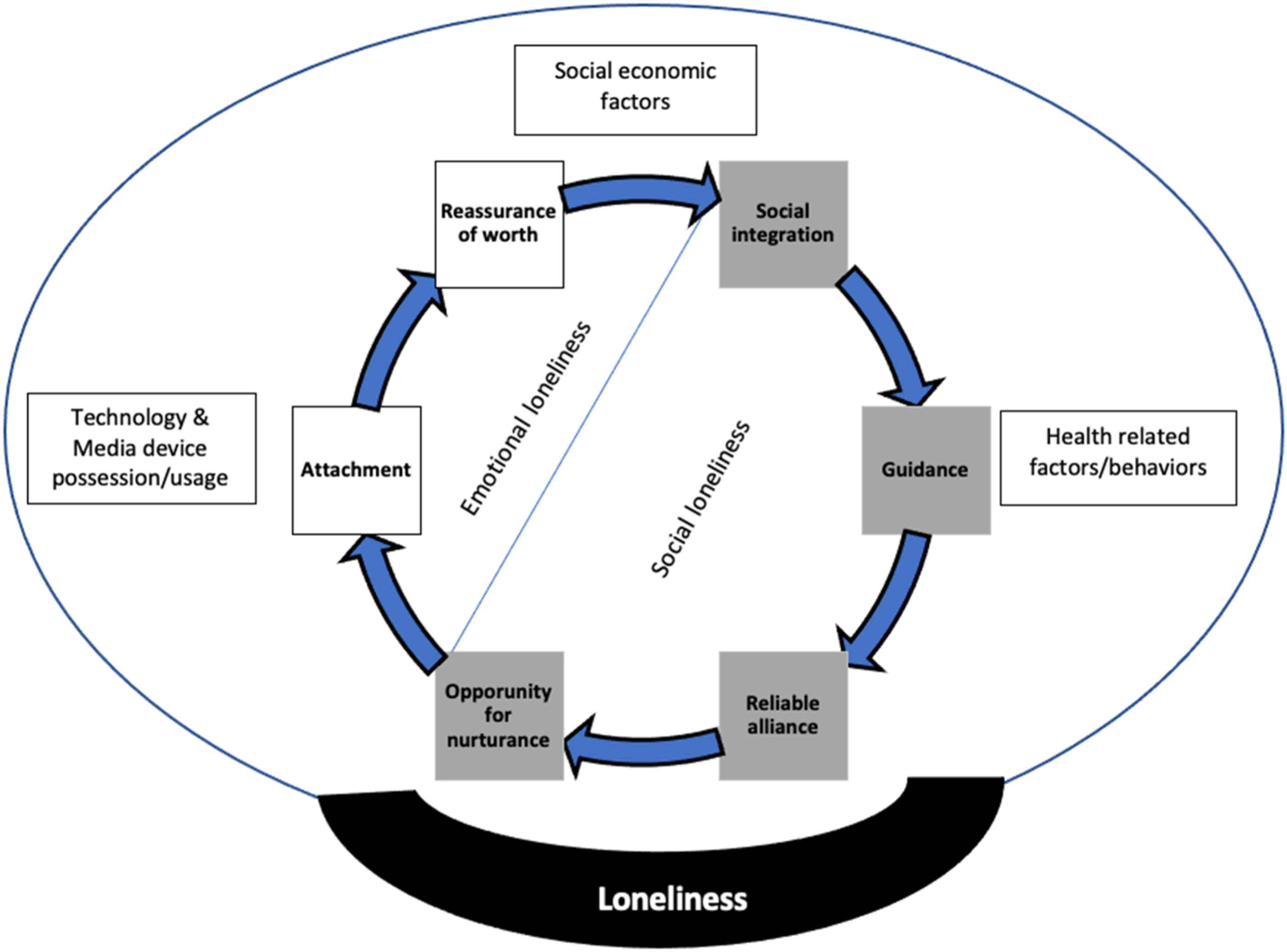
Social Integration
Findings from 14 studies were mapped to “social integration” and were reported as either social engagement, social participation, or social connection (Choi et al., 2021; Creecy et al., 1983; Hawkley & Kocherginsky, 2018; Ojagbemi & Gureje, 2019; Ojembe & Kalu, 2019; Olawa et al., 2021; Olawa & Idemudia, 2020; Roos et al., 2019; Salma & Salami, 2020). These studies highlighted how social loneliness is shaped by the level of involvement or engagement of BOAs in community activities, enabling individuals to build competencies, identity, and specific skills needed to thrive. This theme also elucidated the intensity of socialization and social connection that helped BOAs to feel less lonely. Factors supporting social integration found to reduce the experience of loneliness among BOAs vary, including participation in recreational religious activities and traditional events (Ojembe & Kalu, 2018; Olawa & Idemudia, 2020), face-to-face interaction, quality, and quantity of relationships (Ojembe & Kalu, 2019). Another factor shown to reduce loneliness among BOAs is the frequency with which they socialize and participate in family events, visit friends, attend religious services, and travel out of the country (Hawkley & Kocherginsky, 2018). Lastly, visiting children and other family members was also presented as one of the ways that BOAs engage in social integration, which reduces loneliness (Olawa & Idemudia, 2020). Attending traditional ceremonies predicted a lower risk of loneliness in women than in men (Olawa & Idemudia, 2020)
Having either a poor social network, lack of interpersonal interactions, being alone, limited social activities, or close contact were all found to contribute to loneliness among BOAs (Choi et al., 2021; Creecy et al., 1983; Ojembe & Kalu, 2018; Roos et al., 2019). In addition, BOAs who spent limited time working tend to experience loneliness more than those who worked longer (Creecy et al., 1983). Finally, different forms of exclusion, including ageism, racism, and sexism, also contributed to loneliness among BOAs in Canada (Salma & Salami, 2020).
Guidance
