
Abstract
Co-occurring alcohol use disorder (AUD) and major depressive disorder (MDD) are common and complex conditions that significantly impact patient outcomes. The bidirectional relationship between alcohol use and depression complicates diagnosis and treatment, as alcohol exacerbates depressive symptoms and vice versa. Integrated treatment addressing both disorders simultaneously has shown better outcomes compared to sequential treatments. This article provides evidence-based clinical guidance for managing patients with co-occurring AUD and MDD, focusing on pharmacotherapy, psychotherapy and integrated care models. Pharmacologically, selective serotonin reuptake inhibitors and tricyclic antidepressants are commonly used to treat depression in individuals with AUD, while naltrexone and acamprosate are first-line medications for AUD. Combining antidepressants with AUD medications improves treatment efficacy. Psychotherapeutic interventions such as Cognitive-Behavioural Therapy (CBT) and Motivational Interviewing are essential components of treatment, focusing on addressing both alcohol use and depressive symptoms. Behavioural activation has also proven effective in treating depression while reducing alcohol cravings. Integrated care models, where both disorders are addressed simultaneously, yield the best outcomes and involve coordinated pharmacotherapy, psychotherapy and ongoing follow-up care. A case example of a 33-year-old woman with AUD and MDD highlights the success of an integrated treatment approach, where a combination of sertraline, naltrexone and CBT led to significant improvements in both mood and alcohol use. Clinicians are advised to differentiate between alcohol-induced depression and primary MDD, consider potential medication interactions, and incorporate ongoing psychotherapy and monitoring for optimal patient outcomes. This approach emphasizes the importance of addressing both conditions concurrently to achieve better long-term recovery outcomes for patients with co-occurring AUD and MDD.
Keywords
Introduction
Co-occurring alcohol use disorder (AUD) and major depressive disorder (MDD) are prevalent and complex conditions in clinical practice. 1 The bidirectional relationship between alcohol use and depression complicates diagnosis and treatment. Integrated care addressing both conditions is more effective than sequential treatment, yet often underutilized. This narrative review synthesizes current best evidence, including guideline-concordant care and recent meta-analyses, to provide clinician-oriented, practical guidance. It is not a systematic review or formal guideline, but offers an applied clinical framework based on existing literature.
Prevalence and Clinical Implications
The co-occurrence of AUD and MDD is common, with studies showing a high comorbidity rate. 2 Individuals with AUD are more likely to develop depression, and those with depression may engage in heavy drinking. 3 Their interaction increases the risk of suicide, relapse and poor physical health. Alcohol use can mask underlying MDD, delaying diagnosis and treatment.
Given this complexity, clinicians must also consider alcohol-induced depression (AID), which can present similarly to MDD but typically resolves with sustained abstinence. Early recognition of AID can help tailor appropriate treatment strategies.
Challenges in Diagnosis
