
Abstract
Objective
This study aims to determine the role of alcohol use disorder and other potential risk factors on persistence/recurrence of major depression in a Canadian population sample.
Methods
Data were drawn from the National Population Health Survey (1994/1995 to 2010/2011), a prospective epidemiologic survey of individuals 12 years and older, living in 10 Canadian provinces (N = 17,276). Participants were reinterviewed every 2 years for 9 cycles. This study population was a cohort of individuals who at baseline met the diagnosis of a major depressive episode (MDE) in the previous 12 months (n = 908). After the 6-year (cycle 4) and 16-year (cycle 9) follow-up period, 124 of 718 participants and 79 of 461 participants met the criteria for MDE, respectively. Persistence or recurrence of major depression was defined as meeting a diagnosis of MDE after 6 years and 16 years. Modified Poisson regression models were used to assess the role of alcohol dependence and other risk factors on the persistence/recurrence of major depression using Stata 14.
Results
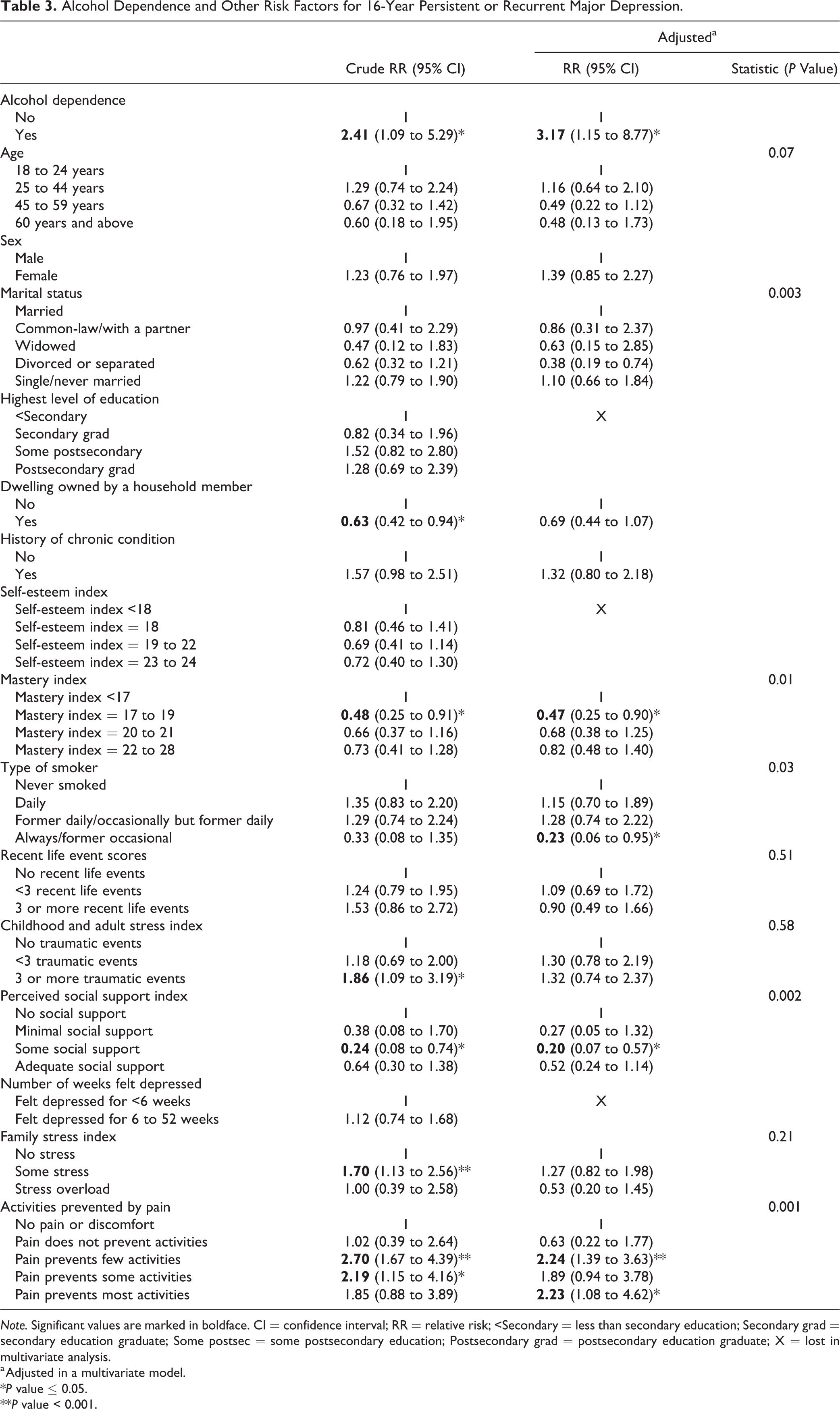
Alcohol use disorder was significantly correlated with a 6-year (odds ratio [OR]: 3.03; 95% confidence interval [CI], 1.68 to 5.48; P < .0001) and 16-year (OR, 3.17; 95% CI, 1.15 to 8.77, P = 0.003) persistence/recurrence of major depression. Other factors associated with the persistence/recurrence of major depression include female sex, childhood traumatic events, chronic pain restricting activities, daily smoking, and low self-esteem.