Findings from three studies were mapped to the social provision of guidance as described in Table 1 (Kwegyir Tsiboe, 2020; Roos et al., 2019; Yoo-Jeong et al., 2020). While Roos et al. (2019) reported that attending or performing socio-cultural rituals mitigates loneliness among South African older adults, Kwegyir Tsiboe (2020) reported that older adults residing in Emmena, an Ashanti region in Ghana, are vulnerable to making bad health choices, including poor eating habits and gambling because they are lonely and lack a support system that objectively helps them to endure and recover from their experience of loneliness. Among African American older adults, those experiencing HIV-related stigma are more likely to be lonely than those not experiencing HIV-related stigma (Yoo-Jeong et al., 2020).
Opportunity for Nurturance
Findings from five studies were mapped to Opportunity for Nurturance, and these concepts included the family (Hawkley & Kocherginsky, 2018; Olawa & Idemudia, 2020) and social support (Ebimgbo et al., 2021; Ojembe & Kalu, 2018); the number of children (Ebimgbo et al., 2021; Victor et al., 2021), and, living arrangements (Ebimgbo et al., 2021; Hawkley & Kocherginsky, 2018; Ojembe & Kalu, 2018). Family support (Hawkley & Kocherginsky, 2018; Olawa & Idemudia, 2020) (only in women), social support (Ebimgbo et al., 2021), reduced friendship strain (how often do you feel friends are demanding and critical of them—Hawkley and Kocherginsky (2018), and living with people (Ebimgbo et al., 2021), were associated with a lower risk of loneliness. A qualitative study reported that living alone and weak family ties were risk factors for loneliness among Nigerian older adults (Ojembe & Kalu, 2018). A mixed-method study on factors that affect loneliness among Nigerian older adults by Ebimgbo et al. (2021) reported conflicting findings. While their quantitative findings reported that having more children was associated with a reduced risk of loneliness, in the qualitative report, they included a quote by one participant stating that “the number of children is not necessary for keeping company with older adults” (Ebimgbo et al., 2021, p. 11). Likewise, two quantitative studies conducted in the US and the UK reported that living alone, the number of close relatives or friends (Hawkley & Kocherginsky, 2018), or the number of children (Victor et al., 2021) were not associated with loneliness.
