
Abstract
Objective
Formal thought disorders (FTDs), a core feature of schizophrenia, have been subdivided into positive and negative types, and are clinically assessed by examining speech (objective) or patient introspection (subjective). Despite being associated with poorer treatment response and worse outcomes, FTDs have been understudied in patients with schizophrenia, in particular treatment-resistant schizophrenia (TRS) or schizoaffective disorder. We aimed to explore the relationship between the severity of positive and negative FTDs and neurocognition as well as social/occupational functioning in this clinical subgroup.
Method
This was a retrospective chart review conducted at the Clozapine Clinic at the Centre for Addiction and Mental Health, Toronto, Canada. We reviewed charted standardized assessment of FTDs using the Thought and Language Disorder (TALD) scale, neurocognition using the Brief Cognitive Assessment Tool for Schizophrenia (B-CATS), and functioning using the Social and Occupational Functioning Assessment Scale (SOFAS) between October 2022 and June 2023. Following the original factor structure of the TALD, we computed 4- factor scores that combined positive or negative and objective or subjective FTDs. We then explored the correlation between the scores from each TALD factor and the neurocognition and functioning scores.
Results
We analysed data for 23 outpatients on clozapine. After the Bonferroni adjustment, total TALD scores, indicating overall severity of FTDs, were strongly and inversely correlated with SOFAS scores (p < 0.001). A strong inverse correlation was found between the objective positive TALD factor and Letter-Number Span verbal working memory scores, r(21) = −0.63, p < 0.001.
Conclusions
Our results demonstrate the strong relationship between FTDs, neurocognition, and social/occupational functioning in a sample of TRS outpatients. Within the cognitive domains assessed, verbal working memory impairment had the strongest correlation with positive FTDs, such as derailment or tangentiality. These findings highlight the value of employing standardized psychopathological scales for FTDs in clinical practice.
Introduction
Formal thought disorders (FTDs) comprise a group of abnormalities in thought form, language production, and communication.1,2 Objective FTDs are observable on clinical examination of speech, distinguishing them from subjective FTDs, which are disturbances in thought flow and communication experienced subjectively by the individual and reported to the examiner.3,4 FTDs have been further subdivided into positive and negative. Positive FTDs include derailment, tangentiality, and pressured speech, indicating an excess or distortion of thought processes and speech. Conversely, negative FTDs indicate a deficit in thought and speech production, as represented by poverty of speech, slowed thinking, or blocking.5,6 These psychopathologies are thought to be integral to the clinical syndrome of schizophrenia.7–9 FTDs can also be found in other neuropsychiatric syndromes, including mania and epilepsy; however, they tend to be more persistent in patients with schizophrenia.10,11 In addition, the presence and severity of FTDs may be predictive of treatment-resistant schizophrenia (TRS)12–14 TRS describes a subgroup of patients with schizophrenia who continue to suffer from positive symptoms after 2 or more trials of antipsychotic medications, 15 and has been proposed as a distinct subtype of schizophrenia.16,17 Patients with TRS have been found to have more severe neurocognitive deficits compared to other patients with schizophrenia. 18
The cognitive mechanism underlying FTDs is not fully understood. Nevertheless, it has been hypothesized that FTDs may be a manifestation of neurocognitive deficits which are commonly found in patients with schizophrenia.19,20 Both executive dysfunction, which impacts high-order cognition such as working memory, and semantic network impairment, which influences aspects of verbal fluency, have been linked to the etiology of FTDs in schizophrenia.21,22 Furthermore, it has been found that performance on executive functioning tests can better differentiate schizophrenia patients with and without FTDs compared to their performance on semantic tests. 23 These findings support the role of neurocognitive mechanisms in FTDs, particularly the hypothesis that impairments in executive functions that govern planning, editing, and monitoring of thoughts underlie the pathogenesis of clinically assessed FTDs. 24
Given the paucity of literature on the relationship between FTDs and neurocognitive measures in TRS, and the association of TRS with more severe FTDs and neurocognitive deficits, we aimed to investigate this relationship in this clinical population. Accordingly, our primary objective was to explore the relationship between the severity of positive and negative, objective and subjective, FTDs and neuropsychological test scores in patients with TRS. Our secondary objective was to investigate the relationship between FTD severity and social as well as occupational functioning.
Methods
This was a retrospective chart review that received approval from The Centre for Addiction and Mental Health (CAMH) Research Ethics Board on November 6, 2023. The review included patients in the Clozapine Clinic at CAMH, Toronto, Canada, who have undergone an assessment of FTDs and neuropsychological testing as part of their outpatient care during the period from October 1, 2022, until June 1, 2023. Consent for data collection was not obtained from the participants as the collected data were anonymized and had been charted as part of routine clinical care. The waiver of consent was approved by the CAMH Research Ethics Board. Psychopathology and functional assessments were completed as a component of good clinical practice by the covering psychiatrists (MA and reviewed with SMA) whereas the neuropsychological tests were completed independently by trained nursing staff in the clinic (LB and VP). The data were collected from the patient's electronic medical records and included clinico-demographic characteristics (e.g., sex, age, and diagnosis) in addition to psychopathological, neuropsychological, and functional assessment scores.
