
Abstract
HIV stigma negatively affects the social experiences of people living with HIV (PLWH) and remains a challenge to HIV prevention, treatment, and care. Research has overwhelmingly focused on individual cognitive measures of HIV stigma (e.g., internalized, anticipated, and experienced). However, little research explores the interactions and societal structures through which HIV stigma is produced. Data from qualitative interviews with 30 black gay and bisexual men living with HIV in the U.S. Deep South revealed an interconnected and interdependent set of processes that produce and reproduce HIV stigma. These included social interactions (silence, euphemism, and gossip), witnessed acts of marginalization, word-of-mouth transmission of HIV misinformation, and laws and policies carried out within the education and criminal justice systems. Efforts to reduce stigma that focus on individual beliefs and attitudes are critical to improving the well-being of PLWH. However, reducing HIV stigma requires intervening on the social interactions and structures through which HIV stigma is produced and reproduced.
Introduction
Most HIV-stigma research begins with Goffman’s conception of stigma as a mark or characteristic that results in reduced social value for people with that characteristic (Goffman 1963). Despite Goffman’s call for a “language of relationships,” there has primarily been a focus on individual perceptions of stigma and the consequences of those perceptions—individual acts of discrimination and rejection. According to Richard Guy Parker and Peter Aggleton (2003), that research has proceeded “as though stigma were a static attitude rather than a constantly changing (and often resisted) social process has seriously limited the ways in which stigmatization and discrimination have been approached in relation to HIV and AIDS” (p. 14). As noted by several authors, stigmatization occurs in a power situation in which the stigmatizing group has more power than the group being stigmatized (Gilmore and Somerville 1994; Link and Phelan 2001). As a group, people living with HIV possess less social power than those who are not living with HIV, and many groups who occupy a marginal social status prior to receiving an HIV diagnosis (e.g., people of color, gay men, sex workers, or people who inject drugs) have even less power to resist stigmatization (M. T. Berger 2010; Gilmore and Somerville 1994; R. G. Parker and Aggleton 2003).
Indeed, research has shown that HIV/AIDS stigma is layered onto other stigmatized identities (e.g., injection drug use [IDU], homosexuality, and commercial sex [CS]), such that “disease stigma of HIV/AIDS is a derivative of the negative meanings attached to IDU and CS, and not the other way around” (Chan et al. 2007:9). Stigma occurs through social relations in which some are made to feel superior while others are devalued and excluded (R. G. Parker and Aggleton 2003). This exclusion is reproduced through social relations, and thus, stigma should be viewed through its relationship to social structures and power relations (Link and Phelan 2001). As argued by George Herbert Mead and Herbert Mind (1934), the self is constructed by taking on the attitudes of the social group, which is learned through social interactions. Thus, one-on-one and community-level gossip, for example, helps to create social meanings and to determine appropriate social behaviors (Fine and Rosnow 1978). Thus, the HIV-stigma production process is ongoing and involves not only labels and stereotypes, but also actions and interactions.
Beyond the individual cognitive processes typically explored in public health HIV-stigma research, stigma occurs at multiple levels (e.g., interpersonal, community). Increasingly, research has explored structural stigma, which refers to societal norms, laws, policies, and institutions (Campbell 2021b; Hatzenbuehler 2016; Hughto, Reisner, and Pachankis 2015; Miller et al. 2018). Importantly, the processes operating at these multiple levels are interacting and cooperating in the production of HIV; “Stigma emanates from many societal and individual systems whose interconnections cannot be divorced from one another. They coexist in a dynamic relationship in which there is an interplay across, for example, the media, the community, and the individual” (Pescosolido and Martin 2015:102).
In this study, I describe HIV-stigma production as an ongoing process operating within structures and through interpersonal and community interactions, with each of these somewhat dependent on the others. Conceptualizing the HIV-stigma production process in this way builds on what is known about HIV stigma at these various levels by describing the ways in which they function as a system. Furthermore, model I present emphasizes that HIV stigma is not “a static attitude” (R. G. Parker and Aggleton 2003:14), but is always being produced and reproduced, and evolves through these social processes.
HIV and HIV Stigma among Black Gay and Bisexual Men in the South
According to the Centers for Disease Control and Prevention (CDC 2020b), black gay and bisexual men continue to bear a disproportionate burden of new HIV diagnoses, accounting for a quarter of all new infections in the United States. Using data from 2010 to 2014, researchers estimated that, if infection rates remained the same as they were at the time of their analysis, one in two black gay and bisexual men would contract HIV in their lifetimes (Hess et al. 2017). Furthermore, lower proportions of black gay and bisexual men living with HIV are linked and retained in care, are currently on treatment, or reach viral suppression compared with white gay and bisexual men (Hoots et al. 2017; Millett et al. 2007; Rosenberg et al. 2014). Importantly, black gay and bisexual men are no more likely than other gay and bisexual men to engage in sexual behaviors considered higher risk (Harawa et al. 2004; Millett et al. 2006; Sullivan et al. 2015). Instead, these disparities are driven by structural realities including segregation, housing insecurity, and economic inequality, as well as racism, homophobia, and stigma (Arnold, Rebchook, and Kegeles 2014; Campbell 2021a, 2021b; Hunter 2010; C. M. Parker et al. 2017; Quinn, Bowleg, and Dickson-Gomez 2019; Sullivan et al. 2021).
States in the U.S. South have the highest HIV and AIDS diagnosis and death rates (Hanna et al. 2012; Reif, Safley, and McAllaster 2015). Louisiana and Baton Rouge rank fourth in the rate of new diagnoses among states and metropolitan areas in the United States, respectively, and in 2018, gay and bisexual men accounted for 60 percent of all new diagnoses in the state (CDC 2020a; State of Louisiana Office of Public Health 2018). Furthermore, in the Southeast region, blacks are less likely than non-blacks to be linked to care at any point post-diagnosis (Rebeiro et al. 2017).
