
Abstract
COVID-19 era lockdown measures resulted in many workers performing their employment tasks remotely. While identifying individual-level predictors of COVID-19 era remote work, scholarship has neglected heterogeneity based on contextual characteristics. Using the first COVID-19 module (2020) of the Survey of Health, Ageing and Retirement in Europe (N = 8,121) and multinomial logistic regression analyses, this study examined how country-level digitalization, stringency of government COVID-19 containment measures, and COVID-19 era excess mortality moderated how individual-level age, health, education, and income affected working partly or fully remotely among older Europeans (50-89 years) continuing to work through the pandemic. The central findings are that higher societal digitalization reduced the positive association between education and fully remote work, and greater country-level excess mortality accentuated how more education and poorer health increased the probability of fully remote work. These findings are interpreted through the fundamental cause theory of health and the health belief model. They further lead to recommendations that during future epidemics, policies and programs should address the remote working capabilities of older persons with fewer years of education, with fewer skills with modern digital technologies, and in worse health, especially within nations that are less digitally developed and harder hit by the epidemic in question.
Introduction
The COVID-19 pandemic is a global medical crisis announced by the World Health Organization (WHO) in January 2020 as a Public Health Emergency of International Concern (Metelmann and Busemann 2020). In consonance with WHO recommendations, many national governments instituted extensive lockdown measures (Dubey and Tripathi 2020) that restricted those employed within occupations not deemed essential (essential occupations include those within healthcare and pharmacies, law enforcement, and food purveyance) from working from their usual locations (Russo et al. 2021).
The consequent remote work arrangements helped contain COVID-19 (Russo et al. 2021). Moreover, they affected well-being, positively for some and negatively for others (Dubey and Tripathi 2020). Additionally, they had profound economic consequences, including sizeable increases in unemployment within occupations with limited potential for remote work (Béland, Brodeur, and Wright 2020). Many employers thus sought means for employees to work remotely, including through advanced information and communications technologies (ICTs) (Dubey and Tripathi 2020).
Pre-pandemic times included increasing potentiality for and utilization of remote work, based substantially on technological developments (Lund, Manyika, and Ramaswamy 2012). Since the 1990s, employers have increasingly provided remote work options, partly to profit from the work of mothers requiring more flexible employment (Lund et al. 2012). Within the European Union (EU), 17 percent of workers were engaging in remote work in 2015 (Nakrošienė, Bučiūnienė, and Goštautaitė 2019).
During the pandemic, negotiations between employers and employees concerning remote work arrangements figured prominently (Davies 2021; Fana et al. 2020). The International Labor Organization (ILO 2020a) emphasized the importance of effective dialogues between employers and employees for finding means, including constructive remote work arrangements, of keeping the workforce safe, healthy, and productive.
Therefore, both individual- and contextual-level factors influenced pandemic-era remote work. While scholarship has identified predictors at both levels of analysis, research has inadequately addressed heterogeneity in how personal characteristics predicted working remotely based on contextual factors, a gap which this study helps fill. This heterogeneity is an interplay of structure and agency since individual motivations and capacities to work from home are embedded within broader contexts whose circumstances and policies affect demand for and encouragement of remote work. Knowledge of these patterns is imperative since remote work was among the most salient features of responses to the COVID-19 pandemic, with substantial effects upon economies and population health. This knowledge will further help prepare responses to future large-scale epidemics; development of national policies should consider that diverse residents are differentially affected by epidemics and their policy responses. Additionally, research in this vein will reveal individual- and country-level characteristics that facilitate working from home, regardless of specific motivations.
This study examines such cross-level moderation specifically among Europeans between 50 and 89 years of age who continued working through the pandemic. This is motivated by population aging throughout industrialized nations (Cooke 2006). Furthermore, older adults are more vulnerable to the health consequences of COVID-19 infection, substantially due to their higher probabilities of having underlying health conditions, causing greater COVID-19-related anxiety (Wolf et al. 2020). Moreover, older persons are more likely employed within occupations less amenable to work-from-home arrangements and may therefore have been more likely to experience pandemic-era unemployment (Li and Mutchler 2020; Monahan et al. 2020).
Study Overview
This study asks, among older Europeans who continued to work during the pandemic, how did country-level digitization, stringency of government restrictions, and health impacts of COVID-19 moderate the relationships of individual-level education and household income (measures of socioeconomic status [SES]), age, and general health with pandemic-era remote work? Accordingly, this study assesses how individual-level desires and choices to work remotely are embedded within and influenced by larger societal structures.
This study’s nominal dependent variable includes work from one’s usual place, working partly from home, and working completely from home. The central findings are that increasing societal digitalization reduces the importance of education for fully remote work, and that increasing country-level COVID-19 health impacts raise the importance of both education and worse health for working fully remotely.
What follows is a framework that discusses individual- and contextual-level predictors of pandemic-era remote work. The latter discussion elaborates on the concept of societal digitalization. This is followed by discussion of this study’s two orienting theoretical frameworks: fundamental cause theory of health and the health belief model. Informed by these theories, what follows is explanation of why we might expect cross-level interactions between country- and individual-level variables in likelihood of pandemic-era remote work, thus interplays between structure and agency, and associated hypotheses.
Previous Research, Conceptual, and Theoretical Framework
This framework centrally addresses how during this medical crisis, various aspects of SES (education, income, and occupation) permit older workers to protect themselves by working remotely, while more advanced age and worse health suggest greater need for remote work. This framework further synthesizes these two paths of inquiry through emphasizing that those at greatest risk of serious morbidity or mortality from COVID-19 infection have the greatest need for remote work possibilities. The latter is thus protective against the former.
Similarly, this study emphasizes that while country-level COVID-19 health impacts and stringency of containment measures affect need for remote work, societal digitalization affects its feasibility. The fact that numerous nations have invested in technological development policies and programs to contain the damage of the pandemic suggests that the most heavily affected nations are in greatest need of remote work potentialities (Organisation for Economic Co-operation and Development 2020). These structural characteristics condition employers’ and employees’ desires and choices concerning remote work.
Individual-level Predictors of COVID-19-era Remote Work
Studies have revealed that COVID-19-era remote work is affected by individual-level socioeconomic indicators, including education, occupations, and types of work. In the Canadian context, Guillermo Gallacher and Iqbal Hossain (2020: S50) showed that poorer workers, male workers, workers without a college degree, private sector workers, single workers, small firm workers, seasonal or contractual workers, part-time workers, younger workers, and non-immigrant workers tend to be employed in jobs for which remote work is less possible.
Jonathan I. Dingel and Brent Neiman (2020) found that typical characteristics of jobs not performable from home include their incumbents rarely reading and sending emails, daily outdoor activity, large amounts of time spent walking or running, regular wearing of gear for safety or protection, high extents of physical activity, manipulation of objects, machines, and vehicles, regular direct interactions with the public, and the maintenance and inspection of materials, tools, and structures. A study of Canadians with disabilities or chronic health conditions revealed that rates of working at least partly remotely were highest among those in white-collar jobs, such as in management and administration, finance and business, the sciences and arts, law, and government (Maroto, Pettinicchio, and Lukk 2021). Conversely, those in health care, services, sales, manufacturing, the skilled trades, and transport showed lower rates of remote work (Maroto et al. 2021). Accordingly, working remotely shows gradients based on SES and on-the-job use of digital technologies.
Furthermore, studies have shown individual-level age and health to predict pandemic-era remote work, since they affect risk of serious health complications and mortality concomitant to COVID-19 infection (Landau et al. 2021; Wolf et al. 2020). Accordingly, having an underlying respiratory condition predicted working remotely (Camacho-Rivera, Islam, and Vidot 2020). More generally, underlying chronic health conditions increased COVID-19-protective behaviors (Camacho-Rivera et al. 2020). As such, those of higher age or in worse health might have more desire to work remotely. However, lower SES might constrain their ability to do so.
Contextual-level Predictors of COVID-19-era Remote Work
Scholarship has further revealed contextual predictors of pandemic-era remote work. Higher-SES areas show higher pandemic-era propensities for remote work, and social distancing more generally (Kavanagh, Goel, and Venkataramani 2021). This is largely because higher-paying work is more easily performed from home (Dingel and Neiman 2020), substantially because of involvement of advanced computer technologies (Sostero et al. 2020). In fact, employers view remote work as associated with fewer productivity declines within sectors marked by higher incomes and extents of education (Bartik et al. 2020). Accordingly, American states with higher proportions of workers employed in professional and managerial occupations, and other sectors focused on information, knowledge, and modern technologies, have more prevalent pandemic-era work-from-home arrangements (Brynjolfsson et al. 2020). As such, general SES and digitalization within a geographical location are structural characteristics facilitating workers’ pandemic-era choices to work remotely.
Societal digitalization is thus one of the key structural characteristics this study examines. It is operationalized through the European Commission’s Digital Economy and Society Index (DESI) (see EU 2021). This index depicts European nations’ differing “digital performance” through the degree to which the government, the economy, and social life integrate digital technologies, and the extent of the workforce’s advanced computer skills. It further incorporates quality of internet connections and the extent to which households regularly use digital and internet technologies (including computers, smart phones, and other ICTs) in their everyday lives, including frequent online events, activities, and market transactions (EU 2021). During nations’ earlier phases of digitalization, economic sectors closely linked with ICTs undergo transformations (Bánhidi, Dobos, and Nemeslaki 2020). Throughout subsequent phases, digitalization spreads to and transforms many additional economic sectors, including “media industries such as music, television and films; retail businesses such as books, newspapers, apparel and electronics; and services such as travel, banking or insurance” (Bánhidi et al. 2020:42–43). During the COVID-19 pandemic, this spread might expand the range of workers with the option of working remotely.
Moreover, contexts facing greater pandemic-era health burdens show increased remote work arrangements (Brynjolfsson et al. 2020), and social distancing practices more generally (Kavanagh et al. 2021). Relatedly, American states with higher rates of COVID-19 infection show higher prevalences of remote work (Brynjolfsson et al. 2020). A further study concurred that remote work increased most in nations more heavily impacted by COVID-19 and in which teleworking arrangements were effectively structured and developed prior to the pandemic (ILO 2020b).
