
Abstract
We characterize the way human immunodeficiency virus (HIV) stigma hinders HIV conversations and testing. Using grounded theory principles, we analyzed in-depth interviews of the experiences of select Philippine key populations (groups with high HIV burden) and their families: 19 men who have sex with men (KPM), 16 transgender women (KPW), and 16 parents of KPM/W. Results show how KPM/W protect the state of being respected by others (management of social standing), a task they engage in by strategically modulating behavior in different life domains, including when considering HIV conversations and testing. Our results specify the management of social standing as an object being threatened by stigma and as a process making KPM/W behavior susceptible to the influence of HIV stigma, even for KPM/W who may not possess the mark of positive serostatus. This raises questions about the theorizing of stigma, which traditionally has focused on the susceptibility of marked but not unmarked individuals.
Human immunodeficiency virus (HIV) serostatus awareness enables individuals to access treatment, which can minimize acquired immunodeficiency syndrome (AIDS)-related mortality and onward viral transmission (UNAIDS 2021; World Health Organization 2020). Two behaviors for individuals that are critical for increasing serostatus awareness are conversing with someone about HIV and getting tested for HIV. Conversing with someone about HIV (referred to hereafter as “HIV talk”) is associated with HIV testing (Hendriksen et al. 2009). HIV testing allows individuals to become aware of their serostatus (World Health Organization 2020). One barrier to HIV talk and testing is HIV stigma (Smith, Rossetto, and Peterson 2008; World Health Organization 2020), which refers to the social devaluation of HIV-positive serostatus (Earnshaw and Chaudoir 2009).
Research has shown a negative association between HIV stigma and a specific kind of HIV talk—disclosure of seropositive status (Smith et al. 2008). Seropositive status disclosure can enhance treatment adherence, likely by improving relational functioning and facilitating social support (Dessie et al. 2019; Katz et al. 2013). Seropositive status disclosure can only be accomplished by persons living with HIV (PLHIV) and not by individuals with unknown serostatus, who are the individuals in need of getting an HIV test. Few studies, however, investigate the impact of HIV stigma on HIV talk that is not about seropositive status disclosure (for systematic search strategy, screening, and results, see Appendix in the online version of the article), such as when individuals who do not know their serostatus seek HIV testing information. HIV talk is linked with increased HIV testing, possibly by shifting individuals’ perceptions of acceptability (Hendriksen et al. 2009).
Research on the link between HIV stigma and HIV testing has consistently shown an association between higher stigma and lower testing (Ajayi et al. 2020; Haider et al. 2020). A preponderance of this research, however, is cross-sectional (e.g., Ajayi et al. 2020; Haider et al. 2020). Evidence of a causal relationship between higher stigma and lower testing is more persuasive when obtained through an investigative methodology that captures changes in testing rates as stigma levels change over time (Marini and Singer 1988). Although there are intervention studies that measure changes in either HIV testing or HIV stigma levels, we have not found any that measured both HIV testing and HIV stigma in the same study. For example, some intervention studies measured HIV testing behavior but not levels of HIV stigma (Martínez-Donate et al. 2010; Washington, Applewhite, and Glenn 2017), and other studies measured changes in HIV stigma levels over time but not changes to HIV testing behavior (Apinundecha et al. 2007; Wu et al. 2008). Furthermore, establishing a causal relationship between stigma and testing involves the specification of a mechanism (Marini and Singer 1988). Yet even qualitative studies that reported HIV stigma as a barrier to HIV testing have not provided a theoretical accounting of the mechanisms that underlie their association (e.g., Okal et al. 2020). As such, specifying the process by which HIV stigma impacted individuals’ HIV testing behavior remains a research gap.
This study posits that the process by which HIV stigma impacted individuals’ HIV talk and testing behavior can be elucidated by comparing incidents in which individuals engaged in HIV talk and testing with incidents in which individuals considered but did not engage in HIV talk and testing. We use open-ended interviews to elicit accounts about HIV talk and testing behavior from two groups in the Philippines with a high HIV burden (key populations): men who have sex with men (KPM) and transgender women (KPW). To understand their social contexts, we also conduct interviews with parents of KPM/W. We use grounded theory (Glaser and Strauss 1999) principles to analyze the accounts, with the goal of specifying a process through which HIV stigma impacted HIV talk and testing.
Prior scholarship on stigma has emphasized the devaluation of individuals who possess or are perceived to possess stigmatized attributes (Earnshaw and Chaudoir 2009; Goffman 1963). Our work, however, shows how HIV stigma influences the HIV talk and testing behavior of KPM/W as individuals whose serostatus may be unknown to themselves and others. Our work identifies a process through which this occurs—the management of social standing—and shows how KPM/W actively manage social standing through their HIV talk and testing behavior.
Background
Stigma Frameworks
Goffman (1963:3) defined stigma as an “attribute that is deeply discrediting” (i.e., mark) such that a person with that mark is reduced “from a whole and usual person to a tainted, discounted one.” Goffman’s (1963) conceptualization of stigma delineated between those who possessed a discrediting attribute (marked) and those who did not (unmarked). He specified how social interactions generate expectations of what ought to be in that situation (i.e., demands); a person can then, by virtue of an actual or perceived attribute, fall short of those demands (Goffman 1963). This framing specifies the stigmatization of individuals who possess or are believed to possess a mark. This framing also specifies the lack of stigmatization of individuals whose possession of a mark is known to the individual but not known to others: Individuals whose marks are concealable means that they have not yet failed to conform to the demands of a situation (Goffman 1963). Nonetheless, Goffman’s (1963) framing does not address the potential stigmatization of persons whose mark possession is unknown, such as individuals considering an HIV test because they do not know their serostatus.
Scholars after Goffman parsed his stigma definition into two important components, typically focusing scholarship on one or the other: the possession of a mark, on the one hand, and the social processes of devaluing the person labeled as possessing a mark, on the other (Link and Phelan 2001; Parker and Aggleton 2003). The HIV stigma framework (HSF) is an example of a stigma conceptualization that is contingent on mark possession (Earnshaw and Chaudoir 2009). It conceptualizes distinct stigma mechanisms engaged in or experienced by individuals, depending on their possession of the mark of HIV-positive serostatus. Specifically, the HSF specifies seronegative individuals as the ones who engage in HIV-related prejudice (negative emotions), stereotypes (negative cognitions), and discrimination (negative behavior); the HSF specifies seropositive individuals as the ones impacted by prejudice and discrimination (enacted stigma), expecting prejudice and discrimination in future interactions (anticipated stigma), and endorsing negative beliefs about HIV (internalized stigma). These stigma mechanisms delineated based on serostatus have provided a conceptual basis for measuring and assessing the perpetration of stigma by seronegative individuals and the behavior and outcomes of seropositive individuals as targets of stigma (Earnshaw et al. 2013). However, the delineation of stigma mechanisms based on serostatus precludes the HSF from specifying stigma mechanisms for individuals whose serostatus is unknown, such as for individuals considering an HIV test and wanting to talk to someone to solicit more information. For example, the HSF categorizes negative beliefs about HIV in two ways: as “stereotypes” when endorsed by seronegative individuals and as “internalized stigma” when endorsed by seropositive individuals (Earnshaw and Chaudoir 2009:1162–63). Neither stigma mechanism is specified in relation to individuals whose serostatus is unknown, even when they endorse negative beliefs about HIV. Furthermore, the HSF specifies seropositive individuals as the targets of stigmatization but does not account for how seronegative individuals can also be stigmatized.
