
Abstract
Objective
The aim of this study was to estimate the six-month prevalence of mental illness in children with chronic physical illness (multimorbidity), examine agreement between parent and child reports of multimorbidity, and identify factors associated with child multimorbidity.
Method
The sample included 263 children aged 2–16 years with a physician-diagnosed chronic physical illness recruited from the outpatient clinics at a pediatric hospital. Children were categorized by physical illness according to the International Statistical Classification of Diseases and Related Health Problems (ICD)-10. Parent and child-reported six-month mental illness was based on the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID).
Results
Overall, 101 (38%) of children had a parent-reported mental illness; 29 (25%) children self-reported mental illness. There were no differences in prevalence across ICD-10 classifications. Parent-child agreement on the MINI-KID was low (κ = 0.18), ranging from κ = 0.24 for specific phobia to κ = 0.03 for attention-deficit hyperactivity. From logistic regression modeling (odds ratio [OR] and 95% confidence interval), factors associated with multimorbidity were: child age (OR = 1.16 [1.04, 1.31]), male (OR = 3.76 [1.54, 9.22]), ≥$90,000 household income (OR = 2.57 [1.08, 6.22]), parental symptoms of depression (OR = 1.09 [1.03, 1.14]), and child disability (OR = 1.21 [1.13, 1.30]). Similar results were obtained when modeling number of mental illnesses.
Conclusions
Findings suggest that six-month multimorbidity is common and similar across different physical illnesses. Level of disability is a robust, potentially modifiable correlate of multimorbidity that can be assessed routinely by health professionals in the pediatric setting to initiate early mental health intervention to reduce the incidence of multimorbidity in children.
Introduction
Chronic physical illness imposes adverse effects on the mental health of children and can lead to reduced life quality, and poorer social, educational, and employment outcomes. 1 Physical and mental health are strongly intertwined, 2 creating challenges for children, families and health professionals, particularly when these emerge early in life. Epidemiological data show that 20–35% of children have cooccurring physical and mental illness (herein multimorbidity), which typically extend throughout the life-course. 3 In addition to its chronicity, 4 the experience of multimorbidity early in life is associated with poorer quality of life5–7 and increased use of mental health services/care, including counseling, medication, hospitalization, and emergency department.8,9 Indeed, child multimorbidity is an important public health concern. Although the literature base is growing, knowledge gaps remain.
First, prevalence estimates of mental illness in higher-risk children with physical illness, including those requiring routine follow-up, is lacking. Few studies exist, each with small samples, resulting in wide estimates from 25% to >50%.6,10,11 More reliable prevalence estimates are needed to understand burden and inform resource allocation.
Second, while evidence suggests various biological 12 and psychosocial factors 13 are associated with childhood mental illness, it is unknown if these associations extend to children with multimorbidity, who are already at increased risk. Known risk factors for childhood mental illness include: older child age, sex (dependent on internalizing or externalizing outcomes), disability/impairment, obesity, lower socioeconomic status, and parental psychopathology. 13 Understanding the confluence of these underlying factors may inform targeted interventions for at-risk children to reduce the incidence of childhood multimorbidity.
Third, commonly in research, physical illnesses are identified using disease-specific checklists that are dependent on diagnosis and/or etiology; however, this method does not consider the broad context of chronic conditions which also includes functional limitations, dependence, and service use/need. Such diagnostic groupings may restrict comparisons across studies and may hinder the provision of health services and healthy public policy. In studying child mental illness, findings have shown diminutive differences in risk and severity across different physical illnesses. 14 Thus, conceptualizing physical illness into a single, non-categorical group may be useful. Further investigation is required to confirm the utility of this approach in the context of child multimorbidity. Such information can inform more universal and integrated pediatric health services, which are often fragmented, siloed, and specific to either physical or mental illness. For instance, within a causal framework, child functioning—a generic illness measure—can be an intervention target across services to prevent multimorbidity. 15
Fourth, the complexity in understanding childhood mental illness in the context of physical morbidity is further compounded given that agreement is generally low between parent and child reports of mental/psychosocial health. 16 In children newly-diagnosed with physical illness, parent-child agreement is low but improves over time; possibly due to the evolution or experience of the psychosocial consequences associated with physical illness during childhood and adolescence. 17 The extent to which parent-child agreement on mental health may be influenced by multimorbidity is unknown and such information can be useful in medical decision-making and in treatment evaluation. Under-endorsement of symptoms by parents could result in inadequate care management and subsequently, worse functioning in children.
In the context of the paucity of research in child multimorbidity and the outlined knowledge gaps in the field, the objectives of this study were to estimate the prevalence of six-month mental illness in children with chronic physical illness (i.e., multimorbidity) attending outpatient clinics at a pediatric hospital, examine agreement between parent and child reports of multimorbidity, and to identify factors associated with child multimorbidity. Based on the limited available evidence, we hypothesized that the overall prevalence of multimorbidity would be approximately 40% and 25% for parent and child reports, respectively, and that the prevalence of six-month mental illness would not differ across different types of physical illnesses. Additionally, we hypothesized that agreement on reports of mental illness between parents and children would be low. It was predicted that the odds of multimorbidity would be higher for children who were older and female, had higher levels of disability, come from households reporting socioeconomic disadvantage, and had parents reporting elevated levels of psychological distress.