HIV stigma has played a significant role in higher rates of infections among black gay and bisexual men, and contributes to disparities in diagnosis, treatment, and care for those living with HIV (Jeffries et al. 2015; Overstreet et al. 2013; Reif, Wilson, and McAllaster 2018). Black gay and bisexual men have described a need to guard their privacy in response to gossip and unwanted disclosure in their communities and internalizing pre-existing negative ideas about HIV once they were diagnosed (Bird, Eversman, and Voisin 2017; Bird and Voisin 2013; Jeffries et al. 2015). Furthermore, some explained that, in their communities, HIV was seen as a judgment for immorality, and that members of their families and broader communities had rejected them and perpetuated negative ideas about HIV (e.g., HIV is a death sentence) and people living with HIV (e.g., they are tainted, nasty, and sick) (Arnold et al. 2014; Bird and Voisin 2013; Jeffries et al. 2015).
Quantitative HIV-stigma research has focused on measuring cognitive, individual-level stigma mechanisms, including perceived (i.e., awareness of stigma), anticipated (i.e., expectations of negative treatment), enacted (i.e., negative reactions or discriminatory treatment), and internalized (i.e., accepting and applying negative ideas about HIV and people living with HIV to the self) stigma (Bauermeister et al. 2019; Earnshaw et al. 2013; Sang et al. 2018). Among black gay and bisexual men living with HIV, these are associated with increased depression and anxiety, lower uptake of prevention strategies, nondisclosure, poor medication adherence and lower retention in care (Balaji et al. 2017; Brewer et al. 2020; Eaton et al. 2018; Miller et al. 2016; Overstreet et al. 2013; Sang et al. 2018). Importantly, these individual-level constructs have also been taken up in qualitative studies in which participant narratives largely agree with quantitative findings (Arnold et al. 2014; Bird et al. 2017; Bird and Voisin 2013; Jeffries et al. 2015; Quinn et al. 2017).
Resulting from these individual-level analyses, most HIV-stigma interventions have relied on individualistic social-cognitive approaches to improve HIV knowledge; increase awareness, acceptance, and compassion toward people living with HIV, among those not living with HIV; as well as to improve self-image and coping among people living with HIV (see Brown, Macintyre, and Trujillo 2003; Sengupta et al. 2011; Stangl et al. 2013). However, in a recent systematic review of stigma interventions, W. Dunbar et al. (2020) identified just two interventions in the United States that aimed to reduce HIV stigma among black gay and bisexual men. In one of those studies, the authors found that, while stigma declined over time, changes in perceived, anticipated, and experienced HIV stigma differed according to education level, HIV status, and whether participants described having experienced HIV stigma (Bauermeister et al. 2019). The second study measured similar stigma mechanisms, with the addition of internalized HIV stigma, and found only a nonsignificant decline in stigma (Hosek et al. 2015). While addressing the effects of stigma on the mental and physical well-being of people living with HIV is necessary, the social processes through which stigma is produced must also be addressed.
Socio-structural Setting
In the South, the cultural norms around sexuality and HIV are largely a matter of silence (Foster and Frazier 2008). Indeed, heterosexism, HIV stigma, and a general silence around sexuality are embedded structurally, particularly in the public school system. In the state of Louisiana, sex education is not required at any grade level (SIECUS 2018), and any school that provides sex education cannot include “any sexually explicit materials depicting male or female homosexual activity” (Louisiana Revised Statute §17:281(A)(3)). Furthermore, in the East Baton Rouge Parish health education standards, very little specific guidance is provided for HIV education, and abstinence is emphasized in the health standards for Grades 8 to 12. While, for Grades 9 to 12, the standards include methods of transmission and symptoms of HIV, they also include stigmatizing language such as “analyze the cost of medicines to treat HIV and other STDs/STIs and how these illnesses affect a person’s ability to attend school or maintain employment” (East Baton Rouge Parish School Board 2019).
Furthermore, HIV stigma was a major motivation for HIV criminal laws and, in turn, these laws reinforce HIV stigma. Louisiana incarcerates its citizens at a higher rate than any other state in the United States (Carson 2020) and has implemented specific laws criminalizing HIV nondisclosure (Lehman et al. 2014). In the state, intent to infect is not required for prosecution, and behaviors such as mutual masturbation and spitting, which have minimal risk of transmission are included among those for which one can be prosecuted (The Center for HIV Law and Policy 2020).
The Present Study
The extant literature on HIV stigma among black gay and bisexual men has remained focused at the interpersonal and intrapersonal level using social psychological measures. To date, no theoretical model of HIV stigma goes beyond positioning stigmatizing behaviors, laws, and policies as manifestations of HIV stigma to describing them as a part of a process of HIV-stigma production and reproduction. In this article, I begin to fill this gap with a model of HIV-stigma production based on the narratives of black gay and bisexual men living with HIV in the deep south region of the United States. This theoretical model refocuses attention away from individual beliefs and attitudes, and toward social interactions, institutions, and structures. In viewing HIV stigma in this way, research and efforts to reduce HIV stigma can focus on addressing structural inequities and community-level interactions.
Method
Between June 2019 and July 2020, 30 black gay and bisexual men living with HIV from the Baton Rouge, Louisiana Metropolitan Area participated in semi-structured, in-depth interviews. Qualitative interviews are an effective method for focusing on the domains of the interview while allowing participant insights and lived experiences related to the subject of focus to emerge (Charmaz 2014; Creswell 2012). Grounded theory interviewing methods also “conceptualize social life as a process that is the production of the simultaneous shaping of different aspects of social life and human agency” (Cuadraz and Uttal 1999:161). Interview domains included childhood and adolescence, family dynamics during childhood and adulthood, current relationships, HIV diagnosis experience, social support, romantic and sexual relationships, community norms regarding sex and sexuality, health and health care, HIV stigma, and HIV status disclosure.
Data Collection
Participants were recruited using a number of strategies, including flyers at clinics and doctors’ offices, advertisements on gay dating sites, announcing the study at community events, and referrals by well-connected community members and previous participants. Men were eligible if they self-identified as a black or African American cisgender man, were above the age of 18 years, engaged in sexual and/or romantic relationships with other men, resided in the Baton Rouge metropolitan area, and were living with HIV. Interviews lasted between 60 and 90 minutes, on average. Half of the interviews were conducted in person, and due to COVID-19 restrictions, half were conducted by phone or internet. All interviews were digitally recorded and transcribed verbatim. This research was approved by the institutional review board (IRB) of the University of California San Francisco, and all participants provided verbal consent.
