
Abstract
Background:
Suicide is a leading cause of mortality among youth globally. Evidence suggests that individuals with physical illness, mental illness, or neurodevelopmental disorders are at increased risk of suicide. However, few studies have estimated the prevalence of suicidal ideation and suicide attempts among youth with compounding health burdens. The purpose of this study is to estimate the prevalence of suicidal ideation and suicide attempts and their associations across morbidity status among youth in Canada.
Methods:
Data come from 6,915 youth aged 15–17 years (49% female) enrolled in the 2019 Canadian Health Survey on Children and Youth. The person most knowledgeable or the youth themselves provided responses regarding sociodemographic characteristics, morbidity status, and indicators of suicide. The prevalence of suicidal ideation (past year) and suicide attempts (lifetime) were compared across morbidities (none, physical illness only, mental illness only, neurodevelopmental disorder only, and multimorbidity). Logistic regression models estimated adjusted associations between morbidity status and suicidal behaviour.
Results:
Suicidal ideation and suicide attempts were most commonly reported by youth with mental illness only (32%, 18%) and multimorbidity (28%, 19%). While all morbidities were associated with indicators of suicide, the strongest association was found between multimorbidity and suicide attempts odds ratio = 5.2 (3.4, 8.0).
Conclusions:
These contemporary estimates of youth in Canada suggest that suicidal ideation and suicide attempts are common and reinforce the need for integrated physical and mental health services for youth with multimorbidity to reduce the incidence. Research investigating causal mechanisms of the intersections between physical illness, mental illness, neurodevelopmental disorders, and suicide is needed.
Plain Language Summary Title:
Morbidity, suicidal ideation and suicide attempts among youth in Canada
Plain Language Summary
Background
Suicide is a leading cause of death among youth worldwide. Youth with physical, mental, or neurodevelopmental disorders are more likely to have suicidal behaviours. However, few studies assess how common suicidal behaviours are among youth with multiple disorders. The purpose of this study is to understand how to estimate how commonly suicidal behaviours occur among youth with different combinations of disorders in Canada.
Methods
Data come from 6,915 youth between the ages of 15 to 17 years (49% female) enrolled in the 2019 Canadian Health Survey on Children and Youth. The person most knowledgeable or the youth themselves provided responses on the youth's characteristics, disorders they experienced, and suicidal behaviours. Various suicidal behaviours such as suicidal ideation (past year) and suicide attempts (lifetime) were compared across different disorders. Statistical techniques were used to measure if childhood disorders were related to suicidal behaviours.
Results
Suicidal ideation and suicide attempts were most commonly reported by youth with mental illness only (32%, 18%) and youth with co-occurring physical, mental or neurodevelopmental disorders (28%, 19%). Youth with co-occurring physical, mental or neurodevelopmental disorders was strongly associated with suicide attempts.
Interpretation
Our findings highlight that suicidal behaviours are common among youth in Canada, and integrated services are needed to reduce suicide. Further studies are needed to understand increased risks among youth with co-occurring physical, mental or neurodevelopmental disorders.
Introduction
Suicide attempts are an important public health concern, with suicide resulting in approximately 700,000 lives lost worldwide in 2019. 1 In Canada, suicide is the second leading cause of death among youth and young adults aged 15–34 years. 2 Sociodemographic characteristics such as low educational attainment and low socioeconomic status have been associated with increased risk of both suicidal ideation and suicide attempts.3,4 Psychosocial factors, such as experiences of victimization (e.g., bullying), have also been associated with increased risk of both suicidal ideation and suicide attempts. 5
Evidence suggests that mental disorders, such as mood disorders,6,7 and neurodevelopmental disorders, such as autism and attention-deficit hyperactivity disorder (ADHD) 8 have been associated with increased risk of suicide. Many mechanisms may underlie the relationship between mental illness, neurodevelopmental disorders, and suicidal ideation. Symptoms of mental illness and neurodevelopmental disorders, such as distress and anxiety may lead some individuals to consider suicidal behaviour as a means to escape. 9 Evidence also suggests that physical illness increases the risk of suicidal behaviour among youth. 10 Potential mechanisms are multifaceted—some evidence suggests that physical illness may reduce pain tolerance or hinder coping mechanisms, which have been associated with an increased risk of suicide. 11
While associations between physical illness, mental illness, and neurodevelopmental disorders, with indicators of suicide have been investigated independently, there is a dearth of evidence estimating their relative and combined impact. This study aimed to estimate the prevalence of suicidal ideation and suicide attempts and quantify the magnitude of the association between morbidity status and suicidal behaviour. We hypothesized that each morbidity status (physical illness only, mental illness only, neurodevelopmental disorder only, and physical–mental/neurodevelopmental multimorbidity (herein referred to as multimorbidity)) would be associated with suicidal ideation and suicide attempts with the strongest magnitude of association for youth with multimorbidity.