Psychopathology Assessment
FTD severity is commonly assessed using clinician-rated scales. 25 Most rating scales, however, do not adequately address subjectively reported FTDs, which constitute an important but neglected aspect of FTDs.26,27 Kircher et al. 28 reviewed the literature and existing FTD scales, and with this as background developed the 30-item Thought and Language Disorder (TALD) scale to introduce a more comprehensive tool for the assessment of objectively observed and subjectively reported FTDs. 28 The TALD is a reliable and valid tool for the assessment of FTDs and correlates strongly with other measures of schizophrenia psychopathology including other scales that measure FTDs. Due to these advantages, the scale was adopted to assess FTD severity in our Clozapine Clinic. The scale was completed for each patient following at least a 50 min psychiatric interview during which psychopathologies were explored and clarified. Following the scale manual, objective FTDs were rated based on their presence and impact on communication during the interview. Subjective FTDs, on the other hand, were explored using semistructured questions to determine their presence and severity during the preceding 24 h based on the associated distress. Each item on the scale was given a score: 0 not present, 1 doubtful, 2 mild, 3 moderate, and 4 severe according to the scale manual. In addition, all included patients were assessed using the 24-item Brief Psychiatric Rating Scale Expanded Version (BPRS-E), 29 utilizing the anchor scores, which assign a score for reported and observed psychopathologies between 1 and 7. 30
Neurocognition and Social/Occupational Functioning Assessment
Neurocognition was assessed by the Letter-Number Span test for verbal working memory, semantic (categorical) and phonological (letter) fluency tasks for verbal fluency, and the symbol coding test for cognitive processing speed. For the verbal fluency tasks, the category used was animals, and the letters were “F” and “S.” These neuropsychological tests are part of the Brief Cognitive Assessment Tool for Schizophrenia (B-CATS),31,32 which explores similar domains to and correlates highly with the MATRICS Consensus Cognitive Battery, 33 considered to be the gold-standard assessment tool of neurocognition in schizophrenia. Social and occupational functioning was assessed using the Social and Occupational Functioning Assessment Scale (SOFAS). 34
Inclusion and Exclusion Criteria
Inclusion criteria included being able to communicate in English, age 18 to 65, capacity to undergo neuropsychological testing, and a clinical diagnosis of schizophrenia or schizoaffective disorder, according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, with treatment resistance to 2 or more antipsychotics documented on clinical charts. Exclusion criteria included a diagnosis of moderate or severe intellectual disability, major or minor neurocognitive disorder such as Alzheimer's or unspecified dementia, and moderate to severe substance use disorders. Patients for whom neurocognitive assessment using the B-CATS was not documented within 3 months of FTD assessment were excluded. All but 2 of the included patients underwent neuropsychological testing on the same visit FTDs were assessed.
Data Analysis
Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS), Version 21.0. 35 Descriptive data were obtained through the means (M), standard deviations (SD), and frequencies (f). Medians (Mdn) and interquartile ranges (IQRs) were used for nonnormally distributed variables. Correlations were estimated using Pearson's correlation coefficient (r) for normally distributed continuous variables and the nonparametric Spearman's rank correlation coefficient (rs) for nonnormally distributed continuous variables. We followed the original factor structure of the TALD in computing the factor scores. 28 This factor structure included 4 factors: objective positive (15 items), objective negative (3 items), subjective positive (2 items), and subjective negative (7 items) FTDs. Each factor's relative score was obtained by dividing the sum of the individual scores by the number of items in each factor. 36 These factor scores have been utilized in other studies using the TALD.37,38 The internal consistency reliability of the factors was estimated by Cronbach's alpha using SPSS. Cronbach's alpha ranges from 0 to 1 with higher values indicating stronger relationships between the included items in each factor. The total BPRS-E score was calculated by adding the scores of the individual 24 items. As for the B-CATS, a total score was obtained by summing the score of the Letter-Number Span, Semantic (categorical) Verbal Fluency, Phonological Verbal Fluency (letter F), Phonological Verbal Fluency (letter S), and Symbol Coding test scores. Total Verbal Fluency was calculated by summing the 3 semantic and phonological fluency scores. To account for multiple bivariate analyses, a Bonferroni adjustment was applied to the level of significance to yield a level of significance when p < 0.0017 (0.05 out of 30).
Results
Clinico-Demographics
Out of 126 patients enrolled in the Clozapine Clinic, 23 patients met the inclusion criteria, having undergone the standardized assessment during the period from October 1, 2022, until June 1, 2023. Clinico-demographic data are summarized in Table 1. There were more male than female patients in our sample and the patients’ age ranged from 23 to 65 years. All patients in the sample were prescribed clozapine, and the majority were receiving clozapine monotherapy or cotreatment with antidepressants for depressive, anxiety, or obsessive–compulsive symptoms. None of the patients were receiving an adjunct Long-Acting Injectable antipsychotic.
Clinico-Demographics and Descriptive Analysis of Psychopathological, Neurocognitive, and Functional Assessment Scores (N = 23).