Analysis
I conducted open coding on the first third of interviews to develop the initial codebook. In line with a grounded theory approach, data analysis began during, and continued throughout, the data collection process (Charmaz 2014). Subsequently, I eliminated redundancy and categorized codes into parent codes. I coded all interviews using MAXQDA 2020 qualitative software (VERBI Software 2019). While coding interview transcripts, I wrote extensive memos to identify and explore emerging themes. Analysis of text segments coded with the “HIV-stigma” code revealed clear patterns of social behaviors and interactions. Men’s narratives illuminated the ways in which HIV stigma is being produced and reproduced in their communities. To answer the research question on how HIV stigma is stigmatized at the intrapersonal, interpersonal, community, and structural levels, this analysis focused on the following codes, from which a theory of an ongoing process of HIV-stigma production emerged: HIV stigma, HIV silence, gossip, fear, euphemisms for HIV, pre-diagnosis HIV attitudes, sex education, and HIV criminalization.
Results
Men in this sample ranged in age from 18 to 56 years (M = 35.21) and had been living with HIV for an average of 10.33 years (range = 4 months–32.5 years). Twenty-eight men (93 percent) were born and grew up in the Baton Rouge Metropolitan Area. Two-thirds (66 percent) had at least some college education, and the majority were employed full-time. Despite being employed, however, nearly half (46 percent) of the sample earned less than $20,000 per year, 21 percent made less than $10,000 per year, while less than a quarter (24 percent) earned more than $40,000 per year. A large majority (83 percent) identified as gay/homosexual; the other 17 percent identified as bisexual, same-sex loving, or fluid. At the time of their interviews, all men reported being on treatment and having an undetectable viral load, and three had received an AIDS diagnosis at some point since they had been living with HIV.
Analyzing men’s narratives regarding the treatment of HIV and people living with HIV in their community revealed an interconnected and interdependent set of processes at several levels, making up an ongoing process of HIV-stigma production and reproduction (Figure 1). These included (1) Social Interactions—silence, euphemism, and gossip; (2) Individual—witnessed and experienced marginalization; (3) Community Interactions—a process of (mis)education; and (4) Social Institutions—laws and policies carried out within the education and criminal justice systems. Each of these is a component of an ongoing process, in which each component relies to some extent on the others to perform its role in the process. A theoretical model representing this process and the relationships between the components is shown in Figure 1. In the results that follow, I describe each component and its role in the process of producing and reproducing HIV stigma. The participant who provided each representative quote is identified by a pseudonym, his age, and the number of years he had been living with HIV at the time of the interview, for example, Martin (30; 4).
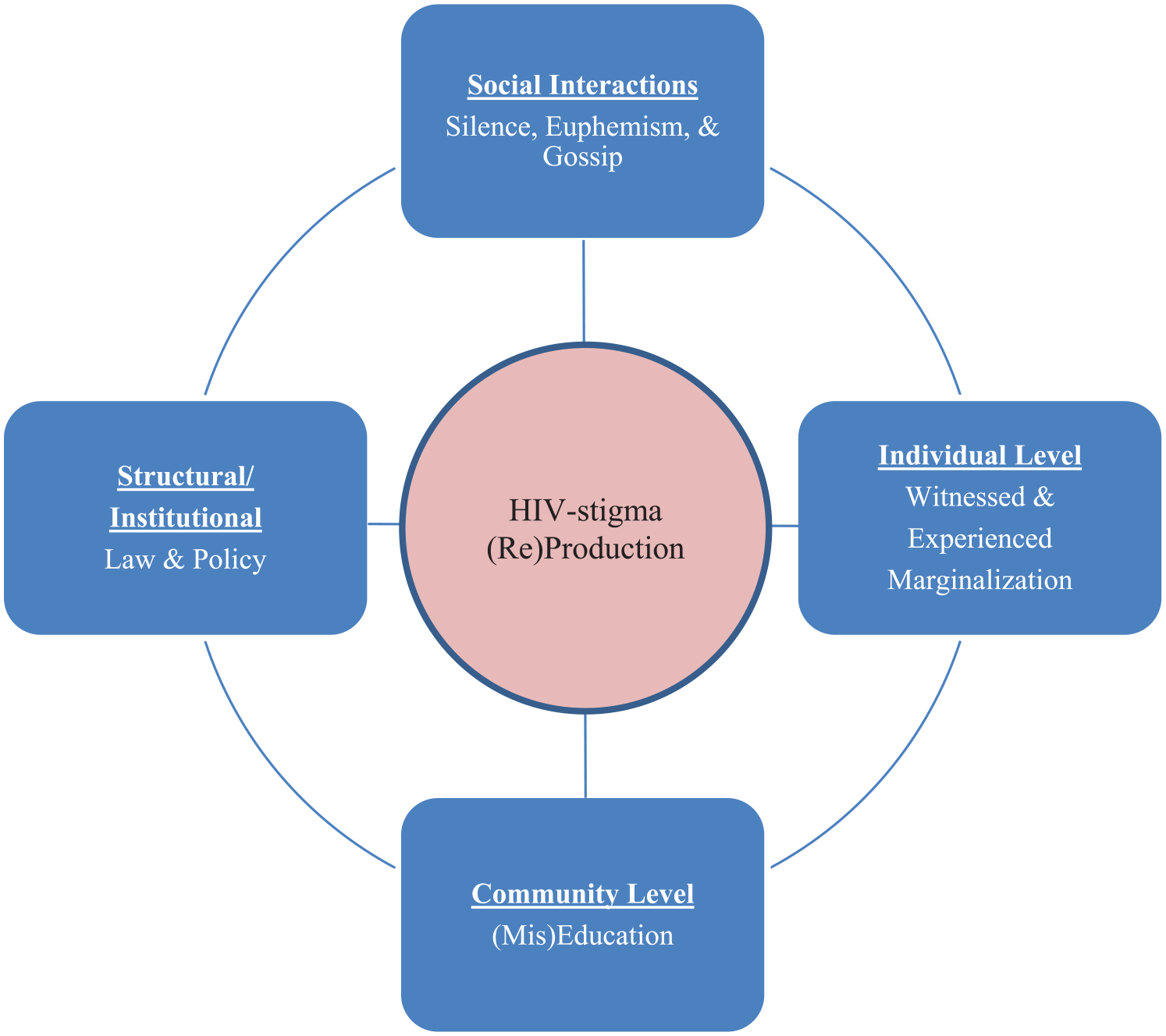
Model of ongoing (re)production of HIV stigma.