Methods
The 2019 Canadian Health Survey on Children and Youth (CHSCY) is a cross-sectional nationally representative survey of children and youth aged 1–17 years that was conducted between February and June 2019 to collect data on the health and behaviours of Canadian children.12,13 The CHSCY utilized the sampling frame of the 2018 Canada Child Tax Benefit file targeting 98% of Canadian households. 13 The sample was selected using multistage, random sampling with field interviews (either in person or by telephone) with the person most knowledgeable (PMK) of the selected youth. Field interviewers informed the PMK about the study, confirmed eligibility, and invited eligible youth to participate in the survey. A total of 47,871 children and youth were included in the CHSCY. Youth aged 12–17 years provided self-reports. The sample for the current study was restricted to measures of suicidal ideation and suicide attempts that were only asked of youth aged 15–17 years (N = 6,915) (Supplemental S1).
Measures
Illnesses, Disorders, and Morbidity Status
Using a self-administered questionnaire, the youth responded as to whether they had been diagnosed with any long-term conditions (binary response). Physical illnesses included severe headaches, allergies, asthma, diabetes, and epilepsy. These conditions represent some of the most common chronic physical illnesses affecting youth. 14 The PMK reported the height and weight of their youth, which was used to calculate and classify youth according to body mass index including underweight (<18.5), optimum (18.5–24.9), overweight (25–29.9), and obesity (≥30). 13 The youth was also asked if they had any other long-term physical, mental, developmental, or intellectual conditions. Response data for this question aggregated physical illnesses, mental illness, and neurodevelopmental disorders; thus, a positive endorsement of this item, but no other physical illness, mental illness, or neurodevelopmental disorders, resulted in study exclusion.
A similar binary response option was used to ascertain whether youth had a Diagnostic and Statistical Manual of Mental Disorders, 5th Edition-aligned mental illness or neurodevelopmental disorder: anxiety disorder (phobia, obsessive-compulsive disorder, or panic disorder), mood disorder (depression, bipolar disorder, mania, or dysthymia), ADHD, autism spectrum disorder (autism, autistic disorder, Asperger's disorder, or pervasive developmental disorder), and eating disorder (anorexia or bulimia). Other diagnoses such as fetal alcohol spectrum disorder or learning disabilities or disorders were also measured. These conditions represent the most common mental illness and neurodevelopmental disorders among youth. 15
Youth morbidity status was defined as physical illness only, mental illness only, neurodevelopmental disorder only, or multimorbidity (≥1 physical illness and ≥1 mental illness and neurodevelopmental disorder).
Suicidal Ideation and Suicide Attempts
Suicidal ideation (past year) and suicide attempts (lifetime) were measured based on binary responses to standardized questions that align closely with gold-standard assessment approaches of suicidal behaviour. 16 Suicidal ideation was assessed by asking, if in the past 12 months, the youth “ever seriously consider attempting suicide or taking their own life?” Suicide attempts were assessed by asking “Have you ever attempted suicide or tried taking your own life?”
Sociodemographic Characteristics
Sex at birth and current gender identity were derived based on youth reports. A combination of both sex at birth and current gender identity was used to derive a variable for cisgender and transgender participants aligning with current gold standards to classify gender identity. 17 Sexual orientation based on youth-reported statements was categorized as heterosexual (i.e., only opposite gender attraction); boys who were only or mostly attracted to boys; girls who were only or mostly attracted to girls; those attracted to more than 1 gender (i.e., individuals with equal attraction to females and males, or mostly attracted to the opposite gender); and unsure. The PMK reported their own demographic factors such as sex, education level, and marital status that were included as covariates in the analyses. The Canadian low-income cut-off reflecting community size and number of individuals within the household was used to determine low-income households. 13 Other characteristics such as PMK and youth ethnicity and immigration status were also collected. PMK mental health was measured based on a 5-point scale ranging from excellent to poor.