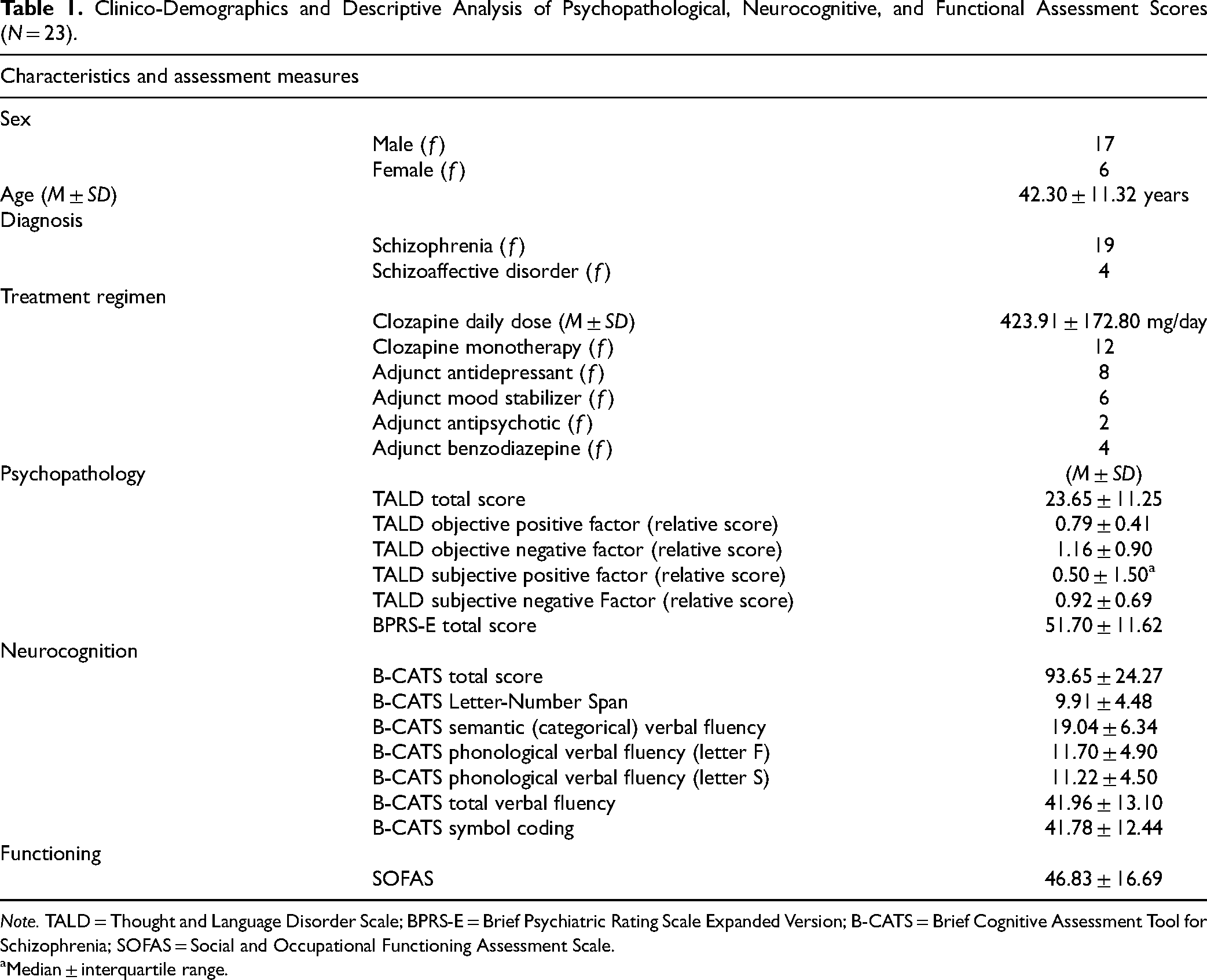
Note. TALD = Thought and Language Disorder Scale; BPRS-E = Brief Psychiatric Rating Scale Expanded Version; B-CATS = Brief Cognitive Assessment Tool for Schizophrenia; SOFAS = Social and Occupational Functioning Assessment Scale. aMedian ± interquartile range.
FTDs Assessment
We analysed the frequency of individual TALD items in our sample. The most frequently encountered FTDs as mild, moderate, or severe were “poverty of content of speech” (f = 17) followed by “poverty of speech” and “tangentiality” (both f = 13). Clanging and echolalia were not encountered at all and were therefore excluded from the bivariate analysis along with verbigeration, which was only encountered in 1 patient. Figure 1 illustrates the frequency of formal thought and language disorders scored as mild, moderate, or severe according to the scale manual and grouped based on the factor structure of the TALD.
