
Abstract
Objectives
The aetiology of mental disorders involves genetic and environmental factors, both reflected in family health history. We examined the intergenerational transmission of multiple mental disorders from parents and grandparents using population-based, objectively measured family histories.
Methods
This population-based retrospective cohort study used administrative healthcare databases in Manitoba, Canada and included adults living in Manitoba from 1977 to 2020 with linkages to at least one parent and one grandparent. Index date was when individuals turned 18 or 1 April 1977, whichever occurred later. Mental disorder diagnoses (mood and anxiety, substance use and psychotic disorders) were identified in individuals, parents and grandparents from hospitalization and outpatient records. Cox proportional hazards regression models included sociodemographic characteristics, individual's comorbidity and mental disorder history in a grandparent, mother and father.
Results
Of 109,359 individuals with no mental disorder prior to index date, 47.1% were female, 36.3% had a mental disorder during follow-up, and 90.9% had a parent or grandparent with a history of a mental disorder prior to the index date. Both paternal and maternal history of a mental disorder increased the risk of the disorder in individuals. Psychotic disorders had the strongest association with parental history and were mostly influenced by paternal (hazards ratio [HR] 3.73, 95% confidence interval [CI] 2.99 to 4.64) compared to maternal history (HR 2.23, 95% CI, 1.89 to 2.64). Grandparent history was independently associated with the risk of all mental disorders but had the strongest influence on substance use disorders (HR 1.42, 95% CI, 1.34 to 1.50).
Conclusions
Parental history of mental disorders was associated with an increased risk of all mental disorders. Grandparent history of mental disorders was associated with a small risk increase of the disorders above and beyond parental history influence. This three-generation study further highlights the need for family-based interventional programs in families affected by mental disorders.
Plain Language Summary Title
The Intergenerational Transfer of Mental Illnesses
Plain Language Summary
Objectives
Both genetics and environmental factors, such as poverty, maltreatment and parental education, have a role in the development of mental illnesses. Some genetic and environmental risk factors for mental illnesses are shared within families. We conducted a large study to test the extent to which mental illnesses are passed down through generations.
Methods
This study used healthcare data from Manitoba, Canada captured during the delivery of healthcare services for administrative purposes. These data included all adults from 1977 to 2020 who had at least one parent and one grandparent with linked data. Mental illnesses were diagnosed in individuals, parents and grandparents by doctors during hospitalizations or physician visits. The illnesses included mood and anxiety, substance use, and psychotic illnesses. We estimated the likelihood of developing a mental illness when parents and/or grandparents had a mental illness as well.
Results
The study included 109,359 individuals; a third developed a mental illness during the study period. The majority had a history of a mental illness in a parent or grandparent. We found that a history of mental illness in a mother and father increased the chance of developing the illness. Psychotic illnesses had the strongest relation with parental history. In particular, having a father with a psychotic illness increased the chance of developing the illness by four times. The likelihood of developing a mental illness was higher if a grandparent had a mental illness, above and beyond parental history influence, particularly for substance use disorders.
Conclusions
Having a parent or grandparent with a mental illness increases an individual's chance of developing a mental illness. Family-based intervention programs are needed to support families affected by mental illnesses in coping with their heavy burden.
Introduction
Mental disorders are a group of conditions affecting emotion, thinking and behaviour. Worldwide, 970 million people were diagnosed with mental disorders in 2019, with an age-standardized prevalence of 12.3%. 1 It is projected that by 2041, one in five Canadians, about 9 million individuals, will be living with a mental disorder. 2 Mental disorders are associated with long-term adverse outcomes affecting physical health, education, employment and relationships.3–5 The interaction of multiple genetic and environmental factors contributes to the aetiology of mental disorders. 6 The genetic liability of mental disorders varies by condition: approximately 40% for major depressive and anxiety disorders and up to 80% for schizophrenia.7–14 The remaining portion of the liability of mental disorders is attributed to environmental factors, some of which are shared in families, such as low socioeconomic status, urbanicity and dysfunctional family relationships.15–20 Therefore, family history of mental disorders, which encompasses both genetic and shared environmental risk factors, is a critical component in assessing an individual's risk of developing a mental disorder.
The influence of family history on mental disorder risk has been previously investigated.21–34 However, most previous investigations examined mental health symptoms, self/parent-reported family histories, or were based on small study populations. Therefore, these previous studies were susceptible to information biases, such as recall and social desirability, and poor generalizability.21–27,29–33 Previous population-based studies investigating the familial relationships of mental disorders were limited to history in parents or siblings and did not consider grandparents.28,34,35 Existing evidence on the influence of grandparent history of mental disorders on an individual's risk is scarce and relies on self/parent-reported measures in small cohorts.21,22,36,37 In the Canadian population, most evidence on the parental transfer of mental disorders is limited to small clinical cohorts of high-risk offspring; no previous studies have examined the transfer of mental disorders from grandparents.34,38–41 Therefore, we aimed to examine the association between family history in parents and grandparents and mental disorder risk, in a population-based study using objectively-measured disease definitions. The hypotheses were (1) mental disorder histories in parents and grandparents are associated with mental disorder risk and (2) grandparent history is independently associated with mental disorder risk, above and beyond parental history's influence.