Accordingly, we know much about individual- and contextual-level factors that influence remote work during the pandemic. However, less is known about how contextual-level factors condition these individual-level predictors of pandemic-era remote work. The present study addresses this gap in our knowledge.
Theoretical Perspectives
Two theoretical perspectives, fundamental cause theory of health and the health belief model, shed light on how contextual characteristics might moderate the impact of individual-level factors upon pandemic-era remote work.
Fundamental cause theory of health (FCT)
FCT suggests that through historical time, the positive relationship between SES (including education and income) and health remains operative even as the mediating mechanisms change (Link and Phelan 1995; Phelan, Link, and Tehranifar 2010). This is because SES “embodies an array of resources, such as money, knowledge, prestige, power, and beneficial social connections that protect health no matter what mechanisms are relevant at any given time” (Phelan et al. 2010: S28). In fact, higher SES positively influences ability to exercise social distancing through the pandemic (Ravenelle, Kowalski, and Janko 2021). During the pandemic, remote work feasibility increased in importance as a mechanism tying SES, including education and income, to health (Table 3 shows a significant negative relationship between self having tested positive for COVID-19 and working completely remotely).
Notably, mediating mechanisms between SES and health also vary across geographical locations (see Dummer 2008). Plausibly, in more digitalized nations, advanced digital technologies (especially ICTs) have spread among a greater range of workplaces and workers. Accordingly, during the COVID-19 era, remote work capability as a mechanism tying SES with health is possibly stronger within less digitally developed nations. As such, FCT suggests studying SES at the individual level, digitalization at the contextual level, and their cross-level interactions, the latter suggesting the embeddedness of individual-level choices within structural contexts.
Health belief model (HBM)
The HBM proposes that health decisions are affected by (1) perceptions of the probability that one becomes ill and the likely physical and social consequences of illness, (2) perceptions of the efficacy of a health-related behavior for reducing or avoiding these risks, and (3) calculations of the barriers and costs associated with a health decision or behavior (Abraham and Sheeran 2015; Becker et al. 1977). Within the context of the pandemic, this theory thus integrates within one framework perceptions of the need to work remotely (first two tenets) and the feasibility of doing so (third tenet). While the former is affected by country-level COVID-19 health impacts, the latter is influenced by country-level digitalization.
The HBM further emphasizes external cues to health behaviors (Abraham and Sheeran 2015; Becker et al. 1977), which in the COVID-19 era include government policies and recommendations for social distancing and work-from-home arrangements. Stringency of government COVID-19 containment policies might create structural circumstances that broadly increase work-from-home arrangements, reducing the importance of workers’ unique characteristics (including SES, age, and health), and the beliefs and preferences of employers and employees. This further highlights how personal calculations and preferences (individual agency) are embedded within and conditioned by social structures. Accordingly, the HBM suggests studying the stringency of governments’ pandemic responses, beyond country-level COVID-19 health impacts and digitalization.
This study further considers how country-level COVID-19 health impacts affect remote work after the stringency of governments’ containment policies is controlled. This net effect of country-level COVID-19 health impacts is likely linked with employers’ and employees’ subjective appraisals that influence health beliefs, and thus work-from-home arrangements.
The HBM’s emphases on perceived risks and vulnerabilities, linked with country-level COVID-19 health impacts and individual-level age and health, and perceived costs and barriers, associated with societal digitalization, stringency of governments’ pandemic responses, and individual-level SES (see FCT above), affecting health behaviors suggest studying these variables and their cross-level interactions.
Plausible Cross-level Interactions and Associated Hypotheses
While scholarship has investigated individual- and contextual-level predictors of COVID-19-era remote work, examination of interactions between these two levels of analysis is lacking. Plausibly, within nations of greater digitalization, wider spans of jobs will integrate advanced technologies, reducing the importance of personal SES (including education and income) for remote work potentiality. Accordingly, I expect that among older Europeans working continuously through the pandemic, the positive associations of education and income with remote work are reduced by societal digitalization (hypothesis 1.1). This concords with the above discussion of FCT suggesting that remote work capability as a mechanism between SES and health is likely stronger within less digitally developed nations. Furthermore, greater societal digitalization might increase the likelihood that those of more advanced age and/or in worse health, and thus in greater danger of COVID-19, are able to negotiate work-from-home arrangements. As such, I expect that among older Europeans working continuously through the pandemic, the positive associations of more advanced age and worse health with remote work are increased by societal digitalization (hypothesis 1.2). This concords with the HBM’s tenets that health decisions are affected by perceptions of risk (accentuated among older respondents and those in worse health) and by calculations of barriers and costs (remote work is hampered within less digitally developed contexts) (Abraham and Sheeran 2015; Becker et al. 1977). Digitalization is thus a structural characteristic that might moderate how individual-level choices to work remotely, based on SES, age, and health, are realized.
Plausibly, more stringent government protective measures generally applied throughout a population reduce differences in work-from-home arrangements based on workers’ unique characteristics. This leads me to expect that among older Europeans working continuously through the pandemic, the positive associations of education and income (hypothesis 2.1), and more advanced age and worse health (hypothesis 2.2), with remote work are reduced by more stringent government containment measures. This corresponds with the HBM’s tenets of the importance of external cues and the perceived costs and barriers of health behaviors. Stringency of governments’ protective measures is thus a structural characteristic that might reduce the importance of individual-level wants and choices.
However, after accounting for the stringency of governments’ containment measures, in contexts of greater COVID-19 health impacts, those with more education and higher incomes might be further motivated (the HBM’s emphasis on perceptions of risks) and better positioned (the HBM’s emphasis on calculated barriers and costs) to protect themselves through complying with work-from-home recommendations. Accordingly, I expect that among older Europeans working continuously through the pandemic, the positive associations of education and income with remote work are increased by greater contextual COVID-19 health impacts (hypothesis 3.1). Moreover, greater country-level COVID-19 health impacts, net of the stringency of governments’ protective measures, might increase the likelihood that a worker of more advanced age and/or in worse health will request for and be granted the option of remote work (the HBM’s emphasis on perceptions of the likely physical and social consequences of illness, at both the individual and contextual levels). As such, I expect that among older Europeans working continuously through the pandemic, the positive associations of more advanced age and worse health with remote work are increased by greater contextual COVID-19 health impacts (hypothesis 3.2). Individual-level choices might thus be conditioned by the structural characteristic of country-level COVID-19 health impact.
Method
Dataset and Sample
This study’s analyses were primarily based on the Survey of Health, Ageing and Retirement in Europe’s (SHARE) first COVID-19 module. The constituent interviews across 27 nations of Europe and Israel took place between June and August 2020 (see Börsch-Supan 2022g), thus at the height of the COVID-19 crisis and lockdowns. The SHARE focuses on the health, labor, economic circumstances, and social connectedness of community-dwelling Europeans of at least 50 years of age. Waves took place generally biennially since 2004 and consistently included refreshment samples. While the first wave (2004) involved 11 European countries, through time the sample came to include 27 European nations and Israel. The first COVID-19 module was effective for this study since it includes respondents’ life and employment circumstances through the pandemic’s earlier phases. Axel Börsch-Supan et al. (2013) provide additional details concerning the SHARE.
This study’s sample were at least 50 years of age during the first COVID-19 module and were employed when the pandemic began (those not then employed were excluded). While the main analyses study only respondents who kept working through the pandemic, supplementary analyses in the appendix consider predictors of not working while keeping one’s job (i.e., being furloughed) and having lost one’s job through the pandemic (see Supplementary Appendix Table A2). Furthermore, respondents of at least 90 years of age were excluded because workers of this age are outliers with highly unique characteristics. After further exclusion of those missing data within the dependent variable (see below), the analytical sample included 8,121 respondents. Notably, the results based on age were specific to advancing years in later life, rather than the entire adult life course.
Due to non-available country-level data on the DESI (see below), Israel and Switzerland were the only countries excluded. This study’s countries included Austria, Belgium, Bulgaria, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Italy, Latvia, Lithuania, Luxembourg, Malta, The Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, and Sweden. The following countries held especially high proportions of this study’s respondents: Belgium (7.02 percent), Denmark (7.57 percent), Estonia (14.68 percent), Germany (7.04 percent), and Poland (8.29 percent). Denmark and Estonia included substantially higher proportions of this study’s respondents than of those of the entire first COVID-19 module (Israel and Switzerland excluded: Denmark: 3.79 percent; Estonia: 8.68 percent). This is because higher proportions of these countries’ original respondents were employed immediately before and kept working through the pandemic. These sampling imbalances are likely not substantial enough to affect the overall findings.
Because they were not assessed within the SHARE’s first COVID-19 module, some required variables (discussed below) were obtained from the sixth (2015), seventh (2017), and eighth (2019–2020) waves (see Börsch-Supan 2022d, 2022e, 2022f), and the easySHARE dataset (see Börsch-Supan and Gruber 2022). The latter is a simplified generated dataset that amalgamates an important set of variables from all respondents and waves within a single file (see Gruber, Hunkler, and Stuck 2014). Exceptionally, for occupations and industries of employment, some values were obtained from earlier than wave six, including back to wave two (2006) for some respondents (see Börsch-Supan 2022a, 2022b, 2022c). This is because values of these two variables were recorded in each wave only if they differed from those of the previous wave.
Variables
Dependent variable
This study’s outcome was a nominal variable based on employment circumstances during the first COVID-19 module: worked at the usual workplace, worked at home and the usual workplace, and worked only at home. For conceptual (work conditions most like earlier circumstances) and cell size reasons, “worked at the usual workplace” (63.82 percent of the analytical sample) was the reference category (ref.).
Independent variables
Respondents’ ages during the first COVID-19 module spanned from 50 to 89 years. To produce more substantial relative-risk ratios (RRRs), they were divided by 10.
Respondents’ self-perceived health was obtained from answers to the first COVID-19 module’s question, “Before the outbreak of Corona, would you say your health was excellent, very good, good, fair, or poor?” When missing, this variable was obtained from wave eight (if available and not missing), based on the same set of possible answers to the question, “Would you say your health is . . .” Because only 1.69 percent of the sample reported “poor” health, answers were dichotomized as (1) good/very good/ excellent (ref.), and (2) poor/fair.