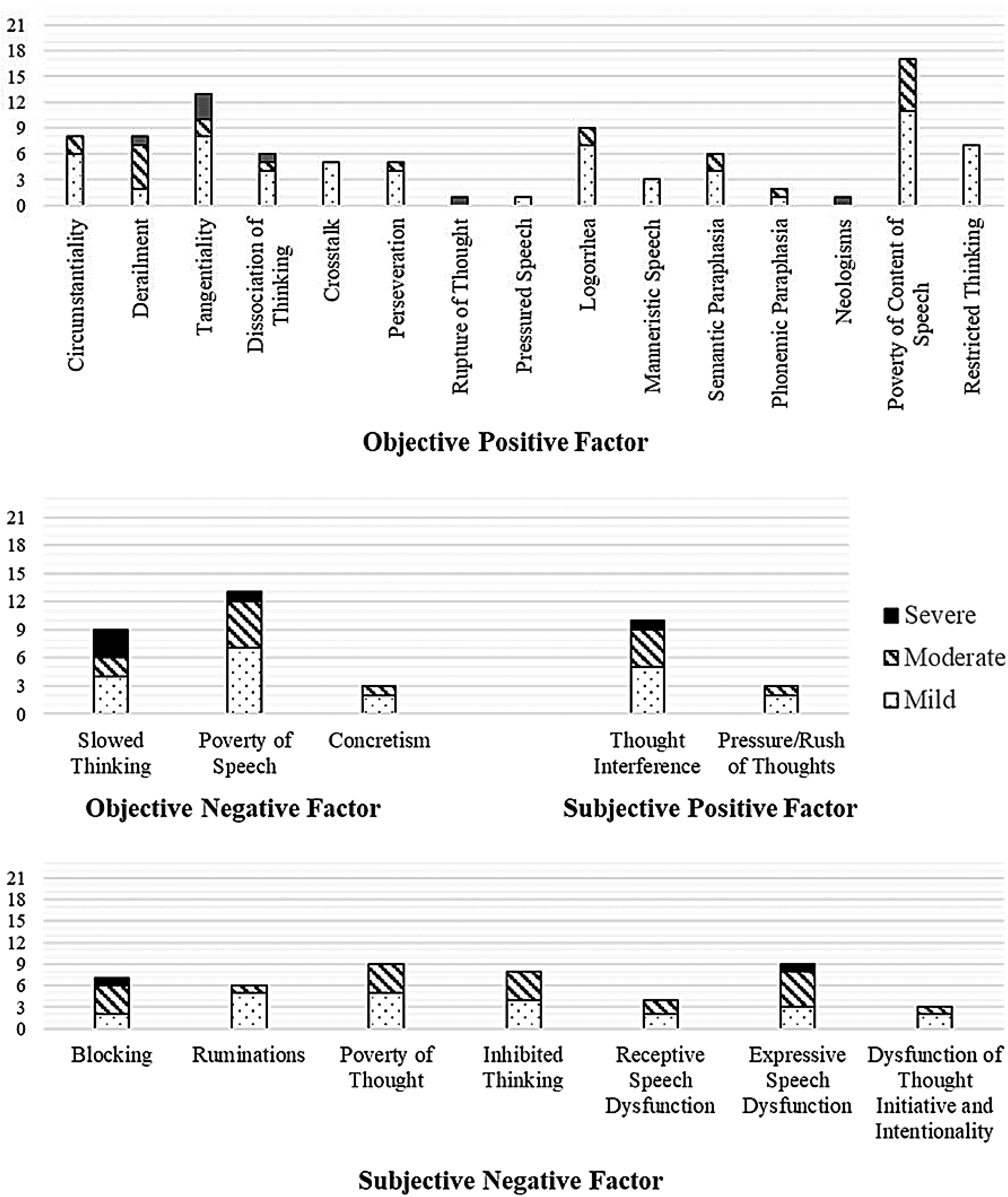
Frequency of formal thought and language disorders by Thought and Language Disorder Scale (TALD) items (N = 23): The TALD items have been grouped into 4 categories based on the factor structure of the scale. 28 Verbigeration, clanging, and echolalia have been excluded.
Psychopathological Assessment Scores
Table 1 shows the descriptive analysis of psychopathological (TALD and BPRS-E), neurocognitive (B-CATS), and functional (SOFAS) assessment scores. The total TALD score provided an assessment of the general severity of FTDs for each patient. The total score ranged from 10 to 54 points. Estimating the internal consistency of the total TALD scale yielded a Cronbach's alpha of 0.78. Using the factor structure of the TALD, we calculated the relative score of positive and negative, objective and subjective, FTDs as 4 distinct factor scores. The Cronbach's alpha was 0.65 for the objective positive factor, 0.57 for the objective negative, 0.79 for the subjective positive, and 0.71 for the subjective negative factor. All factors followed a normal distribution except for the subjective positive TALD factor. The highest average relative scores were for the objective negative factor of the TALD, followed by the subjective negative factor (Table 1). The TALD total score and relative factor scores for each patient are detailed in Appendix 1. Male patients averaged higher scores on the subjective positive factor than female patients (t(20.99) = 2.92, p = 0.008). Otherwise, male and female patients had comparable scores on the TALD and its factors (p > 0.05). Total BPRS-E scores ranged from 32 to 74. Male patients had more severe psychopathologies, as assessed by the total BPRS-E (M = 55.12, SD = 10.82), compared to female patients (M = 42.00, SD = 8.17), t(21) = 2.70, p = 0.014. There were no significant differences in psychopathology scores between patients on different drug regimens (p > 0.05).