Methods
Design and Sample
Data come from the Multimorbidity in Youth across the Life-course (MY LIFE), a prospective study of children with physician-diagnosed physical illnesses and their primary caregiving parent.18,19 In this manuscript, we report the baseline (i.e., cross-sectional) findings from this ongoing study. Briefly, recruited from outpatient clinics at an academic pediatric hospital in Canada, participants are followed for 24 months, with assessments at baseline, six, 12, and 24 months. The inclusion criteria were: children aged 2–16 years, physical illnesses that were chronic in nature (operationally defined as expected to be present for ≥12 months and result in ≥1 of the following: functional limitations; dependencies to compensate for functional limitations [e.g., medication, use of assistive devices]; or, need for additional health services), and children and parents had sufficient English language skills to complete the study interviews and questionnaires. Physical illness in children and time since the onset of their illness were classified according to the International Statistical Classification of Diseases and Related Health Problems (ICD)-10. 20 Children were excluded if they had >1 physical illness at the time of recruitment into the study. Overall, 508 eligible children were identified, of which 294 consented to participate and 263 were enrolled.
Procedure
Research assistants worked with health professionals to identify eligible children and families. Clinic nurses introduced the study to families and invited them to speak with the research assistant after their medical appointment. The research assistant then verified eligibility, described the study, and obtained written permission from eligible individuals to be contacted further about participating in the study. The study coordinator then contacted parents to schedule a time for in-person data collection at the hospital (n = 200) or family home (n = 53), or in some cases, study packages were mailed (n = 9). Data were collected using structured interviews and self-reported questionnaires on laptops (or paper for mail packages). Parent reports were collected for all children, and children aged ≥10 years provided self-reports. Informed consent (parent and children aged 16 years) and assent (children aged 7–15 years) was obtained. Parents consented on behalf of children who were ≤6 years. Approval was obtained from the Waterloo Human Research Ethics Board and Hamilton Integrated Research Ethics Board.
Measures
Six-month mental illness in children was measured using the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID), a structured clinical diagnostic interview aligned with the ICD-10 and Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 by trained research staff. 21 It has been shown to be valid and reliable in clinical and population samples. 22 The most common mental illnesses present in childhood and adolescence were assessed: major depressive episode (MDE), generalized anxiety disorder (GAD), separation anxiety disorder (SAD), social phobia (SoP), specific phobia (SpP), attention-deficit/hyperactivity disorder (ADHD), oppositional defiant (ODD), and conduct disorder (CD). 16 Because all child participants in the sample had a physical illness, children were classified as having multimorbidity if they screened positive for ≥1 mental illness in the past six months.
The 12-item World Health Organization Disability Assessment Schedule (WHODAS) 2.0 was used to measure child disability and functioning in the domains of cognition, mobility, self-care, getting along, life activities, and participation. 23 Higher scores on the WHODAS 2.0 indicate more impairment. Its psychometric properties, including its factor structure, construct validity, and reliability are sound in child and adolescent populations, including those with physical or mental illness. Tompke et al. 24 and Kimber et al. 25 have reported on validity/reliability in 15–19 year-olds, and our own unpublished work indicates validity/reliability in 2–16 year-olds26–28 (for further details regarding psychometric properties in these younger children, readers may reach out via personal communication to the research team). Its internal consistency was α = 0.87 in our sample. Height and weight were measured by research assistants using a stadiometer and digital scale, respectively, and body mass index percentiles for age and sex were used to classify children by weight status. 29 The Kaufman Brief Intelligence Test (2nd edition) was administered to children ≥4 years of age and its composite score used to classify children by intelligence quotient. 30
Given the influence of parent/family health on child mental illness, particularly in the context of child multimorbidity,13,31 measures of parental psychopathology and family functioning were collected. The 20-item Center for Epidemiological Studies Depression Scale (CESD) and 7-item Generalized Anxiety Disorder (GAD7) were administered to parents. The CESD measures depressive symptoms across the domains of depressed affect, positive affect, somatic activity, and interpersonal relations. 32 It has been extensively validated and its internal consistency was α = 0.92. The GAD7 measures seven core symptoms of generalized anxiety and has been shown to be valid and reliable. 33 Its internal consistency was α = 0.88. The 18-item Parental Stress Scale (PSS) measures four domains of parenting: rewards, stressors, loss of control, and satisfaction. 34 It has been shown to be valid and reliable in parents of children with physical illness. 35 Its internal consistency was α = 0.85. The general functioning subscale of the McMaster Family Assessment Device (FAD) was used to measure aspects of communication, problem solving, behavioral control, affective responsiveness and involvement, and roles in the family. 36 Its psychometric properties are robust 37 and its internal consistency was α = 0.85. Higher scores for the CESD, GAD7, and PSS indicate more parental psychological distress; for the FAD, higher scores indicate better family functioning.
Socioeconomic characteristics measured in the sample included parental education, relationship status, and household income as <$90,000 or ≥$90,000; which represents the gross median income of households with >1 persons. 38 A summary of the measures are shown in Table 1.
Summary of Study Measures.