Methods
Design and Setting
This population-based cohort study used administrative healthcare data in Manitoba, Canada, which had a population of 1.3 million as of 2020. 42 Data were derived from the Manitoba Population Research Data Repository housed at the Manitoba Centre for Health Policy from 1 April 1974 to 31 March 2020. 43 All data are de-identified and records are linkable across different datasets using scrambled identifiers. Virtually all Manitobans are included in the Repository and all of their prescription drug dispensations and hospital and outpatient encounters are captured.
Family structures and their temporal changes are available in the Repository through family registration numbers (FRNs), assigned to parents and children living in the same household. FRNs change over time: individuals receive their own numbers at age 18. The FRNs assigned for cohort members at birth were identified. Parents were defined as the male and female adults who shared the same FRNs as the cohort members. Then, the FRNs assigned to the parents at their birth were identified; grandparents were defined as the male and female adults who shared the same numbers as the cohort parents.
We used five datasets from the Repository: Manitoba Health Insurance Registry, Hospital Abstracts, Medical Claims, Drug Program Information Network (DPIN) and Statistics Canada Census. 44 The Registry contains information on all Manitobans registered to receive health coverage since 1970. It was used to create the study cohort, establish the family linkages and obtain individuals’ demographic characteristics. The Hospital Abstracts database contains records of all hospitalization episodes in Manitoba since 1970 and includes up to 25 diagnosis code fields for each hospitalization. Diagnoses were reported using the International Classification of Diseases (ICD) in its eighth revision (ICD-8) until 1979, the ninth revision with clinical modifications (ICD-9-CM) from 1979 to 2004, and the tenth revision with Canadian enhancements (ICD-10-CA) thereafter. Medical Claims contain records of outpatient physician visits since 1970 and diagnoses are coded using ICD-8 until 1979 and ICD-9-CM thereafter. Both Hospital Abstracts and Medical Claims were used to identify mental disorders in individuals and their family members, and individuals’ chronic health conditions. DPIN contains records of drug dispensations in community pharmacies since 1995. DPIN provided an additional source to ascertain mental disorder diagnoses in a sensitivity analysis. Finally, the Statistics Canada Census is a nationwide survey conducted every five years and aggregate demographic information, such as age, income and employment, is reported for dissemination areas. The 2016 Census was used to create income quintiles for individuals based on the dissemination area aggregate household income.
Population
The cohort included individuals who were 18 years or older between 1 April 1977 and 31 March 2020, with linkage to at least one parent and one grandparent in the Registry. The year 1977 was selected to allow time to ascertain mental disorders in family members prior to index date, as such data have been available since 1970. Individuals were required to have at least three years of continuous healthcare coverage prior to and after the index date (the date they turned 18 or 1 April 1977, whichever occurred later). Individuals were excluded if they did not have both a parent and grandparent, each with at least three years of continuous healthcare coverage prior to index date or had a mental disorder diagnosis before the index date. Individuals were followed until a diagnosis of a mental disorder was captured, death, moving out of Manitoba, or the end of study period (31 March 2020), whichever occurred earlier.
Study Measures
Study outcomes were identified in Hospital Abstracts or Medical Claims data using established case definitions for (1) mood and anxiety disorders, (2) substance use disorders, (3) psychotic disorders and (4) any of the three mental disorders. 45 Mood and anxiety disorders included depressive, bipolar and anxiety disorders and were defined as having one or more diagnosis codes in Hospital Abstracts or two or more diagnosis codes in Medical Claims within three years. Substance use disorders, which included drug or alcohol use and psychotic disorders, which included schizophrenia and other psychotic disorders, were defined as having one or more diagnosis codes in Hospital Abstracts or Medical Claims. Supplemental Table S1 lists the ICD codes used to define the mental disorder categories. The exposure of interest was a history of a mental disorder in a mother, father, or grandparent captured prior to index date. Those with missing linkages to a parent or grandparent were assigned an indicator exposure category “missing” in the missing relative.
The sociodemographic covariates ascertained at index date included sex (male, female), decade of birth, region of residence (urban, rural), and income quintile. The latter is an area-level measure of income; the lowest income quintile is defined as Q1 and Q5 designates the highest income quintile. 46 Additional covariates included the number of chronic health conditions diagnosed prior to the index date, based on the Charlson Comorbidity Index (none, one, or two or more). 47 Supplemental Table S2 lists the conditions included in the Charlson Comorbidity Index and their associated ICD codes.
Statistical Analysis
Study cohort characteristics were presented as frequencies and percentages or median values and interquartile ranges, for the entire cohort and stratified by presence of mental disorder. To assess potential selection bias, baseline characteristics between individuals with and without grandparent linkage were compared.
The intergenerational transfer of mental disorders was examined using adjusted Cox proportional hazards regression models, which allows for the censoring of individuals lost to follow-up (i.e., when their health coverage is terminated). Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported. The primary analyses examined the independent association between family history in mothers, fathers and grandparents of each of the investigated mental disorders and the risk of developing that disorder.
Secondary analyses stratified the models by individual's sex to evaluate if the familial relationships in mental disorders are modified by sex. We also examined the independent influence of mental disorder history in maternal compared to paternal grandparents and grandmothers compared to grandfathers on the disorders’ risk. Additionally, we considered the influence of the family history of each mental disorder on the risk of the other mental disorders (i.e., transdiagnostic models). To account for changes in diagnostic criteria and transitions in ICD coding over the study period, which could influence the quality of the study measures over time, we stratified the analysis by birth year: 1960–1969, 1970–1979, 1980–1989, and 1990–2001.