Neurocognitive and Functional Assessment Scores
For neurocognitive measures, the minimum B-CATS total score was 44 and the maximum was 153. We did not find any differences between male and female patients on any of the B-CATS measures (p > 0.05). There was an inverse trend between age and the Letter-Number Span score, r(21) = −0.52, p = 0.011. The level of functioning, as scored by the SOFAS, ranged from 75 (indicating some difficulty in social, occupational, or school functioning but generally functioning well) to a score of 20 (which indicates inability to function independently and occasionally failing to maintain minimal personal hygiene). We did not find a difference between male and female patients in SOFAS scores (p > 0.05).
Bivariate Analysis
The bivariate analysis is detailed in Table 2, which shows the correlation coefficients of psychopathological, neurocognitive, and functional assessment scores in our sample. Overall, more severe FTDs, as scored by the TALD total score, were correlated with lower total B-CATS scores. After the Bonferroni adjustment, however, the only significant correlation between TALD factors and neuropsychological test scores was found for the objective positive factor and the Letter-Number Span verbal working memory, r(21) = −0.63, p < 0.001. Figure 2A shows a scatterplot of objective positive TALD factor scores by the Letter-Number Span verbal working memory scores, demonstrating the strong inverse correlation. More severe psychopathology, as assessed by total BPRS-E scores, was strongly and inversely correlated with both total B-CATS scores and Symbol Coding processing speed scores. Higher TALD and BPRS-E total scores were both strongly correlated with lower functional assessment scores. Figure 2B illustrates the relationship between total TALD scores and SOFAS scores.
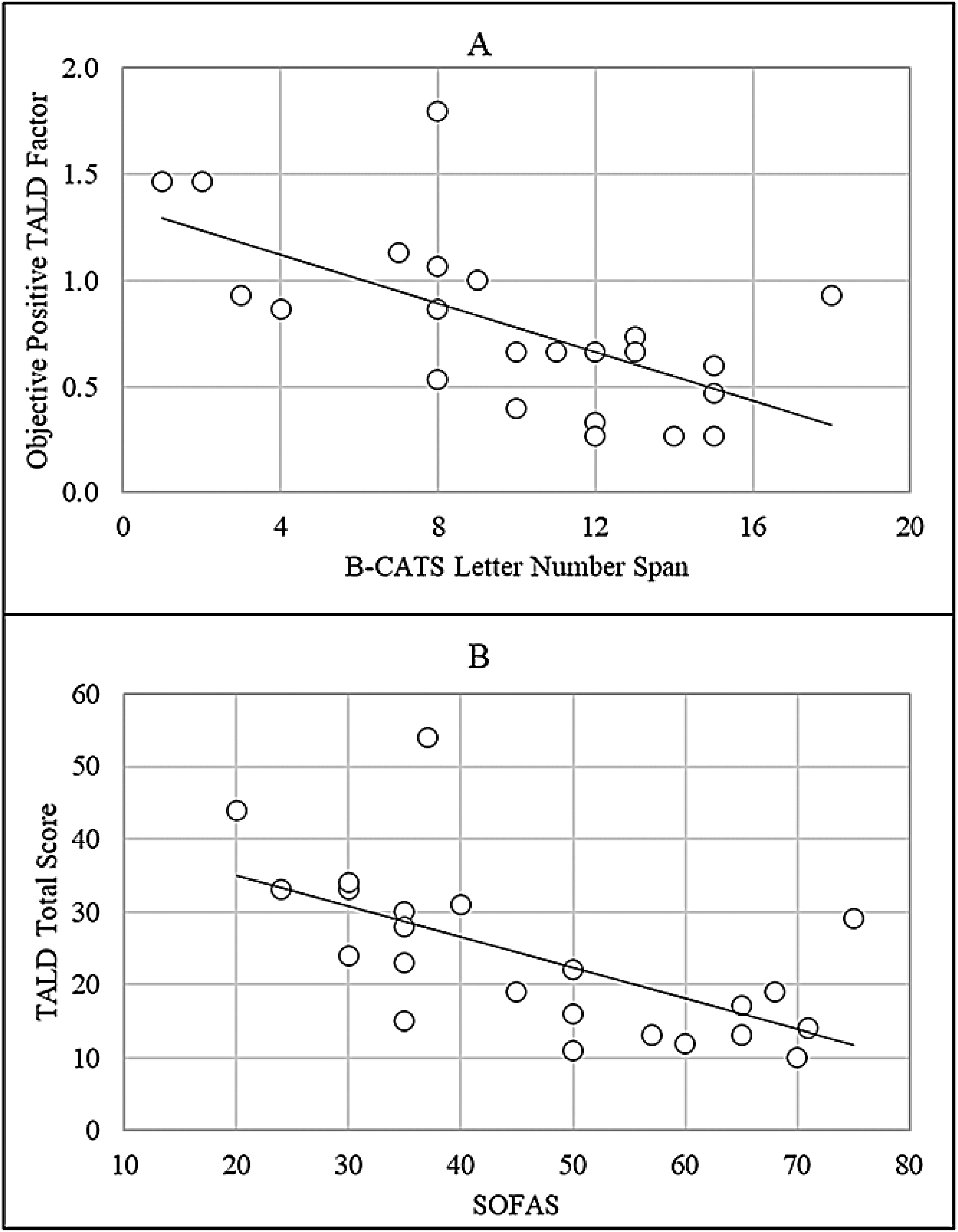
Relationship between formal thought and language disorders, verbal working memory, and functional assessment scores. (A) Scatterplot of objective positive TALD factor scores by the B-CATS Letter-Number Span verbal working memory test scores. (B) Scatterplot of total TALD scores by SOFAS scores.