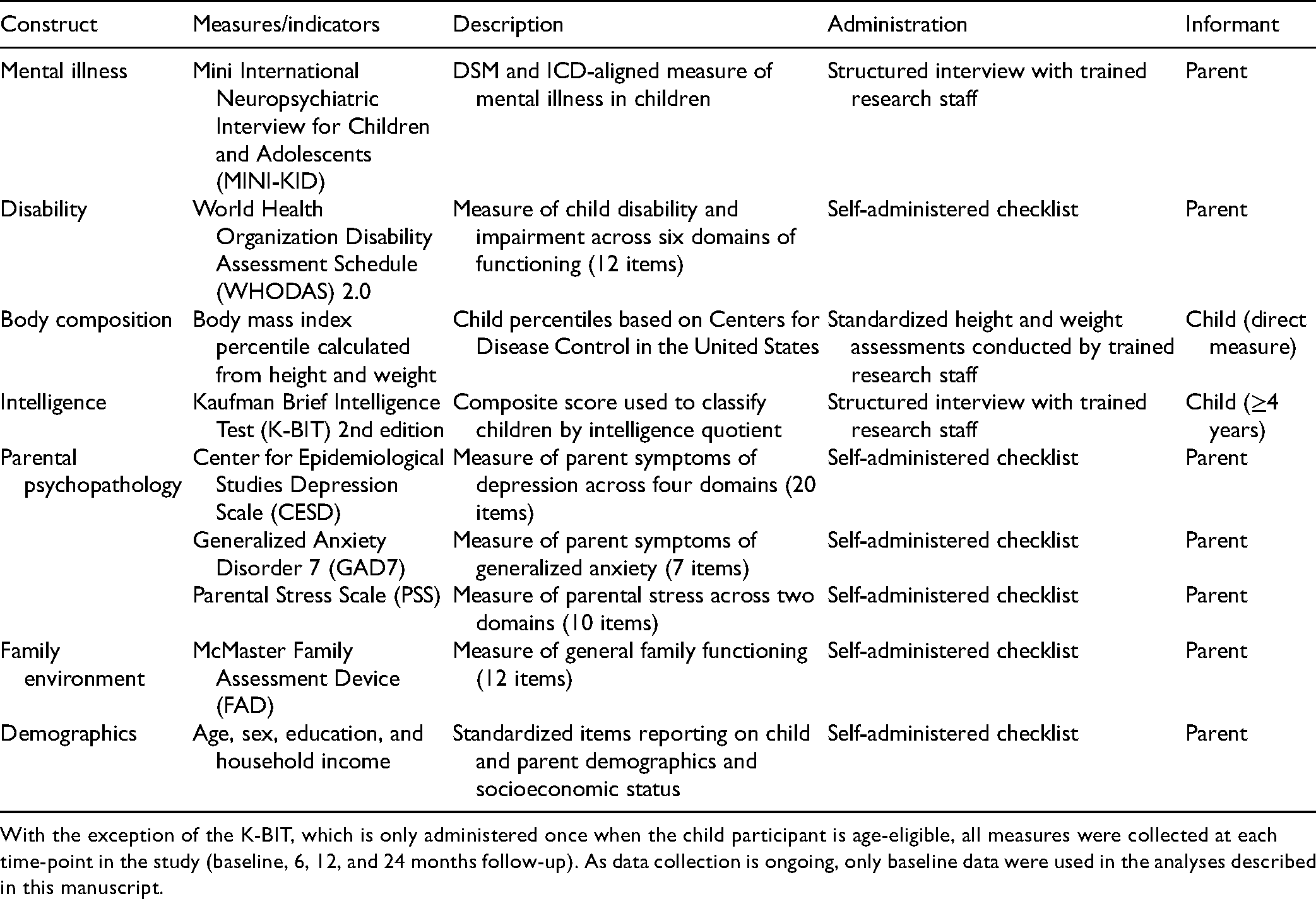
With the exception of the K-BIT, which is only administered once when the child participant is age-eligible, all measures were collected at each time-point in the study (baseline, 6, 12, and 24 months follow-up). As data collection is ongoing, only baseline data were used in the analyses described in this manuscript.
Analysis
Sample characteristics were computed overall and across ICD-10 categories of physical illnesses using ANOVA or χ2 tests, with post hoc testing when a statistically significant overall association was found. Prevalence of mental illness was estimated and compared across ICD-10 physical illnesses using χ2 tests. Kappa was used to estimate agreement between parent and child reports of mental illness. Logistic regression models were computed to identify factors associated with multimorbidity. Four models were created with variables added in blocks according to type of illness, demographic, clinical, and parent/family mental health. Model c-statistics were presented as an indicator of fit, where c≥0.70 is considered good. 39 Ordinal regression models were computed to identify factors associated with the number of child mental illnesses, categorized as 0, 1, or ≥2. Odds ratios (OR) and 95% confidence intervals (CI) were generated for all models. There were no missing exposure or outcome data; however, n = 51 children had missing illness duration, body mass index, or intelligence quotient. Inferences from regression models were unchanged when these variables were removed; thus, fully-adjusted models are presented using complete cases (n = 212). Correlation between parental depression (CESD) and anxiety (GAD7) scores was high (r = 0.77). Thus, only CESD was included in the models. Fit was better with CESD versus GAD7 and associations were similar for either variable and associations of other variables were unchanged. Analyses were completed using SAS 9.4.
Results
Sample Characteristics
The mean age of children enrolled in the study was 9.2 (SD 4.2) years and 53% were male. The mean time since physical illness onset was reported by parents as 4.5 (SD 4.1) years. As shown in Table 2, based on the WHODAS 2.0, the mean disability score was 7.3 (SD 6.8). Most children had average BMI and intelligence (65% for both). Significant differences were found for child age, sex, immigrant status, level of disability, and duration of physical illness onset across ICD-10 categories.
Sample Characteristics.