Conclusions
Comorbid alcohol use disorder was found to be a strong risk factor for the persistence or recurrence of major depression.
Introduction
Alcohol use disorder (AUD) and major depression are prevalent and frequently co-occur. 1 –4 Studies have shown that with depression, the risk of being addicted to alcohol is higher than in the general population, 1,5 and depression is more prevalent with alcohol dependence. 4,6 For example, the Collaborative Study on the Genetics of Alcoholism found a lifetime prevalence of major depressive disorder to be 42.2% among treatment-seeking individuals diagnosed with AUD, while the prevalence prior to alcohol dependence was 5.3% and prevalence occurring outside of the context of alcohol dependence was 11.5%. 7
The major clinical problems associated with depression resulting in significant personal and public health consequences are its persistence and/or recurrence. 8,9 This persistence or recurrence is one of the reasons for depression’s considerable burden. 9 –12 Persistence occurs when there is a prolonged recovery time from a major depressive episode (MDE), while recurrence is the manifestation of a new MDE after a sustained period of remission. 13 Previous studies showed that about half of those who recover from a first MDE will have at least one additional event in their lifetime and nearly 80% of those with a history of two events will have another recurrence. 9,14 Significantly, a population-based Canadian study using the same data set as our study found that 55.3% of the participants reported repeated episodes of major depression in the following 6 years. 15
Previous studies suggest there may be differences in risk factors, neurobiological basis, and therapeutic response between major depression and recurrent or persistent major depression. 9,16,17 Using the “dynamic stress-vulnerability model,” 18 Spijker et al. classified the many risk factors for persistent major depression identified in the literature 19 as age, 20,21 female gender, 20,22 low socioeconomic status, 23 psychiatric illness and comorbidity, 23,24 and previous MDE episode. 20
Studies have been inconsistent in showing the relationship between AUD and persistent or recurrent depression. While some researchers found an association between substance use disorders and recurrent depression, suggesting a resolution of depressive symptoms and consequent loss of depressive diagnosis with abstinence from alcohol, 25 –27 others have not. 19,28,29 In Canada, there is a paucity of longitudinal data in mental health research. A significant number of studies come from cross-sectional data such as the Canadian Community Health Survey: Mental Health and Well-Being data. However, few studies have investigated the mental health research potential of longitudinal cohort studies by utilizing the nationally representative National Population Health Survey (NPHS) database. 30 In light of this, we explored the NPHS data to provide generalizable patterns of the recurrence/persistence of mental health and substance use disorders in Canada. This study aimed to determine whether concurrent AUD predicts persistence or recurrence of MDE after 6 years and 16 years of follow-up in a Canadian population sample. Furthermore, our study examined other factors that predict persistent or recurrent MDE after 6 years and 16 years of follow-up in this cohort.
Methods
Data Source and Study Cohort
Data came from the longitudinal NPHS (1994/1995 to 2010/2011), a nationally representative prospective epidemiologic survey of individuals 12 years and older, living in the 10 Canadian provinces in 1994/1995. Criteria for exclusion from the survey were living in certain remote areas, institutions, and reserves. In addition, full-time members of the Canadian armed forces were not included. The survey sample comprised of 17,276 participants who were reinterviewed every 2 years for 9 cycles (cycles 1 to 9). Detailed information on the NPHS methodology is available on the Statistics Canada web page. 31 In accordance with Statistics Canada rules, controlled access to the NPHS Master data file took place at the Saskatchewan Research Data Centre.