Social Interactions: Silence, Euphemism, and Gossip
Men’s narratives depicted a mutualistic symbiosis between silence, the use of euphemisms for HIV, and gossip. These functioned together to structure an environment in which HIV is not to be discussed, save for its use as a tool of shame and social control. Existing levels of HIV stigma in the broader community provided the foundation for these interconnected social actions and their uptake served to perpetuate the stigma production process. Each featured prominently in men’s narratives, which described a general practice of silence in their families and communities, and, when HIV was discussed, it was often cloaked in euphemistic terms that allowed the virus to remain unnamed. Euphemisms did not stand out as a prominent discrete subtheme. Instead, as illustrated in the following, these euphemisms for HIV (e.g., “situation,” “that shit,” “that gangsta,” and “the stuff”) feature prominently and are woven throughout narratives of silence and gossip.
Silence
Several men described the role of silence around HIV in their families. This was true for men who had disclosed their diagnosis and those who had not. Tyrone’s (35; 14) family was supportive after he disclosed his diagnoses, but HIV was not a comfortable topic of discussion. After learning for the first time that his viral load was undetectable, he felt “blessed” and was excited to tell his mother. She responded, “‘shhh. Don’t talk about that so much.’ She felt that it was a parent-son thing that not everyone should know about.” As was clear in the narratives of a number of men, discussing details of HIV was not comfortable for them or their family members, even when those family members were aware of their status. Shawn (42; 14) described that he does talk to his grandmother about his health: “We talk about it all the time, as far as my health-wise. But she really doesn’t really talk about it. We don’t really talk about it in depth.”
To be sure, some men preferred not to talk about HIV with their families, generally speaking, or with specific members of their families. For example, Kyle (55; 27) described having told his sisters about his diagnosis many years ago. However, it is something that they do not discuss and have never discussed. I asked what it was like to have his family never discuss his health. “It’s fine with me. It’s very good with me because that doesn’t define me as a person. It’s just something we don’t talk about.” Similarly, after disclosing to his cousin, Jamar (32; 9) described that they “had the understanding. We knew. We just never talked about it again.”
Men also described that, outside of their families, HIV is largely a topic that is not to be discussed. Some men felt this was because HIV is seen as something that only affects other people. As Darius (23; 4) described, “I feel like if you’re not affected by it, or if anybody in your family is not affected by it, most people here aren’t concerned. If it doesn’t concern them, they don’t care.” Tyrone (35; 14) suggested that there are two options around HIV in the community—either one does not speak of HIV at all or one speaks of it only using stigmatizing euphemisms: In Baton Rouge I don’t think people really talk about it like that. I’ve heard people talk about it, they talk about it, like “that shit” or “that gangsta,” they talk about it like that still . . . I don’t think people talk about HIV . . . Not even in general. . . just a regular gay person? Probably so, because it’s a gay culture thing. But a straight person, probably not because it’s been a part of our culture since the beginning of time, even though it’s not a gay disease. It’s just weird because it’s been a part of our culture. The people in Baton Rouge, it’s a part of their culture too.
He further highlights what he sees as a perceived cultural separation between heterosexual and gay communities in terms of living with HIV. For the heterosexual community, HIV is seen as only affecting gay men and, therefore, there is no need for them to discuss it.
Others highlighted the role of existing stigma in preventing education about HIV and discussing it openly: We didn’t hear about it at [college] . . . You know? It was nothing. It was like no one to model yourself after. There was nobody. There was no nothing. HIV was just this unspoken truth that carried a whole lot of bad shit with it. You know? . . . There’s still the stigma. They’re still living in that stigmatizing, demeaning world with HIV of what TV and the public portrays it to be opposed to what science tells you. (Jonathan, 32; 11)
Two other men explained why they believe it is a taboo subject: . . . if they do talk about it, it’s negative. . . Because, I don’t know, I guess it’s a subconscious thing with people, because it has this big, negative look on it. . . so people just don’t like to deal with that. (Nathan, 30; 1) Everybody’s just walking around like zombies to me, because they’re like . . . They know we’re up here, statistically, but they’re like, “It don’t affect me.” You know? Go walking around like it doesn’t affect them . . .
Do people talk about HIV?
Hell, no. . . They’re afraid. They are afraid. They are afraid. (Kyle, 55; 27)
When it comes to disclosure, some men described a culture of just keeping a positive diagnosis to oneself. “They hide it down here. . . It’s like, they don’t tell. They don’t tell you . . . To cover their ass? I really don’t know. (Bryce, 18; 4 months)
As each of these men describe, HIV is largely treated as a topic that should not be discussed, and conversations about it come with great social risk in the community. Indeed, even in the context of our interviews, the word HIV was rarely uttered by most participants, illustrating that they were in the practice of talking about HIV using euphemisms in place of the letters.
Another way in which silence functioned as a tool of stigma was illustrated by men who described their own silent reactions in the face of stigma, as a way of protecting themselves. Chance (34; 2) described what it is like for him to hear negative conversations about stigma in his community: I hate it man, it makes me want to go into a shell. It makes me feel like there’s an elephant in the room. Especially being at the barber shop and places like that, and they bring up these conversations, and they end up talking about HIV or it ends up coming up somewhere. People start talking in a negative way it makes you feel like the elephant in the room because I’m living with this every day, but I can’t just bust out and tell you all that I’m living with this, and I’m beating this. I’m fighting. I’m undetectable, my numbers look good, and I don’t have to do nothing but wake up and take these two pills every day.
As he describes, being in the presence of such stigmatizing behaviors and language is difficult not only because it makes him feel like “the elephant in the room,” but also because he does not feel it is safe to disclose his status and try to educate others. He goes on to describe hearing negative things about HIV from total strangers and from people who are close to him: It could be anywhere, in conversation with somebody at the bus stop, hearing other people on the bus in conversation, or just in the grocery store, anywhere people tend to have these conversations, even around my homegirls and stuff like that. I got one homegirl she was mad with her baby daddy, and she made a joke “I wish I could find a guy who got that shit because I would pay him to bite him.” I was like, “girl what?”
How do you respond to stuff like that?
Chance: You don’t, you get quiet because I don’t want to say too much. . . . I get quiet and just back the hell away from the situation.