Attachment
Findings from eleven studies comprising both qualitative and quantitative designs reported on concepts relating to the attachment dimension, highlighting the importance of having or being in relationships that provide a sense of safety, security, well-being, and enhance a sense of importance, thereby reducing loneliness among BOAs (Cacioppo et al., 2017; Ebimgbo et al., 2021; Hawkley & Kocherginsky, 2018; Kwegyir Tsiboe, 2020; Ojembe & Kalu, 2019; Olawa et al., 2021; Olawa & Idemudia, 2020; Phaswana-Mafuya & Peltzer, 2017; Roos et al., 2019; Victor et al., 2021). Among BOAs in Nigeria and South Africa, it was reported that more than half of the participants who were married were less lonely than those who were divorced, separated, or widowed (Ebimgbo et al., 2021; Phaswana-Mafuya & Peltzer, 2017). Similarly, Ojembe and Kalu (2018) reported that bereavement increased loneliness among older adults in the Southern part of Nigeria. Among older adults in the US, having a strained relationship or friendship contributes to loneliness among BOAs (Hawkley & Kocherginsky, 2018). It was also shown that BOAs who have weak ties with their family members are more likely to be lonely than those who share a strong family bond (Ojembe & Kalu, 2018). Furthermore, loss of significant relationships, engagement in a painful interaction with significant others, and involvement in a strained friendship increased loneliness among BOAs in both South Africa and the US (Hawkley & Kocherginsky, 2018; Roos et al., 2019). Among three studies that explored the influence of behavioral tendency on loneliness, self-centeredness (Cacioppo et al., 2017), Extraversion, and neuroticism (Olawa et al., 2021; Olawa & Idemudia, 2020) were also reported as predictors for loneliness among BOAs.
Reassurance of Worth
Finding from six studies were mapped to the reassurance of worth category, which shows how much BOAs feel a sense of community and reception of attention which counters feelings of unwantedness (Kwegyir Tsiboe, 2020; Ntozini & Abdullahi, 2021; Nzabona et al., 2016; Van Der Geest, 2004; Yoo-Jeong et al., 2020). Among BOAs in rural Ghana, a study reported that older adults still actively engaged with their communities are respected and provided companionship. However, the older adults who feel that their community members do not value their wisdom or seek their advice reported more experience of loneliness (Van Der Geest, 2004). Among older adults in South Africa, low self-acceptance, environmental mastery, and autonomy were some predictors of loneliness moderated by ethnic affiliation. Overall, having these skills improved their well-being and reduced their experience of loneliness (Ntozini & Abdullahi, 2021). Among subsets of vulnerable groups among BOAs in the US, findings show that older adults who are homeless and live in unstable housing conditions tend to have a higher experience of loneliness (Yoo-Jeong et al., 2020). Similarly, older adults in rural Emmena—Ghana, who felt more vulnerable due to their health and sexual orientation, reported more loneliness than their counterparts (Kwegyir Tsiboe, 2020).
Other Emerging Themes
Socio-Economic Factors
Eleven studies highlighted some socio-economic factors contributing to loneliness among BOAs. Quantitative studies from the US, Nigeria, and South Africa reported that BOAs with lower levels of education are more likely to be lonely than those who are well-educated (Choi et al., 2021; Creecy et al., 1983; Ebimgbo et al., 2021; Igbokwe et al., 2020; Phaswana-Mafuya & Peltzer, 2017). Among BOAs in the US, Africa, and the UK, both qualitative and quantitative studies reported that poor income (Choi et al., 2021; Ebimgbo et al., 2021; Nzabona et al., 2016; Victor et al., 2021), female gender (Olawa et al., 2021; Phaswana-Mafuya & Peltzer, 2017; Victor et al., 2021), increase in age (Hawkley & Kocherginsky, 2018; Phaswana-Mafuya & Peltzer, 2017; Victor et al., 2021), and residing in a rural area (Kwegyir Tsiboe, 2020; Ntozini & Abdullahi, 2021) were all risk factors for loneliness.
Technology & Media Device Possession/Usage
Two studies reported that BOAs who are lonely repeatedly watch television (Creecy et al., 1983; Ojembe & Kalu, 2019). Specifically, Ojembe and Kalu (2019) noted that technology helped older adults who were lonely to connect to the outside world. In addition, the lack of old-age friendly television and radio programs demotivated BOAs from watching television, and reduces loneliness among BOAs who dislike watching programs that elicit negative feelings (Ojembe & Kalu, 2019).
Health-Related Factors/Behavior
Fifteen articles reported several health-related factors and behaviors as risk factors for loneliness, including depression (Gonyea et al., 2018; Igbokwe et al., 2020; Ojagbemi & Gureje, 2019; Taylor et al., 2018; Taylor & Nguyen, 2020; Yoo-Jeong et al., 2020), poor cognitive function (Han et al., 2017; Phaswana-Mafuya & Peltzer, 2017), psychological distress (Taylor et al., 2018), stress (Gonyea et al., 2018), poor general health (Ebimgbo et al., 2021; Nzabona et al., 2016), functional status, and higher score in comorbidity burden (Yoo-Jeong et al., 2020). Van Der Geest (2004) described several living conditions, such as poor health, psycho-social, and financial living conditions, as factors influencing loneliness among BOAs.