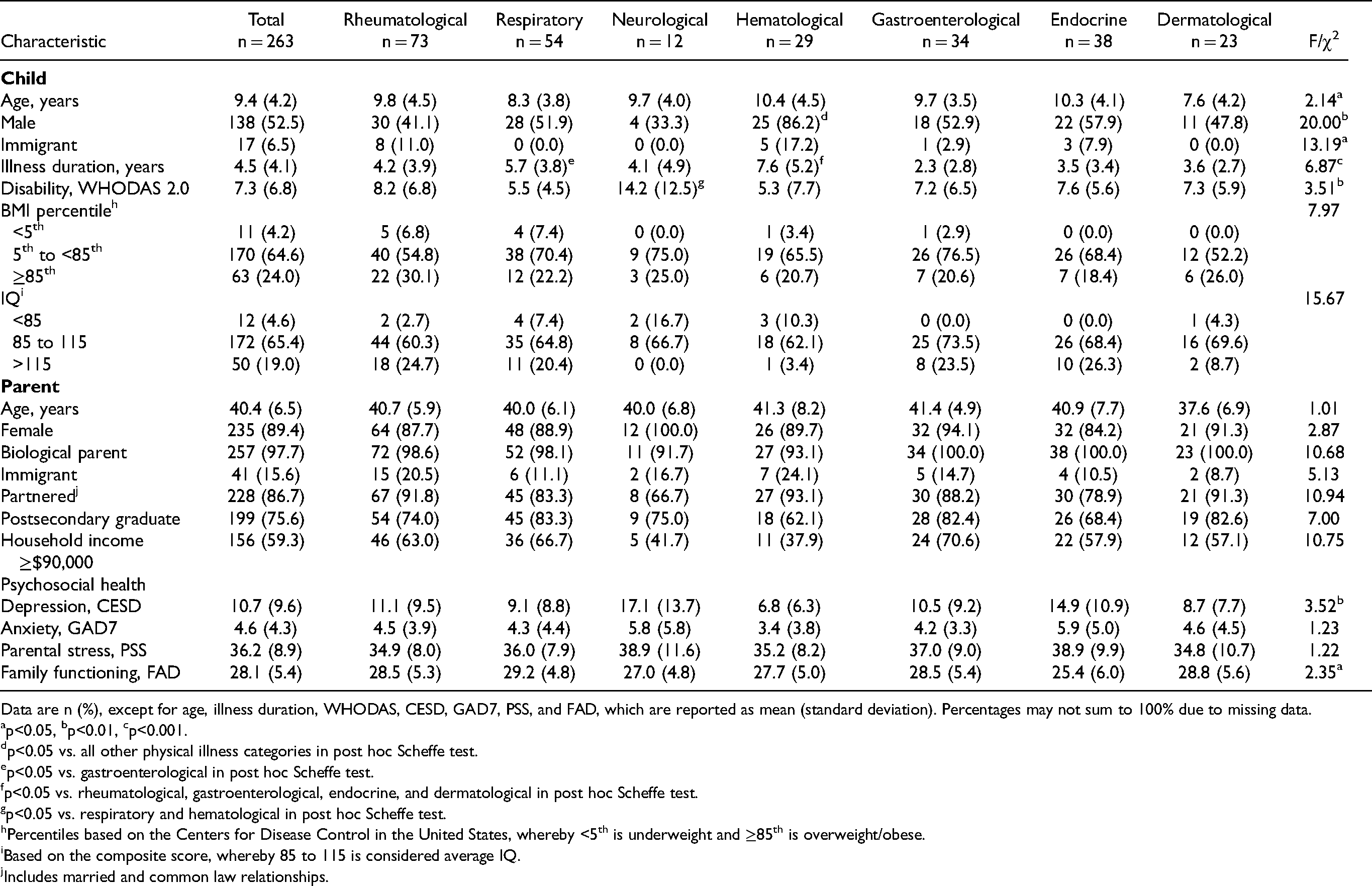
Data are n (%), except for age, illness duration, WHODAS, CESD, GAD7, PSS, and FAD, which are reported as mean (standard deviation). Percentages may not sum to 100% due to missing data.
p<0.05, bp<0.01, cp<0.001.
p<0.05 vs. all other physical illness categories in post hoc Scheffe test.
p<0.05 vs. gastroenterological in post hoc Scheffe test.
p<0.05 vs. rheumatological, gastroenterological, endocrine, and dermatological in post hoc Scheffe test.
p<0.05 vs. respiratory and hematological in post hoc Scheffe test.
Percentiles based on the Centers for Disease Control in the United States, whereby <5th is underweight and ≥85th is overweight/obese.
Based on the composite score, whereby 85 to 115 is considered average IQ.
Includes married and common law relationships.
The mean age of parents was 40.4 (SD 6.5) years, with most being the biological mother of the participating child (89%). Parents generally had high socioeconomic status: 87% were partnered, 76% completed postsecondary education, and 59% had a household income of ≥ $90,000. Overall, tests suggested significant differences in CESD and FAD scores across ICD-10 categories; however, post hoc tests showed no specific pairwise differences (Table 2).
Prevalence of Multimorbidity
According to parent reports, 101 (38%) of children screened positive for mental illness in the past six months (Table 3). The most common internalizing disorder was GAD (11%) and externalizing disorder was ADHD (16%). There were no significant differences in parent-reported mental illness across ICD-10 categories or data collection location (χ2 = 2.2; p = 0.339). Among children who had parent-reported six-month mental illness, 56 (55%) had one mental illness, 27 (27%) had two, and 18 (18%) had three or more. The distribution of the number of mental illnesses across ICD-10 categories was similar (χ2 = 15.7; p = 0.614).