Psychosocial and Health Factors
Victimization was measured based on experiences of bullying within the past year. A 5-point scale (from never to daily experience) was used to measure the frequency of 8 bullying experiences. A composite measure of victimization was computed based on these measures with higher cumulative scores indicating a greater frequency of victimization. Functional disability was measured using the UNICEF/Washington Group functioning module and dichotomized. 18 Communities were also classified based on standardized thresholds for community size. Neighbourhood safety was measured based on a 5-point scale ranging from very unsafe to very safe.
Analysis
Sampling weights as calculated by Statistics Canada were used to ensure comparability between the sample and the general youth population in Canada (13). The prevalence of illness/disorder, morbidity status, suicidal ideation, and suicide attempts among youth were reported. The Rao–Scott χ2 test determined if the prevalence of indicators (i.e., suicidal ideation and suicide attempts) were different across morbidity status. Logistic regression models quantified associations between morbidity status and indicators of suicide, adjusting for sociodemographic characteristics. Odds ratios (ORs) and associated 95% confidence intervals were reported. Data were analyzed using SAS 9.4.
Results
The characteristics of the sample are detailed in Table 1. Youth had a mean age of 15.9 years, and 48.6% were female. Most youth identified their sexual orientation as heterosexual (90.1%) and 36.1% identified as a racial or ethnic minority. The majority of PMKs were female (90.2%), were partnered (79.2%), and 37.4% had a postsecondary degree. Immigrants or permanent residents accounted for 34.7% of PMKs. Most households resided in large urban centers with community sizes ≥100,000 (61.8%).
Sociodemographic Characteristics, Psychosocial and Health Factors of the Sample (n = 6,915).
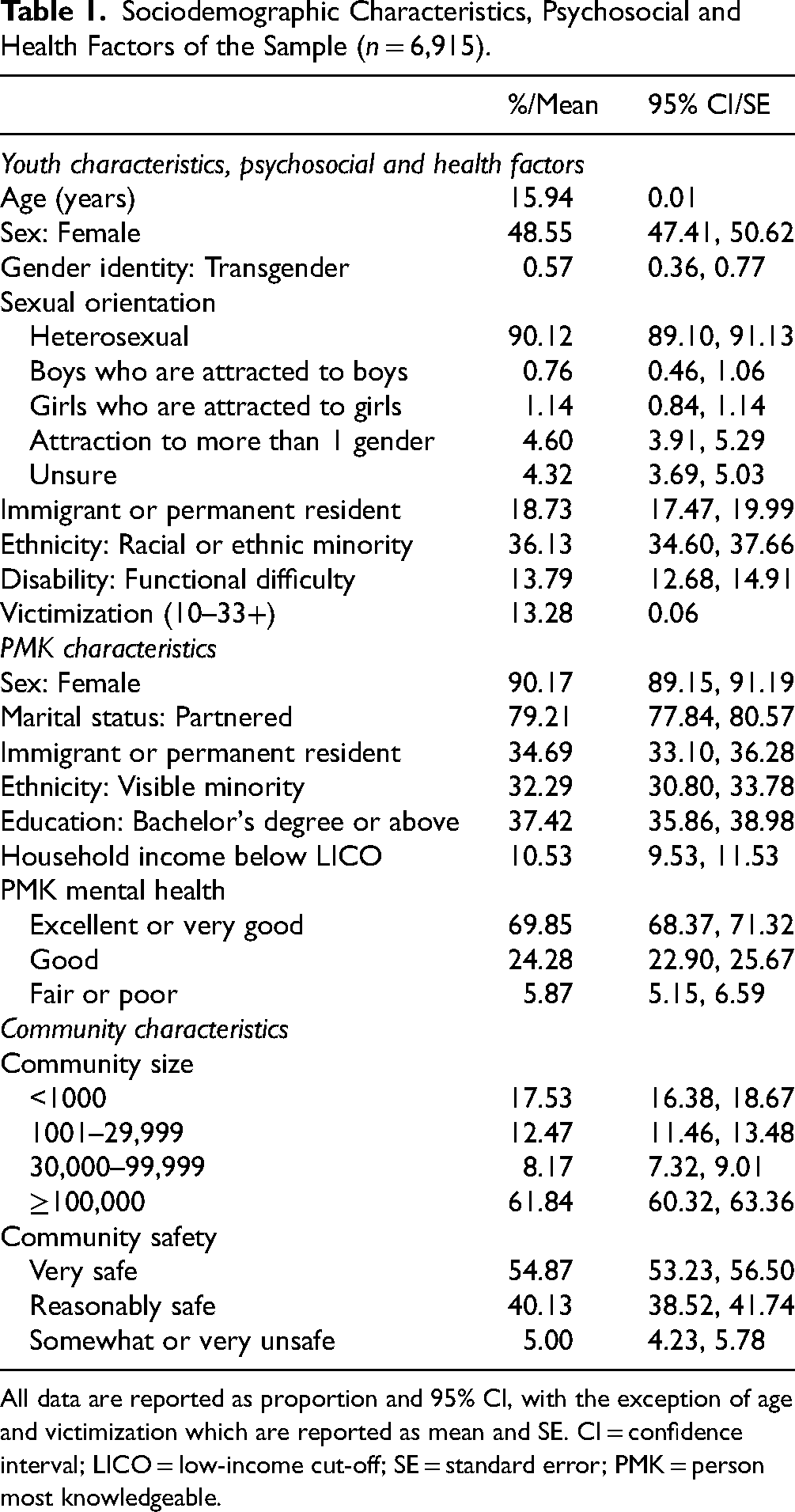
All data are reported as proportion and 95% CI, with the exception of age and victimization which are reported as mean and SE. CI = confidence interval; LICO = low-income cut-off; SE = standard error; PMK = person most knowledgeable.