Three sensitivity analyses were conducted. First, we compared the association of parental mental disorder history with individuals’ risk in those with and without grandparent linkage, to examine the potential selection bias. Second, prescription drug dispensations were used as an additional source to capture mood and anxiety and psychotic disorder cases not recorded in hospital and outpatient records. 48 This sensitivity analysis aimed to reduce misclassification in ascertaining mental disorders, and was conducted in a cohort of individuals who were 18 years or older between 2000 and 2020. Finally, to examine whether the method selected for handling missing parental linkages influenced the results, we also evaluated a complete case analysis that excluded individuals with missing linkages to both parents.
All analyses were performed using SAS® version 9.4 (SAS Institute, Cary, North Carolina, United States). This study was approved by the Health Research Ethics Board of the University of Manitoba, and data access was approved by the Manitoba Health Information Privacy Committee.
Results
Cohort Characteristics
Of the source population of 517,293 individuals, 206,182 (39.9%) were missing grandparent linkages. Individuals without grandparent linkage were more likely to be males, urban residents, born earlier, have linkage to fathers, have lower incomes and have a mental disorder diagnosis (Supplemental Table S3). A cohort of 125,070 individuals met the inclusion criteria (Figure 1); 13,277 (10.6%), 3,488 (2.8%) and 831 (0.7%) individuals had a prevalent diagnosis of mood and anxiety, substance use and psychotic disorders, respectively. Those individuals were excluded, resulting in 111,793, 121,582 and 124,239 individuals included in the mood and anxiety, substance use and psychotic disorder analyses, respectively. 15,711 (12.6%) had a diagnosis for any mental disorder prior to index date and were excluded, resulting in 109,359 individuals included in the “any mental disorder” analysis. Of those, 99.1% were linked to mothers and 68.1% to fathers. Individuals without paternal linkages were more likely to be born during the last 10 years of the study period, urban residents and in the lowest income quintile (Supplemental Table S4). The entire cohort was 18 years old at index date; 47.1% were females and 52.8% lived in an urban region (Table 1). 99,434 (90.9%) had a parent or grandparent with a history of a mental disorder during a median observation period of 17.7 years before index date, the majority (85.9%) of which had mood and anxiety disorders. During a median follow-up of 7.7 years, a mental disorder diagnosis was recorded for 39,651 (36.3%) individuals; of those, 18.9% had comorbid mental disorders. Among individuals who developed a mental disorder, mood and anxiety disorder diagnoses were the most frequent (88.2%), followed by substance use disorders (28.3%); only 4.2% developed psychotic disorders. Individuals with a diagnosed mental disorder were more likely to be female, in the lowest income quintile, reside in an urban region, and have a family history of mental disorders.
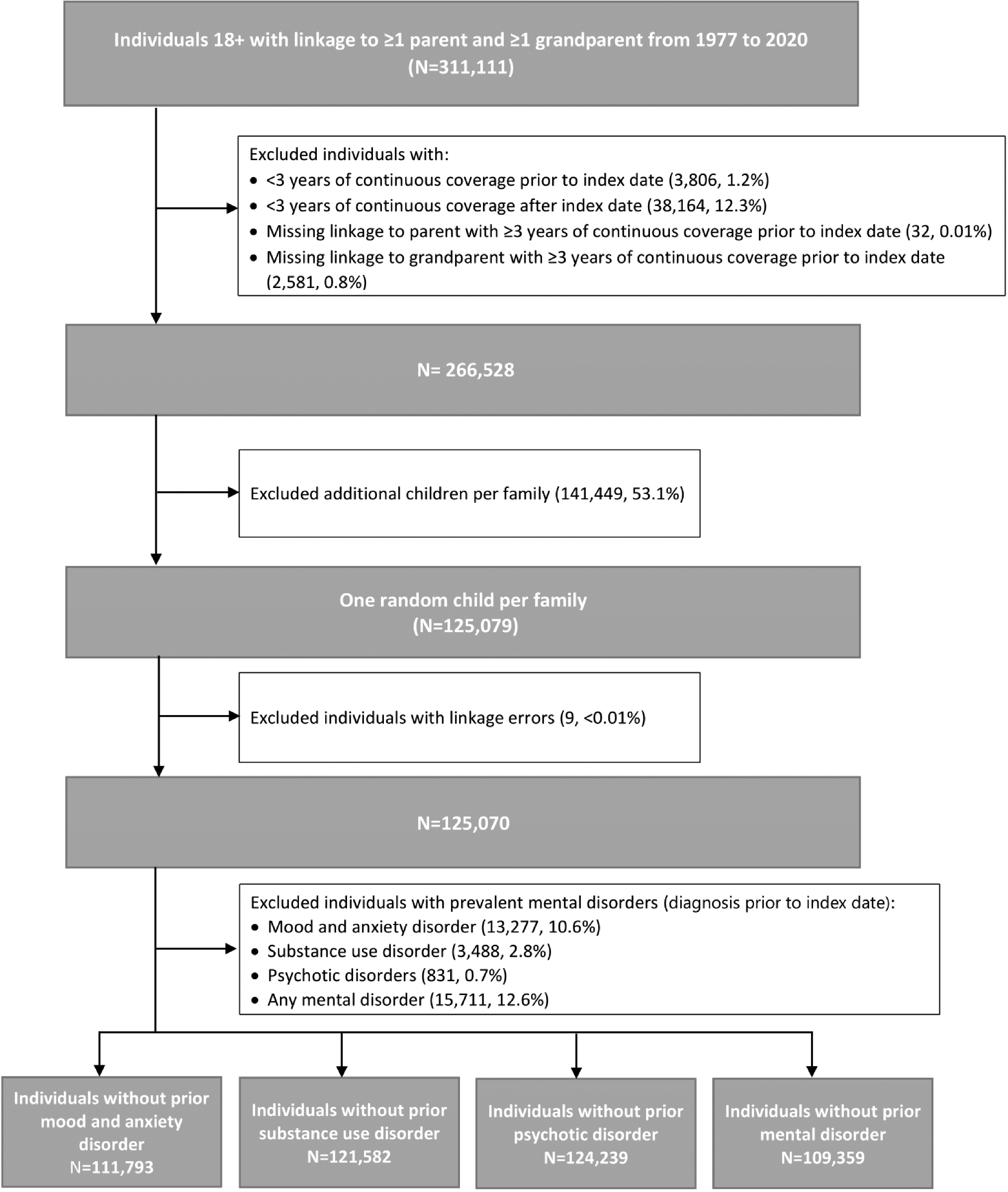
Flow chart for the development of the study cohort consisting of adults living in Manitoba during 1977–2020 with linkage to at least one parent and one grandparent.