Prevalence of Mental Illness by Informant.
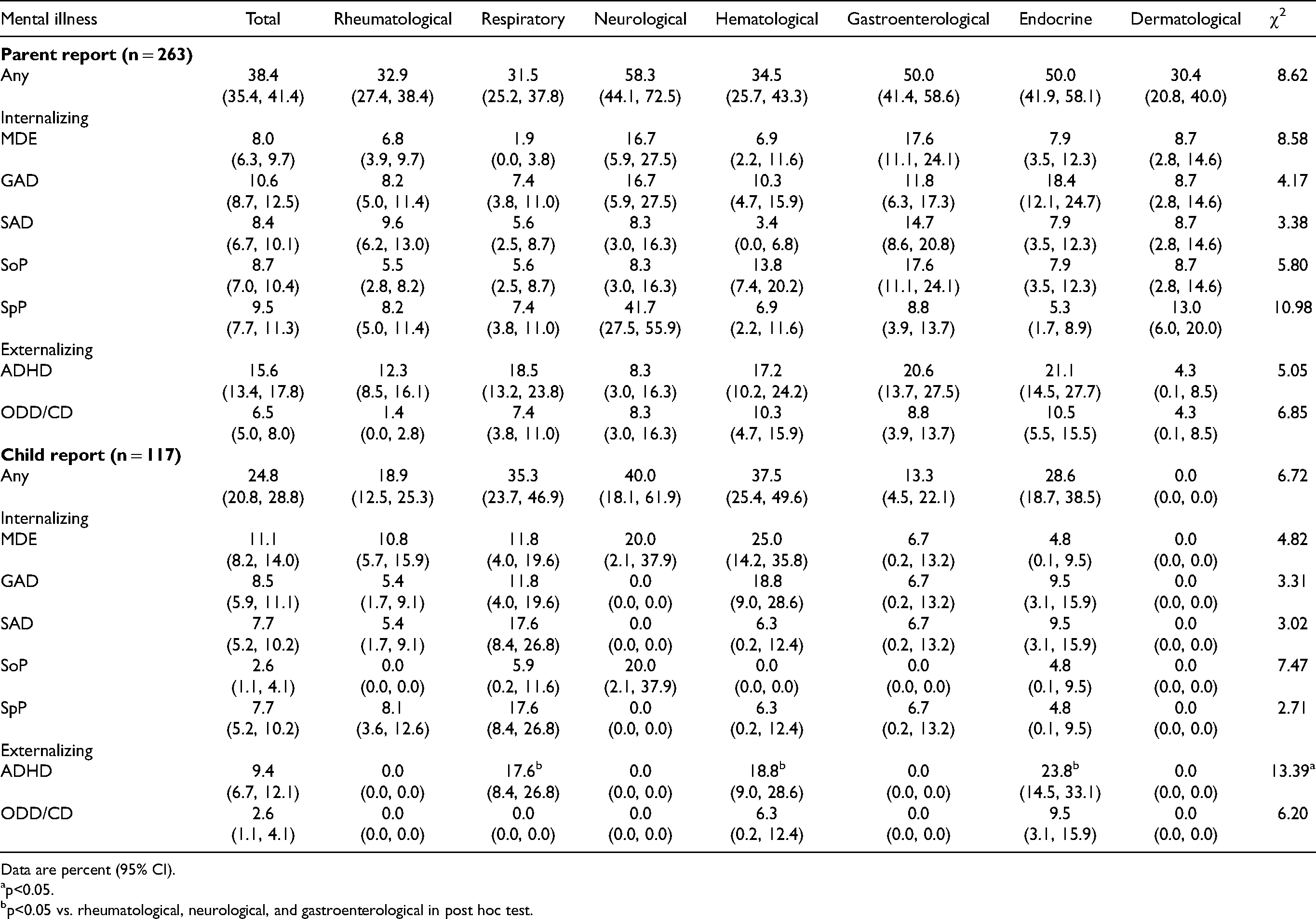
Data are percent (95% CI).
p<0.05.
p<0.05 vs. rheumatological, neurological, and gastroenterological in post hoc test.
Of the children who were age-eligible to provide self reports (age ≥10 years), 29 (25%) had screened positive for mental illness in the past six months, the most common being MDE and ADHD at 11% and 9%, respectively. Among these children, 12 (41%) had one mental illness, 10 (35%) had two, and 7 (24%) had three or more. Consistent with parent reports, there were no differences in the number of mental illnesses across ICD-10 categories (χ2 = 13.37, p = 0.690).
In contrast, 48 (41%) of children aged ≥10 years had a parent-reported mental illness in the past six months, with GAD and ADHD being the most common at 14% and 15%, respectively. Significant differences across ICD-10 categories for child-reported ADHD were found, though may have been due to multiple zero-counts.
Agreement between parents and children ≥10 years for any six-month mental illness was poor overall (κ = 0.18). Mental illness-specific agreement was MDE κ = 0.22, GAD κ = 0.05, SAD κ = 0.20, SoP κ = 0.04, SpP κ = 0.24, ADHD κ = 0.03, and ODD/CD κ = 0.04.