Correlation Coefficient Matrix Between Formal Thought and Language Disorders, Neurocognition, and Functional Assessment Scores:.
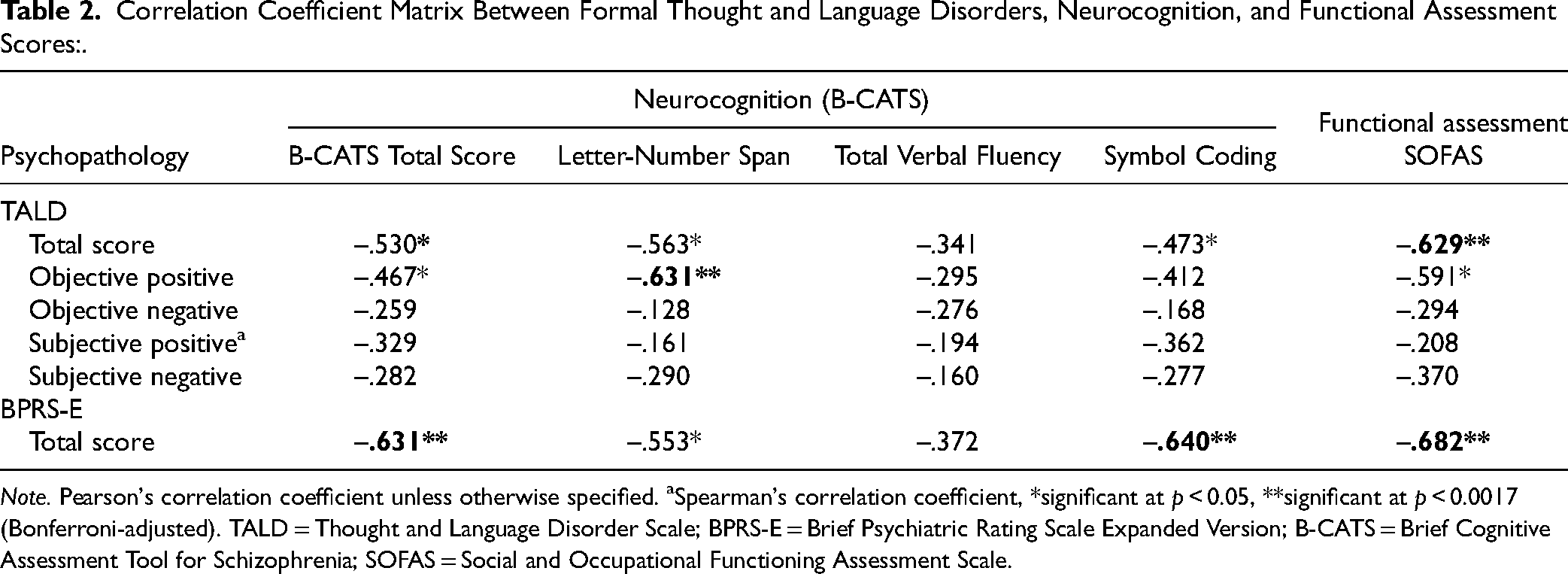
Note. Pearson's correlation coefficient unless otherwise specified. aSpearman's correlation coefficient, *significant at p < 0.05, **significant at p < 0.0017 (Bonferroni-adjusted). TALD = Thought and Language Disorder Scale; BPRS-E = Brief Psychiatric Rating Scale Expanded Version; B-CATS = Brief Cognitive Assessment Tool for Schizophrenia; SOFAS = Social and Occupational Functioning Assessment Scale.
Discussion
This chart review examined the relationship between FTD severity and neurocognitive measures in a sample of outpatients with TRS. Our results demonstrate the relationship between neurocognition and severity of FTDs in schizophrenia. We found a strong inverse correlation between verbal working memory and objectively assessed positive FTDs such as derailment, tangentiality, or poverty of content of speech. Moreover, the overall severity of FTDs was associated with worse social and occupational functioning. These findings are discussed in the context of the existing literature on FTDs and their relationship to neurocognitive measures in schizophrenia.
The relationship we found between FTDs and neuropsychological test scores is in line with the literature investigating symptom domains and their relationship to neurocognition. Indeed, a large meta-analysis of studies has shown that neurocognition is more linked to disorganization than to other positive symptoms such as delusions or hallucinations. 39 This further justifies positioning FTDs as distinct from other positive symptoms, in line with numerous factor analyses separating disorganization from reality distortion.40–42
We did not find a relationship between FTDs and semantic or verbal fluency test scores, in contrast to published reports on the link between semantic memory and FTDs in schizophrenia. For example, the severity of FTDs has been correlated with semantic memory deficits. 43 Horn et al. 44 compared the difference between patients with schizophrenia and normal controls in the semantic network on functional magnetic resonance imaging and found that these differences correlated with increasing severity of FTDs. The nonsignificant correlation between semantic verbal fluency and FTDs in our sample could be due to the small sample size or low variability in performance.