Chance illustrates not only what it feels like for him to hear these negative things as a person living with HIV, but also the difficulty in challenging stigma. For him, it feels safer to just be quiet, than to speak up.
Similarly, when I asked Eugene (45; 17) how he responds to hearing negative comments about HIV, he responded, . . . when I hear people say that stuff? I don’t react, because that’s their life. I mean, I don’t react at all. I don’t feel the need or see the notion to react, because it’s. . . I mean, you’re going to run into that. You’re going to have those problems, so I just don’t react.
And Bryce (18; 4 months) described that “I don’t entertain it. I just go on with business. It’s not my conversation. Just step away.” When I asked him what he believed would happen if he were to speak up to challenge the negative things he heard, he responded, “Rumors, that’s how they spread. Rumors from ‘Oh, he’s the sweetest thing, now he got it.’” For these men, silence is an act of self-protection and a strategy of resilience. Challenging stigma comes with social risks that they have determined to be too high of a cost. In this way, stigma self-perpetuates, as one stigma producing social process—rumor and stigmatizing language—activates another process—silence.
Gossip
In contrast to narratives of silence, men described social interactions in which discussions of HIV in their community were largely centered around rumor and gossip. When I asked what they hear being said about HIV in the community, nearly every participant described negative talk about people living with HIV. Noah (27; 8) described previously thinking HIV was “a disgusting disease.” When I asked where he learned to think about HIV in that way, he said “It was just a group of friends talking. . . They were saying like, ‘Oh he got this shit,’ and all that.” These euphemisms were prominent in men’s descriptions of the kinds of gossip they hear about HIV. David (43; 14) explained that he hears a mix of positive and negative: I have a neighbor, she says things like “My son has HIV and he’s doing great and it doesn’t really affect him.” But there’s other people around who are like “Oh, that one from around the corner, he got that stuff. He got HIV, stay away from him.”
Being seen seeking care was often the genesis of gossip about one’s status. As Louis (57; 14) described, Some people they hear, “Oh, I heard that he was at the clinic the other day, so that mean he has HIV.” And that doesn’t mean that they have HIV, but you’re being frowned upon because somebody said it . . .
And, as Brian (35; 10) explained, a lot of people don’t want everybody to know, because people like to talk, like to expose. People just be afraid to open up. The first time going to the doctor, to the clinic, I was shocked when I walked into that room. Because I’m like, damn, I don’t want nobody to know that I have HIV and most places like on [that] street, when you go on that block, they know that certain area, that’s for HIV people. Once you hit that block and everybody look or somebody at the urgent care side, they looking like, “Damn, I didn’t know that person had such and such.”
A number of men described ways that an HIV-positive status could be weaponized in the community. For example, Jamar (32; 9) described that it is common for people to be accepting and supportive until you “piss them off tomorrow and then now all your business out on the street.” Steven (28; 6 months) and his partner are both living with HIV. However, he had not yet disclosed his diagnosis to his family. When they were having a conflict, his partner disclosed his status to his family to get back at him. “I didn’t tell my family that I had HIV. [My partner] did. He told them out of anger and stuff like that because he was mad.” Michael (48; 16) described trusting people he wanted to date, who might then disclose his status to others: I find somebody that I really like. You’re investing time into getting to know them. You getting all these feelings. You getting worked up because you find somebody and you really like them. You know what I mean, when you finally disclose, then they’re the ones that’s going to go out there. They’re going to spread your business, too. It’s not just to one person. It’s going to be a whole group of people.
Furthermore, Keith (29; 6) explained how he believes one’s social status shifts once they are diagnosed: When a person is diagnosed, they become . . . to the person from the outside looking in, they become the person that’s spreading it. No one knows what goes on behind closed doors but when it comes out, and the people here have this thing about exposing people.
Here, Keith points to the ways that blame has been placed on people living with HIV, positioning them as villains and a threat to others. This is a common trope that has existed since the early days of the epidemic, and that has been perpetuated through laws and policies, social interaction, and by media coverage of HIV criminal cases (as I discuss later in the “Results” section). As illustrated above by Chance, Eugene, and Bryce, men often “just get quiet” when they hear gossip about HIV to avoid becoming a target. Thus, this culture of rumor and gossip furthers the production of HIV stigma and reinforces more silence around HIV.
Witnessing and Experiencing Acts of Marginalization
At the individual level, one of the most salient themes in men’s stigma narratives was that many of them had developed their understanding of what HIV meant in their families and communities by witnessing and experiencing acts of marginalization. These experiences reinforced the belief that people with HIV were bad and risky to be around, both in terms of their potential to transmit the virus and the likely damage that will be done to one’s own social standing. Steven’s (28; 6 months) mother had been diagnosed with HIV years before his own diagnosis. He described the way his siblings treated her after she was diagnosed: . . . my sisters, they kind of kept they distance and they were treating her kind of bad. Like my other sister actually didn’t want my mom inside the house. [My sister] used to sleep in the garage and stuff like that. . . it’s like they were treating her awful, you know what I’m saying? I’m saying like “damn. . . like she got this and this is the way they treating her.” Like, “damn, if I get this, it make me feel like y’all gonna treat me like that!”
For Steven, watching the way his siblings treated his mom was instructive—it taught him that having HIV was bad and resulted in being alienated by others, even those closest to you.
Similarly, Marcus (27; 4) described witnessing the poor treatment of people living with HIV: “I’ve seen where people be actually telling people, ‘Get away from me. You got that shit’, like, just crazy stuff.” When I asked him whether he thought he would be treated that way if people knew he was living with HIV, he responded, “Oh, I know I would if I said it.” Nathan (30; 1) described watching his family members interact with people they believed to have HIV: The people in my family, they kind of treat HIV like COVID-19. . . I have watched them, how they have treated other people that they thought they had HIV. They was very cautious. . . they cleaned up behind those people at all times. People would use the bathroom, they was right behind the people cleaning it. Shit like that. I watched this stuff happen. In my head, it’s like, I don’t want to go through that.
Importantly, as Marcus and Nathan state clearly, watching people be treated this way left a clear impression and the expectation that people would treat them similarly.