Link and Phelan (2001:363–75) articulate an alternative stigma framework that emphasizes social processes rather than mark possession. They specify stigma as several co-occurring processes, including “distinguishing and labeling differences,” “associating [such] differences with negative attributes,” and the “downward placement of a person in a status hierarchy.” None of these processes require the individual perpetrating them to either possess or not possess a mark. As an illustration, anyone—irrespective of serostatus—can engage in distinguishing and labeling differences. This approach takes the perpetration of stigma out of the exclusive remit of the unmarked, recognizing that even those who possess a mark can stigmatize themselves or stigmatize others possessing the same mark. The processes specified by Link and Phelan (2001) also do not require the individual being targeted by those processes to either possess or not possess a mark. This means that stigmatization occurs when a person is treated as different rather than when a person possesses a devalued attribute. Their conceptualization’s indifference as to whether the target of stigma actually possesses a mark enables the examination of stigma in relation to individuals who do not know if they possess a mark. Link and Phelan’s (2001:363–75) framework specifies processes from the initiation of stigmatization (“labeling differences”) until stigmatization is produced and maintained (“downward placement of a person in a status hierarchy”). Their framework, however, does not specify mechanisms for the way individuals then respond to the produced stigmatization. In theorizing stigma’s impact on HIV talk and testing, it is not the production of stigma that needs further characterization but the way that stigma is attended to, dealt with, and translated by affected individuals into behavior modulations in the areas of HIV talk and testing.
A framework that does characterize the way individuals deal with and modulate behavior in response to stigma is “stigma management,” defined as the “shifting or manipulation of internal and external processes in order to address stigma in a given situation or setting” (Fielden, Chapman, and Cadell 2011:270). Research using this framework has shown how PLHIV act strategically to deal with stigma, including by being silent and by selectively disclosing their serostatus (Fielden et al. 2011; Poindexter and Shippy 2010). Research using this framework has also specified the elements of the decision-making process when PLHIV consider disclosing their serostatus; these elements include considering when and to whom one might disclose and the positive and negative consequences of disclosing (Sandelowski, Lambe, and Barroso 2004). Notwithstanding, we found no studies that used the stigma management framework to specify the impact of HIV stigma on individuals’ HIV talk and testing behavior.
In sum, previous scholarship has specified the stigma processes implicating marked individuals as targets and unmarked individuals as perpetrators of stigma (Earnshaw and Chaudoir 2009; Goffman 1963), the production of stigma (Link and Phelan 2001), and the way PLHIV strategically use behavior to deal with stigmatization (e.g., Poindexter and Shippy 2010). Prior scholarship has not yet specified the way that HIV-related stigmatization is managed by individuals with unknown or negative serostatus. Such a framework is needed to characterize the impact of HIV stigma on HIV talk and testing behavior, which can be accomplished by anyone, irrespective of serostatus. The aim of our study is thus to characterize the way HIV stigma influences the behaviors of talking about and getting tested for HIV and in so doing, develop a stigma framework that can account for the way individuals, irrespective of serostatus, deal with being targets of stigmatization.
To this end, we wish to address an issue of terminology. We have shown how in some frameworks, the term “stigma” is used to refer to devaluation that targets persons who possess a mark (Earnshaw and Chaudoir 2009; Goffman 1963). This scholarship shows the usefulness of understanding “stigma” in relation to the devaluation of individuals who may not possess a mark. We note that from this point forward, our use of HIV “stigma” is broadly construed to include processes of HIV-related devaluation that can implicate any individual as targets, irrespective of their serostatus.
Data and Methods
Sampling
Site
We conducted semistructured interviews with Philippine KPM/W and parents of KPM/W, who were recruited through the social networks of local HIV advocacy organizations and researchers’ personal networks. We selected the Philippines as the site because of its potential relevance to the phenomenon. The Philippines has a concentrated HIV epidemic that disproportionately burdens several key populations, including KPM and KPW (Republic of the Philippines Department of Health 2021a). Fewer than 40% of KPM/W correctly answer five basic questions on HIV symptoms and transmission (Republic of the Philippines Department of Health 2021a). The low rate of HIV knowledge suggests that the Philippines is a site that can benefit from improving individuals’ ability to solicit information. Furthermore, only 68% of Philippine PLHIV have been diagnosed (Republic of the Philippines Department of Health 2021b) despite KPM/W awareness of testing services and the availability of free HIV testing (“Republic Act 8504” n.d.; Republic of the Philippines Department of Health 2021a). These suggest that factors not related to testing awareness and cost, such as the potential role of HIV stigma, are playing a heightened role in impeding testing behavior. These make the Philippines ideal for exploring the operation of HIV stigma.
Key population participants
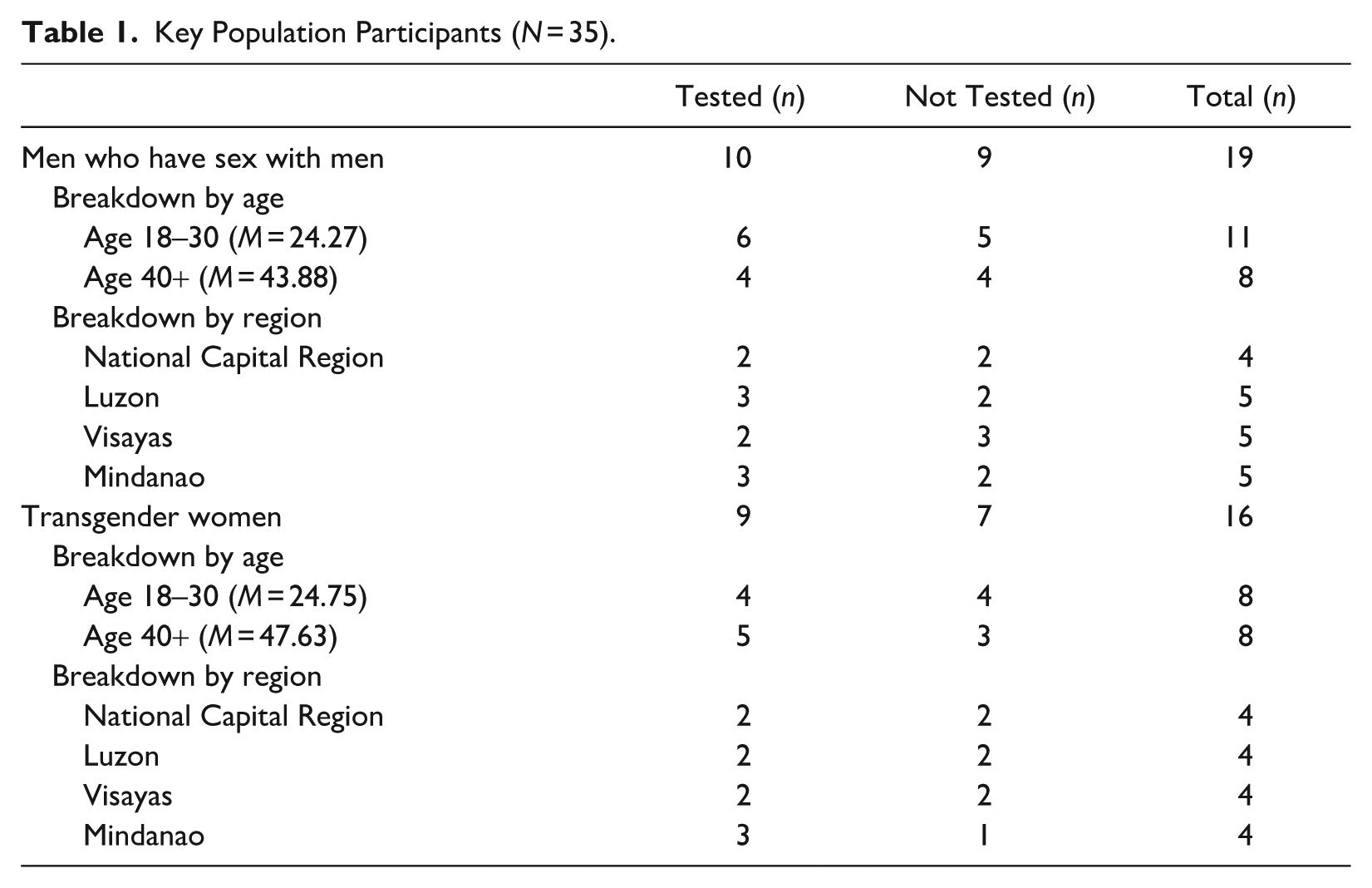
We conducted interviews with 19 KPM and 16 KPW participants, purposively recruited to be representative of the Philippine KPM/W population according to three characteristics: HIV testing status, age cohort, and macrogeographic region. We recruited based on HIV testing status because the meaning-making of those who have and have not received an HIV test may be distinct. For example, even if stigma was in operation for both groups, only those who have undergone an HIV test can hold meanings produced from their own personal experiences of getting tested. We also recruited based on age cohort because of the way national policy changes could have impacted HIV testing practices. For example, although the first cases of HIV were detected in the Philippines in the 1980s, it was not until 1998 that Philippine law prohibited compulsory testing (“Republic Act 8504” n.d; Republic of the Philippines Department of Health 2021b). Finally, we recruited participants from different macrogeographic regions because these are inhabited by distinct cultural groups. It is not the goal of this article to discuss these cultural differences, only to acknowledge that they exist and that sampling representativeness necessitated the recruitment of adequate samples from each macrogeographic region. We thus purposively recruited participants from the National Capital Region (NCR) and the Philippines’s three macrogeographic regions: Luzon (north), Visayas (central), and Mindanao (south). In sum, we purposively recruited KPM and KPW participants based on HIV testing status (tested, never been tested), age cohort (18–30, 40 years or older), and macrogeographic region (NCR, Luzon, Visayas, and Mindanao). For a summary of key population participant characteristics, see Table 1.