Factors Associated With Multimorbidity
Data reported in Table 4 showed no evidence to suggest that the type of physical illness in children was associated with six-month multimorbidity. Rather, level of disability was the only clinical factor that correlated with multimorbidity in children, such that a one-unit increase on the WHODAS 2.0 was associated with a 21% increase in odds of multimorbidity over the past six months (OR = 1.21, [1.13–1.30]). Higher odds of multimorbidity were found in children who were older, male, and come from households with incomes ≥ $90,000. Parental stress and family functioning were not found to be associated with child multimorbidity. Children whose primary caregiving parent had elevated CESD scores were more likely to have multimorbidity; a one-unit increase in the CESD corresponded to a 9% increase in odds of multimorbidity over the past six months (OR = 1.09, [1.03–1.14]).
Models of Multimorbidity (Parent Report).
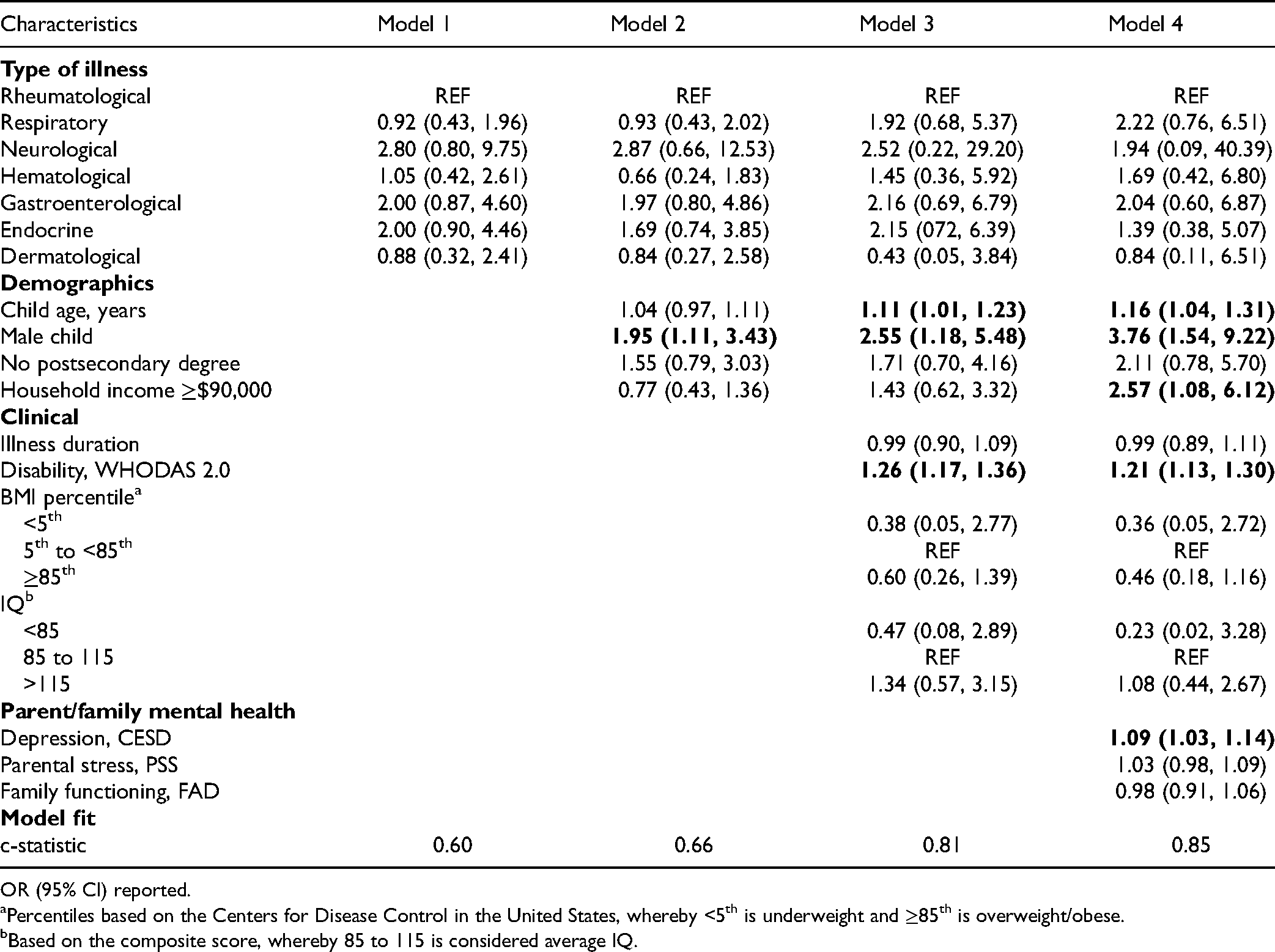
OR (95% CI) reported.
Percentiles based on the Centers for Disease Control in the United States, whereby <5th is underweight and ≥85th is overweight/obese.
Based on the composite score, whereby 85 to 115 is considered average IQ.
Similar results were found when modeling the number of six-month mental illnesses present in children (Table 5); no evidence was found for associations between the type of physical illness and the number of mental illnesses. Higher WHODAS 2.0 scores were associated with an increase in the number of mental illnesses experienced over the past six months (OR = 1.15 [1.08, 1.22]). Male children had increased odds of a higher number of mental illnesses (OR = 3.84 [1.75, 8.45]), as were those whose parents had elevated CESD scores (OR = 1.09 [1.05, 1.15]).
Models of Number of Mental Illnesses (Parent Report).