This secondary analysis of the NPHS data included only individuals 18 years and older who met the criteria for a diagnosis of an MDE in the previous 12 months at baseline (n = 908; Figure 1). The age restriction was based on the structured instrument for the diagnosis of MDE, which was only administered to individuals 18 years and older. This study focused on cycles 4 (6 years from baseline) and 9 (16 years from baseline). The original follow-up period for the NPHS ended in cycle 9. Cycle 4 which had a reasonable time interval from baseline (6 years) and a good response rate was used in this analysis due to a significant loss to follow-up in cycle 9 (Figure 2). The estimated response rates reported by Statistics Canada were 84.9% and 69.7% for cycles 4 and 9, respectively. 31
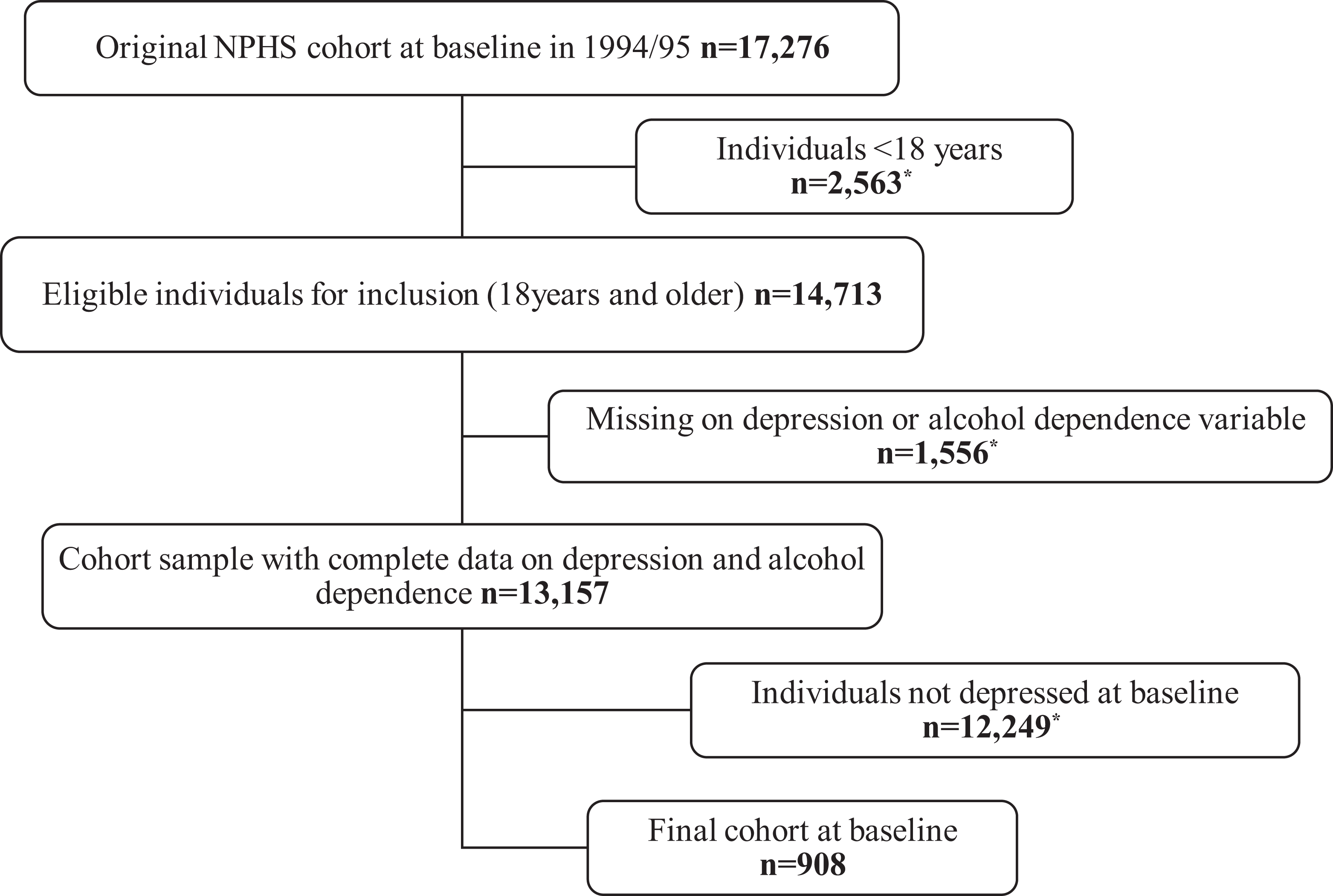
Cohort sample derivation. *Excluded from the analysis. NPHS = National Population Health Survey.