However, in the current study, we found a strong correlation between objectively assessed positive FTDs and verbal working memory, a correlation not found for other neurocognitive domains in our sample. This finding aligns with the existing literature implicating executive dysfunction as underlying positive FTDs. For example, executive functioning was more closely associated with improvement in FTDs than semantic function in a sample of patients with first-episode schizophrenia or schizoaffective disorder. 45 Moreover, executive dysfunction at the onset of schizophrenia was found to be predictive of FTD persistence after 1 year of follow-up. 46 Furthermore, currently available evidence from neuroimaging studies does not indicate that aberrations in the brain's language network are specific to FTDs in schizophrenia, nor does it rule out the relevance of other brain regions to these psychopathologies. 47 Could executive dysfunction be the underlying abnormality affecting patients’ performance on verbal fluency tasks? It has been suggested that semantic fluency impairment itself might be explained by executive dysfunction in working memory, which, in turn, affects cognitive search and retrieval strategies in patients with schizophrenia. 48 However, this finding is challenged by evidence showing that executive functioning in schizophrenia is not related to semantic memory function as assessed by semantic fluency tasks. 49
What about the relationship between neurocognitive measures and subdivisions of FTDs? In a systematic review of reports on 2805 patients, Bora et al. 50 investigated the correlates of FTDs in schizophrenia and found that executive dysfunction correlated with both positive and negative FTDs. They found that deficits in working memory and planning correlated with both types of FTDs, while fluency deficits were only associated with negative FTDs. The correlation between positive FTDs and working memory was found in our sample, but not the relationship between negative FTDs and verbal fluency impairments.
Our results demonstrate the relationship between social and occupational functioning and severity of FTDs. In turn, FTD severity has been previously linked to measures of real-world outcomes.51,52 In addition to predicting lower social and occupational functioning, FTDs have been shown to predict more frequent relapses and rehospitalizations.53,54 Moreover, previous studies have found that negative FTDs and their severity are associated with poorer treatment response and worse long-term outcomes.55,56 In our sample, however, the relationship between subjective negative FTDs, such as blocking, and functioning was moderate but not significant.
The limitations of this chart review include its retrospective design and small sample size. A convenience sampling strategy was used based on suitability and availability to undergo the standardized assessment during routine clinical care. In addition, the associations are based on cross-sectional assessments. The sample contained more male patients than female, which may have influenced our results. Despite these limitations, our findings support the value of standardized psychopathological assessments as part of good clinical practice. In our sample of TRS outpatients, the current analysis demonstrated a strong relationship between FTDs, neurocognition, and social and occupational functioning. Particularly, the results show how the overall severity of FTDs in patients with TRS is correlated with lower functional assessment scores, and that impairment in verbal working memory is strongly correlated with more severe positive FTDs. Large, longitudinal studies are needed to shed light on how the relationship between FTDs and neurocognition evolves over time in patients with TRS.
Footnotes
Acknowledgements
We are grateful to all staff working in the clozapine clinic at CAMH for their efforts in implementing measurement-based care.
Data Access
Anonymized datasets used and analysed in the current study can be requested by contacting the corresponding authors.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SMA has served as a consultant for HLS Therapeutics and Boehringer Ingelheim Canada. GR has received research support through HLS Therapeutics.
Funding
MA is supported by SABIC Psychological Health Research and Applications Chair, Department of Psychiatry, College of Medicine, Deanship of Post Graduate Teaching, King Saud University, and the Saudi Arabian Cultural Mission in Canada. SMA is supported, in part, by an Academic Scholars Award from the Department of Psychiatry, University of Toronto and the CAMH Discovery Fund.