Key Population Participants (N = 35).
Parent participants
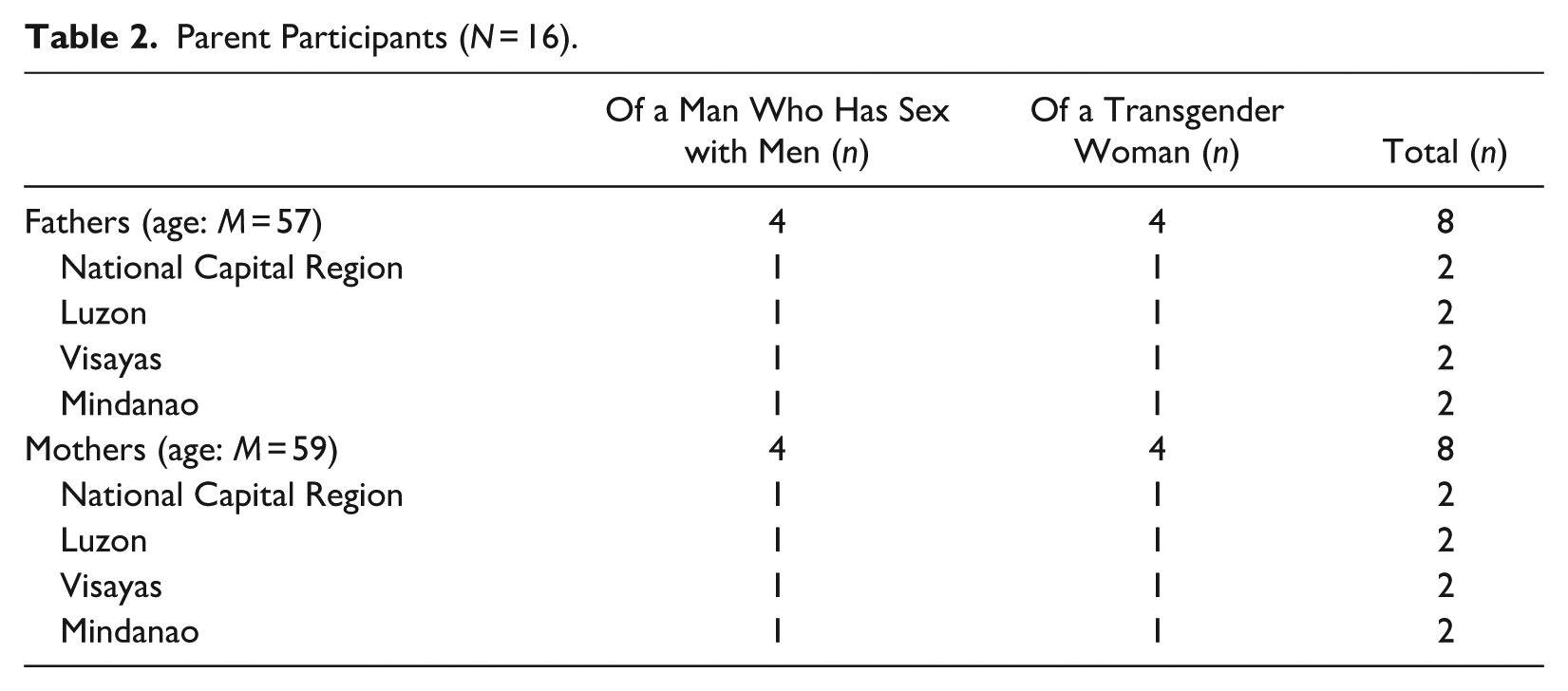
We also conducted semistructured interviews with 16 parents of KPM/W because we aimed to situate HIV stigma as a phenomenon operating within the social contexts of KPM/W. To ensure representativeness, we recruited parent participants according to gendered parental role (father, mother), child’s identity (KPM, KPW), and macrogeographic region (NCR, Luzon, Visayas, Mindanao). For a summary of parent participant characteristics, see Table 2. Recruited parents were not necessarily the parents of the KPM/W participants in this study. Although recruitment was open to adoptive parents, all recruited parent participants were nonadoptive parents of a KPM/W child.
Parent Participants (N = 16).
Sampling sufficiency
We stopped sampling when sufficient numbers of participants representing each characteristic were recruited. We defined sampling sufficiency as the recruitment of at least two people with each relevant characteristic (e.g., two KPW from Visayas who have never been tested, two fathers from Mindanao). Having a minimum of two participants with each characteristic ensured that if any generated concepts were later analyzed in relation to a characteristic, they would not be attributed to a characteristic based on the account of only one individual with that characteristic. Sampling was not determined by theoretical saturation.
Addressing recruitment bias
It is possible that contacts of HIV advocacy organizations are more likely than the KPM/W population at large to have familiarity with HIV-related discourses and testing practices. However, we did not aim to investigate familiarity with these discourses and practices per se but to explore how HIV stigma might influence a person’s deployment of such discourses (HIV talk) and engagement in such practices (HIV testing). As such, even participants who have greater familiarity with these discourses and practices are not disqualified from being able to provide valid data on the research questions by reason of their familiarity. Moreover, the study purposively recruited both participants that have been tested and those that have not. If testing is an indicator of greater engagement in HIV discourses and practices, the recruitment of a nearly equal sample size of participants who have not engaged in HIV testing should mitigate potential engagement-related sampling bias, even if they were recruited through HIV advocacy organizations.
Interview
Development
We developed an interview protocol after pilot testing and iteratively refined it throughout data collection so that later interviews would elicit data on topics identified as relevant in earlier interviews. We trained interviewers on using the interview protocol. To minimize potential data elicitation bias due to interviewer differences, we also trained interviewers regarding relevant concepts (HIV, sexual orientation, and gender identity), interview skills, and the way questions were to be and not to be phrased. The principal investigator debriefed interviewers after their first interviews to identify gaps and enhance future data elicitation.
Process
We conducted interviews between August and October 2021. Interviews were approximately two hours and conducted in the following languages: Cebuano, English, Hiligaynon, and Tagalog. Interviews were conducted via telephone or mobile apps, such as Zoom and Facebook Messenger. To protect confidentiality, only the audio of each interview was recorded. The recording of one parent interview was damaged; although field notes from that interview supported preliminary analysis, its data were not used to support the final analysis.