As shown in Table 2, suicidal ideation (past year) and suicide attempts (lifetime) were reported by 14.1% and 6.8% of youth, respectively. The distribution of morbidity status was 39.5% physical illness only, 3.3% mental illness only, 6.1% neurodevelopmental disorder only, and 14.9% multimorbidity.
Prevalence of Illnesses/Disorders, Morbidity Status, and Indicators of Suicidal Behaviour (n = 6,915).
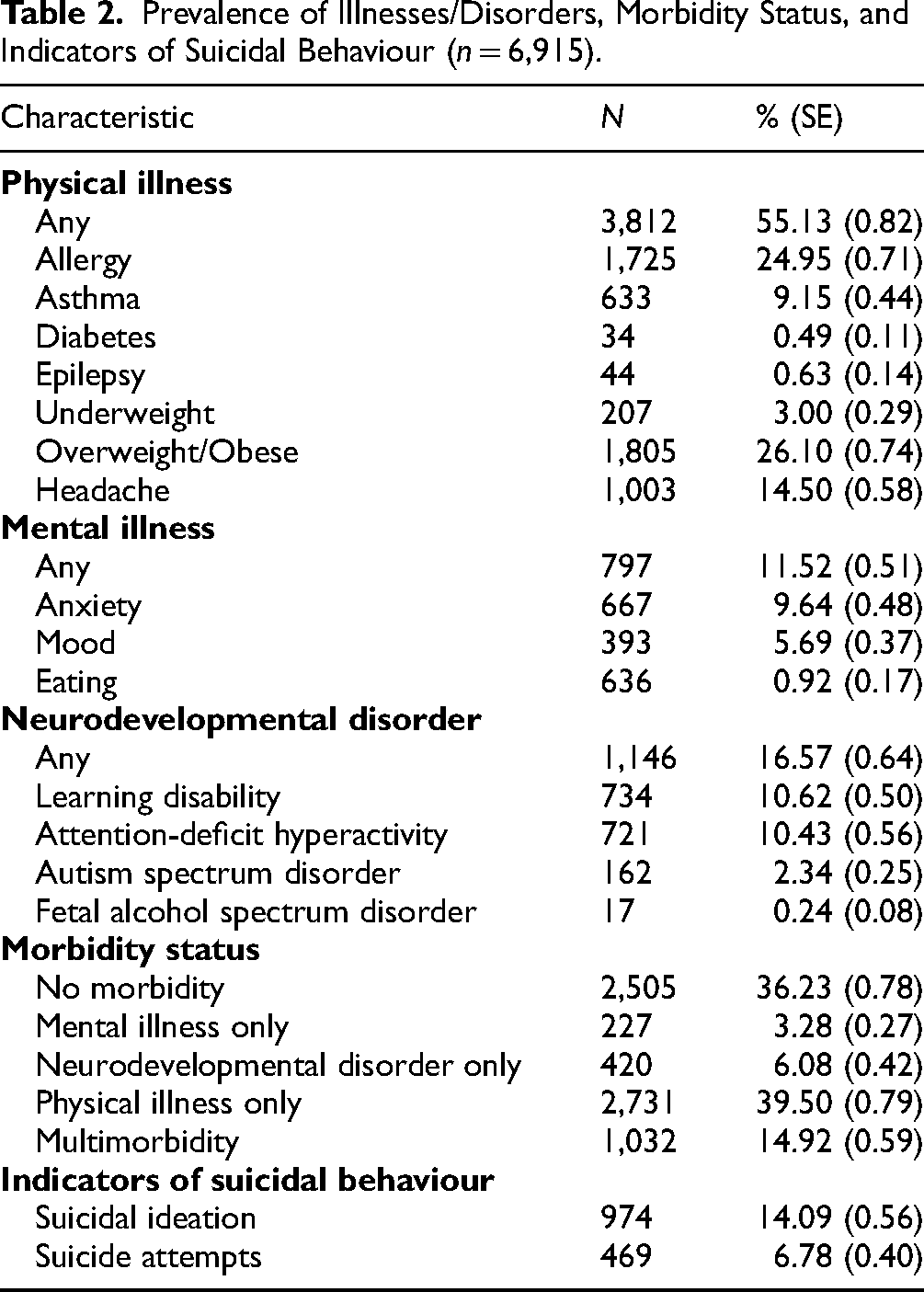
Table 3 shows the distribution of indicators of suicidal behaviour across individual physical illness, mental illness, and neurodevelopmental