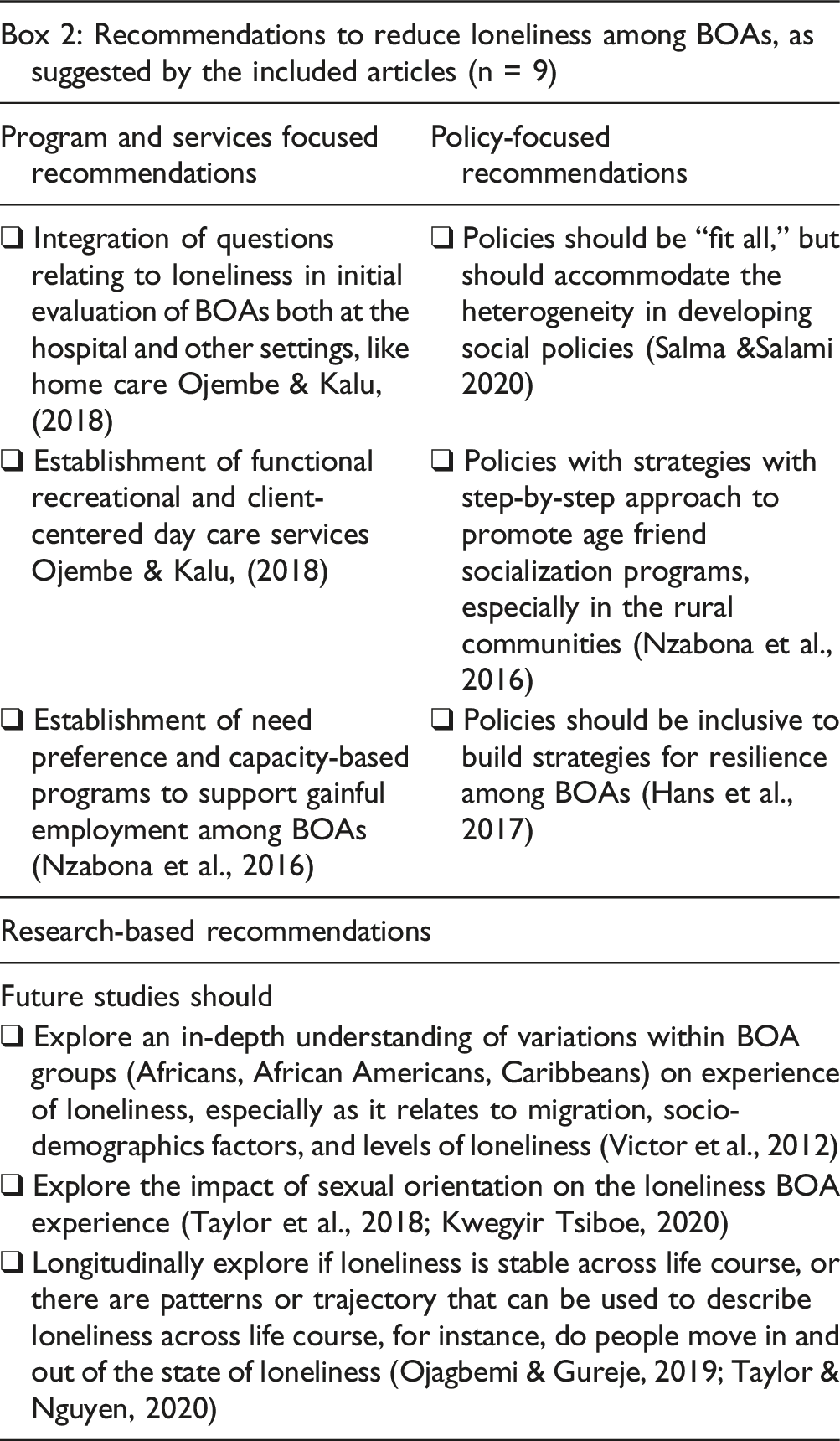
Recommendations
Discussion
Presumably, this is the first review that provides insights into the existing literature on loneliness among BOAs, mapping this evidence across Weiss' six social provisions, including social integration, guidance, reliable alliance, an opportunity for nurturance, attachment, and reassurance of worth. We found that the Social Provisions Framework provided a more effective method to capture and show the factors contributing to loneliness among BOAs. Given the lack of a clear definition of the six social provisions in the literature, we redefined all six categories to enable researchers interested in exploring the concepts of social and emotional loneliness to have a clear conceptual meaning of these terms (see Table 1). These definitions were adopted from Wiess' Loneliness conceptualization (Weiss, 1973). We found additional themes, such as socio-economic, technology-based, and health-related factors influencing loneliness among BOAs. We included only 27 articles (all peer-reviewed, as no gray literature was found) published in six countries, including Nigeria, Ghana, the USA, the UK, Canada, and Uganda, highlighting the limited number of articles in Black-dominated regions like Africa and the Caribbeans. No single article was mapped across all the six categories, highlighting the heterogeneousness of what factors contribute to loneliness among BOAs.