Respondents’ education, household incomes, and occupations were measures of SES. The former was operationalized through years of education, obtained from wave eight. When missing, this time-constant variable was obtained from the easySHARE (if available and not missing). Because further years of education held little relevance for even higher extents of SES, years of education were top-coded at “20.”
Household incomes were obtained from answers to the first COVID-19 module’s question, “How much was the overall monthly income, after taxes and contributions, that your entire household had in a typical month before Corona broke out?” When missing, household incomes from wave eight (and then wave seven if still missing) served as replacements (if available and not missing), obtained from answers to the question, “How much was the overall income, after taxes and contributions, that your entire household had in an average month in [the previous year]?” Amounts were in Euros. Household incomes were then translated into 20 quantiles, computed separately within each nation, to assuage concerns with national differences in purchasing power parities and distributions of household incomes. Furthermore, computing 20 quantiles of household income permitted this variable to be studied as continuous.
Occupations were based on the International Standard Classification of Occupations (ILO 2022), composed of managers; professionals (ref.); technicians and associate professionals; clerical support workers; services and sales workers; skilled agricultural, forestry and fishery workers; craft and related trades workers; plant and machine operators and assemblers; elementary occupations; and armed forces occupations. This variable was obtained from wave eight (for some respondents, values extended back to wave two, see above), within which respondents stated either their current occupation or that of their last job, if not currently employed.
The first country-level independent variable was societal digitalization, operationalized through the Digital Economy and Society Index (DESI) (based on the year 2020), obtained from the European Commission (2021). This index spanning from 0 to 100 is a weighted combination of the extent to which a European nation has:
Connectivity: effective internet connectivity (weighted 25 percent)
Human capital: based on internet and broader advanced computer skills (weighted 25 percent)
Use of internet services: regular internet usage, including online activities and economic transactions (weighted 15 percent)
Integration of digital technology: extent and effectiveness of business digitalization and e-commerce (weighted 20 percent)
Digital public services: extent and effectiveness of government services and operations digitalization (weighted 15 percent)
These five weights were standards pre-chosen by the European Commission (2021). This index spanned from 36.43 (Bulgaria) to 72.30 (Finland). Because of non-availability of DESI scores, this study excluded respondents from Israel and Switzerland.
The second country-level independent variable was the stringency index developed by Our World in Data (2021). This index spanning from 0 to 100 displays for each individual day how strictly each country’s policies restrained human social and economic activities to contain the virus. Nine metrics are amalgamated: “school closures; workplace closures; cancellation of public events; restrictions on public gatherings; closures of public transport; stay-at-home requirements; public information campaigns; restrictions on internal movements; and international travel controls” (Our World in Data 2021). For each country here studied, stringency index scores were averaged across all days from January 21, 2020 (the first day of stringency index data) and July 16, 2021 (the midpoint in time of the SHARE’s first COVID-19 module’s interviews).
The third country-level independent variable was excess mortality (EM) p-scores (an operationalization of COVID-19 health impact), a measure of relative increase in mortality through the COVID-19 pandemic, based on comparisons of actual death rates with the death rates that would be expected had the pandemic never occurred (see Aron and Muellbauer 2020). The specific percentages here utilized were obtained from Ariel Karlinsky and Dmitry Kobak (2021a), computed through data within the World Mortality Dataset (Karlinsky and Kobak 2021b), which they maintain. Table 1 within Karlinsky and Kobak (2021a) further displays for each country the date up until the excess mortality data were obtained, the most recent being May 30, 2021 (Croatia and Hungary) among the countries here studied.
Descriptive Statistics (N = 8,121).
Note. GDP = gross domestic product.
Tim Vlandas (2020) explained the following advantages for research of excess mortality rates instead of direct assessments of COVID-19-specific mortality:
They do not vary according to geographical differences in definitions of COVID-19-specific death.
They are not affected by national differences in medical capacity for COVID-19 testing.
They more effectively assess the total health consequences of the pandemic, including excess deaths caused directly by COVID-19 infections and those whose sources are policy responses to COVID-19.
Control variables
Some demographic characteristics that might influence motivation and feasibility to work remotely, thus potentially confounding the central relationships here studied, were controlled. One control variable was gender (ref.=men). A second was marital/relationship circumstances, categorized as married/partnered-spouse/partner not working (ref.), married/partnered–spouse/partner working, and not married/partnered. This variable was obtained from the SHARE’s wave eight. When missing, it was obtained from the easySHARE’s wave eight (and then its wave seven if still missing) (if available and not missing). Parental status from the SHARE’s wave eight was additionally controlled, based on number of living children: no children, one or two children, and three or more children (ref.). When missing, this relatively time-constant variable was obtained from the easySHARE’s wave eight (and then its wave seven, and then its wave six, if still missing) (if available and not missing).
The second set of individual-level control variables were based on past COVID-19 infections, both (1) within the respondents themselves, and (2) among their close contacts (for both, ref.=absence of past infection).
While years of education and occupations were independent variables because they are more directly tied with SES and types of work tasks, every industry of employment includes many different extents of education and occupations, the activities of which differ. Accordingly, industry of employment was a control variable. This nominal variable includes agriculture, hunting, forestry, fishing; mining and quarrying; manufacturing; electricity, gas and water supply; construction; wholesale and retail trade, repair of motor vehicles, motorcycles and personal and household goods; hotels and restaurants; transport, storage and communication; financial intermediation; real estate, renting and business activities; public administration and defense, compulsory social security; education; health and social work; other community, social and personal service activities (ref.). This variable was acquired from wave eight (for some respondents, values extended back to wave two, see above), within which respondents declared either their current industry of employment or that of their most recent job, if not currently employed.
Some country-level variables were controlled because they likely affect work-from-home patterns and are thus potential confounders. One was median age of the population in 2020, obtained from Eurostat (2021) (divided by 10 to develop more substantial RRRs). Since older persons and those with health problems are more vulnerable to serious morbidity and mortality consequent to COVID-19 infection (Wolf et al. 2020), this variable might affect remote work patterns.
The country-level independent variables are substantially correlated with overall resources (see Supplementary Appendix Table A1). To avoid confounding based on national wealth, gross domestic product (GDP) per capita (current US$) in 2020 (obtained from the World Bank Group [2022a]) was controlled (divided by 10,000 to develop more substantial RRRs).
Analysis
This study’s focus is four sets of multinomial logistic regressions. The first set comprised one regression including both years of education and occupations, all other variables, and no interaction terms. This was the main analyses’ sole regression that included occupations, thus revealing how education and occupations uniquely affect remote work. In the remaining main analyses, which assessed interactions between individual- and country-level variables, occupations were not included, since there is substantial overlap between education and occupations in types of work tasks.
The remaining sets of multinomial logistic regressions studied the individual-level independent variables (including education while not including occupations) in interaction with country-level DESI (second), stringency of government COVID-19 response (third), and EM p-scores (fourth). The four models within each set sequentially and individually further included interaction terms between the respective country-level interactant and age/10, self-perceived health, years of education, and quantiles of household income. Within each regression, the remaining individual- and country-level variables were included as non-interactants.
All the continuous interactants were mean centered for the interpretability of their main effects. Through mean centering, the main effect of each interactant is interpreted as the RRR pertaining to when the other interactant is at its mean, rather than at zero (see Jaccard, Wan, and Turrisi 1990), which is not a logical value for this study’s continuous interactants.
Furthermore, two figures graphically display the significant interactions between years of education and (1) the DESI (Figure 1), and (2) the EM p-scores (Figure 2) in their prediction of working completely from home. A third figure graphically depicts the significant interaction between self-perceived health and the EM p-scores in their prediction of working completely remotely. These three figures displaying this study’s central findings were developed through predictive margins, realized through Stata’s “margins” command.
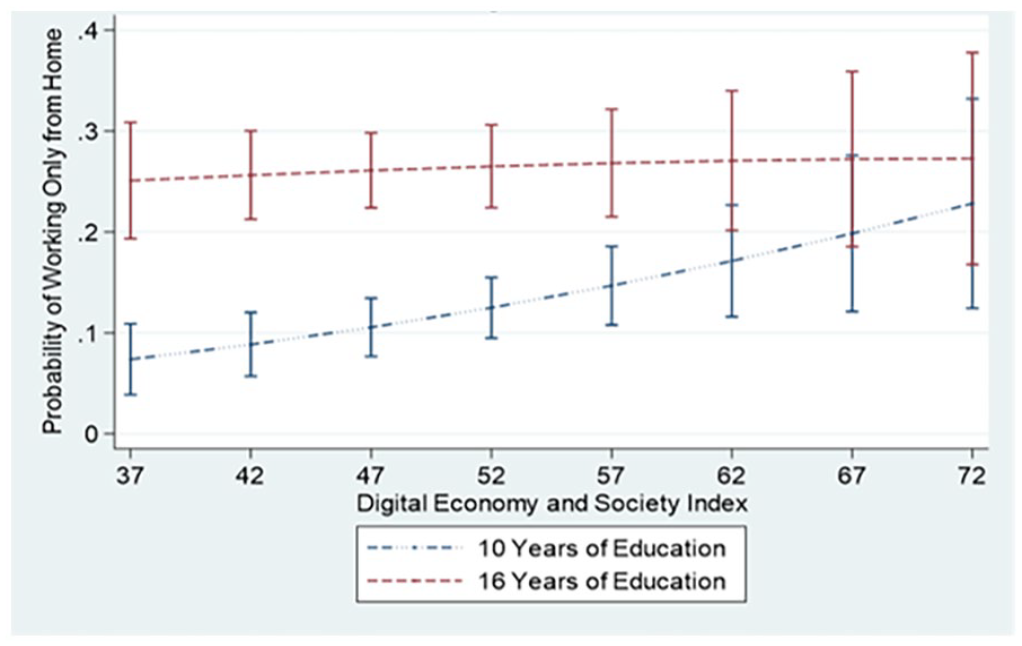
Predicted probabilities of working only from home, Digital Economy and Society Index in interaction with years of education, 95 percent confidence intervals included.