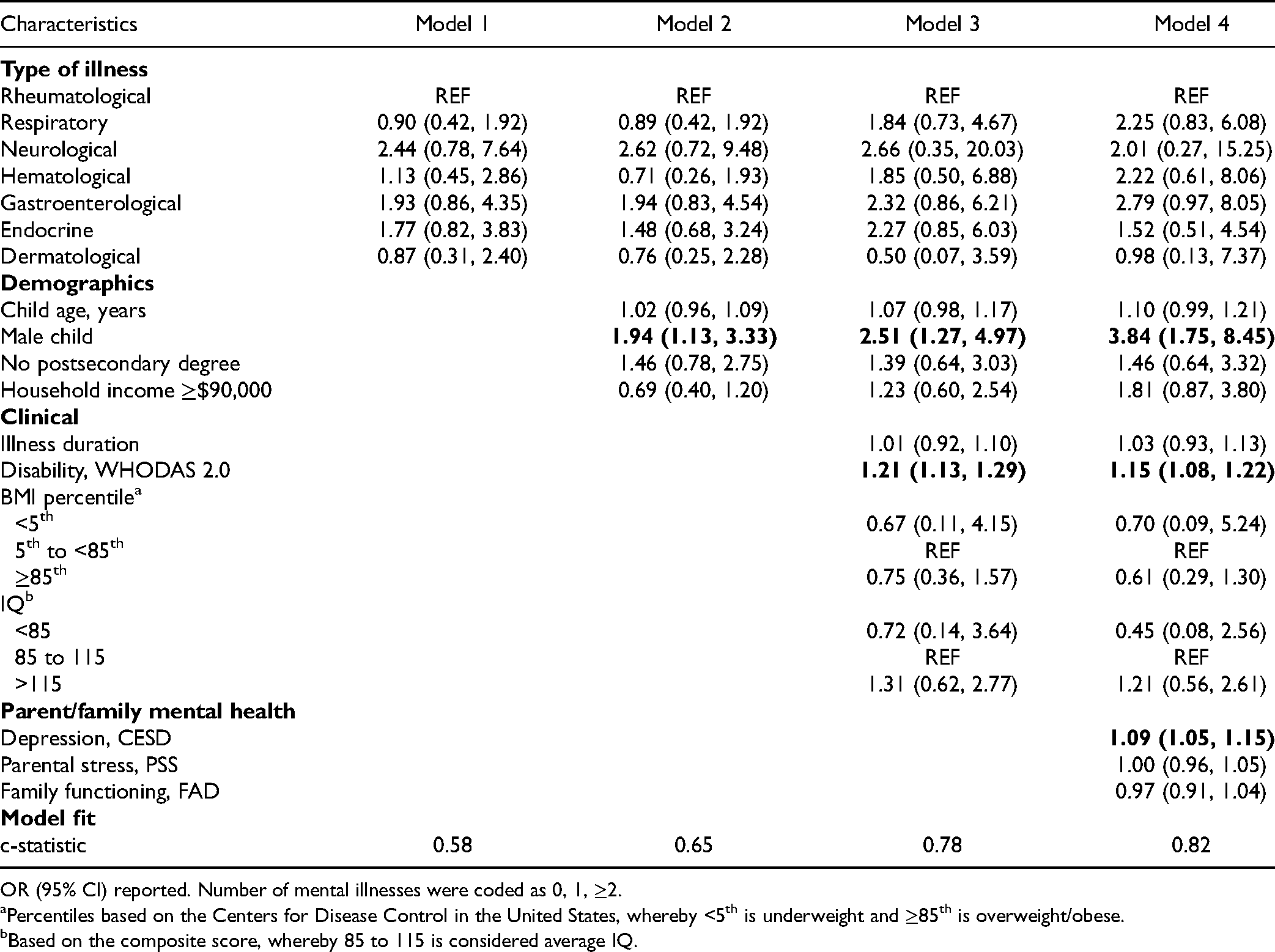
OR (95% CI) reported. Number of mental illnesses were coded as 0, 1, ≥2.
Percentiles based on the Centers for Disease Control in the United States, whereby <5th is underweight and ≥85th is overweight/obese.
Based on the composite score, whereby 85 to 115 is considered average IQ.
Discussion
Six-month mental illness in children with chronic physical illness attending outpatient clinics at a pediatric hospital is common and frequently characterized by the presence of multiple mental illnesses. Six-month multimorbidity is similar across different physical illnesses, is more common among older children, males, those with higher levels of disability, children who come from higher income households, and those who have a primary caregiver with elevated symptoms of depression.
Compared to the population estimate in Canada (18%), 16 the prevalence of mental illness is more common among children with physical illness (20–35%). 3 Our findings are consistent with other clinical samples (25–58%),6,10,11 supporting observations that outpatient children represent a vulnerable population and positions child multimorbidity as a pressing health priority. Indeed, 5% of children (most with multimorbidity) account for nearly two-thirds of pediatric health service costs in Canada. 40 Routine screening for mental health concerns soon after the diagnosis of physical illness and attention to early intervention is needed to prevent or minimize the burden of multimorbidity on children, families, and the health system. Models of care that integrate physical and mental health systems are well positioned to meet the complex service needs of these children. 41 Successful integration of systems should ensure collaboration and care-related decision-making involves the child and their family, as well routine evaluation of services ensure targets to reduce the incidence of child multimorbidity are met. 42
Agreement between parent and child reports of six-month mental illness was low, but consistent with previous reports of children in the general population or those with mental illness in the clinical setting.16,43 Our findings suggest that the context of childhood physical illness does not influence parent and child perspectives of mental illness in this clinical sample. Use of multiple informants for mental health surveillance and comprehensive assessments should remain standard practice for children with physical illness in outpatient settings. Research investigating how agreement may change over time during the course of the physical illness or whether agreement differs across developmental periods (i.e. early childhood, late adolescence) will be examined within the MY LIFE cohort once data collection is completed. Such work is relevant to for health professionals to help foster communication within families to ensure these children and their parents successfully transition from pediatric to adult health services, at which time children, now young adults, will bear a greater responsibility in their medical decision-making.