Questions
We asked KPM/W participants to recount instances when they talked about and got tested for HIV and instances when they considered but did not talk about or get tested for HIV. To ensure analytic rigor, we included control topics to provide comparative data. For comparative data on HIV talk, we asked participants to recount instances of talking about and not talking about an important topic. We did not specify a topic of importance because we recognized that different participants could consider different topics important. Our criterion for the validity of a topic as a comparator was not the content of the topic itself (e.g., talking about career vs. talking about their partner) but the fact that the topic was considered important by the participant. For comparative data on HIV testing, we asked participants to recount instances of wanting and not wanting to get a diabetes test. We selected diabetes as the comparator because of the characteristics of the diabetes test (the need to draw blood, as with an HIV test) and the characteristics of diabetes itself (being a noninfectious condition, unlike with HIV). This ensured that any differences in participant meanings to the two tests would not be a function of the test procedure (i.e., the need or lack of need to draw blood) but a function of the underlying condition itself.
We asked parent participants to recount instances when they talked to their KPM/W child about HIV and instances when they considered but did not talk to their KPM/W child about HIV. We also asked them about their willingness to talk to other people about their KPM/W child getting an HIV test. For comparative data, we asked parents about their willingness to talk to their KPM/W child about an important topic and their willingness to talk to other people about their KPM/W child getting a diabetes test.
Analysis
Process
We recorded the audio of interviews, which were transcribed by independent transcribers and validated by interviewers. Interviewers collaboratively developed a coding frame during joint meetings. Interviewers then used this coding frame to independently code transcripts, which were subsequently validated by the principal investigator. The principal investigator used these codes to independently develop the explanatory framework. All interviewers jointly refined and validated the explanatory framework in a process that involved testing it on data extracts for fit and exceptions. The principal investigator formally conducted a negative case analysis that was subsequently validated by one analyst.
Coding
Using validated transcripts, we identified participant accounts about talking and not talking about HIV, getting and not getting tested for HIV, talking and not talking about an important topic, and getting and not getting a diabetes test. During initial coding, we thematically labeled (coded) these accounts using in vivo descriptions and sorted them by directionality (i.e., facilitated or hindered talk or testing). We then compared these codes across the data set to identify codes that represented more than one account (patterns). We identified patterns of explanation (e.g., why participants thought they did not get an HIV test) and patterns of antecedents and sequelae (e.g., what happened after talking about HIV). We then compared patterns across behavioral domains (e.g., Does an explanation provided in relation to getting an HIV test apply as an explanation for getting a diabetes test?); we used this process to discern the breadth of a pattern. We also compared accounts in which a pattern was applicable to accounts in which that pattern was not applicable (e.g., Why does X explain the testing behavior of Participant 1 but not of Participant 2?); we used this process to discern the limits of a pattern. We then formulated the breadth and limits of a pattern’s applicability as principles—the set of conditions when a pattern was in operation and the set of conditions when it was not in operation. These principles together constituted the explanatory framework to characterize the relationship of HIV stigma to talking about and getting tested for HIV.
We restricted our analysis to codes that were substantiated by accounts from participants with different characteristics (e.g., a code that applied to a young person and a mature person). This ensured that no code was a function of the characteristics of any one participant, including their self-presentational characteristics during the interview. We also did not seek to differentiate the experiences of one group of participants against other groups (e.g., stigma experiences of the mature vs. stigma experiences of the young). We only sought principles that applied to accounts of participants with different characteristics. The applicability of a code to participants with different characteristics increases the validity of the analysis (Glaser and Strauss 1999). We further restricted our analysis to codes that were supported by data provided by at least two interviewers. This ensured that codes were unlikely to be artifacts of the way any one interviewer elicited data. Finally, we only included analytic principles that applied to HIV talk and testing and to other life domains. The applicability of analytic principles in different contexts enhances validity (Glaser and Strauss 1999). For this reason, this article begins with a discussion of the operation of these analytic principles in life domains outside of HIV talk and testing.
We aimed to explore the meaning-making processes engaged in by KPM/W and their parents in relation to HIV talk and testing rather than how particular characteristics might objectively influence these processes. For this reason, we did not determine a priori that we would use participant characteristic categories (HIV testing status, age, macrogeographic region, parental role, child identity) as lenses to analyze the data, even though we used these characteristics as a recruitment basis to ensure that the recruited sample could represent characteristics of the general KPM/W and parent populations. For the same reason, we did not a priori determine that we would use economic inequality and intersecting stigmas as lenses to analyze the data, even though we were aware of prior scholarship that demonstrated their influence on HIV stigma (Lim et al. 2013; Turan et al. 2019).
Presentation
We present data extracts that illustrate codes to enable readers to assess validity and fit. We numbered these data extracts and reference these extract numbers in relation to the analytic points to which they apply. This format allows an account to be cited repeatedly to support different parts of the analysis without being chopped up to support nonadjacent parts of the analytic story. Data extracts presented in the analysis were translated into English and validated through a process involving two speakers of the language.
Researchers
Twelve researchers with professional or educational backgrounds in psychology conducted the interviews and analysis. We represent transgender, cisgender, lesbian, gay, bisexual, and heterosexual identities and persons who are and are not living with HIV. We assigned interviewers to participants only on the basis of familiarity with the language spoken by the participant.
Ethical Approval
The study received ethical approval from the Institutional Review Board (Protocol 2021-029-NPCALAGUAS-MSBHIV) of Holy Angel University.
Results
In Their Social Context: “You Will Amount to Nothing”
KPM/W can grow up in a social context in which they were devalued for being lesbian, gay, bisexual, transgender (LGBT). For example, some parents regarded their LGBT child as unacceptable (Extracts 1, 2) and contemplated violence against their child because their child was LGBT (Extract 3). Some parents directly communicated their lack of acceptance to their LGBT child (Extracts 1, 2), and others withheld doing so (Extract 3). KPM/W were keenly aware of the lack of acceptance, including how they were looked down on and expected to “amount to nothing” (Extract 4). This devaluation can result in KPM/W feeling emotional pain (Extract 4) and dealing with the threat of violence (Extracts 3, 5).
(Extract 1) Mother of KPM: I did not want to accept [my son was gay] . . . when [he] comes home for the weekend and acts in a way that isn’t good, I tell him off. Can you not be like that? Things like that. (Extract 2) Interviewer: Was there a time that you talked [with your LGBT child] about something important or serious? Father of KPM: Yes, I told them, I wish you had been a man. (Extract 3) Interviewer: [What was] your reaction when you found out [your child was LGBT]? Father of KPW: I didn’t ask about [it] anymore. I might beat them up. (Extract 4) Young KPM: When [they] say “LGBT” before, it meant that that’s all you are, that you will amount to nothing. . . . So I said to myself, that can’t be. Firstly, it’s painful to think that they look down on you as a person. . . . So I became diligent in studying, I strived and strived to finish so that at least the way they see us [sic, end of sentence]. . . . I think I succeeded somewhat. I was able to earn respect because until now, I don’t really experience being bullied. (Extract 5) Mature KPW: That’s why this needs to be done—even if we are like this, let’s do some good, right? . . . We are already like this, we need to do good around us, to our fellow humans, so that they don’t discriminate against us, so they don’t bully us.
Behavior as Strategic: “Show That Even if You’re LGBT”
KPM/W felt the need to do something about being a devalued person. For example, a KPM found it necessary to strive in their education (Extract 4), and a KPW felt the need to do good in the community (Extract 5) and to behave in a particular way in public (Extract 6). These things that KPM/W felt they needed to do can be effortful (Extract 4) but are construed as compulsory to compensate for being a devalued person (Extracts 5 and 6). Succeeding in education, doing good, and behaving in public are actions in different life domains, yet participants construed them as sharing a common goal—to earn respect. Participants specified “earning respect” as what was accomplished by their actions (Extract 4) and as what KPM/W actions should aim to accomplish (Extract 6). Participants also specified “avoiding disgrace” or “avoiding the loss of being respected” as goals their actions can accomplish. For example, a KPM discussed how not wearing makeup can be a strategy to avoid disgrace (Extract 7), and a parent stated that dressing formally was a strategy for avoiding being disrespected (Extract 8). A KPW construed the action of getting an enema before sex as a way to avoid demerits in the way she would be regarded by her sex partner (Extract 9).