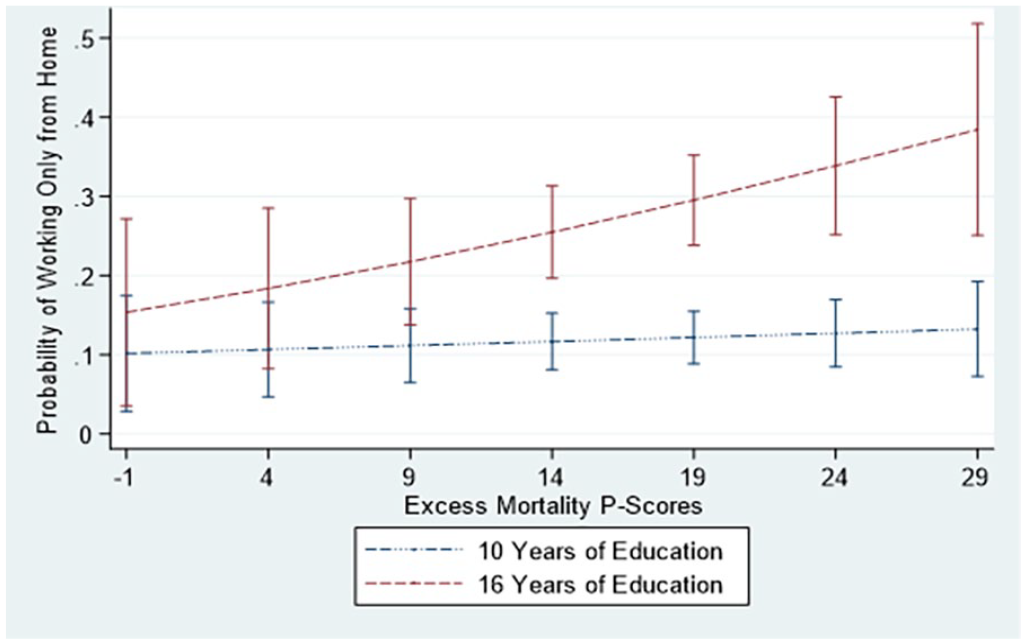
Predicted probabilities of working only from home, excess mortality p-scores in interaction with years of education, 95 percent confidence intervals included.
Multiple imputation using chained equations was used to address missing data; 10 imputed datasets were created. Industry of employment had 14.48 percent missing data and occupations had 18.67 percent missing data. Because these variables were based on many nominal categories, whether a multiple imputation procedure will effectively categorize the imputed missing data can be doubted. Accordingly, each of these two variables’ missing data were instead dealt with through placement within a missing-indicator category. Further variables with 10 percent or more missing data were quantiles of household income (10.39 percent) and parental status (16.45 percent). While there were no missing data for respondents’ ages, missing data were 0.01 percent for self-perceived health, and 5.68 percent for years of education. Since this study’s analytical sample was based solely on countries with data for the country-level independent variables, none of these variables had missing data. While the outcome variable, respondents’ work circumstances, was included in the multiple imputation process, all respondents originally missing data within this variable (0.10 percent) were excluded from the final analyses. This study’s analytical sample was thus 8,121 respondents.
To account for unequal sample selection probabilities, all models included weighting through the SHARE’s first COVID-19 module’s design weight. Standard errors were adapted for clustering according to country of residence during the first COVID-19 module. All analyses employed the Stata 17 statistical software package.
Supplementary Analysis
Table A2 in the Supplementary Appendix depicts a multinomial logistic regression (N = 10,814) based on having worked through the pandemic (ref.: 75.10 percent) versus having been furloughed (6.62 percent) and having lost one’s work (18.28 percent). Thus revealed are variables predicting selection into the main analyses’ sample of continuing workers. This table includes all variables, including education and occupations, with no interaction terms.
Robustness Checks
Further analyses additionally controlled for each nation’s percentage of total employment based in essential occupations because of its effects upon remote work arrangements. This 2018-based variable was obtained from Daniel Garrote Sanchez et al. (2020), who tabulated for each country the percentage of non-essential jobs (then subtracted from 100). Because data were unavailable for Malta, this variable was controlled only within robustness checks.
Table A3 in the Supplementary Appendix depicts whether the three main interactive findings (years of education * DESI, health * EM p-scores, years of education * EM p-scores, all in the prediction of working completely remotely, see below) are reproduced when studied through multilevel models that include random intercepts for each country. These models thus address the nested structure of the data and country-level unobserved heterogeneity. Since a multilevel command is lacking for multinomial logistic regressions, these robustness checks are multilevel mixed-effects logistic regressions with dependent variables denoting having worked only from one’s usual place (ref.) versus having worked completely remotely (mirroring the main analyses’ three significant interactive findings here emphasized).
It was important that this study employ multinomial logistic regressions assessing both partial and fully remote work since these two work arrangements involve different extents of risk of COVID-19 infection and adjustment of work routines. Accordingly, a thorough and accurate analysis of remote work during the COVID-19 era should not exclude either of these two groups and should treat them both as separate and specific categories. Therefore, multinomial logistic regressions were the modeling strategy for the main analyses and multilevel logistic regressions were employed as robustness checks.
Results
Descriptive Results
Table 1 presents descriptive statistics for this study’s variables. In all, 63.82 percent of the sample were working at their usual place during the pandemic. While 16.87 percent were working partly remotely, 19.31 percent worked completely remotely. The average respondent was sixty-one years of age. In all, 15.58 percent of the sample reported poor or fair health. The sample’s mean extent of education was just over thirteen years (13.29). As expected, the mean of the 20-quantiles of household income (10.48) was near 10. Respondents were broadly distributed across occupations, with “armed forces occupations” holding the least (0.29 percent) and “professionals” holding the most (20.82 percent). A slight majority of the sample were women (53.12 percent).
There were appreciable amounts of variability in the DESI (mean: 54.87, standard deviation (SD): 9.79) and EM p-scores (mean: 13.21 percent, SD: 9.05 percent) among the sampled nations. The EM p-scores’ mean implies substantial pandemic-era excess deaths across Europe. While considerable, variability in the stringency index was somewhat less (mean: 47.41, SD: 5.69).
Table 2 displays descriptive statistics specific to each of this study’s 26 countries. Respondents were broadly distributed throughout these countries, with Luxembourg including the least (0.79 percent) and Estonia holding the most (14.68 percent). The remaining columns depict this study’s country-level variables and the percentages of the population of at least 15 years of age participating in the labor force in 2020 (from the World Bank Group 2022b). The latter added further relevant contextual information.
Country-level Descriptive Statistics.
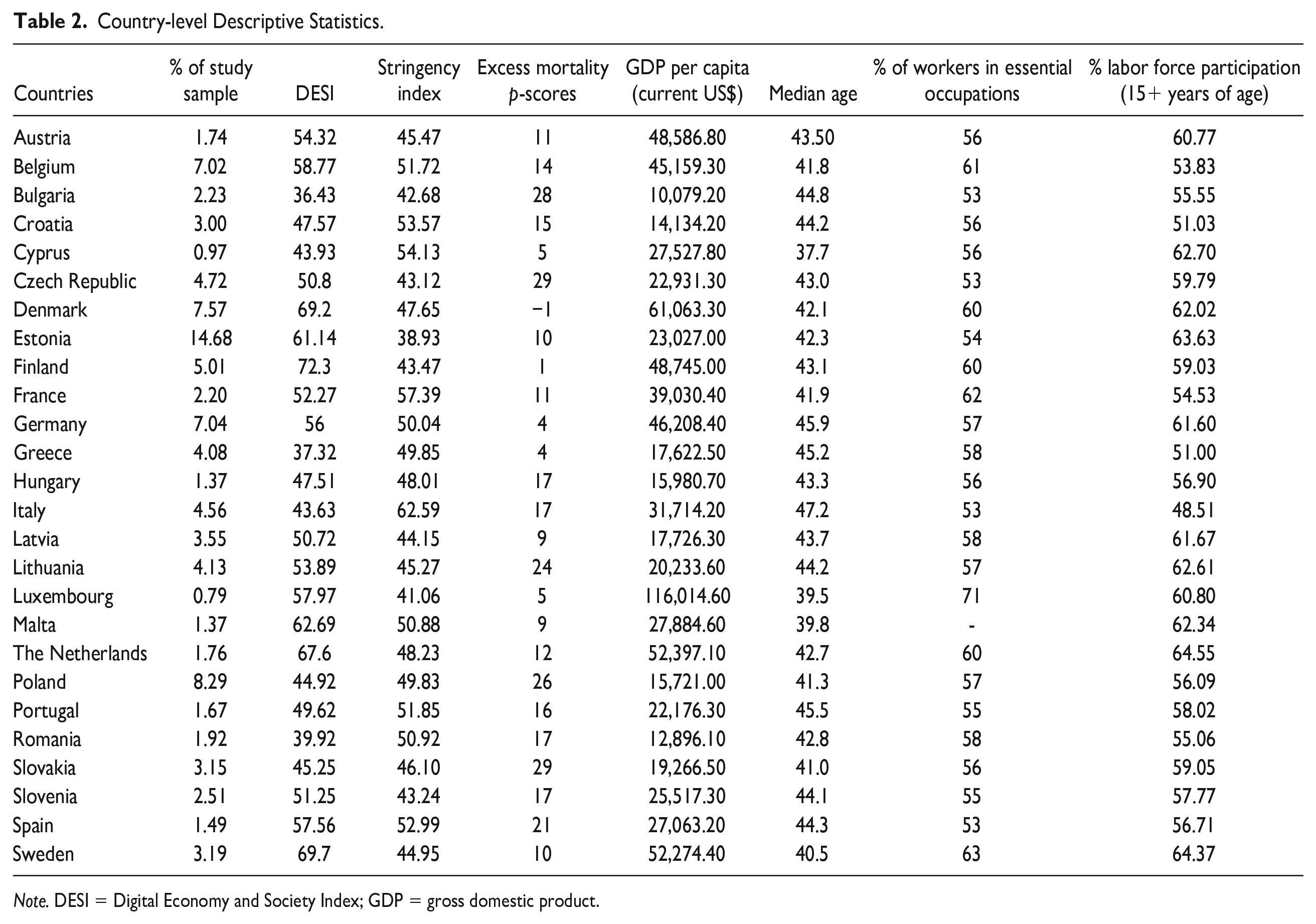
Note. DESI = Digital Economy and Society Index; GDP = gross domestic product.