Characteristics of the Study Cohort Without Prior Mental Disorder History (N = 109,359), Stratified by any Mental Disorder Diagnosis a .
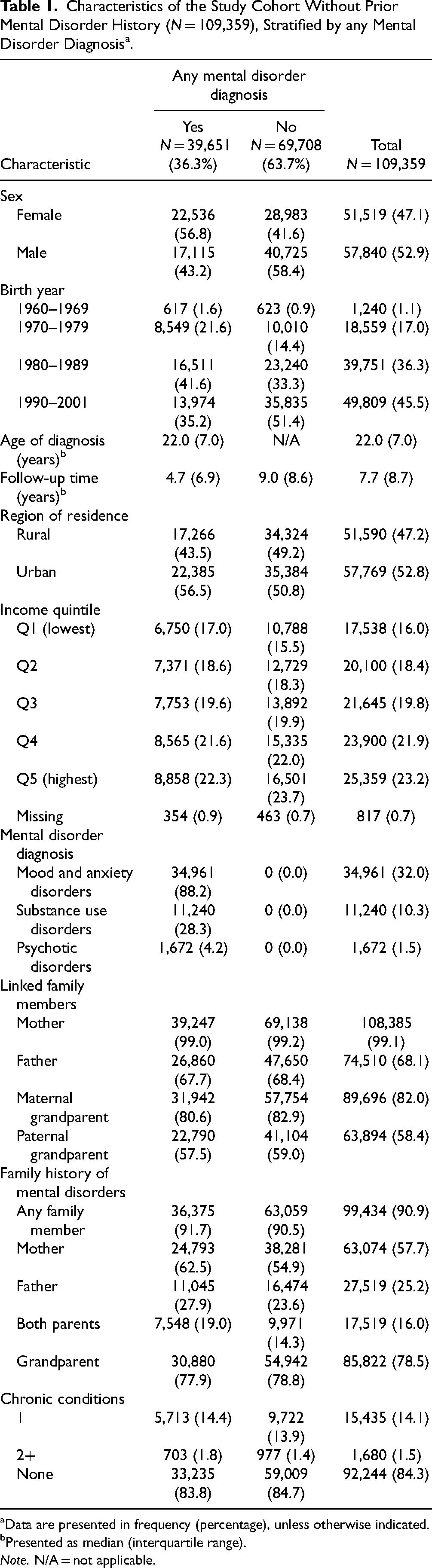
Data are presented in frequency (percentage), unless otherwise indicated.
Presented as median (interquartile range).
Note. N/A = not applicable.
Primary Analyses
Figure 2 presents the independent associations of family history in parents and grandparents with risk of developing a mental disorder. Parental history of mood and anxiety, and substance use disorders was associated with the risk of the disorders, but there was a slightly stronger association with maternal history: mood and anxiety disorders (HR 1.41, 95% CI, 1.38 to 1.44), substance use disorders (HR 1.73, 95% CI, 1.66 to 1.80). Parental history of psychotic disorders was also associated with an increased risk but was highest with paternal history (HR 3.73, 95% CI, 2.99 to 4.64). Parental history of any mental disorder was associated with the risk of the disorders; maternal history had the strongest influence (HR 1.39, 95% CI, 1.36 to 1.41). Among all mental disorders, parental history had the strongest influence on psychotic disorder risk. An independent association of grandparent history with the risk of all mental disorders was observed: mood and anxiety disorders (HR 1.12, 95% CI, 1.06 to 1.18), substance use disorders (HR 1.42, 95% CI, 1.34 to 1.50), psychotic disorders (HR 1.18, 95% CI, 1.02 to 1.37), any mental disorder (HR 1.16, 95% CI, 1.09 to 1.23).