disorders. Across categories of morbidity, suicidal ideation was most reported by youth with diabetes (34.7%), mood disorder (51.7%), and ADHD (16.3%); and suicide attempts were most reported by youth with chronic headache (17.1%), eating disorder (37.7%), and ADHD (12.9%).
Prevalence of Suicidal Ideation and Suicide Attempts Across Individual Physical Illness, Mental Illness, and Neurodevelopmental Disorder (n = 6,915).
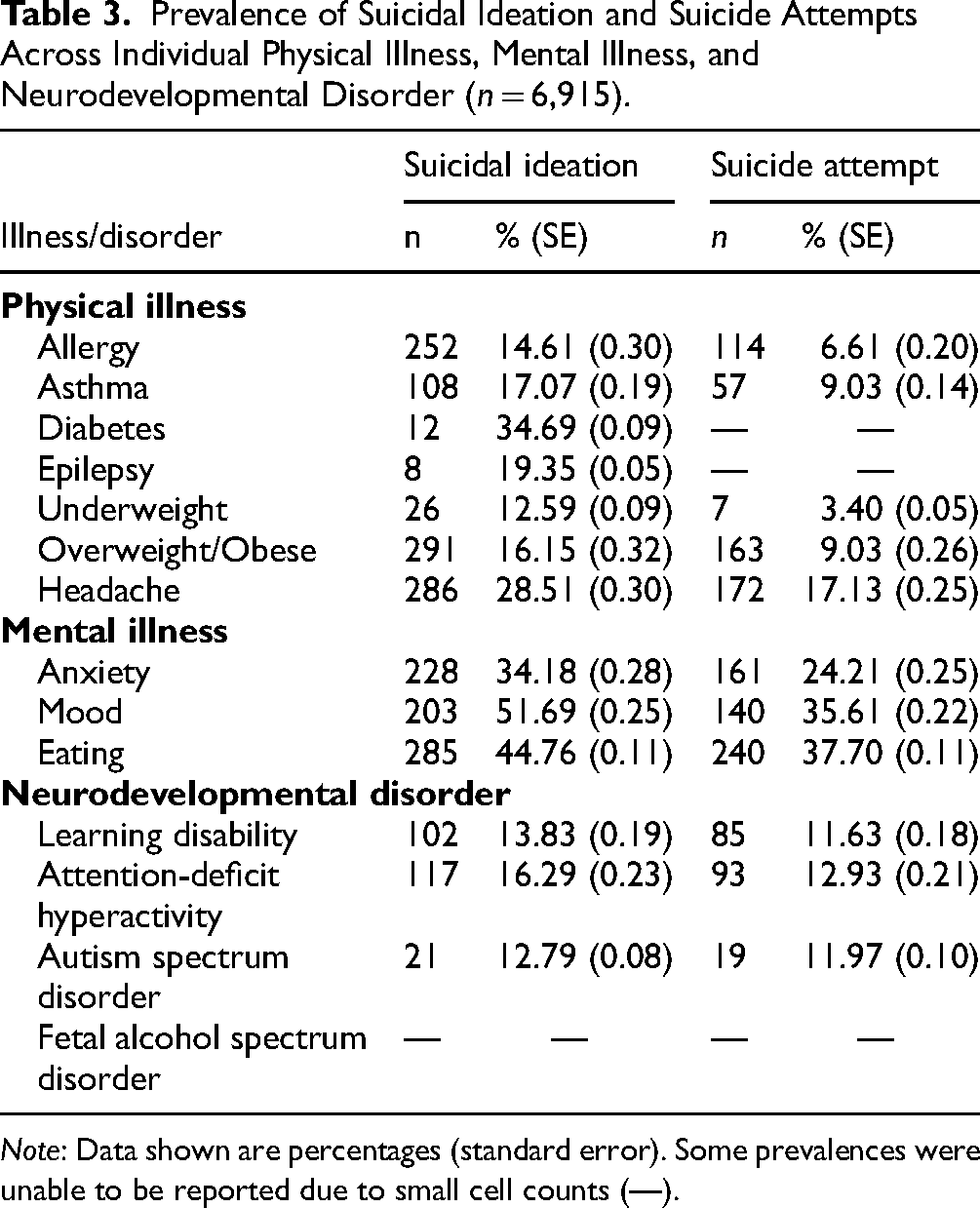
Note: Data shown are percentages (standard error). Some prevalences were unable to be reported due to small cell counts (—).