(Extract 6) Mature KPW: The LGBTQ that I guide, I teach them #1, you want to be respected? You need to be respectable. If you want to be transwomen you need to behave like a girl . . . don’t be vulgar. (Extract 7) Mature KPM: My mom told me back then, I accept you as whatever you are, if you’re LGBT, as long as you don’t bring us disgrace. Interviewer: Did your mom say what she meant by the things that would bring disgrace? Mature KPM: For example, dressing like a woman, wearing makeup. (Extract 8) Mother of KPW: I told [my child] . . . study well so that you can show that even if you’re LGBT, you have achieved something . . . even though you are LGBT, I hope you would be respectable . . . you should be formal-looking, you shouldn’t be unpresentable or be in a way that people around you will disrespect or be rude to you. Isn’t it that the LGBT out there that aren’t formal, aren’t they the ones that get ridiculed or judged? . . . I really don’t want makeup, [be] really formal, as if they were men, like their LGBT is hidden. (Extract 9) Interviewer: Are there things you do to prepare yourself for sex? Young KPW: Yes . . . enema. Of course this is to avoid gossip . . . if you’re not clean then maybe your sex partner will make it an issue . . . to them it’s minus points. Interviewer: Do you think there are any risks, threats, or possible harms that can come from having sex? Young KPW: When there’s no condom, all the more [when] you don’t know the person you had sex with, that’s where that [risk] is . . . [when you don’t know] whether they’re safe or maybe they already have [an] illness, then you had sex with them. . . . That’s why it’s better to have condom [sic] and to get clean [do an enema] before and after sex.
Social Standing: “The Way They See Us”
“Earning respect” and “avoiding disgrace” both refer to one’s symbolic status—the state of being respected or disgraced. This status is social in that it occurs in the gaze of others. Thus, being respected and avoiding disgrace pertain to social standing. The construct of social standing finds explicit textual support in “the way they see us,” invoked in relation to earning respect (Extract 4). Additional evidence for the way participants orient toward social standing can be found in participant accounts of being concerned about gossip, which they specified in relation to sexual relations (Extract 9), being taken to the hospital (Extract 10), and getting a blood sugar test (Extract 11). In these accounts, participants treated being the subject of gossip as a distinct problem, independent of other problems in those life domains. For example, the KPW who used “getting an enema” as a strategy for avoiding gossip also used “getting an enema” as a strategy for avoiding the risk of sexually transmitted disease, construing these as distinct purposes (Extract 9). In addition, participants treated gossip as its own kind of consequence (“even more pitiful when gossiped about,” Extract 10; “I am the one affected,” Extract 11). The salience of social standing as a task may in part be because of its perceived necessity (“we need to”; (Extract 5; cf. Extracts 4 and 8) as a strategy against violence and ridicule. For example, a KPM construed “earning respect” as the reason he was not bullied (Extract 4; cf. Extract 5), and a parent construed “being respectable” and “avoiding disrespect” as critical for avoiding ridicule (Extract 8).
Participants construed social standing as a singular object that can be managed through accomplishments and failures in different domains. For example, a parent told her child to “study well so that you can show that even if you’re LGBT, you have achieved something” (Extract 8). That parent did not construe a social standing that was specific to being LGBT and a separate social standing that was specific to educational accomplishments. Rather, that parent construed her child’s perceived failure in the area of being LGBT and success in the area of education—together—as acting on the singular object of her child’s social standing. This construal is similar to that of a KPW, who saw “do[ing] good” as a way to compensate for being LGBT (“we are already like this, we need to do good around us”; Extract 5). These suggest that the impact on social standing in any one life domain (e.g., being LGBT, succeeding in school), whether positive or negative, impacted the social standing of the individual as a whole. Our data set shows that participants have managed social standing in the domains of education (Extracts 4 and 8), public and community life (Extracts 5–8), intimate relations (Extract 9), and health (Extract 11).
(Extract 10) Interviewer: Was there a time when a person became the subject of gossip because they got tested . . . or went to the doctor? Father of KPM: Yes, but don’t think it was HIV. Someone was rushed to the hospital because they were throwing up blood . . . that person is already pitiful, [they’ll be] even more pitiful when gossiped about. (Extract 11) Young KPW: The ones I wouldn’t want to find out? My friends especially, and neighbors of ours those gossipers. . . . It would be scary . . . they might spread it . . . it’s just a blood sugar test, [but what they say] might end up [as] various diseases. Maybe [that] I’m positive for COVID, positive for this . . . it’s hard because isn’t it that [when things] get passed around, that people won’t understand what really happened to you? . . . It would be ok if they were the ones being affected [by their gossiping], but no, I am [the one affected].
Applicability to HIV Talk: “She Will Read between the Lines”
Participants also managed social standing in the domain of HIV talk. Participants discussed that bringing up the topic of HIV in a conversation could elicit negative inferences for the interlocutor about the person speaking (speaker), including inferences that the speaker has had sex (Extract 12) and that the speaker had HIV (Extracts 13 and 14). Participants specified the elicitation of these inferences in relation to soliciting information about HIV itself and HIV testing (Extracts 13 and 14). Another participant discussed how bringing up the topic of HIV in conversation can risk diminishing the social standing of their interlocutors because doing so can signify that the people listening had HIV (Extract 15). To protect social standing, participants actively avoided talking about HIV, even when they wanted to acquire more information about it (Extracts 13 and 14).
(Extract 12) Interviewer: What do you feel your mom would think of you if you talked with her about HIV? Young KPW: She would probably think [I brought up] the topic because I had sex . . . I tell her things like that, she will read between the lines. (Extract 13) Interviewer: Was there a time that you wanted to talk to someone about HIV testing, but . . . it didn’t push through? Young KPW: No . . . if I wanted to know something, especially about HIV, we can watch YouTube, things like that, about HIV testing, what are the symptoms . . . if I ask other people about HIV and so on, they might think that I’m positive, so I’m embarrassed to look for someone to talk to about these things. (Extract 14) Interviewer: Was there a time that you wanted to talk about HIV screening with someone but you didn’t? Mature KPW: Yes . . . I wanted to get an HIV exam but . . . I was afraid to talk to anyone about it because maybe they’ll think that I am sick with HIV. (Extract 15) Interviewer: [What] will happen if you talk about HIV? Mature KPW: That will likely be a big issue . . . if it’s discussed, especially in [the] General Assembly or what, what they will immediately think is, “Why, has someone here gotten it?”
On the other hand, participants talked about HIV when doing so did not risk their own or their interlocutor’s social standing. For example, a KPW talked to her family about a seronegative test result, an action she construed as enhancing rather than diminishing her social standing (Extract 16). A KPW who got tested regularly (Extract 17) and a KPM who was known as an HIV advocate (Extract 18) expected to elicit no negative inferences when talking about HIV. A KPW recalled a graphic conversation with her mother about another person dying of AIDS (Extract 19). This suggests that graphicness was not itself an impediment for engaging in HIV talk. Because that conversation was about a third person, the conversation did not elicit any negative inferences about the speaker (KPW) or the interlocutor (her mother). In sum, participants did not talk about HIV when doing so risked their own or their interlocutor’s social standing, and participants talked about HIV when doing so did not risk social standing.