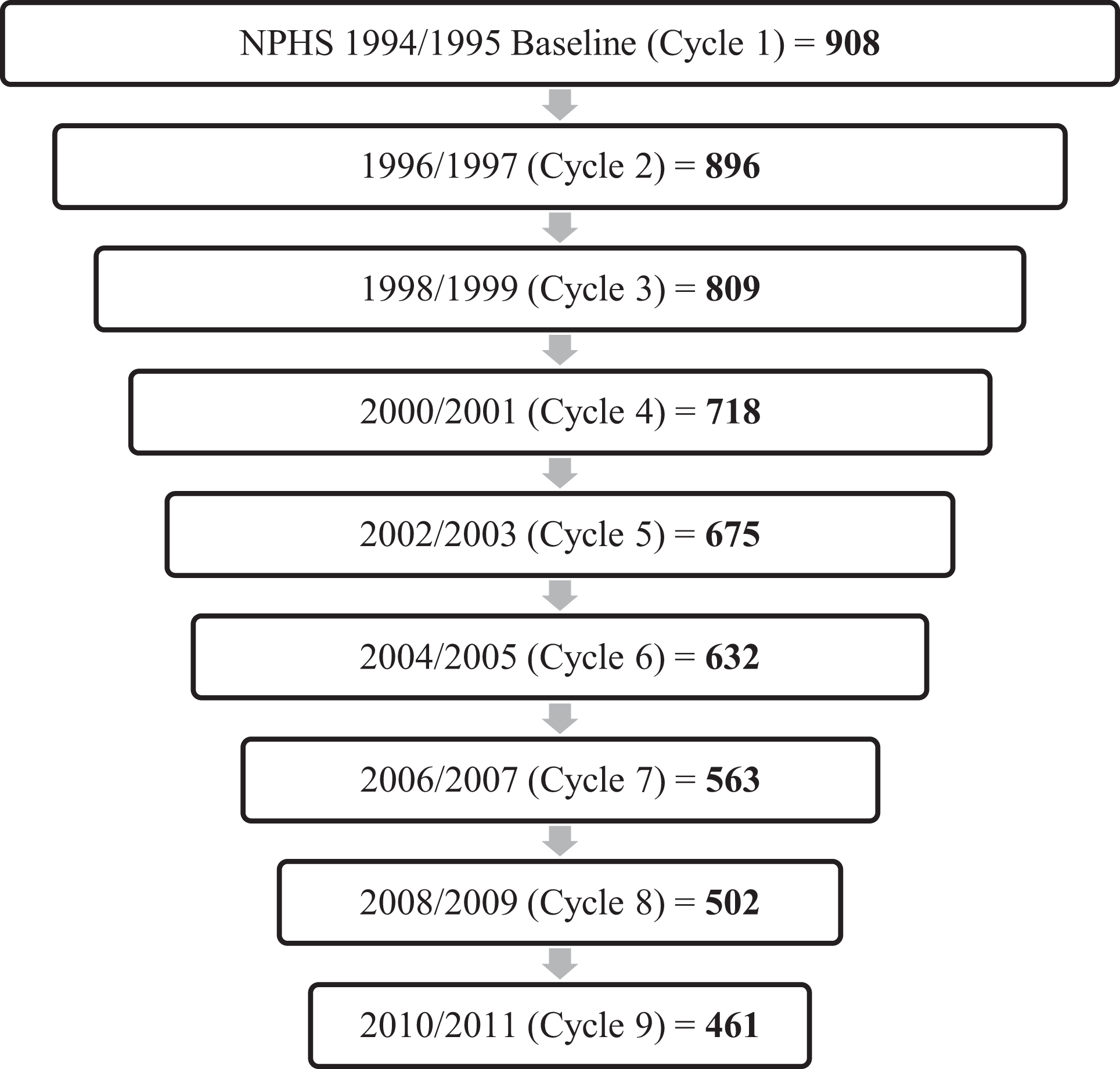
Follow-up chart. NPHS = National Population Health Survey.