Accurate diagnosis is crucial in treating individuals with both AUD and MDD. AID improves with alcohol abstinence, while MDD persists. 4 Differentiating between these requires a thorough assessment of the onset, course and relationship of depressive symptoms to alcohol use (Table 1). Persistent symptoms despite abstinence may indicate MDD.
Clinical Decision Guide: Distinguishing AID versus MDD and Pharmacologic Considerations.
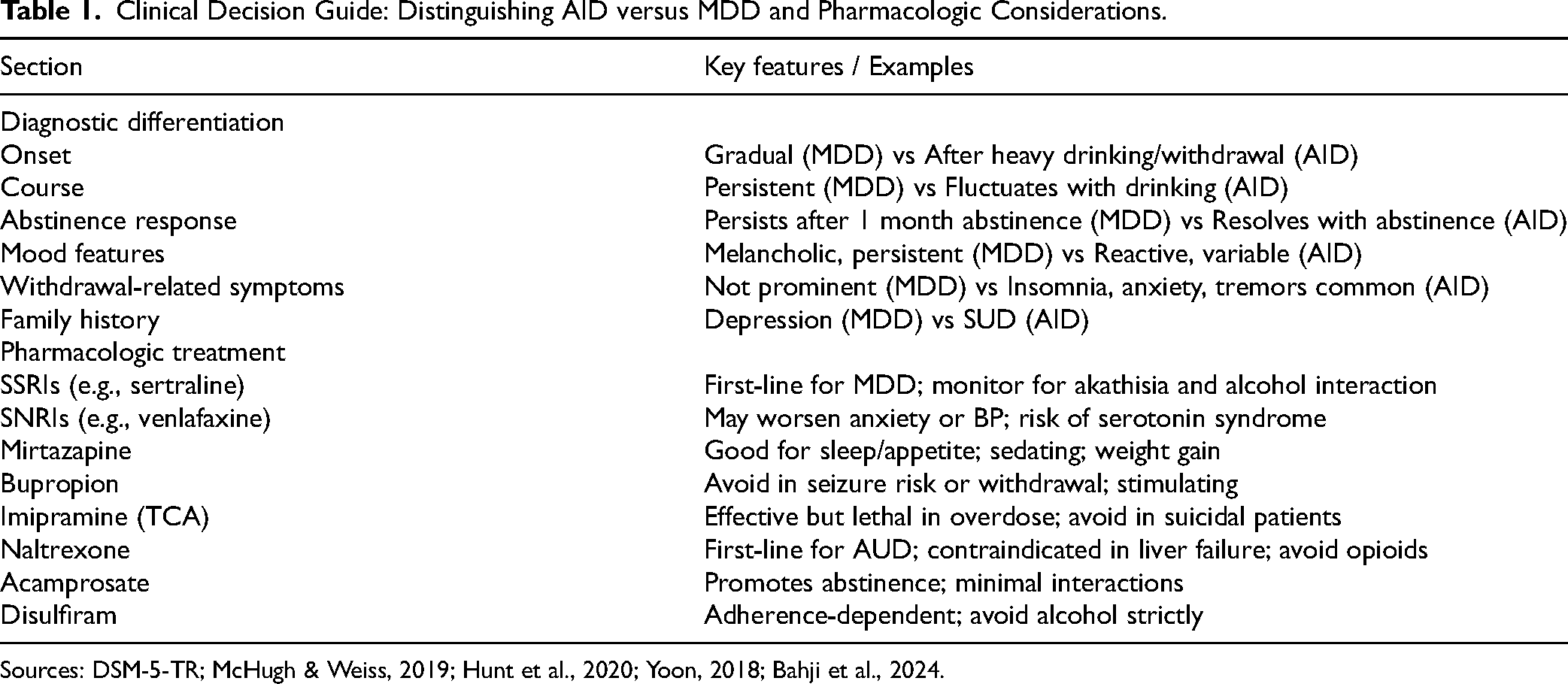
Sources: DSM-5-TR; McHugh & Weiss, 2019; Hunt et al., 2020; Yoon, 2018; Bahji et al., 2024.
Integrated Treatment Approaches
CBT focuses on identifying and modifying negative thought patterns and behaviours that contribute to both alcohol use and depression. CBT reduces cravings, improves coping and alleviates depression. MI helps increase a patient's motivation for change by exploring ambivalence towards treatment. MI is particularly helpful for individuals who may not be ready to fully engage in treatment or abstain from alcohol. Behavioural activation (BA) promotes meaningful activity to counter anhedonia and improve coping with alcohol cravings.
Case Example: Integrated Treatment Success
A 33-year-old woman with a history of AUD and MDD presented for assessment. Her history included childhood trauma and family history of SUD and MDD. She had previously tried naltrexone for AUD without success but found acamprosate helpful in reducing alcohol use. Her depression was managed with sertraline and buspirone. Despite successfully reducing her alcohol consumption with acamprosate, she struggled with low mood, anhedonia and social withdrawal. Given her persistent depressive symptoms, an integrated treatment approach was recommended, combining sertraline (antidepressant), naltrexone (AUD medication) and individual psychotherapy (CBT). After 12 weeks, the patient showed significant improvement in both mood and alcohol use. She reported fewer cravings, better sleep and sustained abstinence with regular therapy and social support. This case demonstrates the importance of an integrated treatment approach that targets both alcohol use and depressive symptoms. By addressing both conditions simultaneously, the patient achieved better outcomes than with a sequential treatment approach. Her depressive symptoms persisted well beyond a month of reduced alcohol use, were independent of withdrawal periods and included melancholic features (e.g., early morning awakening, psychomotor slowing), supporting a diagnosis of primary MDD rather than AID.
Clinical Pearl
The guidance in this article is derived from a narrative synthesis of high-quality studies, published clinical guidelines and recent systematic reviews or meta-analyses where available. Our aim is to equip clinicians with pragmatic tools for decision-making, recognizing the nuanced and often overlapping features of co-occurring AUD and MDD in real-world settings.
Footnotes
Declaration of Conflicting Interests
Dr M Danilewitz reports personal fees from advisory board/speaker fees/consultation/education grants from Eisai ltd, Otsuka, Janssen/Johnson & Johnson, Lundbeck, Winterlight Labs, Rapids health ltd, and the Ontario Brain Institute. He receives a stipend from the Canadian Psychiatric Association for administrative work and has received support for academic meeting attendance and presentations/rounds from Ontario Shores Centre for Mental Health Sciences, Southlake Health, the BC Psychiatric Association, Pearls for Primary Care, the Canadian Academy of Addiction Psychiatry, Western Canada Addiction Forum and the Canadian Psychiatric Association.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.