(Extract 16) Interviewer: What was the conversation like with your family members when you shared that you had gotten tested and the result was negative? Mature KPW: I think they had more respect when that happened. I’m not saying that if I had been positive that they would have no respect, but I think they respected me, that our child hadn’t lost [their] way, because negative. (Extract 17) Interviewer: [What] your family will think of you if ever you tell them you got tested for HIV? Mature KPW: Normal, because they know me . . . I’ve taken several tests, haven’t I? So there’s nothing new for them. (Extract 18) Interviewer: Are there times you talk about [HIV]? Young KPM: Yes, . . . In our workplace—well they know that I . . . volunteer [as] . . . an advocate. . . . There are times they ask me, there are times I tell them. Interviewer: [How about] in the group of friends you mentioned earlier? Young KPM: Yes. . . . Nothing out of the ordinary . . . their perspective of me is that, because I’m an advocate, I have more knowledge about HIV. (Extract 19) Interviewer: Have you ever talked to your mom about HIV? Young KPW: Yes, because our friend who died of AIDS . . . I showed the picture of my friend, the before and the after when [the friend] was extremely thin like bones. She was really shocked because she had also known my friend [as] healthy-looking. . . . She then asked for the reason. Then I said, having sex with just anybody, got AIDS, and suddenly after a month the [immune] system was consumed.
Applicability to HIV Testing: “It Would Be a Big Issue if People Found Out”
Participants further managed social standing by avoiding an HIV test (Extracts 23 and 24). KPM/W who have never had an HIV test reported negative inferences about people who have gotten tested, viewing the person who got tested as someone who engaged in risky behavior (Extracts 20 and 21), mistrusted their partner (Extract 20), or was experiencing HIV-related symptoms (Extracts 21 and 22). KPM/W specified these negative inferences in relation to the action of getting an HIV test and not specifically in relation to a seropositive test result (Extracts 20–23). Participants also reported concern about being the subject of gossip were they to get an HIV test (Extracts 22 and 23). These participants, when considering HIV testing, oriented toward potential threats to their social standing (how they might be talked about) rather than toward threats inherent in the HIV testing procedure itself (e.g., the threat of needle pain). In addition, one participant reported that the reason he did not get an HIV test was to protect the social standing of his family members (“it will be a shame for the family”; Extract 24). As with other areas of life (Extracts 4, 5, and 8), the loss of social standing in connection with HIV testing can have detrimental consequences, including social exclusion and the inability to find intimate partners (Extract 22).
(Extract 20) Interviewer: What do [you] think of . . . those who get an HIV test? Mature KPM: They’re probably exposed, or they’re too active in risky behavior, in sex. . . . Plus, they’re not sure about their partner. (Extract 21) Interviewer: [If] a friend of yours would get tested for HIV, what would it mean about them? Young KPW: I would maybe judge like, “Why is that? . . . So you feel symptoms? Or did you have sex with somebody like that?” (Extract 22) Mature KPW: It would be a big issue if [people] found out that you had . . . gotten an HIV test. Even if you just get a swab test, no one here will talk to you anymore. Interviewer: What does it mean if you are getting tested? Mature KPW: It means that you are really feeling something. . . . [News will] spread immediately . . . my neighbors stopped talking to me because I had gotten swabbed. The reaction will be the same, all the more for HIV. My goodness, I may never get guys again. (Extract 23) Interviewer: What were you thinking while [your friends were] talking [about their HIV test]? Young KPW: I just wondered if I would ever do that . . . the people conducting the test, I was thinking, “What if they gossip about me?” Whether it turns out positive or negative—if negative this and that, if positive they might tell other people, other people will find out. That’s what I’m afraid of. . . . So I said I’m not going to let myself go through that. (Extract 24) Interviewer: Was there a time you considered getting an HIV screening but didn’t go through with it? Mature KPM: Yes . . . because I had recently reconnected with my mother’s side of the family. . . . [If] you get a test and you’re positive . . . then it will be a shame for the family, and . . . I am the pride of my family.
Participants took an HIV test when doing so did not risk social standing. A KPW discussed how her negative HIV test signified to her family that she was on the right track in life, resulting in her being respected “more” (enhanced her social standing, Extract 16). A KPM discussed how his HIV test signified that he had not done something against his intimate partner (Extract 25). Both instances show participants’ awareness that getting an HIV test can, in some situations, elicit positive changes in the way a person is regarded by others. In sum, participants did not get tested for HIV when doing so risked diminishing social standing, and participants got tested for HIV when doing so did not diminish social standing.
(Extract 25) Young KPM: I was able to get tested before . . . I am not saying that I had done “something,” well maybe that’s what it meant, that I’m in some [way] trying to prove something to my partner that I do not have HIV.
Explanatory Framework: Managing Social Standing
Given these findings, KPM/W construed HIV talk and testing behavior as strategic for managing social standing (see Figure 1): They did not engage in HIV talk and testing when doing so risked diminishing social standing, and they engaged in HIV talk and testing when doing so did not diminish social standing. In this framework, HIV stigma was the risk of diminishing social standing when engaging in HIV talk or testing. HIV stigma affected HIV talk or testing when KPM/W avoided engaging in these to protect social standing, whether their own or that of another.
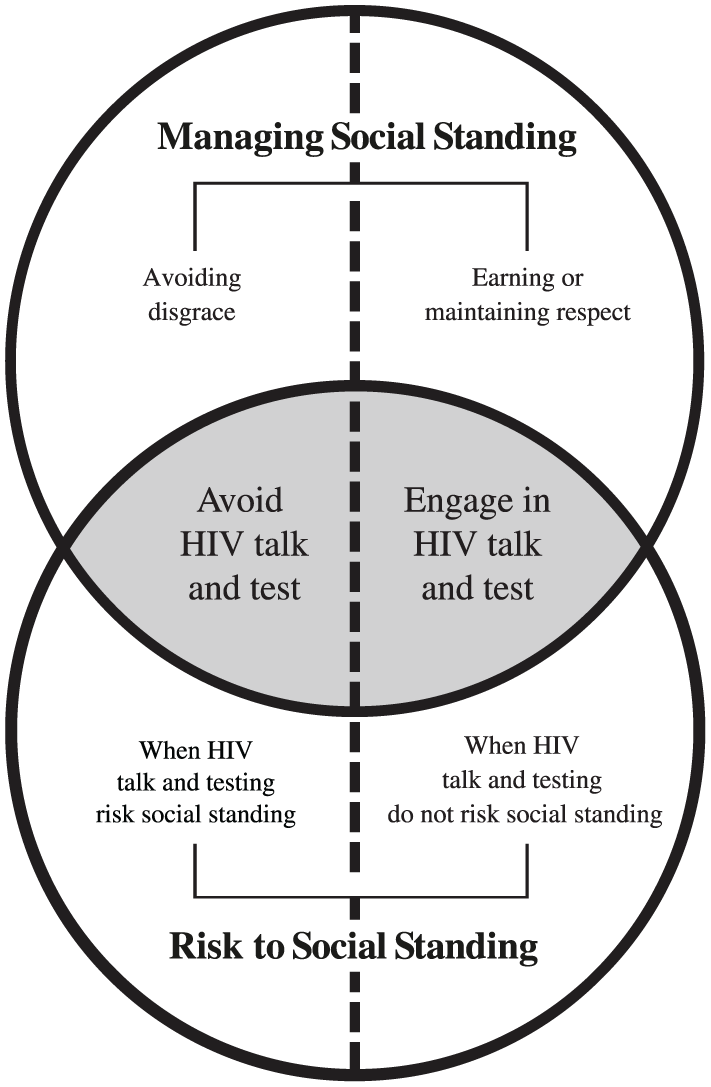
Analytic Model: The Management of Social Standing and Human Immunodeficiency Virus (HIV) Talk and Testing.