The literature synthesis showed some overlaps between the findings from studies included in this review but using the Social Provisions framework presented a straightforward method to organize and synthesize the results. All the categories in the framework were mainly represented in the literature, except the reliable alliance category. However, some categories were more defined than others in the articles (e.g., health-related factors, socio-economic factors, social integration, and attachment), showing what social provision might be more critical to BOAs (see Table 1). An explanation of why no article represented the reliable alliance social provision using the definition we provided (a supplementary relationship) could be explained by the fact that the Black culture values relationship with family and community members more than people outside these networks (Ebimgbo et al., 2021; Ojembe & Kalu, 2019; Olawa & Idemudia, 2020). This potentially highlights the critical role of the collectivist culture, which values more interaction with family members (Lykes & Kemmelmeier, 2014), since culture emerges in forming a society’s normative values and meaningful practices. Moreover, the absence of a reliable alliance in the literature might also reveal that no study included immigrant BOAs living alone while their families and children live in another country, since this was not reported by any of the studies. For example, when BOAs arrive as refugees in another country without their families, they may naturally seek opportunities to create networks with nonfamily members, such as religious leaders or attending healthcare workers. These individuals will serve as BOAs’ reliable assurance to mitigate experience of loneliness in their new country. Additionally, it is plausible that migration actively plays a role in shaping the experiences of loneliness (Victor et al., 2012).
Furthermore, the findings suggest that some social provisions seem more prominent in some geographical regions than others. For instance, the synthesis highlights that articles from countries in Africa and the US reported more on social integration than those conducted in the UK and Canada, reconfirming the importance of relationship cohesion with the social networks available and accessible to the individual (Hawkley & Kocherginsky, 2018). Similarly, attachment is considered another social provision significant to BOAs in all the countries represented, except Canada. This might be due to the gaps in the literature on loneliness among BOAs in Canada.
Although similar factors influence loneliness in men and women, Olawa and Idemudia (2020) found that attending traditional events or ceremonies increased loneliness among men but reduced women’s loneliness. This finding is surprising because, especially in the African culture where the study was conducted, men are the traditional leaders and are responsible for conducting traditional ceremonies, while women play a subordinate role (Fonjong, 2001). One plausible argument could be the type of traditional ceremony. Anecdotally, women attend traditional ceremonies more than men, for instance, traditional weddings and child dedications, while men attend and officiate in traditional events such as wrestling.
Lastly, our findings revealed the overlap between loneliness and socio-economic status. Specifically, this finding highlights how the disproportionate disadvantages that BOAs face across their life course and their unique aging experience is exacerbated by poor health, poor living conditions, financial constraints, and other social inequities influence loneliness.
Recommendations for Future Research
Given the findings from this review, we discuss the gaps in the literature relating to loneliness among BOAs. First, while there have been studies that explored the prevalence of loneliness in high-income countries, including the USA and UK, there are limited studies in middle and low-income countries, including Nigeria, Kenya, and Ghana. Therefore, it is challenging to understand whether the prevalence of loneliness among BOAs differs or is shaped by the region. As such, studies exploring the prevalence of loneliness among BOAs in middle and low-income countries are needed to compare guiding global policies targeting loneliness. Furthermore, since it was shown that the disproportionate and cumulative disadvantages faced by BOAs across their life course exacerbate their experience of loneliness and create a unique differential experience of aging, perhaps developing culturally specific interventions would be potential in understanding effective ways to address their complex life experiences. To achieve this, research, programs, and services should engage BOAs more in establishing effective strategies.