Comparing the prevalence of suicidal ideation and suicide attempts demonstrates significant variation across morbidity status (Table 4). Prevalence was consistently lowest among youth without any chronic health condition (i.e., no morbidity). Prevalence of suicidal ideation and suicide attempts was consistently highest among youth with mental illness only (31.6%, 17.6%) or multimorbidity (27.5%, 18.7%). Estimates of prevalence were not significantly different between those with mental illness only versus multimorbidity, but both groups had a prevalence significantly higher than the physical illness only and neurodevelopmental disorder only groups.
Prevalence of Suicidal Ideation and Suicide Attempts Across Morbidity Status (n = 6,915).

Note: Data shown are percentages (standard error). CTL = control (no morbidity); MI = mental illness; ND = neurodevelopmental disorder; PI = physical illness; MM = multimorbidity. All comparisons are statistically significant (p < 0.05)
Table 5 shows the final adjusted estimates of the associations between morbidity status and indicators of suicidal behaviour (estimates from the unadjusted and semi-adjusted models are shown in Supplemental S2 and S3). Mental illness only and multimorbidity showed significant positive associations with both suicidal ideation and suicide attempts, and these associations showed smaller associations for suicidal ideation and larger associations for suicide attempts. Physical illness only showed associations with suicidal ideation, but not suicide attempts while neurodevelopmental disorder only showed associations with suicide attempts but not suicidal ideation. There was significant variation in the magnitudes of association across all morbidities for both suicidal ideation and suicide attempts. The likelihood of reporting suicidal ideation (OR = 3.5 [2.2, 5.5]) was strongest for youth with mental illness only. However, odds of suicide attempt were highest for youth with multimorbidity (OR = 5.2 [3.4, 8.0]).
Final Adjusted Logistic Regression Models Predicting Suicidal Ideation and Attempts (n = 6,915).