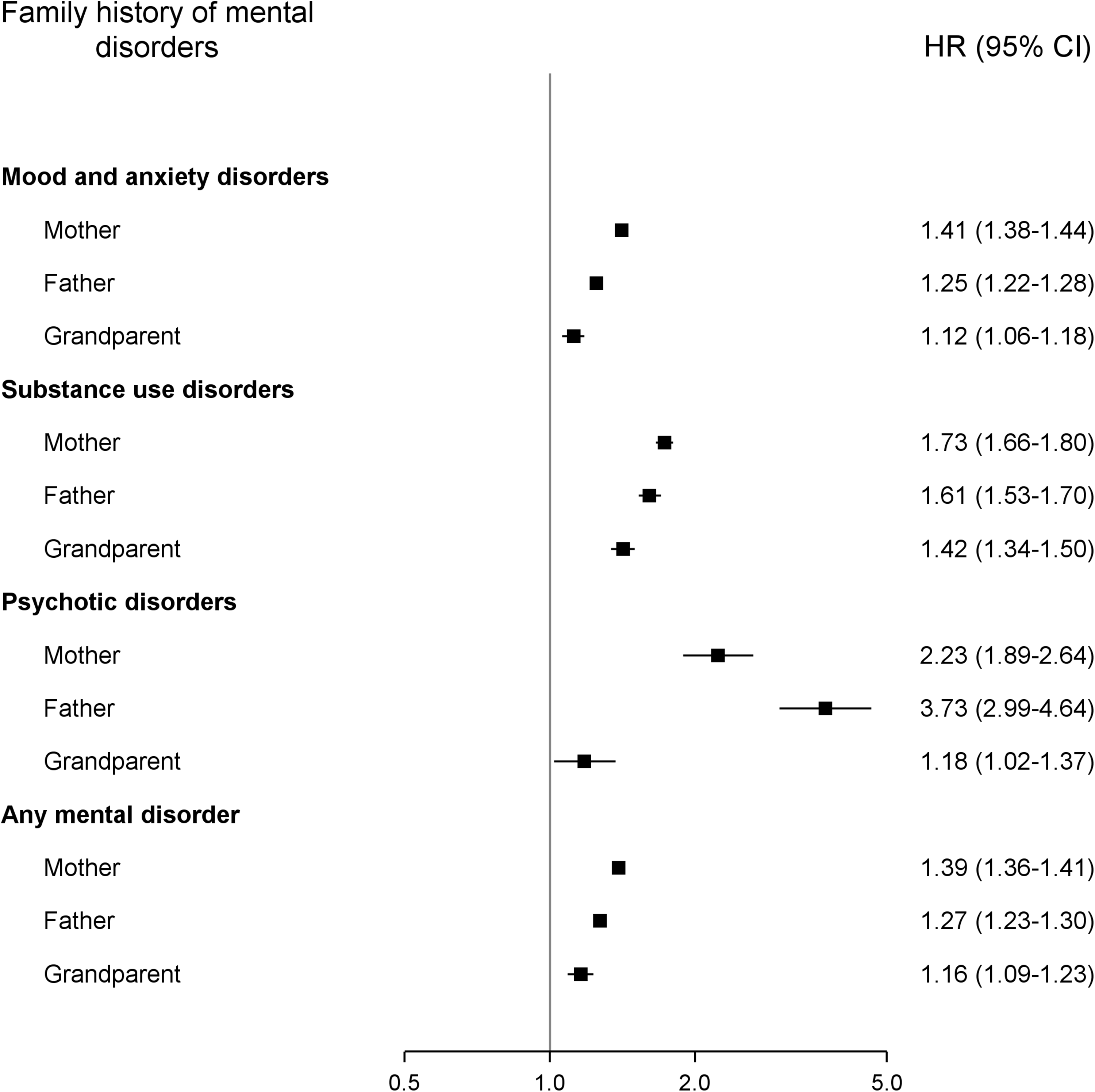
Risk of mental disorders among individuals with a family history of the disorder. Associations are reported as hazard ratios (HRs) with 95% confidence intervals (CIs), and mutually adjusted for history in the mother, father, and grandparent; sex; region; income quintile; number of chronic conditions and decade of birth.
Secondary Analyses
Table 2 outlines the results of the secondary analyses: (1) stratifying by cohort sex, (2) comparing maternal and paternal grandparent's influence on mental disorder risk and (3) comparing grandmother's and grandfather's influence on mental disorder risk. The association of family history with risk of mental disorders was observed for both males and females. However, parental history influence on psychotic disorders risk was higher for females (maternal history: HR 2.54, 95% CI, 1.97 to 3.28 and HR 2.05, 95% CI, 1.64 to 2.57; paternal history: HR 3.89, 95% CI, 2.78 to 5.45 and HR 3.56, 95% CI, 2.67 to 4.76 in females and males, respectively). No significant differences were observed when comparing the influence of maternal and paternal grandparent history on the risk of developing mental disorders. Compared with grandmothers, a history in grandfathers was associated with a slight increased risk of developing mood and anxiety (grandfathers: HR 1.12, 95% CI, 1.08 to 1.17 and grandmothers: HR 1.04, 95% CI, 1.01 to 1.07), and substance use disorders (grandfathers: HR 1.42, 95% CI, 1.33 to 1.51 and grandmothers: HR 1.22, 95% CI, 1.15 to 1.29).
Secondary Analyses Showing Hazards Ratios and 95% Confidence Intervals for the Risk of Mental Disorders Among Individuals With a Family History of Mental Illness, Stratified by Sex, and Estimated Separately for Maternal Grandparents, Paternal Grandparents, Grandmothers, and Grandfathers.