Measures
Major depressive episode
The diagnosis of an MDE in the past 12 months was assessed at baseline (1994/1995) using the World Health Organization Composite International Diagnostic Interview Short Form (CIDI-SF) based on the Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised (DSM-III-R) criteria. 32 The past year’s MDE was evaluated on the same cohort every 2 years. The 6-year and 16-year persistence/recurrence of major depression were defined as meeting a diagnosis of MDE in the past 12 months at cycle 4 (2000/2001) and at cycle 9 (2010/2011) follow-up periods, respectively. No distinction is or could be made between persistence and recurrence major depression during the follow-up periods because the study time frame and data did not allow for such accuracy.
Alcohol use disorder
AUD was assessed in cycle 2 (1996/1997) as alcohol dependence using the World Health Organization CIDI-SF based on DSM-III-R criteria. 32 Alcohol dependence was not assessed at baseline.
Although the term “alcohol use disorder” better reflects the more recent iteration of the Diagnostic and Statistical Manual of Mental Disorders, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), the term “alcohol dependence” is used in this article in circumstances where appropriate to flag the use of the DSM-III-R criteria in the data. Studies assessing the differences in the DSM-III-R versus the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and DSM-5 criteria for problematic alcohol use suggest that the transition from DSM-III-R to DSM-IV saw modest increasing rates of abuse reported in epidemiological studies but decreasing rates of dependence. DSM-5 criteria that set aside the abuse/dependence dichotomy may result in an inflation of the prevalence rates of AUD. 33 –36
Other measures
The covariates were determined using Spijker et al.’s classification of risk factors for persistent depression based on the “dynamic stress-vulnerability model.” 18,19 Demographic factors (age, gender) and social vulnerability factors (education, marital status, dwelling owned—used as a proxy for socioeconomic status). The following are the psychobiological vulnerability factors measured: childhood and adult stress index—this measured the number of traumatic events respondents have been exposed to during their childhood, adolescence, or adulthood. Higher values indicate more stressors/traumatic events respondent has been exposed to in childhood/adolescence 32 ; presence of a physical chronic illness; Mastery index; and Self-esteem index scores. Higher scores indicate better mastery or self-esteem. 32 Sustaining factors measured were perceived social support, negative life events score (which included physical abuse, unwanted pregnancy, abortion or miscarriage, major financial difficulties, and serious problems at work or in school), and family stress index (a measure of ongoing difficulties/stressors such as activity overload, financial difficulties, and problems with relationships in day-to-day encounters). 32
Statistical Analyses
All statistical analyses were conducted using STATA version 14.0. First, we described the participant’s sociodemographic characteristics and risk factors for persistent or recurrent major depression in both the baseline and follow-up cohorts. Second, modified Poisson models were used to fit the data. The modified Poisson model is an effective way of estimating the relative risk (RR) of binary data in a cohort. 37
The RR for the persistence or recurrence of MDE, the main outcome of interest, was assessed for 6 years (model 1) and 16 years (model 2) of follow-up. The modeling was carried out in two stages for each model. First, all covariates were assessed independently as potential predictors of persistent or recurrent major depression. In stage 2, covariates that were independent risk factors or met a significance level of P < 0.25 were included in a multivariate model. The multivariate modified Poisson models were built using stepwise analyses with backward elimination of covariates. Covariates that were eliminated were assessed for confounding and re-entered into the model if found to confound the RR for alcohol dependence. Plausible interactions for gender and alcohol dependence, smoking, and alcohol dependence were tested for in each model but were not significant. Deviance and Pearson goodness-of-fit were tested on each model to justify the use of Poisson models. The postestimation command “fitstat” in Stata 14 was used to compute other measures of fit and to compare models with the interaction term and models without the interaction term.
Results
Participants’ Characteristics
At baseline, almost half of the cohort sample were aged between 25 and 44 years (48.7%); one-third were male (31.7%); almost half were married or common-law with a partner (42.7%); and 69.4% or almost two-thirds self-identified an existing chronic condition (Table 1). After 6 years (cycle 4) and 16 years (cycle 9), approximately 20% and 49% of participants were lost to follow-up, respectively (Figure 2).
Participant Characteristics of the NPHS and Cohort Sample at Baseline.