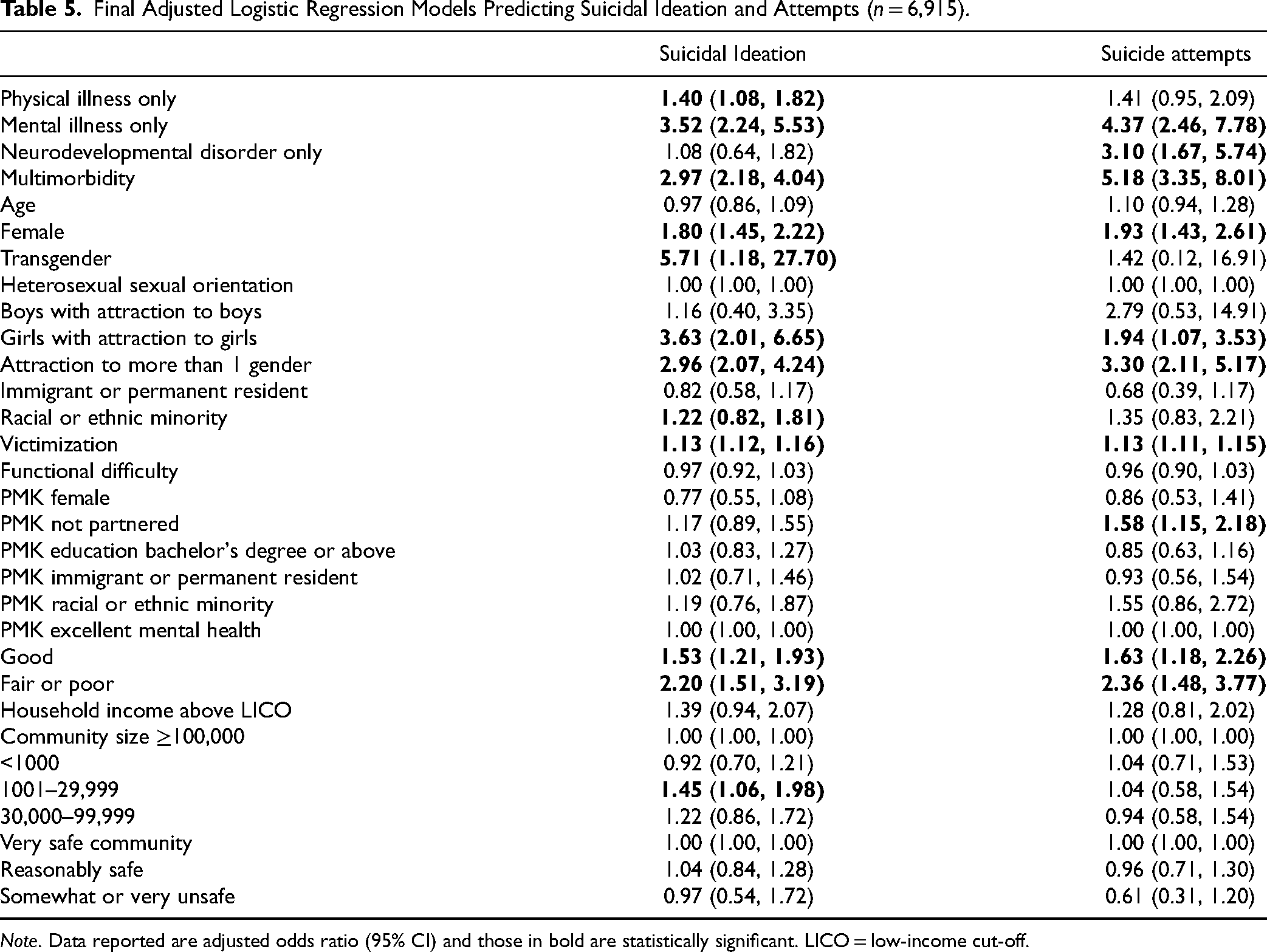
Note. Data reported are adjusted odds ratio (95% CI) and those in bold are statistically significant. LICO = low-income cut-off.
Amongst covariates in the model, several noteworthy associations were found. The odds of suicidal ideation and suicide attempts were relatively high for youth who were female, identified as transgender or reported some nonheterosexual orientations. Youth who had a PMK with lower ratings of mental health were also more likely to report suicidal ideation and suicide attempts.
Interpretation
This study provides contemporary estimates of the prevalence of suicidal ideation and suicide attempts among youth in Canada, specifically among those with multimorbidity and other morbidities. Findings showed strong positive associations between morbidity status, especially mental illness only and multimorbidity with suicidal ideation and suicide attempts. Associations were found for mental illness only and multimorbidity across suicidal ideation, and suicide attempt. Adjusting for relevant covariates, youth with multimorbidity had the highest likelihood of reporting suicide attempts.
Prior studies have linked multimorbidity to higher complex care needs and lower life satisfaction and quality of life. 19 Elevated risk of suicidal ideation and suicide attempts among youth with multimorbidity may reflect the heightened challenges they face in managing co-occurring chronic health conditions that impact their daily activities. Indeed, our findings showed that the association between multimorbidity was significantly larger than the independent associations of the other morbidity groups. This evidence supports the crucial need for policy and action that supports universal implementation of integrated physical and mental/developmental health services. 20 Such care must acknowledge that the intersection of physical illness, mental illness, and neurodevelopmental disorders has compounding negative consequences for youth and health systems with siloed physical and mental/developmental health services may be ill-equipped to promote positive mental health and timely upstream interventions to reduce the incidence of suicidal behaviours among youth with multimorbidity. 21
Other morbidities also showed robust associations with indicators of suicidal behaviours—a finding consistent with previous studies of epidemiological samples of youth with physical illness, mental illness, or neurodevelopmental disorder conducted over the past decade. 22 These associations may reflect the emotional, behavioural, and functional impairments, as well as potential social interaction difficulties experienced by these subgroups of youth that exacerbate the risk of suicidal ideation and suicide attempts. Mechanistic studies that elucidate the biological and psychosocial pathways that mediate or moderate these associations, and whether findings generalize across morbidities, including multimorbidity, are warranted. Findings from these studies can identify modifiable processes amenable to intervention using broad and targeted preventive interventions across the health, social, and educational systems.