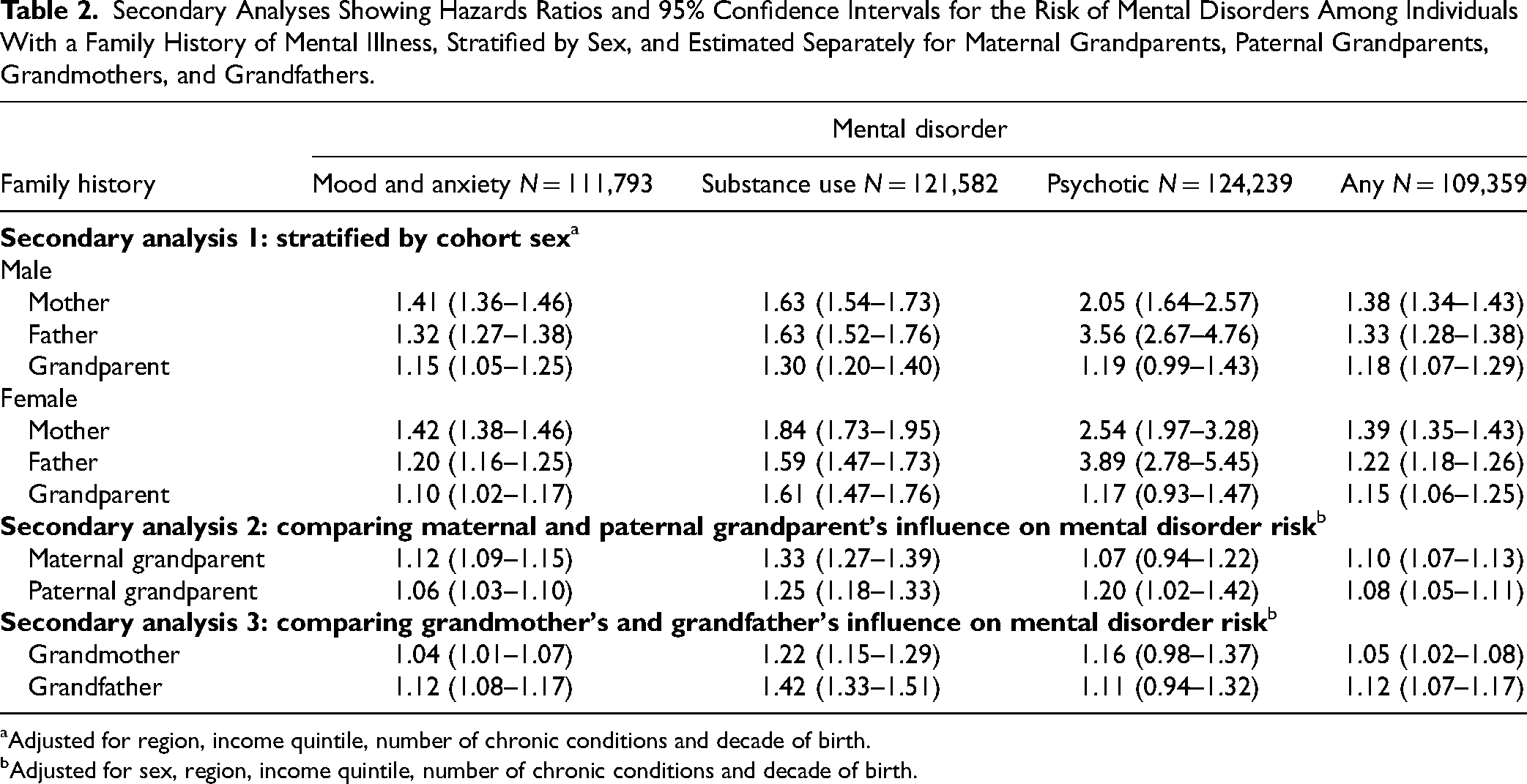
Adjusted for region, income quintile, number of chronic conditions and decade of birth.
Adjusted for sex, region, income quintile, number of chronic conditions and decade of birth.
Table 3 summarizes the influence that a family history of mood and anxiety, substance use and psychotic disorders has on the transdiagnostic risk of other mental disorders. Parental history of any mental disorder was associated with an increased risk of other mental disorders. In particular, parental history of any of the mental disorders was strongly associated with the risk of psychotic disorders. Except for mood and anxiety disorders, a grandparent's history of a mental disorder was associated with an increased risk of the other mental disorders. The association of family history with mental disorder risk remained broadly consistent across the study years; however, some variations were observed. For example, the influence of maternal history on mood and anxiety disorder risk increased over time (Supplemental Figure S1).
Hazards Ratios and 95% Confidence Intervals for the Transdiagnostic Risk of Mental Disorders Among Individuals With a Family History of Other Mental Disorders.