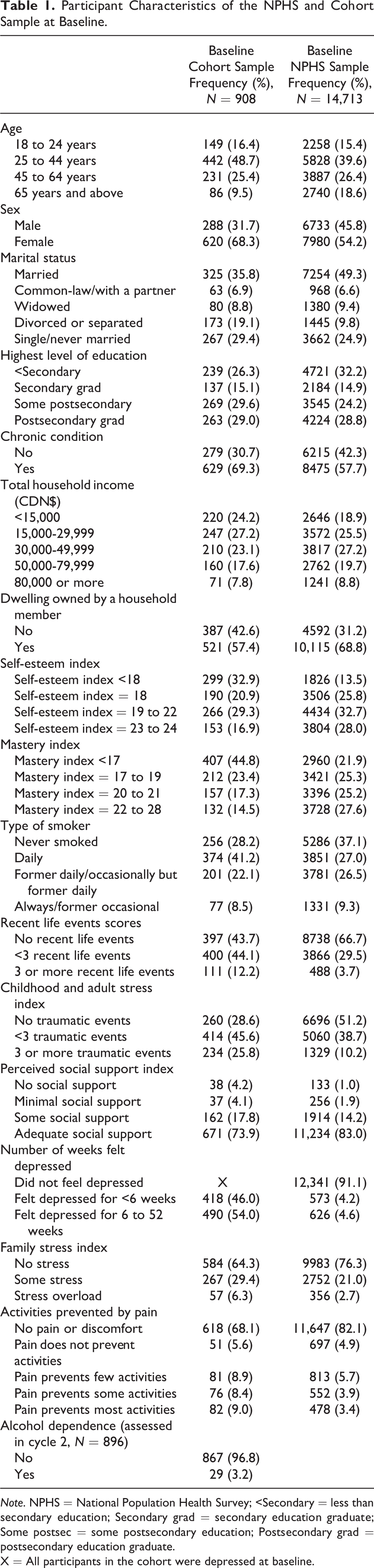
Note. NPHS = National Population Health Survey; <Secondary = less than secondary education; Secondary grad = secondary education graduate; Some postsec = some postsecondary education; Postsecondary grad = postsecondary education graduate.
X = All participants in the cohort were depressed at baseline.
Six-Year Persistence or Recurrence of Major Depression
After 6 years (cycle 4), 718 participants of the cohort sample of 908 participants meeting a diagnosis of MDE in the past 12 months at baseline remained in the study (Figure 2). Of these 718 participants, 124 still met the criteria for MDE in the past 12 months at this time. This accounted for 17.3% of the participants who were still in the study at cycle 4. Overall, 13.7% of the baseline cohort reported MDE symptoms after 6 years. The presence of alcohol dependence gave a 3-fold increase in the risk of having persistent or recurrent depression (Table 2). Other factors associated with the risk of persistent or recurrent depression were being a female, a daily smoker, having pain that prevents activities, and experiences of 3 or more traumatic life events. A self-esteem index of 23 and above was correlated with a reduction in the risk of persistent or recurrent depression by 46%.
Alcohol Dependence and Other Risk Factors for 6-Year Persistent or Recurrent Major Depression.
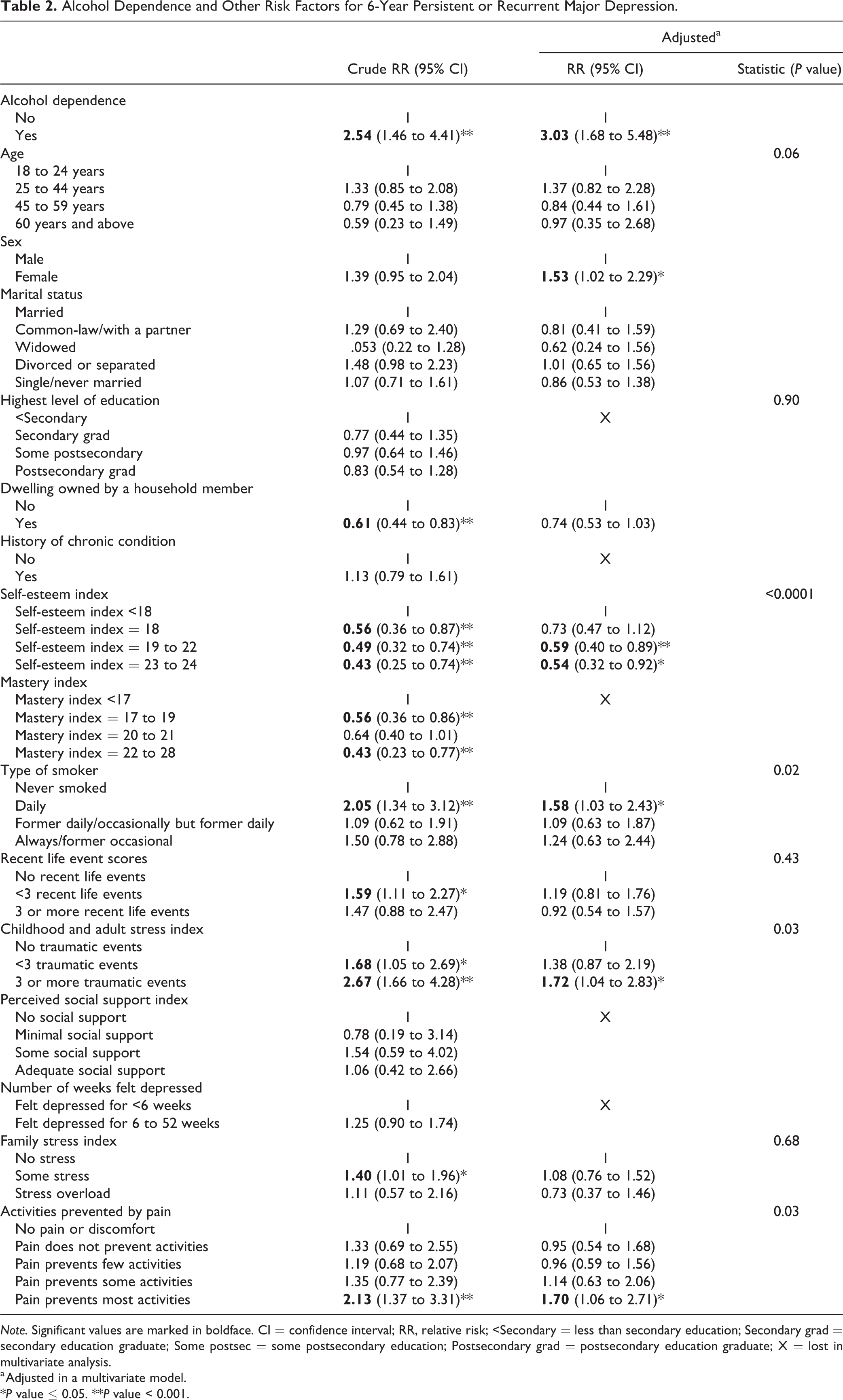