Central Multinomial Logistic Regression Results
Table 3 presents the results of the multinomial logistic regression with both education and occupations, and no interaction terms. Each column depicts a dependent variable category. While substantial differences were found among the industries of employment (F-test (Wald test) revealed significant contribution to model fit (p < .0001)), they were excluded from Table 4 for parsimonious presentation of results.
Multinomial Logistic Regression Analysis of Work Circumstances, Only Main Effects Models, Reference Category Is Worked at the Usual Workplace, Relative-risk Ratios.
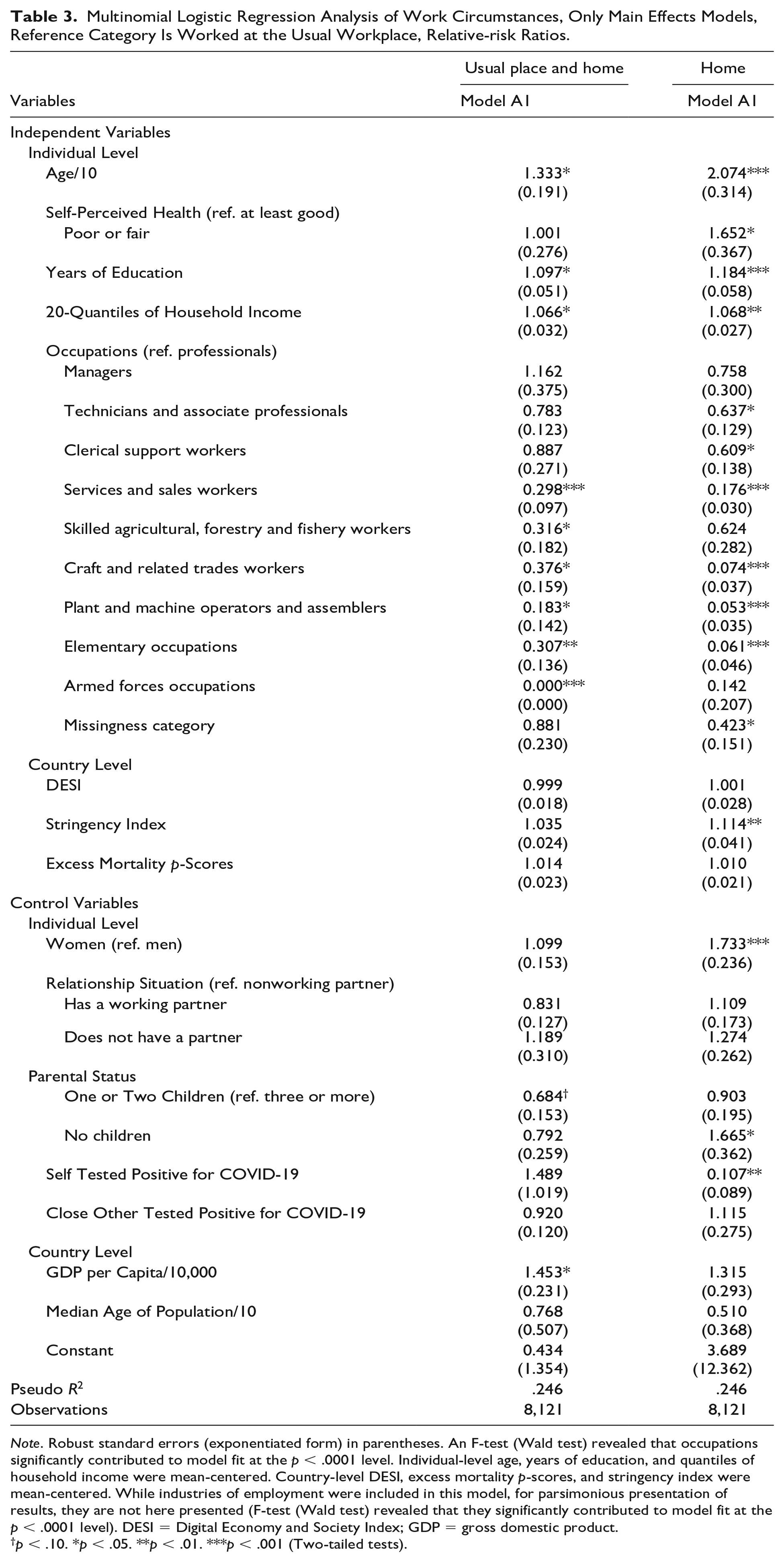
Note. Robust standard errors (exponentiated form) in parentheses. An F-test (Wald test) revealed that occupations significantly contributed to model fit at the p < .0001 level. Individual-level age, years of education, and quantiles of household income were mean-centered. Country-level DESI, excess mortality p-scores, and stringency index were mean-centered. While industries of employment were included in this model, for parsimonious presentation of results, they are not here presented (F-test (Wald test) revealed that they significantly contributed to model fit at the p < .0001 level). DESI = Digital Economy and Society Index; GDP = gross domestic product.
p < .10. *p < .05. **p < .01. ***p < .001 (Two-tailed tests).
Multinomial Logistic Regression Analyses of Work Circumstances, DESI as the Focal Interactant, Reference Category Is Worked at the Usual Workplace, Relative-risk Ratios.
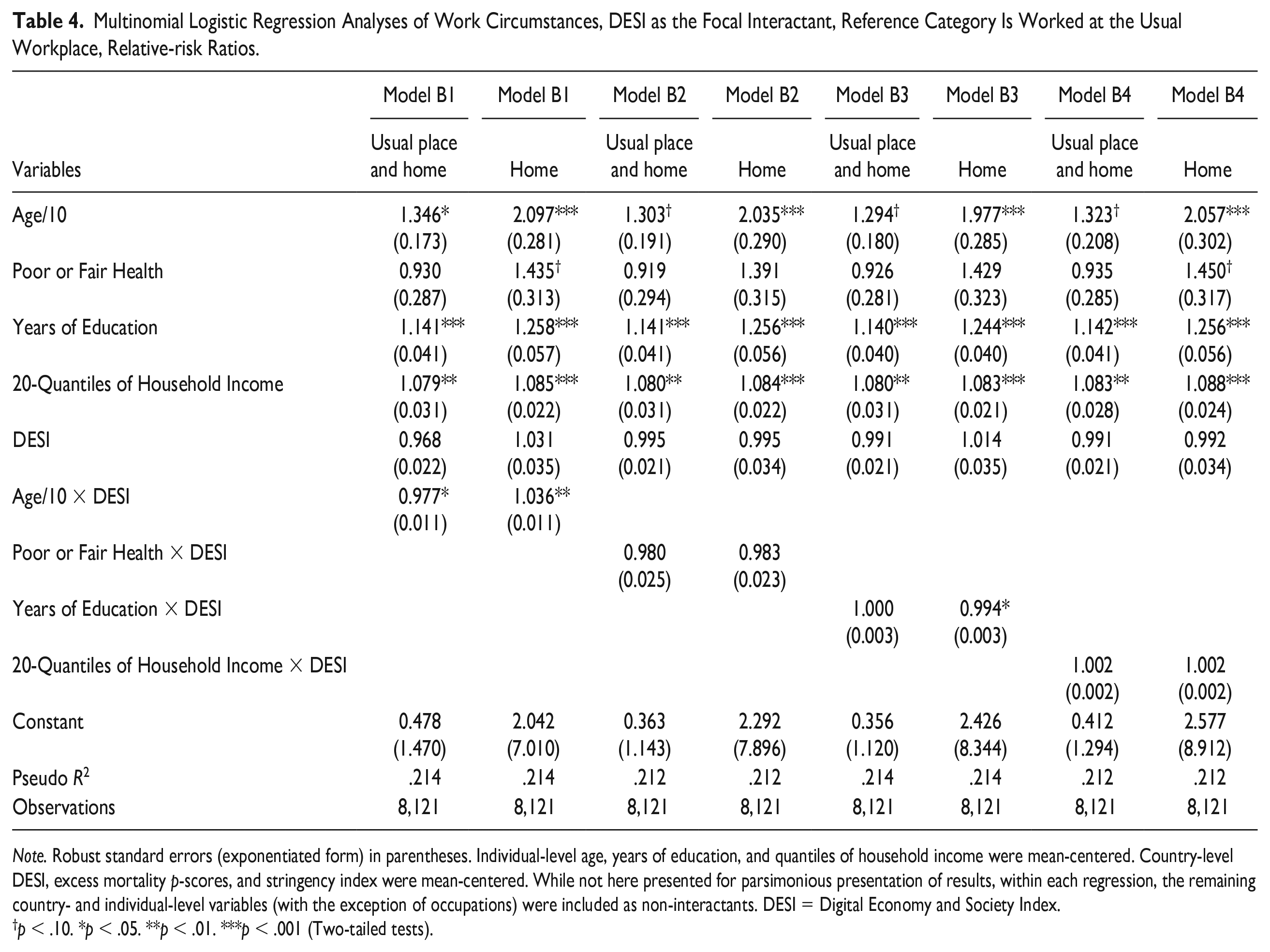
Note. Robust standard errors (exponentiated form) in parentheses. Individual-level age, years of education, and quantiles of household income were mean-centered. Country-level DESI, excess mortality p-scores, and stringency index were mean-centered. While not here presented for parsimonious presentation of results, within each regression, the remaining country- and individual-level variables (with the exception of occupations) were included as non-interactants. DESI = Digital Economy and Society Index.
p < .10. *p < .05. **p < .01. ***p < .001 (Two-tailed tests).
Seemingly discordant with the findings of Yang Li and Jan E. Mutchler (2020) and Caitlin Monahan et al. (2020), Model A1 reveals advancing age being positively associated with working partly (RRR: 1.333, p < .05) and completely remotely (RRR: 2.074, p < .001). Being in poor or fair health was positively associated with working completely from home (RRR: 1.652, p < .05). Education was positively associated with working partly (RRR: 1.097, p < .05) and completely (RRR: 1.184, p < .001) remotely. Likewise, household income was positively associated with working partly (RRR: 1.066, p < .05) and fully (RRR: 1.068, p < .01) from home. Furthermore, there is evidence that lower-SES occupations were negatively associated with working partly or fully remotely (F-test (Wald test) revealed significant contribution to model fit (p < .0001)).