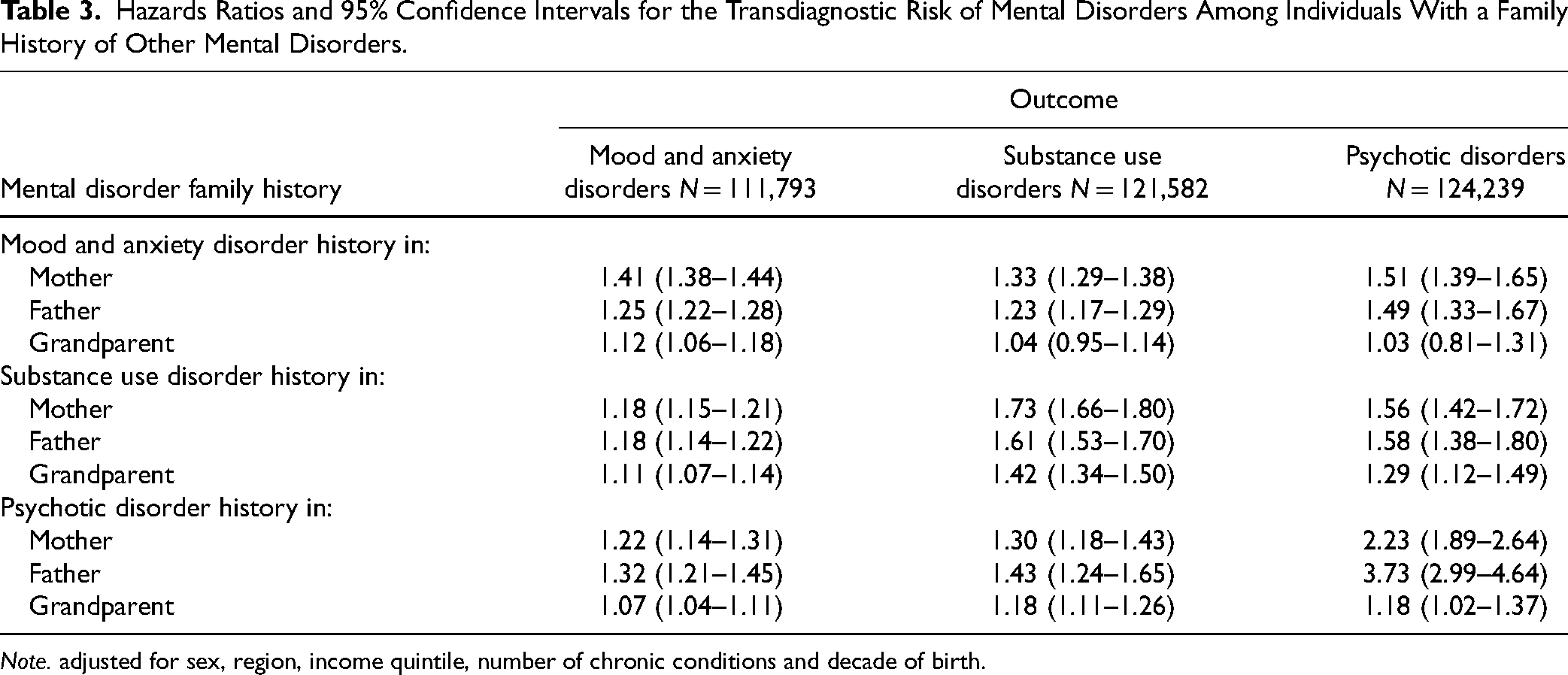
Note. adjusted for sex, region, income quintile, number of chronic conditions and decade of birth.
Sensitivity Analyses
The association of family history with mental disorder risk in individuals missing grandparent linkage was similar to those with grandparent linkage; however, the influence of paternal history on the risk of psychotic disorders was significantly lower in individuals missing grandparent linkages (Supplemental Figure S2). The association of family history with mental disorders remained largely unchanged in the sensitivity analyses that used drug dispensation in the case definition of mental disorders or excluded individuals without complete family linkages (Supplemental Figures S3-S4, respectively). One exception was the association of paternal history with psychotic disorder risk, which significantly declined when prescription dispensations were additionally used to identify the disorders (Supplemental Figure S4).
Discussion
This population-based cohort study found a strong association between parental history and mental disorder risk. The strongest association with family history was observed for psychotic disorders. Paternal history had the strongest influence on psychotic disorder risk; the impact of parental history on psychotic disorder risk was highest in females. Grandparent history of mental disorders was independently associated with a small increase in the risk of the disorders, above and beyond the influence of parental history.
A high prevalence of mental disorder family history was observed; nearly all individuals had a parent or grandparent with a diagnosed mental disorder. This could be attributed to the long observation period before index date, the inclusion of a wide range of mental disorders and the number of linked family members with a maximum of two parents and four grandparents. The association of parental history with mental disorders was previously reported.22,24,34 Mental disorder aetiology involves “multi-factorial gene-environment interactions.” 6 Many of the environmental factors associated with mental disorder risk, such as poverty, urbanicity, maltreatment and dysfunctional family relationships, are shared in families.15–20 Family history of mental disorders represents the genetic and shared environmental risk factors, both of which may explain the observed associations. The observed strong association of family history with psychotic disorders is consistent with previous literature.32,35 This could be partially attributable to the strong influence of genetics in the aetiology of psychotic disorders, with a heritability of up to 80%.10–14 The stronger association between paternal history of psychotic disorders with individual's risk compared to maternal history is inconsistent with a previous study. A Danish population-based study reported a strong association of schizophrenia with parental history; the association was higher with maternal than paternal history (relative risk 8.97, 95% CI, 6.93 to 11.62 and 6.63, 95% CI, 4.83 to 9.09, respectively). 32 However, our study examined a wide range of psychotic disorders, which might have contributed to this discrepancy. It is worth noting that the estimated impact of paternal psychotic disorder history on its risk in individuals was sensitive to changes in population, that is, selection bias, and disease definitions, that is, misclassification bias, as shown in Supplemental Figures S2 and S3. The higher risk of psychotic disorders in females with parental history is consistent with previous literature indicating a higher heritability of psychotic disorders in females.35,49
Evidence on the influence of grandparent history on mental disorders risk has been lacking and limited to smaller studies with self-reported measures.21,22,36,37 For example, a cohort study of 4600 children reported an association of parent-reported grandparent mental health problems with social and emotional wellbeing in young children. 21 A clinical cohort study of 968 adults with bipolar disorder reported an association with self-reported family history of mental disorders across three generations. 22 Another cohort study of 92 young children observed an increased risk of emotional and behavioural problems with parent-reported grandmother's depression and anxiety. 37 Our study overcame the critical limitations in these studies by including a large and representative population, using objectively diagnosed mental disorders in individuals, parents and grandparents, and investigating multiple mental disorders. Our work identified the role of grandparent history above and beyond parental history in mental disorder risk, which was statistically significant, but could be clinically insignificant, except for substance use disorders. The smaller influence of grandparent compared to parental history on the risk of mental disorders could be attributed to sharing less genetics and environmental factors. Parents share half of their genetic material with individuals compared to only a quarter of the genetic material shared with grandparents. Additionally, individuals share more environmental factors with parents than grandparents, such as housing, socioeconomic status, and lifestyle factors.