Rodney (56; 33) was diagnosed in 1987 and had witnessed the worst days of the epidemic. During the early 1980s, he was caring for his partner who had been diagnosed with AIDS: He had cancer, whatever, you could tell. You know a person that has AIDS, you know that type. [My aunt] wanted me to come over and mow grass, but I was taking care of him at the time. I said, “Well you’ll have to come lay in the bed,” because he was almost dead. [My cousin] said, “Oh no [Rodney], I don’t want nobody. . . He can’t lay in the bed!” That was one experience that kind of tripped me out. Or people thinking you can catch it from laying in a bed or something. People was like that back then. . . it just stayed that way with me. I just, and I think that’s how it all really began. People were scared of you.
The way people were treated back then was etched into his memory and, at the time of his interview, in 2019, he still feared being labeled with “gay and AIDS.” He believes that he will be treated a certain way and held tightly to those stigmatizing ideas. He was so committed to secrecy around his status that he hoped not have a prolonged illness at the end of life, so that no one would ever know. “I just hope I drop dead.”
Others described experiencing these marginalizing social interactions when the negative treatment was directed at them personally. Shawn (42; 14) described how his friends reacted and how it affected him long term: My trust level is off. I don’t trust a lot of people. I’m not going to come to a lot of people. I’m not going to trust a lot of people with my business because of what I experienced dealing with HIV. . . my classmates at school knew I had HIV, and they got scared of me. People wouldn’t talk to me. That affected me. So, I learned not to let people get too close. But I also learned that people will let you down as well. . . [they were] scared to touch me, and thought I was going to infect them, and stuff like that.
Several men had experienced family members treating them as though they feared them, including not wanting them in the house, or bleaching household items they used (Campbell 2021b). As Michael (48; 16) explained, “You had your own families that were serving you with plastic plates and stuff like that.” When I asked if he was describing his own family, he responded, “Right. They were buying certain products to make sure and clean the toilet. It was bad.”
In some cases, the marginalization of HIV was performed by celebrating the idea of being HIV negative. For example, when Darius (23; 4) was diagnosed, he was worried about telling his friends because he previously had another sexually transmitted infection that required several treatments. When he told his friends about that diagnosis and treatment, their responses were “Well you know, thank God it’s not ‘that.’” He described it as “heartbreaking . . . when I actually had to come back and tell them, ‘Well, it is.’” Walter (29; 6) had been increasingly ill with no confirmed cause. His coworkers and boss were aware that he had been having health problems. He finally received an HIV diagnosis at his doctor’s office in the middle of his workday. When he returned, I clocked back in, went to my boss and she was like, “Okay, so it’s not HIV?” was the first thing she said. And I was like, no, it’s not. And so she gave me like a high five and a hug and everything and I was just like, oh my God, how am I supposed to tell these people? I don’t know why there was so much riding on it not being HIV.
Walter’s and Darius’ experiences illustrate how the messages conveyed by celebrating not having HIV are similar to those conveyed by explicitly negative statements about HIV.
Community (Mis)Education
At the level of community interactions, word-of-mouth communications were key in disseminating erroneous and stigmatizing information about HIV. This form of (mis)education, particularly given the lack of formal education (which I discuss in the next section), shapes a belief that one should avoid people with HIV and, if diagnosed with HIV, one should not expect to live much longer. James (27; 8) described that he had learned “nothing about how [HIV] works; more that it was bad. It was something that you don’t want to do, you don’t want to have. It was like a death sentence. It was like, it was over with.” Similarly, Trey (37; 16) said he believed his life was over when he was diagnosed, “because that’s just the stigma with AIDS. You get AIDS, you die. That’s all I knew. That’s all I ever was told.” The narrative that HIV = death had a particularly negative impact on Sam (32; 7): From what I had known about it, AIDS was deadly, it was the worst thing to ever happen for anybody. There’s no cure for it. You get down, your immune system starts to shut down, your body starts to shut down and you just become a vegetable, and then you just die. . . I didn’t want any of my family members to see me like that. . . And then I didn’t want to have to go through the fact of people just knowing that I had it . . .
Sam had considered suicide immediately after receiving his diagnosis because he did not want to put his family through the horrible demise that he expected for himself.
When I asked Marcus (27; 4) where he got the idea that HIV was a death sentence, he replied, “my circle that I was hanging with. . . So that’s just how it was presented to me. ‘You going to die tomorrow if you got it.’” Some described other negative and inaccurate information. Eugene (45; 17) had been told, “You know you can catch that by them touching on you.” Walter’s only knowledge about HIV was from word of mouth. “If someone spits on you, you can get it from them. It’s so much bad information out there and people believe it because it’s just word of mouth or they heard it from somebody they trust.”
Nathan’s (30; 1) understanding of what it meant to have HIV was based on having heard that people with HIV are “sick, they dying, stuff like that at first. . . they say they dying, some people, they call them dead. ‘They dead’, whatever, stuff like that.” After receiving his own HIV diagnosis, all those thoughts shaped his outlook on his future. These inaccurate perceptions did not simply exist in the minds of people in their communities. They were being actively transmitted. Importantly, the spreading of such ideas contributes to the silence and gossip that was so prevalent in men’s narratives, illustrating how interactions at various levels intersect, furthering the HIV-stigma process.
This (mis)education is, in large part, driven by stigma and, at the same time, stigma stands as a barrier to HIV education. From Steven’s (28; 6 months) perspective, HIV stigma “detours them away from actually wanting to know more about it . . .” Louis (57; 14) explained, I think there’s still a lot of ignorance here in Baton Rouge, when it comes down to HIV. And sometimes, I just feel like people, they just have a one-track mind and that’s what they learned and what they first heard about HIV is what they will retain. Then they don’t broaden their knowledge scientifically or none of that. They just feel, “Oh well. I know such and such died of HIV.” So they think everybody who has it is going to die of HIV.
Chance (34; 2) wished “people get [the stigma] out their heads. If they were more educated about it, but you can’t make someone learn something they don’t want to learn. Some people just got stuck in their ways.”
As Louis and Chance both illustrate, the stigmatizing ideas that people learned earlier in the epidemic were cemented in the minds of some people who are unwilling to learn about HIV or believe it isn’t relevant to their lives. As Walter (29; 6) explained, I feel like a lot of people don’t do a lot of research on their own about it because they just feel like, “Oh, it’s never going to happen to me.” Or this and that, and then they just hold onto those negative stereotypes without having done any research to dispel them or to put themselves in situations where they can speak to people with it and know that this is not something like, it’s not a death sentence . . .