Delimitation
The management of social standing did not apply to every instance of HIV testing in this data set. In one exception, a KPM got an HIV test because he was experiencing serious symptoms (Extract 26). In another exception, a KPM got tested after learning that a past sexual partner had tested positive (Extract 27). In both exceptions, participants invoked a sense of urgency in relation to the threat that needed to be resolved, using the word “immediately” (Extracts 26 and 27). Participants in both exceptions also specified the threat of HIV in physiological terms, using the words “symptoms” (Extract 26) and “virus” (Extract 27). Although such terms may seem analytically unremarkable given that HIV is a virus, the specification of the threat as physiological becomes of analytic interest when compared with the incidents that support the explanatory framework. In the incidents that support the explanatory framework, participants oriented toward a threat, but the threat was to their symbolic status rather than to their body (Extracts 12–16 and 22–23). For example, a KPW considering an HIV test demonstrated awareness of the possibility of a seropositive test result (“whether it turns out positive or negative,” Extract 23) but did not specify this possibility as an issue of concern; she only specified being the subject of gossip as the threat to which she was oriented (Extract 23). Our analytic model and exceptional cases thus show that KPM/W can orient to the threat of HIV in two distinct ways—as a threat to their symbolic status and as a threat to their body. The management of social standing explains the HIV talk and testing behavior of KPM/W when they orient to HIV as a symbolic threat but not when they orient to HIV as a physiological threat requiring immediate action.
(Extract 26) Interviewer: What was the primary reason . . . you got tested? Young KPM: Because there were . . . symptoms I was feeling, so I was bleeding, blood from my anus. So like, it was not normal. . . . This seemed different. When I realized this I got tested immediately. (Extract 27) Young KPM: I had [a] very close friend who—something happened [between] us. And then after 6 months . . . he committed suicide . . . because he had the virus. That’s why I was worried for myself. So that’s why I immediately [had myself] checked.
Validity and generalizability
We demonstrate the validity of the management of social standing as an explanatory construct of behavior in three ways. First, our analysis showed how KPM/W managed social standing in areas of life outside of HIV talk and testing (Extracts 4–9, and 11). Second, we presented multiple accounts where KPM/W construed HIV talk and testing as managing social standing (Extracts 12–16, 20–25, and 28). Third, we now discuss how the family members of KPM/W also orient to social standing as a concern. Parents communicated to their children the need to modulate behavior in service of earning respect or avoiding disgrace; this need was specified in relation to the domains of getting an education (Extract 8) and manner of self-presentation (Extracts 7 and 8). Another parent, in their account about a neighbor taken to the hospital, oriented to gossip as a salient concern (Extract 10). Furthermore, a KPW living with HIV discussed how her family requested that she not disclose her serostatus to others to avoid potential demerits to the reputations of her family members (Extract 28). These show that the family members of KPM/W also oriented toward the management of social standing as a task in various life domains; this strengthens the case for its existence and salience as an explanatory construct of behavior.
(Extract 28) Interviewer: How about your family members?
Mature KPW: They support[ed] and assisted me. But with the condition that I shouldn’t tell anybody my status. . . . They probably just didn’t want to get dragged into ill-repute when someone hears about me.
Discussion
This study aimed to characterize the relationship of HIV stigma with HIV talk and testing behavior among KPM/W in the Philippines. We found that KPM/W were concerned with social standing and actively managed it by strategic action and inaction in several life domains. We also found that KPM/W construed HIV talk and testing behavior as able to diminish and avoid diminishing social standing, depending on the circumstances. Consequently, KPM/W did not engage in HIV talk and testing when doing so risked social standing and engaged in HIV talk and testing when doing so did not risk social standing. Our study thus shows that the management of social standing was a process through which HIV stigma hindered HIV talk and testing behavior among KPM/W. This principle applied to a broad range of accounts, with an exception for when participants perceived HIV as a physiological threat requiring immediate action.
This specification addresses a gap in stigma scholarship that we earlier identified—the lack of a theoretical framework that can account for the impact of stigma on HIV talk and testing, which can be accomplished by persons who may not possess the mark of positive serostatus. We earlier discussed how existing stigma frameworks have specified the processes that produce stigmatization (Link and Phelan 2001), the mechanisms by which marked individuals are targeted by stigmatization (Earnshaw and Chaudoir 2009), and the way that marked individuals act strategically to deal with being the targets of stigmatization (Poindexter and Shippy 2010). Yet no framework has specified the processes by which the behavior of persons who may not possess a stigmatized mark can also be implicated in stigmatization. The current study addresses this gap, specifying the way HIV stigma affects the HIV talk and testing behavior of Philippine KPM/W as persons who may not possess the mark of HIV-positive serostatus.
Theoretical Contributions
Stigmatization processes that entangle the unmarked
Our findings show that the management of social standing involves at least three underlying processes through which the behavior of KPM/W, as persons who may not possess the mark of seropositive status, become susceptible to the influence of stigmatization. First, KPM/W regarded the maintenance of being respected as important (Extracts 4 and 6). Second, in relation to this concern, KPM/W attended to potential threats to being respected, including the threat of having HIV as a mark applied to themselves or their associates (Extracts 9, 13, 14, 23, and 24). Third, in relation to these potential threats, KPM/W regarded their future talk (avoiding HIV talk) and behavior (avoiding HIV testing) as instrumental means for avoiding these threats (Extracts 13, 14, 23, and 24). Prior scholarship has shown that PLHIV, as individuals possessing marked status, also engage in these three processes. First, PLHIV regarded the maintenance of being respected as a concern when navigating disclosure (Bond 2010; Mackworth-Young, Bond, and Wringe 2020). Second, PLHIV anticipated or expected future stigmatization (Earnshaw and Chaudoir 2009). Third, PLHIV used talk and behavior as strategies to deal with these anticipated threats. For example, PLHIV managed with whom and how they talked about their serostatus as a strategy to protect against negative social and relational consequences (Poindexter and Shippy 2010). PLHIV also managed treatment-related behaviors (e.g., hiding pills) as a strategy for avoiding inadvertently revealing their serostatus to another (Katz et al. 2013).
Together, these show that persons who possessed (i.e., PLHIV) and persons who may not possess (e.g., KPM/W) the mark of HIV-positive serostatus engaged in similar processes—the concern for being respected, the anticipation of threats to being respected, and the construal of talk and behavior as means for dealing with such threats. The difference in mark possession (serostatus) did not lead them to differ in these processes. Given this, we suggest that it is not an individual’s possession of a mark but their engagement in these three processes that makes their behavior susceptible to the influence of stigmatization. This formulation expands the remit of the stigma construct beyond special, marked people to include even the behavior of ordinary, unmarked people. This conclusion finds support in Goffman’s classic conceptualization of stigma, wherein he contends that the marked and unmarked are “parts of the same complex, cuts from the same standard cloth” (Goffman 1963:130).
A novel object in the stigma phenomenon
The study provides a second contribution to the conceptualization of stigma by specifying a novel dimension of the phenomenon. Earlier stigma definitions have emphasized either the possession of a devalued attribute or the social processes of devaluing persons believed to possess a mark (Link and Phelan 2001; Parker and Aggleton 2003). Either way, earlier definitions frame the phenomenon “stigma” in relation to the problem or the object threatening affected persons. By contrast, “social standing” frames the phenomenon in relation to what affected persons care about or the object that is being threatened by stigma. To clarify using a health-related analogy, illness is problematic for people, but it is problematic against an intention or expectation to be well. The intention or expectation to be well may not always be in the foreground of people’s meaning-making, but illness as a problem is only intelligible against a backdrop where there is an intention or expectation to be well. Analogously, “social standing” specifies a valued object that makes stigma, as the threat of devaluation, intelligible as a problem.
In this view, the constructs of social standing and stigma are complementary. Social standing specifies that which stigma threatens. Stigma specifies a category of experience within the range of individuals’ possible experiences when managing social standing. Stigma is the experience when social standing is threatened or when its management has failed. Stigma is absent when the management of social standing is not being threatened. Stigma is mitigated or overcome when the management of social standing is experienced as having succeeded despite threat.