Findings support the adoption of using the non-categorical approach to studying child multimorbidity and is consistent with findings from previous population and clinical samples of children, adolescents, and young adults.2,6,14,44 Other clinical, biological, and psychosocial factors, such as changes in illness severity/impairment, stress responses and dysregulation, inflammatory processes, family environment, and parent-child relations, inherent to most childhood physical illnesses may represent the mechanisms that underlie the causal links between physical and mental illness.13,45,46 This shared risk across physical illnesses facilitates broad, or universal, implementation of surveillance, prevention, and treatment strategies for children; the feasibility and effectiveness of which has been examined and reported to be acceptable. 47
Further affirming this non-categorical approach, level of disability was associated with six-month child multimorbidity in this clinical sample. Disability, particularly when measured using the WHODAS 2.0, may be a useful indicator of multimorbidity for health professionals to quickly, and routinely, examine children who may require additional assessment. With its brevity, ease of measurement, relatively large effect size, and amenability to be modified, disability may be a key target for intervention to prevent or reduce the incidence of multimorbidity in children and adolescents in outpatient settings. However, interrelationships among physical and mental illness and disability are complex, and causal mechanisms are not definitive. Evidence supports disability as a predictor and outcome of mental illness, as well as showing disability mediating the bidirectional association of physical and mental illness.48–50
Six-month multimorbidity was more likely in older children—a finding consistent with our hypothesis and evidence that most mental illnesses have their initial onset in adolescence. 51 Contrary to our hypothesis, but consistent with findings from a recent population study, 52 males were more likely to have multimorbidity. While this finding may be a function of over-representation of males with externalizing disorders (primarily ADHD), resilience may also be implicated. Evidence shows that resilience may be lower in males compared to females. 53 This may represent gendered expectations for children whereby boys are expected to be physically active (e.g., through participation in sports), which is associated with improved mental health. 53 However, due to their physical illness, they may unable to do so, thus contributing negatively to their mental health. In contrast, mood and anxiety disorders may be more likely to be triggered by the stress and functional limitations associated with a physical illness affecting both genders similarly.
Our hypothesis regarding household income was also not supported and contradicts previous findings. 52 It is possible that higher income (a proxy for higher socioeconomic status) is associated with increased mental health literacy 54 and thus parents were more likely to recognize symptoms of recent/current mental illness in their children. Lastly, our findings reaffirm the robust association between parent and child mental health and the need to ensure that family-centred approaches to care are adopted and remain implemented for children with multimorbidity. 42 Responding to the mental health needs of parents may reduce the odds of child multimorbidity in outpatient settings. 13
There are noteworthy limitations to this study. First, the use of cross-sectional data barred any conclusions about causality. Second, relatively small physical illness subgroups may have resulted in tests that were underpowered and prevented the ability to compare specific diagnoses (e.g., epilepsy vs. colitis); thus, our findings supporting the non-categorical approach are not definitive. Third, our sample was generally homogenous and took place in a nation where health care is universally available. Ethical approval to collect information on non-participants was not obtained and thus comparisons with the study sample could not be conducted. Fourth, the recruitment of families from a single pediatric hospital using convenience sampling may not adequately represent the experience of this population, including those not accessing health services from a tertiary care setting. Fifth, the exclusion of children with >1 physical illness likely resulted in underestimating multimorbidity in the target population; thus, findings cannot be generalized to this subgroup of children. Finally, the limited number of child informants prevented the modeling of child-reported mental illness.
Conclusion
Findings of this study conducted in outpatient clinics of a pediatric hospital suggest that six-month multimorbidity is common, is similar across different physical illnesses, and that these children often have multiple mental illnesses. Disability, as measured by the WHODAS 2.0, is a robust correlate of multimorbidity and can be used as part of routine surveillance by health professionals for children with physical illness. Initiating early mental health intervention, through integrated physical and mental health services, is paramount in reducing the incidence of child multimorbidity and promoting overall health in children, particularly in outpatient hospital settings.
Footnotes
Acknowledgments
The authors gratefully acknowledge the children, parents, and health professionals and their staff at McMaster Children's Hospital without whose participation this study would not have been possible. We especially thank Jessica Zelman, Robyn Wojicki, and Charlene Attard for coordinating the study and Melissa Elgie and Sophie Rosen for assisting with data collection.
Data Access
Ethical approval was not obtained for the sharing of study data. Individual requests for data access can be made to the corresponding author and will be considered by the study team on a case-by-case basis.
Conflict of Interest Statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ferro serves on the editorial board of the Canadian Journal of Psychiatry. None of the remaining authors has a conflict of interest to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant awarded to Dr. Ferro by the Canadian Institutes of Health Research (PJT-148602). Dr. Ferro is the recipient of an Early Researcher Award from the Ontario Ministry of Research, Innovation and Science. Drs. Ferro, Van Lieshout, and Timmons are supported by the Canada Research Chairs Program.