The strengths of this work are the use of a large population-based cohort and objective measures of mental disorders and family histories, the inclusion of both parents and grandparents and the inclusion of multiple mental disorders. To our knowledge, this study is the first population-level investigation of grandparent influence on objectively measured mental disorders risk. However, a few limitations should be noted. First, misclassification of mental disorder status could have arisen from using case definitions that have not been independently validated or individuals who have mental illnesses but do not seek care and remain undiagnosed. This traditionally biases results towards the null, which could underestimate the associations of family history with mental disorder risk.50,51 In the sensitivity analysis in which we used prescription medication dispensations to ascertain mental disorders, most associations remained unchanged, except for paternal influence on psychotic disorder risk, which was smaller in the sensitivity analysis. Second, the diagnostic criteria for mental disorders and versions of ICD to capture these disorders changed during the study period. To account for this, we stratified the results by decade of birth and found an overall consistent influence of family history on mental disorder risk over time. Third, we did not have complete family linkages to parents and grandparents for all individuals, which could have introduced selection bias. We observed differences in demographic characteristics as well as the prevalence of mental disorder diagnosis between individuals with and without grandparent linkage. However, in a sensitivity analysis, grandparent linkage status did not seem to introduce selection bias except for paternal history influence on psychotic disorders, which was higher in our cohort. There is also a potential for misclassification of the family linkages as they are not confirmed to be biological. Finally, our data source did not capture all the variables that could potentially influence the association between family history and the risk of mental disorders, such as parental educational level, ethnicity and race, and the severity of mental disorders, which could have resulted in unmeasured confounding. Nevertheless, this study demonstrated at the population level that mental disorder impact within families extends across three generations. Therefore, it is crucial to identify high-risk children and adolescents living in families affected by mental disorders to target intervention programs that provide effective support to these individuals and significantly improve their mental health outcomes as well as reduce the burden on healthcare systems and societies in Canada and elsewhere.
Conclusion
In this first population-level investigation of the intergenerational transfer of mental disorders across three generations, parental history was strongly associated with mental disorder risk. However, grandparent history had a smaller impact that may not be clinically significant except for substance use disorders. Replication studies in other jurisdictions are needed to confirm these findings. Study findings highlight the need for interventional programs targeting families living with mental illnesses to reduce the burden of mental disorders on families, healthcare systems and societies.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241255096 - Supplemental material for The Intergenerational Transfer of Mental Disorders: A Population-Based Multigenerational Linkage Study: Le transfert intergénérationnel des troubles mentaux : une étude sur les liens multigénérationnels basée sur la population
Supplemental material, sj-docx-1-cpa-10.1177_07067437241255096 for The Intergenerational Transfer of Mental Disorders: A Population-Based Multigenerational Linkage Study: Le transfert intergénérationnel des troubles mentaux : une étude sur les liens multigénérationnels basée sur la population by Amani F. Hamad, Barret A. Monchka, James M. Bolton, Oleguer Plana-Ripoll, Leslie L. Roos, Mohamed Elgendi and Lisa M. Lix in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We acknowledge the Manitoba Centre for Health Policy for the use of data contained in the Population Health Research Data Repository (HIPC/PHRPC #: 2019/2020-52; MCHP Project #: 2020-005). The results and conclusions are those of authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Seniors and Active Living, or other data providers is intended or should be inferred. AFH is supported by a Canadian Institutes of Health Research (CIHR) Fellowship. LML is supported by a Tier 1 Canada Research Chair.
Data Access
Data used in this article were derived from administrative health data as a secondary use. The data were provided under specific data sharing agreements only for approved use at the Manitoba Centre for Health Policy (MCHP). The original source data are not owned by the researchers or MCHP and as such, cannot be provided to a public repository. The original data source and approval for use have been noted in the acknowledgments of the article. Where necessary, source data specific to this article or project may be reviewed at MCHP with the consent of the original data providers, along with the required privacy and ethical review bodies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported jointly by the Winnipeg Foundation Innovation Fund of the Rady Faculty of Health Sciences and a Canadian Institutes of Health Research (CIHR) Foundation Grant (FDN-143293).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.