Among the country-level independent variables, only the stringency index showed a significant finding (working completely from home, RRR: 1.114, p < .01). While the DESI was insignificantly associated with both outcomes, when it was studied in a bivariate model (results not shown), it significantly positively predicted remote work. This discrepancy is likely because the full models adjusted for individual-level education (among other important covariates), which likely covaries with both the DESI and remote work.
Tables 4–6 (focused on country-level DESI, stringency index, and excess mortality, respectively) present the results of models including interactions between the individual- and country-level independent variables. The columns are organized according to model and dependent variable outcome. For parsimonious presentation of results, these tables present only the individual-level independent variables (except for occupations), the respective country-level interactant, and the interaction terms. The elaboration on these results focuses on these interaction terms.
Table 4 shows that with greater societal digitalization, more advanced age did less to increase the likelihood of working partly remotely (B1, usual place and home, interaction RRR: 0.977, p < .05) and more to increase the probability of working fully remotely (B1, home, interaction RRR: 1.036, p < .01) (providing mixed evidence concerning hypothesis 1.2: the positive associations of more advanced age and worse health with remote work are increased by societal digitalization). Furthermore, with greater societal digitalization, more years of education did less to increase the likelihood of working fully remotely (B3, home, interaction RRR: 0.994, p < .05) (providing partial support for hypothesis 1.1: the positive associations of education and income with remote work are reduced by societal digitalization).
Table 5 reveals that while greater stringency of pandemic response positively moderated the association between age and working partly from home (C1, usual place and home, interaction RRR: 1.042, p < .001), it negatively moderated the association between age and working fully remotely (C1, home, interaction RRR: 0.958, p < .01) (providing mixed evidence concerning hypothesis 2.2: the positive associations of more advanced age and worse health with remote work are reduced by more stringent government containment measures). Moreover, greater stringency of pandemic response negatively moderated the association of household income with working partly remotely (C4, usual place and work, interaction RRR: 0.996, p < .05) (providing partial support for hypothesis 2.1: the positive associations of education and income with remote work are reduced by more stringent government containment measures).
Multinomial Logistic Regression Analyses of Work Circumstances, Stringency Index as the Focal Interactant, Reference Category Is Worked at the Usual Workplace, Relative-risk Ratios.
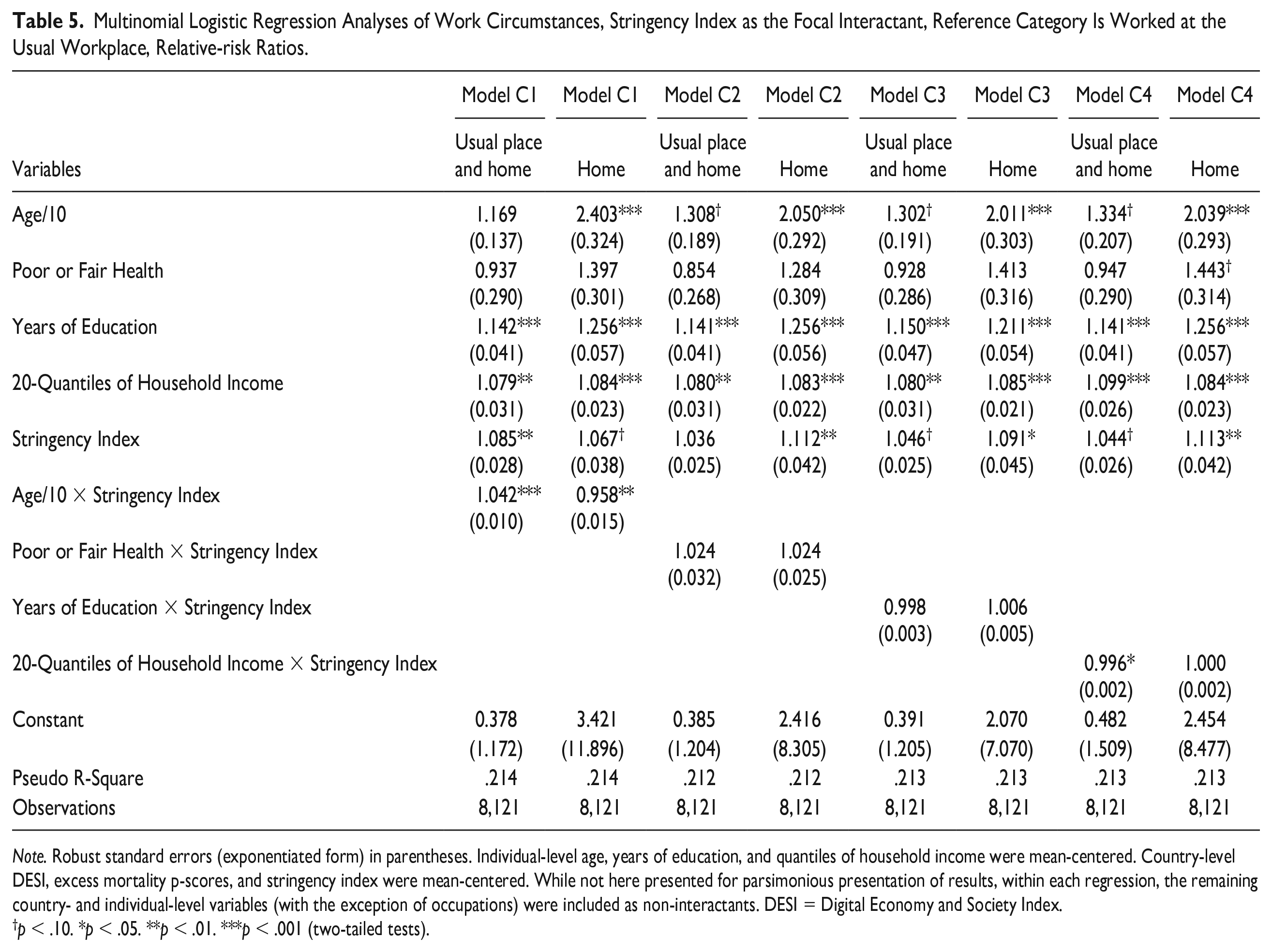
Note. Robust standard errors (exponentiated form) in parentheses. Individual-level age, years of education, and quantiles of household income were mean-centered. Country-level DESI, excess mortality p-scores, and stringency index were mean-centered. While not here presented for parsimonious presentation of results, within each regression, the remaining country- and individual-level variables (with the exception of occupations) were included as non-interactants. DESI = Digital Economy and Society Index.
p < .10. *p < .05. **p < .01. ***p < .001 (two-tailed tests).
Table 6 shows that with greater country-level excess mortality, poor/fair health did more to increase the likelihood of working partly (D2, usual place and home, interaction RRR: 1.055, p < .05) and fully (D2, home, interaction RRR: 1.039, p < .01) remotely (providing partial support for hypothesis 3.2: the positive associations of more advanced age and worse health with remote work are increased by greater contextual COVID-19 health impacts). Furthermore, greater country-level excess mortality accentuated how more education increased the likelihood of working completely from home (D3, home, interaction RRR: 1.008, p < .01) (providing partial support for hypothesis 3.1: the positive associations of education and income with remote work are increased by greater contextual COVID-19 health impacts).
Multinomial Logistic Regression Analyses of Work Circumstances, Excess Mortality p-scores as the Focal Interactant, Reference Category Is Worked at the Usual Workplace, Relative-risk Ratios.
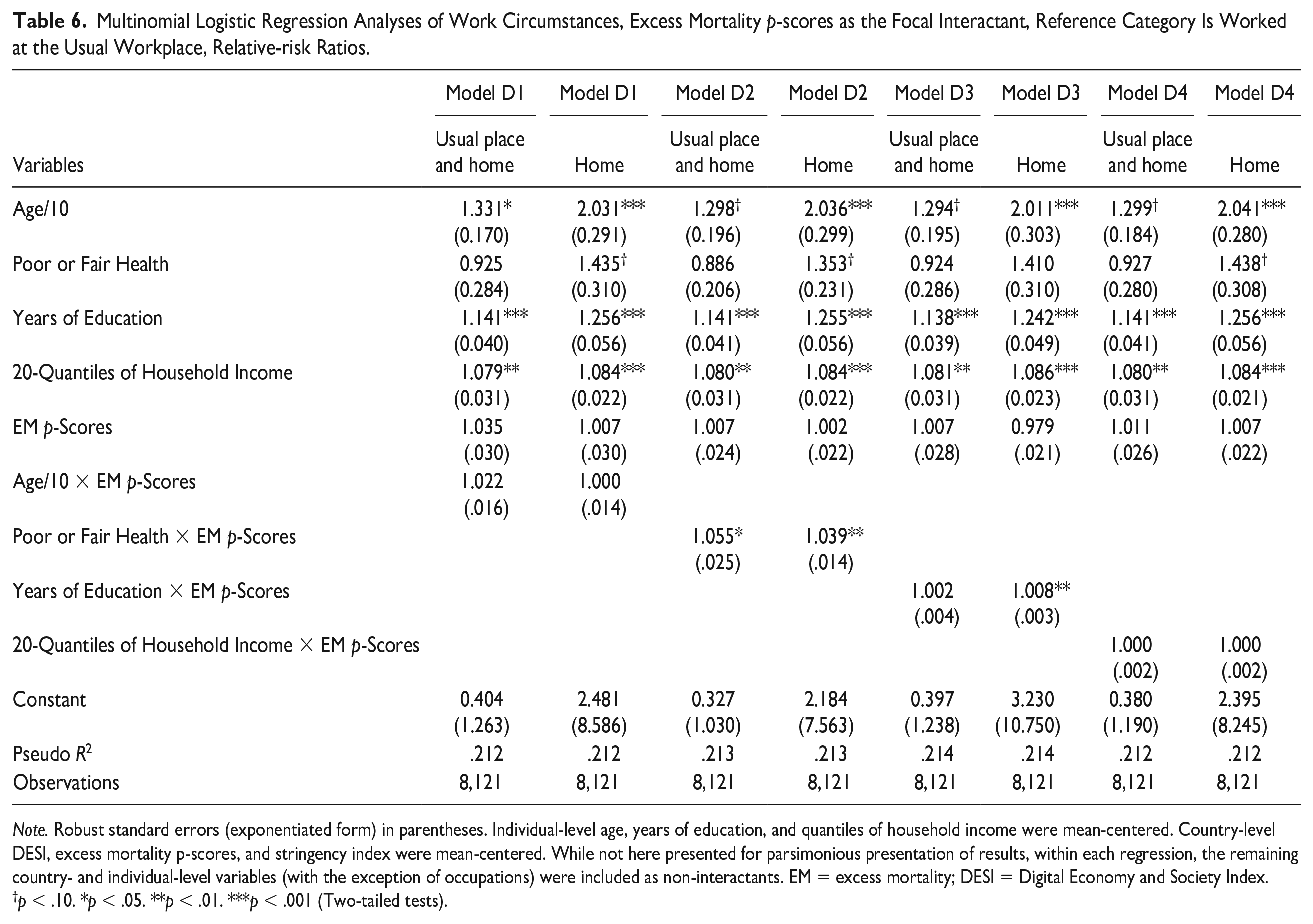
Note. Robust standard errors (exponentiated form) in parentheses. Individual-level age, years of education, and quantiles of household income were mean-centered. Country-level DESI, excess mortality p-scores, and stringency index were mean-centered. While not here presented for parsimonious presentation of results, within each regression, the remaining country- and individual-level variables (with the exception of occupations) were included as non-interactants. EM = excess mortality; DESI = Digital Economy and Society Index.