Social Institutions: Public Education and Criminal Justice
Sex education
Reflecting the embeddedness of structural HIV stigma and heteronormativity within state and local sex education policies, most men described learning very little about HIV and nothing about nonheterosexual sex. These policies reflect deeply embedded stigma that creates an environment in which gay and bisexual men are not equipped with the information they need to protect themselves. Jamar (32; 9) pointed specifically to the impact of the lack of comprehensive sex education: There was never a thought. [HIV] was never brought up in school, which they have sex education, but I don’t think they. . . yeah, they got into STDs, but they never got into HIV or AIDS or anything like that. Never. Now that I look back, I’m like, we were doomed from day one.
Charles (26; 6) explained that he had a similar experience: They didn’t, actually come to think, like they didn’t touch on it. The base that they touched on was how to put on a condom and pregnancy. That’s all they touched on, was pregnancy. It’s like they skipped out over all the diseases and just with like pregnancy and condoms and how to put on the condom. That’s about all the Sex Ed that was given.
As Jamar and Charles explain, the topic of HIV was left unaddressed.
Several men described the lack of information they received that was relevant to nonheterosexual behavior, and the ways HIV stigma and homophobia intersected in these classes. For example, when I asked Carl (39; 20) if he learned anything about gay sexuality and HIV, he responded, “Oh, not at all, no. That was not even a subject. It just pretty much talked about the basic STDs and how you make a baby and how the sperm and egg, all that kind of stuff, the basics.” Similarly, Brian (35; 10) explained, I know when I was in high school and in the health book they had HIV. . . they had AIDS and all that in the health book, but this is stuff that wasn’t talked about. I can only talk about going to [high school] in my club when we was required to pass health. This is areas that didn’t get discussed . . . Everything from been getting a baby, parenthood, all that was being discussed. In the health book that got skipped over, HIV always got skipped over. Even sex, you’ll do how to make a baby, but after that it was no consequences behind it. That got skipped over. . . I felt like if I had known about that in high school or if my parents would have sit down and really talked to me and said that we accept the fact that you’re gay. I felt like if I had knew that more about it, then I could have been more protected for myself.
For Sam (32; 7), the intersection of HIV stigma and homophobia were more explicit: I remember being educated in school, and just in high school they taught sex education for a little while. [The teacher] was telling us about AIDS, syphilis, gonorrhea and all that stuff. And he was like, “AIDS is deadly.” He thought it was a gay person disease. He said gay people brought it over here. I felt like it was a bad thing.
As Carl, Brian, and Sam illustrate, there was either a complete lack of education about HIV or negative information about HIV, and a focus on conception, but no information relevant to their sexuality. Furthermore, similar to Jamar, Brian highlights how this lack of information left him unprepared to protect himself.
HIV criminal law
Just over half of men had ever heard of HIV nondisclosure criminal laws. However, in most cases, their knowledge of those criminal statutes was limited. Several participants learned about HIV disclosure criminal laws from news reports of criminal cases. “I think it was an article or something about it, where somebody had got intent to distribute AIDS, or something like that. And I read an article about it” (Trey, 37; 16). Similarly, David (43; 14) also said he knew about HIV criminal laws “from the news, I found that out.” And Eugene (45; 17) had mostly seen a lot of news and things like that. People also had it and do not tell somebody, and end up sleeping with them or whatever, whatnot, and giving it to them. I’ve actually seen people go to jail for actually giving it to them, giving it to other people.
Importantly, several media analyses have shown that reporting on these cases serves to further stigmatize HIV and people living with HIV, and to regularly employ homophobic and racialized tropes when discussing defendants (Campbell et al. 2022; Persson and Newman 2008; Shevory 2004). In each of these quotes from Trey, David, and Eugene, there is stigmatizing language used in describing these laws (e.g. “distribute AIDS”; “giving it to them”). Furthermore, David went on to describe what he believed these laws meant for him. “. . . it means whether I feel comfortable about it or not that I need to make sure I [disclose] for legal reasons.”
Noah (27; 8) first heard about nondisclosure laws when someone from the public health department called him, after his diagnosis, to inquire about partners who may need to be notified. I asked him what he thought when he heard about them and he simply responded, “scary! I mean they shouldn’t take people to jail for not telling people that they have HIV.” Nearly all men who were aware of these laws agreed with Noah that criminal punishment was unfair to people living with HIV. Keith’s (29; 6) concerns about the effects of these laws highlight their stigmatizing and oppressive nature: . . . for the person who was raped, for the person who was born with [HIV]—so I’m born into a world where I have to tell everybody this or I go to jail, but I was born with this. I didn’t contract this, I didn’t go out there and just get it. I was born with this. I was born into a world . . . I can’t love anyone just to love them. I always have this hanging over my head that I can go to jail if I don’t say this.
His concern about having your status “hanging over your head” illustrates the way that people living with HIV are burdened by these laws and fear what could happen to them if they do not meet the societal and legal expectations.
In addition, the existence of these criminal disclosure laws can also be used as a weapon against people living with HIV. A number of men described ways the laws have been used against themselves or others. During his interview, Rodney (56; 33) was cautious in discussing his status and his experience of these laws. He believes that he has been targeted and set up to be arrested under criminal nondisclosure statutes: Probably about three years ago. I met somebody online and it was a very, very, very sexual conversation about what we was going to do to each other. . . I went to the hotel to meet him. . . Then he said he was over across by the bank [in the same parking lot]. “I’m just standing by the dumpster over there. Come meet me over there.” So I pulled in there and I saw a person standing back there all dark color. I said something ain’t right about this, so I hurried up and backed out. And then I saw some other people. . . So I feel it’s some type of set up. Then after that I got phone calls that I was going to get arrested and all kinds of stuff. That I was passing AIDS around and just all kinds. They had my license plate number and called me and said I was going to get arrested and all kinds of stuff. It was a set up.
Importantly, Rodney had never met this man before and did not end up meeting him, as he describes. Nonetheless, these phone calls and threats terrified him and caused him to stay home and not meet new people for several months.