While most other variables in the analyses were used to minimize biases in the estimates of the association between morbidity status and suicidal ideation or suicide attempts, some findings warrant discussion. Youth who identify as female, transgender, or having some nonheterosexual orientation represent particularly vulnerable subgroups in the general Canadian population. 23 This vulnerability may be amplified in the context of having a chronic health condition or multimorbidity. 24 The extent to which these individual-level factors may moderate associations between morbidity status and indicators of suicide using an intersectionality lens requires investigation with larger and more diverse epidemiological samples of youth. Evidence-based mental health services for these individuals are needed to address unique experiences of bias-based victimization, stigma, social oppression, and multilayered discrimination 25 that may heighten risk of suicidal ideation and suicide attempts.
Our finding that poorer PMK mental health is associated with an increased likelihood of reported suicidal ideation, and suicide attempt among youth is consistent with previous evidence. Prior studies suggest that suicidal ideation and suicide attempts are higher among youth whose parents seek health services for their own mental health. 26 Integrated pediatric health services should incorporate family centred approaches to care that address the holistic needs of youth, which include promoting and supporting parent mental health. Indeed, such models of care have been shown to be effective. 27
While the CHSCY is a large, nationally representative study of Canadian youth, some limitations require mentioning consideration. First, conditions included in the CHSCY reflect a nonexhaustive list of physical illnesses, mental illnesses, and neurodevelopmental disorders. The potential of misclassification of youth by morbidity status may impact the magnitudes of association with suicidal ideation and suicide attempts. The direction of this potential bias on reported estimates is unknown. Second, the cross-sectional nature of the CHSCY prevents inferences of causality. Third, the CHSCY sample was restricted to those families listed in the Canada Child Tax Benefit file. This excludes on-reserve Indigenous children; thus, findings do not generalize to this population. Fourth, the COVID-19 pandemic has arguably changed the global landscape of youth mental health, and these findings may underestimate current burdens associated with suicidal ideation and suicide attempts. However, the opportunity exists to use these findings as the baseline for future studies examining associations between morbidity status and suicidal behaviours post-COVID-19.
This study provides the first available evidence on both suicidal ideation and attempts, and their associations with morbidity using nationally representative data of youth in Canada. Findings reinforce the need for policies and resource allocation that promote and support family centred integrated physical–mental/developmental health services for youth. This model of care should prioritize screening and early intervention for suicidal ideation and suicide attempts among youth, particularly those diagnosed with physical illness, mental illness, neurodevelopmental disorder, or multimorbidity. Studies that investigate the intersectionality of morbidity on suicidal behaviours are warranted, as are longitudinal studies that examine changes in prevalence (relative to these pre-COVID-19 baseline findings) and the nature of the association between morbidity status and suicidal ideation and suicide attempts over the life course. Future studies should also explore whether variation in type of multimorbidity (e.g., multiple mental illnesses) increases risk of suicidal ideation and suicide attempts.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251343292 - Supplemental material for Morbidity, Suicidal Ideation and Suicide Attempts Among Youth in Canada: A Nationally-Representative Study: Morbidité, idées suicidaires et tentatives de suicide chez les jeunes au Canada : Une étude représentative à l’échelle nationale
Supplemental material, sj-docx-1-cpa-10.1177_07067437251343292 for Morbidity, Suicidal Ideation and Suicide Attempts Among Youth in Canada: A Nationally-Representative Study: Morbidité, idées suicidaires et tentatives de suicide chez les jeunes au Canada : Une étude représentative à l’échelle nationale by Danielle Fearon, PhD, Alex Luther, PhD, Dillon Browne, PhD, Ian Colman, PhD, Joel A. Dubin, PhD, Laura Duncan, PhD and Mark A. Ferro, PhD in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the American Foundation for Suicide Prevention (grant number SRG-0-008-22).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.