p < .10. *p < .05. **p < .01. ***p < .001 (Two-tailed tests).
Graphical Presentations of Central Interaction Findings
Figures 1–3 graphically display this study’s three most substantive interaction findings (no variables mean-centered) pertaining to working completely from home, thus revealing their magnitudes. In each case, while the country-level interactant is on the x-axis, probability of working completely remotely is on the y-axis. The first two figures include two lines, one for 10 years of education (denoting below having a high school diploma (typically 12 years of education)) and one for 16 years of education (denoting having a university degree).
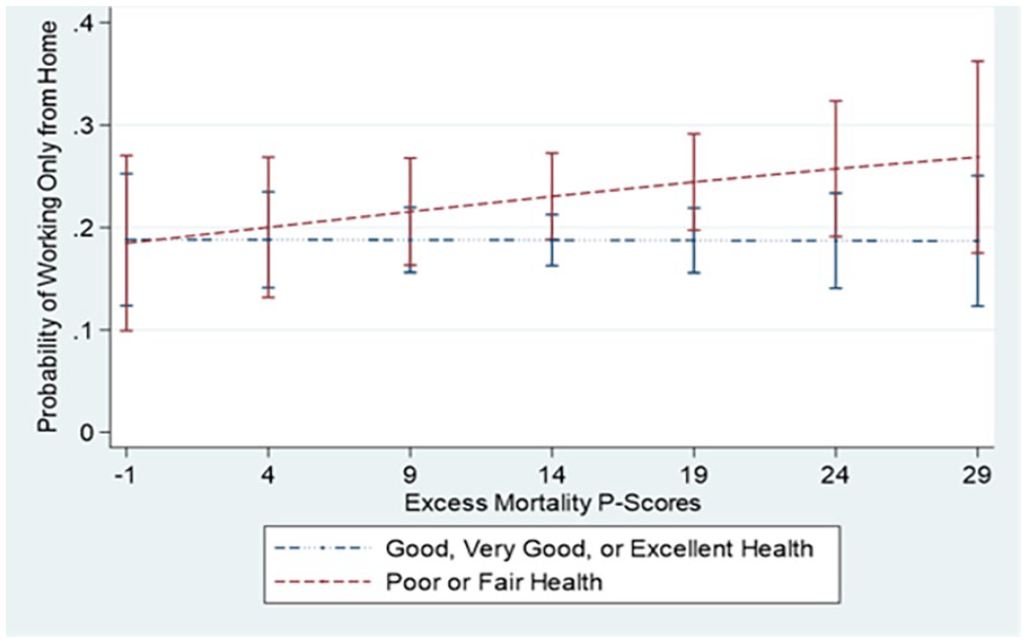
Predicted probabilities of working only from home, excess mortality p-scores in interaction with self-perceived health, 95 percent confidence intervals included.
Figure 1 displays that those with 16 years of education were consistently more likely to work completely remotely than those with ten years of education. However, with rising DESI, likelihood of working completely remotely rose only slightly for the former, while substantially increasing for the latter. In fact, these two lines’ 95 percent confidence intervals overlap as of a DESI score of 62. Among those with 16 years of education, probability of working completely from home rose from 0.25 to 0.27 as DESI scores rose from 37 to 72. The corresponding rise for those with 10 years of education was 0.07 to 0.23.
Figure 2 also reveals that more education implies higher likelihoods of working completely from home. This figure further shows that while greater country-level excess mortality only moderately increased the probability of working completely remotely for those with 10 years of education, it substantially increased this probability for those with 16 years of education. In fact, as of an EM p-score of 14, these two lines’ 95 percent confidence intervals cease to overlap. Respondents with 10 years of education showed a likelihood of completely remote work that rose from 0.10 to 0.13 as the EM p-scores rose from -1 to 29. The corresponding increase for those with 16 years of education was 0.15 to 0.38.
Figure 3 also includes two lines, one denoting poor/fair health, the other representing good/very good/excellent health. Figure 3 reveals that except at the lowest amounts of excess mortality, those in poor/fair health were more likely to work completely remotely than those in good/very good/excellent health. While rising excess mortality hardly changed the likelihood of working completely remotely for those in good/very good/excellent health, it substantially increased this likelihood for those in poor/fair health. While the 95 percent confidence intervals of these two lines overlap throughout the figure, the statistically significant interaction term on which this figure is based implies that the slopes of these two lines are significantly different. Among respondents in good/very good/excellent health, likelihood of fully remote work was 0.19 across the range of EM p-scores. However, for respondents in poor or fair health, probability of completely remote work rose from 0.18 to 0.27 as the EM p-scores rose from -1 to 29.
Supplementary Results
Table A2 in the Supplementary Appendix reveals variables that affected selection into this study’s sample of continuing workers. The significant findings across numerous variables suggest that this study’s sample of continuing workers profited from some demographic and socioeconomic advantages. As these variables affected inclusion in this study’s sample, it was important that they be included in this study’s models.
Robustness Checks Results
The central findings were substantively the same with further control for country-level percentage of essential workers.
Table A3 in the Supplementary Appendix reveals that within multilevel mixed-effects logistic regression models that accounted for the nested structure of the data and adjusted for country-level unobserved heterogeneity, this study’s three most substantive interactive findings pertaining to working completely remotely were reproduced, supporting their robustness.
Discussion
Among older Europeans continuously working through the pandemic, while notable findings were revealed for both remote work outcomes vis-à-vis continued work at one’s usual place, the most substantial findings are for working completely from home. This is of conceptual importance for at least three reasons: (1) those working completely remotely are the most protected from COVID-19, (2) those working completely from home likely profit from the greatest potentiality for remote work, and (3) those working completely remotely face the greatest adjustments to their usual work patterns.
This study reveals substantial moderation of individual-level variables’ effects by countries’ characteristics. Greater societal digitalization reduced the importance of education for working completely remotely. Greater stringency of government pandemic response significantly reduced the importance of household incomes for working partly remotely. Furthermore, higher excess mortality significantly increased the importance of both more education and worse self-perceived health for working completely from home. Since these are the most notable interactive findings that do not display ambiguities between fully and partly remote work, they are this discussion’s focus. They each display how individual-level choices are embedded within larger societal structures.
The findings pertaining to societal digitalization and excess mortality were obtained after adjusting for the stringency of pandemic control measures. Therefore, these significant findings were substantially based on the inclinations, capabilities, requests, decisions, calculations, and negotiations of employees and employers.
Some main effect findings are noteworthy. Among older Europeans continuing their work through the pandemic, more advanced age increased the likelihood of working partly or completely remotely. This is in seeming contradiction to Li and Mutchler (2020) and Monahan et al. (2020), who suggested that older workers are more likely restricted in their teleworking abilities. However, the present study addressed only adults of at least 50 years of age. A chief age-based distinction concerning remote work might be between older and younger workers (revealed within Li and Mutchler [2020] and Monahan et al. [2020]). The present study did not include this comparison, reducing the span of age-related differences in technological abilities. Furthermore, these age-based findings were obtained after controlling for education, occupation, and income, which are strong determinants of remote work capabilities (Bartik et al. 2020; Brynjolfsson et al. 2020; Dingel and Neiman 2020; Kavanagh et al. 2021). More so than in younger adulthood, advancing age in later life implies greater vulnerability to the consequences of COVID-19 infection (Landau et al. 2021; Wolf et al. 2020), a fact that obtains throughout the socioeconomic spectrum. Accordingly, in concert with the HBM, older workers within later life might show intensified remote work negotiations.
The findings that education, household income, and occupational prestige were positively associated with partly and fully working from home, likely because of employment tasks more amenable to remote work, concord with earlier scholarship (Bartik et al. 2020; Brynjolfsson et al. 2020; Dingel and Neiman 2020; Kavanagh et al. 2021). Interestingly, this implies that all three variables, though intercorrelated, are uniquely impactful upon likelihood of working remotely.
This underscores the fact that many older adults were disadvantageously positioned to weather the consequences of COVID-19, both in social life and employment, because of lack of skills with advanced digital technologies (Seifert, Cotten, and Xie 2021). Beyond associations with technological capabilities that ease remote work (Bartik et al. 2020), education increases cognitive abilities (Strenze 2007) that aid acquisition of technological skills for continued employment and social activity during the pandemic. In accordance with FCT, these results suggest that during the COVID-19 pandemic, ability to work remotely rose as a potent mechanism through which SES can affect health.