Theoretically, does understanding these social provisions (defined as what individual gains from their relationship with others) highlight the trajectorial experience of loneliness among BOAs? For instance, could one of the provisions be more critical than the other, and where should intervention be placed? Besides, most of these social provisions are amenable to targeted interventions; is it possible that intervening in one of the social provisions could influence or act on other provisions? Future studies should identify which social provisions (when targeted) could reduce loneliness, allowing clinicians to allocate resources. Another area of importance is co-developing a screening tool following the six provisions with the older adults, guiding clinicians to identify which social provisions, when targeted, are essential to reduce loneliness for BOAs, promoting a patient-centered approach to care.
Methodologically, qualitative studies are required to examine the role of geographical location (e.g., BOAs residing in high or middle and low-income countries) in explaining the experiences of loneliness among BOAs. Surprisingly, qualitative studies exploring the experiences of BOAs were lacking in North American countries (e.g., the USA and Canada) that have many blacks. Most studies in these regions lumped racial and ethnic groups together, undermining the examination of critical differences related to diversity that may present varied experiences related to loneliness. Exploring specific experiences of each ethnic group, especially in multicultural countries like the USA and Canada, would inform policies to effectively address the unmet needs of targeted groups. Although not explored deeply in this review, older Black women experience loneliness differently than men. Therefore, researchers should explicitly disaggregate data on loneliness among BOAs by gender to help inform gender-based policy and intervention. In addition, studies should explore longitudinally the role of immigration in shaping the specific experience of loneliness among BOAs, especially in countries with many immigrants from the black-dominated nations in Africa and Caribbeans. In addition, we found no article in the Caribbean, suggesting the need for relevant studies that will explore loneliness among BOAs living in the region. Regardless, studies that explore loneliness in Black-dominated nations like Nigeria and Ghana do exist. Therefore, future reviews should focus on conducting a qualitative meta-analysis of qualitative studies in this region to explore the experience of loneliness among BOAs. We believe the recommendations that we have suggested in this review will further inform policy and research that will generally promote the well-being of BOAs.
Limitations
While our review is the first to provide global evidence on loneliness among BOAs, there are some limitations. We ensured that all the eligible literature was included in the review. However, we could still have omitted some articles, especially from the African region, since some of the journals are not indexed in related databases (Hofman et al., 2009). Also, by limiting the inclusion to only articles that addressed subjective loneliness and were published in English, we may have excluded some relevant articles. Finally, the six Weiss provision is utilized in this review for a practical purpose, solely to facilitate classification and easy identification of factors influencing loneliness among BOAs, which might also benefit other ethnic groups of older adults. However, because of the ambiguity and possible overlap of the six of Weiss’s provisions, we may have mapped some articles in the wrong category. Therefore, readers should reflect on this when interpreting the review findings.
Conclusion
Contributory factors for loneliness among BOAs were mapped across five of the six social provisions (social integration, guidance, opportunity for nurturance attachment, reassurance of worth), excluding reliable alliance. Socio-economic, technology-based, and health-related factors were also key contributors to loneliness among BOAs. While all six provisions seem essential in shaping experience of loneliness among BOAs, future studies should identify which social provisions (when targeted) could reduce loneliness, allowing clinicians to allocate resources effectively and efficiently.
Supplemental Material
Supplemental Material - Understanding Social and Emotional Loneliness among Black Older Adults: A Scoping Review
Supplemental Material for Understanding Social and Emotional Loneliness among Black Older Adults: A Scoping Review by Blessing Ugochi Ojembe, Michael Ebe Kalu, Chigozie Donatus Ezulike, Anthony Obinna Iwuagwu, Prince Chiagozie Ekoh, Oluwagbemiga Oyinlola, Temitope Osifeso, John Osuolale Makanjuola, and Lydia Kapiriri in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Understanding Social and Emotional Loneliness among Black Older Adults: A Scoping Review
Supplemental Material for Understanding Social and Emotional Loneliness among Black Older Adults: A Scoping Review by Blessing Ugochi Ojembe, Michael Ebe Kalu, Chigozie Donatus Ezulike, Anthony Obinna Iwuagwu, Prince Chiagozie Ekoh, Oluwagbemiga Oyinlola, Temitope Osifeso, John Osuolale Makanjuola, and Lydia Kapiriri in Journal of Applied Gerontology
Footnotes
Acknowledgments
We want to thank the Emerging Research and Professionals in Aging—African Network (ERPAAN) for their support and for allowing us to involve some of their members in this research. We also want to appreciate Dr Meridith Griffin, Dr Ann Fudge Schormans and the three anonymous reviewers for their constructive feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
Research Ethics
There is no HIPPA identifier associated with this research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.