A novel characterization of stigma’s consequence
Given that “social standing” specifies an object being threatened by stigma, it provides a novel way to characterize the consequences of stigma. Previous stigma studies have elaborated on stigma’s consequences to mental and physical health (Rueda et al. 2016) and to sex- and other health-risk behavior (Gamarel et al. 2020; Hatzenbuehler et al. 2011). Previous studies have also identified stigma’s material and economic consequences, through mechanisms of resource allocation that are based on how persons are deemed worthy of social investment (Reidpath et al. 2005). Previous studies have further considered the impact of stigma on social support, which they define in relation to the size of support networks, the availability of persons within those networks to provide support, and the support one has actually received (Kalichman et al. 2003; Schwarzer, Dunkel-Schetter, and Kemeny 1994). Even though the way they conceptualize support can include dimensions of being understood and validated by others (Simoni et al. 2000), previous studies have conceptualized social support in relation to the material assistance or emotional succor one believes that they can receive or has actually received from persons in their network.
By contrast, “social standing” focuses the analysis of the consequences of stigma in relation to the valuation or devaluation of persons, independent of downstream consequences to health, economic, and behavioral outcomes. Social standing pertains to the way an individual is regarded by others, a status that is held of an individual by others. This is not to say that such status cannot unlock material or social assistance or that losses to material, health, and relationship outcomes are unimportant. Rather, social standing is both an instrumental good and a good that is valued in its own right. In the lived experience of KPM/W and their parents, stigma did not have to lead to loss in their number of relationships, or to loss in the support they could count on from their relationships, or to material and health disadvantage to be consequential. Even when the only thing that was lost because of stigma was their standing in the eyes of other people, this loss was devastating. It was to avoid this loss that KPM/W and their parents modified behavior in various domains in life, including in relation to HIV talk and testing. “Social standing” thus specifies a construct that characterizes the consequences of stigma in the relationship, even when the relationship was not itself lost (e.g., “We remain friends, but she respects me less”). This specification also finds support in Goffman’s (1963:3) conceptualization that stigma should be understood in “a language of relationships, not attributes.” The “management of social standing” is a step toward specifying such a language.
Appropriateness of the Term “Social Standing”
In selecting a term to represent the phenomenon at hand, we considered two terms: “social standing” and “face.” Prior scholarship used “social standing” to denote stature within a web of symbolic relations (Ho 1976); this usage captures the dimension of the phenomenon of being well or poorly regarded within a relationship, community, or wider society. Prior scholarship defined “face” as “the social anchoring of self in the gaze of others” (Qi 2011:280) and in relation to notions of adequacy or fitness for social life (Ho 1976). “Social standing” and “face” are related ideas, with both having consequences for social fitness. However, they are distinct in that “face” includes the dimension of an individual’s self-image, whereas “social standing” is the status accorded a person by how other people see that person (Qi 2011). In the current study, participants were not out to manage their self-image, but they were out to manage the way other people saw them. We thus deemed “social standing” more appropriate than “face” to represent the phenomenon at hand.
Limitations and Transferability
Our analysis only included factors that were invoked by participants in their meaning-making. This does not mean that factors that were not invoked had no bearing on the phenomenon, only that their influence on the phenomenon was outside the explicit meaning-making processes reported by participants. To this end, participants invoked their sexual orientation and gender identity in their accounts about HIV talk and testing; as such, we included these in the analysis. Participants did not invoke socioeconomic status (SES) in their accounts about HIV talk and testing; for example, even when a participant invoked “educational attainment” in their account, it was in the context of earning respect rather than improving economic prospects (Extract 4). As such, we did not consider SES in this analysis. The study also did not deliberately recruit or track participants based on SES markers. Previous research, however, has established that SES factors, including educational attainment, can be determinants of HIV stigma (Lim et al. 2013). It is therefore unclear if the analysis here represents KPM/W belonging to all or only some SES categories.
In addition, the study has no cross-cultural data and is unable to make direct claims about validity outside the Philippines. “Social standing” as an explanation of behavior has also not been well elaborated in the literature; however, the elaborated literature on its sister construct “face” may illuminate the degree of transferability of this analysis to other populations. “Face” is specifically relevant in the help-seeking attitudes of Filipino and Filipino American samples (David 2010; Tuliao et al. 2016). “Face” is also relevant to the help-seeking intentions and mental health outcomes of other Asian American, East Asian, and Emirati samples (Heath, Vogel, and Al-Darmaki 2016; Kim and Yon 2019; Leong, Kim, and Gupta 2011; Mak et al. 2015). This shows that the current analysis likely has applicability to global sites other than the Philippines. However, marked differences were found in the variances explained by “face” in the mental health service use of Asian American versus European American student samples (Gee et al. 2020). As such, the management of “face”—and by extension, social standing—may have different degrees of salience in different cultural groups as a factor in health-seeking behavior. Because “face” anchors the “self in the gaze of others” (Qi 2011:280), we surmise that the “management of social standing” will find greater explanatory salience in cultural groups where the self tends to be construed in consideration of the perspective of others. This phenomenon has been called “third-person” self-construal, in contrast with construing the self from one’s own “first-person” viewpoint (Cohen, Hoshino-Browne, and Leung 2007). Further cross-cultural research is needed to establish the degree to which the “management of social standing” can explain help-seeking behavior in other cultures, particularly in contexts with more salient first-person self-construal.
Conclusion
We applied grounded theory principles to the HIV talk and testing experiences of Philippine key populations. This elucidated a novel construct—the management of social standing, which specifies an ongoing, a priori concern to protect the state of being respected by others. This concern permeates the way everyday life is lived, with key populations avoiding perceived threats to social standing by acting strategically in several areas of life, including by modulating HIV talk and testing behavior. We specify stigma as a threat to the management of social standing, a process in which anyone, irrespective of mark status, can engage. This enables an analysis of HIV stigma’s influence on the behavior of key populations who may not possess the mark of HIV-positive serostatus. Although the construct needs examination in other cultural contexts, the management of social standing forwards an understanding of the consequences of stigmatization in “a language of relationships” (Goffman 1963:3) and places the concerns of key populations at the heart of understanding HIV stigma.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465251388639 – Supplemental material for The Management of Social Standing: Characterizing the Influence of HIV Stigma on HIV Talk and Testing Behavior in Philippine Key Populations Using a Grounded Theory Approach
Supplemental material, sj-docx-1-hsb-10.1177_00221465251388639 for The Management of Social Standing: Characterizing the Influence of HIV Stigma on HIV Talk and Testing Behavior in Philippine Key Populations Using a Grounded Theory Approach by Gideon Livingstone P. Bendicion, Augil Marie Q. Robles, Moniq Muyargas, Timoteo Balensoy, Bea Izabeaux T. Mendoza, Kiara Angela A. Sarmiento, ML Demaisip Farinas, Aron Harold G. Pamoso, Angelique Pearl Virtue P. Villasanta, Just Lynn D. Panaligan, Joseph Eleut G. Violago, Ver Reyes and Jonathan Fontilla in Journal of Health and Social Behavior
Footnotes
ORCID iDs
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data was gathered as part of the project May stigma ba? (Is there stigma?) A qualitative investigation into HIV stigma in the Philippine context 2021 (MSB project). The MSB project received funding from the Sustainability of Services for the Key Populations in Asia (SKPA program) managed by the Australian Federation of AIDS Organisations (AFAO); The Love Yourself, Inc. (TLY); and the Culture and Arts Managers of the Philippines Pag-ayo, Inc. (CAMP). The funding organizations played a role in participant recruitment, but had no role in the selection of study methodology, data elicitation, or data interpretation. A representative of AFAO (J. Fontilla) participated in project supervision and conceptualizing the study problem, but had no role in conceptualizing the method or interpreting the data. All other authors have no competing interests to declare.
Supplemental Material
The Appendix is available in the online version of the article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.