Shawn (42; 14) explained that he knew other people who have been threatened with these laws: I’ve had people around me, or friends that I know that have been threatened about not disclosing status and things like that. So, yeah, I’ve heard that. . . Maybe that’s part of some of the reason why I don’t tell certain people that I’m not close to about me being positive. . . because not everyone has good intentions. I’ve learned over the years, not a lot have good intentions when you tell them certain things. That’s why I’m not very open to everyone about me being positive. . . I think [the laws are] silly. I think it’s more a deterrent to keep people from being more open about it.
Shawn’s concerns were realized for one of Carl’s (39; 20) friends: I have friend of mine who was in a contentious relationship with someone. He told his partner his status and everything. And they broke up, and he lied and said he didn’t tell him. And he went to jail for that for a little while.
Others lived with the fear that someone could use their status against them because these laws exist. The potential to be arrested or the invocation of nondisclosure laws as a threat decreases the likelihood of disclosure and more open discussion around HIV. Walter (29; 6) explained how he believed nondisclosure laws were a barrier to communication about HIV: I feel like HIV criminalization pushes us so far back in reference to how much we’ve grown and how much we’ve sacrificed to get to the point where we can actually have conversations about it, openly without ramifications. I do feel like the criminalization does add a fear factor back to things, especially for those that are positive because in the court of law as I see it, it’s our word versus their word. And the law system has tended to take their side more often than not. And proving that you have disclosed is a very difficult thing to do in court and to show that you did not have the intent to transmit the virus to anyone else is again very subjective. . . I get the intent of the law to make people disclose ’cuz I would hate for someone to knowingly transmit the virus to somebody else on purpose. . . But I don’t know if the laws they have in place protect those people who are positive and protect those that are not. Right now, I feel like it’s just protecting those people who are not positive.
Discussion
In this analysis, I examined the social relations through which HIV stigma is produced and reproduced. Men described that HIV is a topic largely left unspoken in their communities and families and, when it is discussed, it is normally in the form of gossip using euphemistic terms for HIV. Misinformation about HIV is spread through community-level interactions, while the state further produces HIV stigma by criminalizing nondisclosure and restricting formal education about sexuality and HIV in the classroom. To date, our understanding of HIV stigma has described these social interactions as manifestations of stigma and have focused on cognitive measures of HIV stigma’s impact on individuals (Earnshaw et al. 2013). The narratives of men in this study suggest that these are not simply how HIV stigma is manifested. Instead, they are critical aspects of the ongoing and ever-changing social process of HIV stigma production and reproduction. Framing HIV stigma in this way shifts the focus from perceived, enacted, and anticipated stigma as stigma mechanisms, which only allow for individual-level intervention, to the interactions and processes at multiple levels of the social world. Thus, my findings push beyond the individual level to include the levels of social institutions, social interactions, and community, and highlight the ways in which the social processes at these various levels work together to produce and reproduce HIV stigma.
Public health studies have provided much evidence of the negative effects of HIV stigma on mental health, retention in HIV care and clinical outcomes, disclosure, and sexual behavior (e.g., Balaji et al. 2017; Bird et al. 2017; Eaton et al. 2018; Overstreet et al. 2013; Quinn et al. 2017). However, a sociological analysis allows for an emphasis on the ways that the realities of the social world come from “thoughts and actions, and is maintained as real by these” (P. L. Berger and Luckmann 1966:20). The grounded theory resulting from this analysis provides a model of HIV stigma that centers actions, interactions, and structures from which HIV stigma originates and through which it is reproduced. Importantly, each component of this stigma process interacts with, and is somewhat dependent on the others. For example, community (mis)education processes persists, in part, because of the lack of formal education about HIV and sexuality in the East Baton Rouge school system (East Baton Rouge Parish School Board 2019; SIECUS 2018). Importantly, in some cases, sex education included negative and stigmatizing ideas about HIV. That lack of education about HIV contributes to silence around HIV (Gwadz et al. 2018), as does the fear of HIV criminalization. These findings are in line with a number of other authors who describe the ways that HIV criminal laws perpetuate HIV stigma (Burris and Cameron 2008; Cameron 2009; Federman, Holmes, and Tremblay 2011; Hoppe 2017; Jürgens et al. 2009; Kane and Mason 2001). Furthermore, the acts of marginalization that men witnessed or experienced result from community (mis)education, silence, and gossip, and the lessons learned from these experiences sustain as there no formal HIV and sex education to counter the beliefs that undergird this mistreatment.
This study has limitations worth noting. First, findings should be seen as representing a convenience sample of black gay and bisexual men in the Deep South region of the United States. Thus, the theory of an HIV-stigma process is one that emerged from that particular context and would likely differ in samples of different demographic groups in different geographic regions. Additional research needs to be conducted to explore the stigma process in other social contexts. Second, HIV status was self-reported and not confirmed through testing or documentation.
Important implications emerge from these findings. First, framing HIV stigma as an ongoing process embedded in social interactions and institutions provides new spaces in which to intervene. Efforts to reduce stigma that focus exclusively on individual beliefs and attitudes are critical, although they do not address interconnected social processes. It is not necessary for individual people to engage in stigmatizing behavior toward people living with HIV to be participants in the process of stigmatizing HIV. “We are all enmeshed in a complex web of problematic relationships that grant our mirror images full human subjectivity while stereotyping and objectifying those most different from ourselves” (Collins, 2016; 36). Indeed, as these findings illustrate, some members of men’s families and social networks actively participated in marginalizing behaviors. However, as important are others who simply remain quiet or encourage silence, but see people living with HIV as “other” and likely fail to recognize their role in the HIV-stigma process.
Second, the role of institutions is largely absent from HIV-stigma research and interventions. Men’s narratives point to not only stigmatizing behavior by individual people but highlight the critical role of HIV criminal laws and sex education policies. Intervening at the structural level is crucial to disrupting processes such as community (mis)education and the silence and fear that men describe because of draconian HIV nondisclosure statutes. Finally, it is worth restating that HIV stigma is not a “static attitude” but a “constantly changing (and often resisted) social process” (R. G. Parker and Aggleton 2003:14). Thus, quantitative measures, thus far, have failed to capture the reality that HIV stigma means something different in each place and to each person depending on the social context, and that it is continuously being produced. Stigma cannot be “reduced” or “ended” until the social processes through which it is reproduced are interrupted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Mental Health grant number 5P30MH062246.