Notably, the findings reveal that after control for the country- and individual-level covariates, the main effects of country-level digitalization and excess mortality did not reach statistical significance. However, even after adjustment for these covariates, these structural features significantly moderated the effects of individual-level characteristics and were thus of substantial importance for remote work among older Europeans continuously working through the pandemic. Net of the covariates, country-level stringency of government pandemic response yielded main effects indicating significantly increased remote work, thus evidencing the importance of this structural characteristic.
The interaction findings provide answers to all three research questions. Concerning the first question (based on the DESI moderating individual-level predictors of remote work), the first hypothesis (1.1) is partially confirmed. Among older continuously working Europeans, the positive impact of education, but not household income, upon fully remote work was reduced within more digitalized nations. In concert with FCT, this suggests that a nation’s digitalization is an aspect of its progress through historical time that might reduce the potency of a specific mechanism between SES and health (in this case, ability to work remotely). Accordingly, it is a structural characteristic that reduces the importance of individual-level education for negotiating working remotely. Plausibly, the interaction with education, but not with household income, reached statistical significance because the former is more directly tied to use of advanced technologies at work.
Contrary to the first question’s second hypothesis (1.2), while age showed conflicting interactive findings between partly and fully remote work, self-perceived health’s effects were not significantly moderated by societal digitalization. Perhaps pessimistically, this suggests no consistent pattern of societal digitalization increasing the extents to which those who are older or in worse health are motivated to seek and likely to be permitted working remotely.
In answer to the second question (based on the stringency index moderating individual-level predictors of remote work), in partial support of hypothesis 2.1, greater stringency of government pandemic response reduced the positive association of household income, but not education, with working partly remotely among continuously working older Europeans. In contradiction of hypothesis 2.2, the stringency index showed no consistent moderation of how age or worse health affected working remotely. There is thus only partial evidence that when national governments have instituted strong and broad COVID-19 containment measures (structural characteristic), workers’ specific features, and the preferences and calculations of employers and employees (individual-level choices), wane is importance as predictors of remote work.
Regarding the third question (based on EM p-scores moderating individual-level predictors of remote work), the first hypothesis (3.1) is partially confirmed. Among older Europeans continuing to work through the pandemic, education, but not household income, was more strongly positively associated with working completely remotely within nations undergoing more excess mortality. Concordant with the HBM, within nations facing higher COVID-19 health impact, more educated older persons might have had intensified motivation to actualize their remote work potentialities (see Bartik et al. 2020; Brynjolfsson et al. 2020; Dingel and Neiman 2020; Kavanagh et al. 2021) and to have negotiated with their employers for work-from-home arrangements. Also in accordance with the HBM, employers might have calculated that permitting these employees to work remotely will have provided their organizations with health protection while minimizing efficiency and productivity losses. The nonsignificant interaction finding for household income was plausibly because income is less directly related than education is to the use of ICTs and internet technologies at work.
This finding highlights the accentuated disadvantages faced by employees with less education within countries with higher COVID-19 health impact and the importance of practical constraints on work-from-home arrangements. Because their employment tasks are less amenable to remote work, these workers’ greater preferences for working remotely might not be realized. Employers might prioritize efficiency and productivity by primarily arranging for their more educated employees to work remotely. Within structural circumstances of greater need for remote work, accentuated individual-level desires to work remotely are more likely to be realized by those benefiting from more education.
Partially confirming the second hypothesis (3.2), worse self-perceived health, but not more advanced age, was positively moderated by country-level excess mortality in its predictions of partial and fully remote work among older Europeans continuously working through the pandemic. The HBM also helps interpret this finding, which is likely influenced by pandemic-era apprehensions (Loustaunau et al. 2021). Because of heightened vulnerability to the health consequences of COVID-19 infection (Wolf et al. 2020), older persons in worse health might experience intensified wariness of COVID-19 when their environments include higher COVID-19 health impacts. They might make more extensive requests for work-from-home arrangements that their employers are more willing to grant. This finding is a cause for optimism, as both structural conditions and individual-level choices here operate in concert. The nonsignificant interaction finding for age might be because it does less than worse health does to accentuate fears of COVID-19.
These two interactive findings with country-level COVID-19 health impact highlight how need for remote work (related to worse health) and feasibility of working remotely (related to education) are integrated, such that greater country-level risk magnifies how both are associated with working from home.
Theoretical Implications
This study suggests that FCT scholarship should further consider variations in SES-health mechanisms based on structural differences across geographical locations, additional to structural changes across historical time. Both types of structural variations condition individual-level characteristics and choices. Moreover, related to historical structural changes, the COVID-19 pandemic has shown the importance of unpredictable chance events in influencing patterns of health based on SES, including accentuating the importance of particular mechanisms (at least for a period of time). FCT scholarship should further consider the importance of such unpredictable chance events. The pandemic accentuating the mechanism based on remote work potentiality provides new evidence that bolsters the veracity and usefulness of FCT; in this specific circumstance, SES develops new health-protective potencies. Further warranting scholarly attention, remote work will likely be increasingly accepted in the future as a structural consequence of the pandemic (Kun, Shaer, and Iqbal 2021). SES will likely be associated with both potential to work remotely and its health outcomes (see Schieman and Glavin 2011). Accordingly, mechanisms between SES and health based on remote work will likely increase in importance in future times.
While the HBM has primarily elucidated individuals’ behaviors regarding their own health concerns, the COVID-19 pandemic exemplifies how this model also applies at the structural levels of work organizations and governments (meso and macro levels). In the pandemic era, employers and governments are also required to evaluate risks, calculate costs, and employ the most rational behavioral strategies. These evaluations and calculations, at all levels, are substantially affected by perceptions of vulnerability to COVID-19 (including based on individual-level age and health, and country-level health impacts), and ease and feasibility of transferring to remote work (including based on individual-level education, income, and occupation, and country-level digitalization). A stated limitation of HBM scholarship is that it inadequately addresses how more macro-level structures can facilitate or hinder individual-level health behaviors and decisions (Kim and Kim 2020; Rejeski and Fanning 2019). The COVID-19 pandemic further encourages this expanded focus.
Policy Recommendations
This study provides recommendations for responses to future infectious epidemics. The interaction findings imply that persons with less education in less digitalized economies and societies will face obstacles to working remotely during future epidemics. Furthermore, within the more dangerous structural circumstances of greater country-level health impacts, persons with less education will experience more difficulty protecting themselves by transitioning into remote work. Therefore, especially within national structural circumstances of lower digitalization and/or greater health impacts, further provisions should be made for remote work and/or more sanitary employment environments, particularly for workers with less education, whose choices will be further restricted.
Moreover, especially among those with less education, policies and programs should help older adults with fewer skills with ICTs and internet technologies in acquiring these capabilities (Seifert et al. 2021). Training in digital technologies provides older persons with social and well-being advantages (see Czaja et al. 2018). This is of especially strong relevance to the COVID-19 era and future epidemics, during which many older persons will desire working remotely and will face social restrictions.
The finding that those is worse health are especially motivated to work remotely within nations with greater COVID-19 health impacts leads to recommendations that governments and employers give priority to those in worse health when making decisions concerning work arrangements. Policies concerning work-from-home arrangements during epidemics should generally be responsive to workers’ vulnerabilities and capabilities to work remotely, based on both individual- and country-level characteristics.
More broadly, this study speaks to older persons’ ability to remain employed through a widespread medical shock. During the COVID-19 pandemic, remaining employed is strongly related to remote working capability (Béland et al. 2020). In fact, older adults are at greater risk of being laid off during the pandemic, the reasons for which include fewer technological skills (Celbiş et al. 2022; Li and Mutchler 2020; Monahan et al. 2020). Accordingly, efforts should improve internet infrastructure and re-organize jobs to be more easily adjusted for remote work in case of widespread medical emergencies, thus preventing many workers across many occupations from losing their employment. Additionally, for older adults especially, more on- and off-the-job training in advanced digital technologies should be provided.
Limitations and Future Research Paths
This study’s focus on older adults is effective because they showed especially strong health (Wolf et al. 2020) and economic (Li and Mutchler 2020) consequences of COVID-19. However, the interactions between structural features and individual-level characteristics here studied might have contrasting effects upon the remote work of younger workers because of differences in health, economic and employment circumstances, family arrangements and responsibilities, and so on. Future research should replicate this study’s analyses with younger samples.
This study investigated three important country-level variables as structural moderators of individual-level variables’ effects upon remote work. However, other country-level structural variables might also be potent moderators. For example, welfare state provisions and COVID-19-era-specific economic protection measures might have affected fears of unemployment and business closure, influencing negotiations between employers and employees concerning remote work. Healthcare systems’ coverages and capacities are structural characteristics likely affecting fears of morbidity and mortality from COVID-19 infection, influencing employees’ requests for and employers’ allowances of remote work. Future research should study complex interactions with other important country-level structural variables.
Supplemental Material
sj-docx-1-spx-10.1177_07311214231167171 – Supplemental material for Conditional on the Environment?: The Contextual Embeddedness of Age, Health, and Socioeconomic Status as Predictors of Remote Work among Older Europeans through the COVID-19 Pandemic
Supplemental material, sj-docx-1-spx-10.1177_07311214231167171 for Conditional on the Environment?: The Contextual Embeddedness of Age, Health, and Socioeconomic Status as Predictors of Remote Work among Older Europeans through the COVID-19 Pandemic by Jason Settels in Sociological Perspectives
Footnotes
Acknowledgements
This paper uses data from SHARE Waves 2, 4, 5, 6, 7, and 8 (DOIs: 10.6103/SHARE.w2.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800, 10.6103/SHARE.w8ca.800), see Börsch-Supan et al. (2013) for methodological details. The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see www.share-project.org). This paper uses data from the generated easySHARE data set (DOI: 10.6103/SHARE.easy.800), see ![]() for methodological details. The easySHARE release 8.0.0 is based on SHARE Waves 1, 2, 3, 4, 5, 6, 7 and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800).
for methodological details. The easySHARE release 8.0.0 is based on SHARE Waves 1, 2, 3, 4, 5, 6, 7 and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the 2020 Research Block Grant Allocation Scheme–Merit Based Funding Scheme: Incentive B, Faculty of Humanities, Education and Social Sciences, University of Luxembourg. This funding source had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the article; and in the decision to submit it for publication.
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.