Note. Significant values are marked in boldface. CI = confidence interval; RR, relative risk; <Secondary = less than secondary education; Secondary grad = secondary education graduate; Some postsec = some postsecondary education; Postsecondary grad = postsecondary education graduate; X = lost in multivariate analysis.
a Adjusted in a multivariate model.
*P value ≤ 0.05. **P value < 0.001.
Sixteen-Year Persistence or Recurrence of Major Depression
After 16 years of follow-up (cycle 9), 461 (51%) participants of the cohort sample of 908 participants who met the criteria for a MDE in the past 12 months at baseline remained in the study (Figure 2). Of these 461 participants, 79 (17.14%) still met the criteria for MDE in the past 12 months at this time. Alcohol dependence remained a risk factor for the persistence/recurrence of major depression with a 3-fold increase in the risk compared to those who were not alcohol dependent (Table 3). There was a 2-fold increase in the associated risk of persistent or recurrent depression if participants had pain preventing activities compared to no pain or discomfort.
Alcohol Dependence and Other Risk Factors for 16-Year Persistent or Recurrent Major Depression.
Note. Significant values are marked in boldface. CI = confidence interval; RR = relative risk; <Secondary = less than secondary education; Secondary grad = secondary education graduate; Some postsec = some postsecondary education; Postsecondary grad = postsecondary education graduate; X = lost in multivariate analysis.
a Adjusted in a multivariate model.
*P value ≤ 0.05.