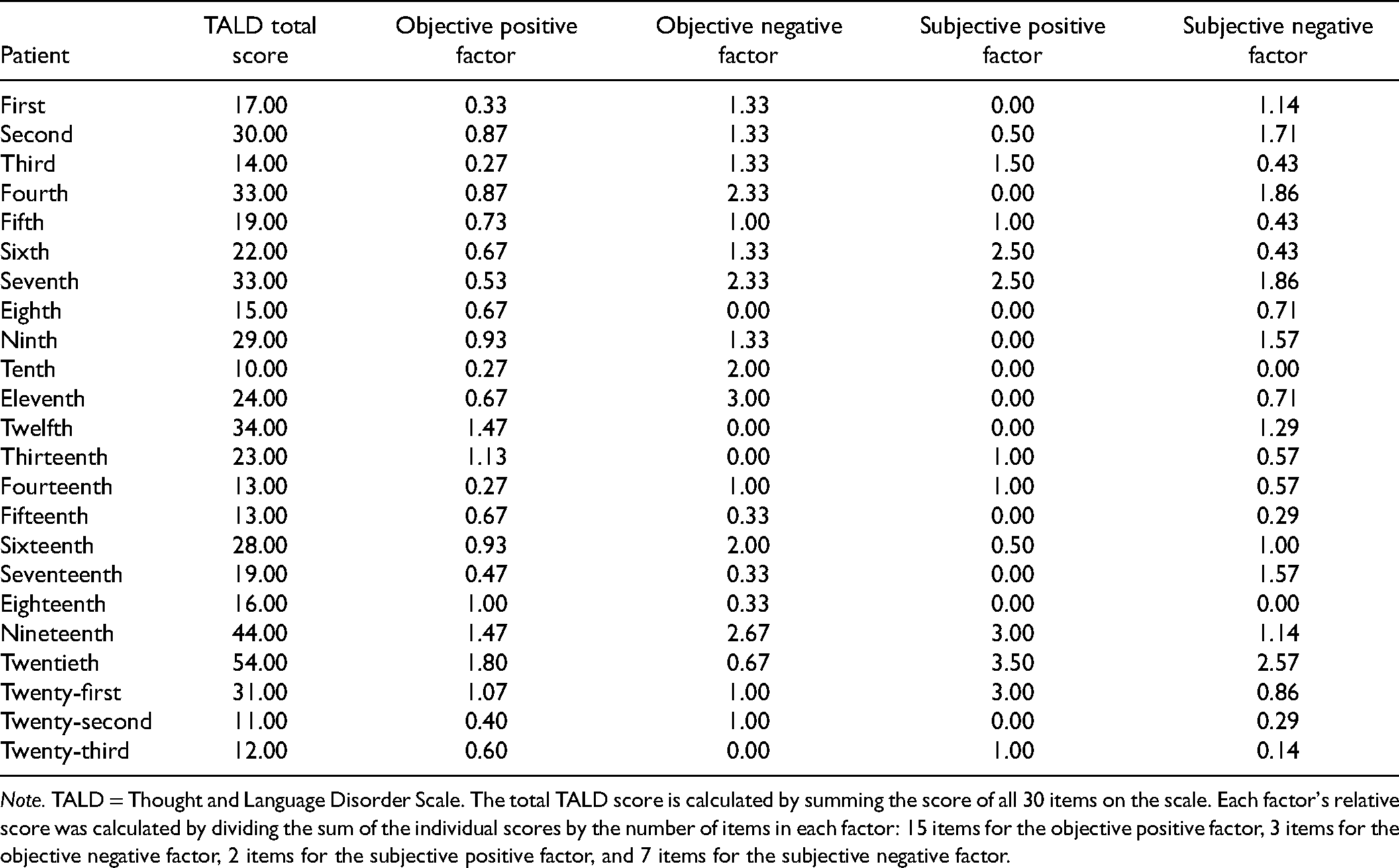
Appendix 1. TALD Total Score and Relative Factor Scores by Patient ( N = 23).
| Patient | TALD total score | Objective positive factor | Objective negative factor | Subjective positive factor | Subjective negative factor |
|---|---|---|---|---|---|
| First | 17.00 | 0.33 | 1.33 | 0.00 | 1.14 |
| Second | 30.00 | 0.87 | 1.33 | 0.50 | 1.71 |
| Third | 14.00 | 0.27 | 1.33 | 1.50 | 0.43 |
| Fourth | 33.00 | 0.87 | 2.33 | 0.00 | 1.86 |
| Fifth | 19.00 | 0.73 | 1.00 | 1.00 | 0.43 |
| Sixth | 22.00 | 0.67 | 1.33 | 2.50 | 0.43 |
| Seventh | 33.00 | 0.53 | 2.33 | 2.50 | 1.86 |
| Eighth | 15.00 | 0.67 | 0.00 | 0.00 | 0.71 |
| Ninth | 29.00 | 0.93 | 1.33 | 0.00 | 1.57 |
| Tenth | 10.00 | 0.27 | 2.00 | 0.00 | 0.00 |
| Eleventh | 24.00 | 0.67 | 3.00 | 0.00 | 0.71 |
| Twelfth | 34.00 | 1.47 | 0.00 | 0.00 | 1.29 |
| Thirteenth | 23.00 | 1.13 | 0.00 | 1.00 | 0.57 |
| Fourteenth | 13.00 | 0.27 | 1.00 | 1.00 | 0.57 |
| Fifteenth | 13.00 | 0.67 | 0.33 | 0.00 | 0.29 |
| Sixteenth | 28.00 | 0.93 | 2.00 | 0.50 | 1.00 |
| Seventeenth | 19.00 | 0.47 | 0.33 | 0.00 | 1.57 |
| Eighteenth | 16.00 | 1.00 | 0.33 | 0.00 | 0.00 |
| Nineteenth | 44.00 | 1.47 | 2.67 | 3.00 | 1.14 |
| Twentieth | 54.00 | 1.80 | 0.67 | 3.50 | 2.57 |
| Twenty-first | 31.00 | 1.07 | 1.00 | 3.00 | 0.86 |
| Twenty-second | 11.00 | 0.40 | 1.00 | 0.00 | 0.29 |
| Twenty-third | 12.00 | 0.60 | 0.00 | 1.00 | 0.14 |
Note. TALD = Thought and Language Disorder Scale. The total TALD score is calculated by summing the score of all 30 items on the scale. Each factor's relative score was calculated by dividing the sum of the individual scores by the number of items in each factor: 15 items for the objective positive factor, 3 items for the objective negative factor, 2 items for the subjective positive factor, and 7 items for the subjective negative factor.