**P value < 0.001.
Discussion
Alcohol Use Disorder
This study showed that the associated risk for persistence/recurrence of major depression was 3 times higher with concurrent alcohol dependence. This supports the evidence that comorbidity is one of the strongest risk factors for persistent/recurrent major depression. 9,25,26,38 This also supports the evidence of the adverse effects of substance use disorders on the course of severe mental illness. 39 –41 Dependence on alcohol could be associated with an increased risk of persistent or recurrent depression by increasing the likelihood of symptom exacerbation, decreased social functioning, and treatment nonadherence. 9,39,42
Our findings could be explained by the “disorder-inducing” theory, which believes that one disorder causes the other, and the “self-medication” theory where major depression is being treated with alcohol to suppress symptoms. 43 –45 Another possible explanation could be the “overlapping predisposition” theory which postulates a common underlying vulnerability to AUD and major depression. This common vulnerability may be genetic and/or environmental 46,47 with a possible predisposition of individuals with significant vulnerability to have persistent or recurrent MDEs. 9,48 –50
Regardless of which pathway might be involved in causing the comorbid occurrence of major depression and alcohol dependence, once it is developed, a vicious cycle where one disorder exacerbates or maintains the other may have been triggered. 51,52 In other words, if one were to treat one disorder without addressing the other disorder, the risk of persistence or recurrence would be very high, 48,53,54 resulting in increased health-care utilization and costs. 55
Other Risk Factors
Childhood and adult stress index, a measure of the number of traumatic events the respondents have been exposed to, was associated with an increased risk of persistent/recurrent major depression in our study. This finding substantiates previous findings. 28,56 –58 Traumatic events such as physical and sexual abuse increase the prevalence, risk, and chronicity of depression, 56,57 which might be responsible for our finding. Physiologic dysregulation which results from stressful events during development might also lead to the increased risk of persistence/recurrence of depression 59 –61 and possibly treatment resistance. 56 –58
Consistent with previous findings, pain, smoking, lack of social support, low mastery, or low self-esteem were associated with persistent/recurrent depression. 9,21,62 –64 Social vulnerability factors such as education and socioeconomic status were not associated with persistence or recurrence, consistent with findings from the Netherlands 19 but inconsistent with findings from the United States. 20,23,65 This may reflect the income inequality in these countries, with the United States having more income inequality than the Netherlands and Canada. 66
The risk of persistent/recurrent depression was increased in females after 6 years of follow-up, consistent with previous findings. 20,22 In contrast with previous studies, 19 –21 age was not a determinant of persistent/recurrent depression in our study. There was no association between the duration of the most recent episode (number of weeks depressed) and persistent depression. This was consistent with previous findings of no associated risk of recurrence with the duration of the index episode. 9,67 This finding could be attributed to the fact that the index episode may not be the first episode, and results may simply be reflecting treatment response of participants. 68
Strengths and Limitations
The fairly large sample size based on a nationally representative sample of the Canadian population makes this study generalizable to the general Canadian population except individuals living in remotes areas, institutionalized, and are full-time members of the Canadian armed forces. This is one of the strengths of this study. The longevity of the study and the consistency of the relationships are other strengths of the study. Another strong feature of our study is that the diagnoses of alcohol dependence and MDE were derived using structured diagnostic instruments based on DSM-III-R criteria. However the transition from DSM-III-R to DSM-IV to DSM-5 diagnostic criteria for alcohol abuse and dependence poses a challenge for generalizing our findings to today’s diagnostic environment. Several articles have looked at the changing criteria for alcohol abuse and dependence and their potential impact of epidemiological estimates. 33 –36 As earlier mentioned, it is suggested that the transition from DSM-III-R to DSM-IV saw modest increasing rates of abuse reported in epidemiological studies but decreasing rates of dependence. DSM-5 criteria that set aside the abuse/dependence dichotomy may result in an inflation of the prevalence rates of AUD. However, these changes in diagnostic criteria do not distract from the main finding of our research that alcohol dependence is a strong risk factor for persistent or recurrent depression. Another limitation of this study was the loss of participants to follow-up. The inability to distinguish persistent depression from recurrent depression was a limitation. In addition, the diagnosis of MDE and alcohol dependence was interview-based, potentially introducing recall bias, and the severity of the index MDE which is an important determinant of prognosis was not assessed in the data.
Conclusion
There is a significant overlap in the mechanisms leading to AUD and major depression. The adverse effects of AUD on the long-term course of major depression and the increased health-care utilization caused by this comorbidity is a public health concern. It is imperative to treat both disorders simultaneously to improve treatment outcomes and reduce health-care costs.
Footnotes
Authors’ Note
VO conceived and designed the study, and analyzed the data. VO, TOF, and CD contributed to materials/analysis tools; VO, TOF, and CD wrote and edited the article.
Acknowledgments
The analysis presented in this article was conducted at the Saskatchewan Research Data Centre (SKY-RDC) which is part of the Canadian Research Data Centre Network (CRDCN). The services and activities provided by SKY-RDC are made possible by the financial or in-kind support of the SSHRC, the CIHR, the CFI, Statistics Canada, and the University of Saskatchewan. The views expressed in this article do not necessarily represent the CRDCN’s or that of its partners.’
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.