
Abstract
Objectives
To determine if and to what degree neighbourhood-level marginalization mediates mental health service use among transgender individuals.
Methods
This retrospective cohort study identified 2,085 transgender individuals through data obtained from 4 outpatient community and hospital clinics in 3 large cities in Ontario, which were linked with administrative health data between January 2015 and December 2019. An age-matched 1:5 comparison cohort was created from the general population of Ontario. Outcome measures were analysed from March 2020 to May 2022. The primary outcome was mental health service utilization, which included mental health-related visits to primary care providers, psychiatrists, mental health- and self-harm-related emergency department visits, and mental health hospitalizations. Mediation variables included ethnic concentration, residential instability, dependency, and material deprivation at the neighbourhood level and were derived from the Ontario Marginalization Index.
Results
This study identified 2,085 transgender individuals from participating outpatient community and hospital clinics, who were matched to the general population (n = 10,425). Overall, neighbourhood-level marginalization did not clinically mediate mental health service use. However, transgender individuals were more likely to be exposed to all forms of neighbourhood-level marginalization, as well as having higher rates of health service use across all outcome measures.
Conclusions
In this study, mental health service use among transgender individuals was not clinically mediated by marginalization at the neighbourhood level. This study highlights the need to explore marginalization and mental health service use at the individual level to better understand the mental health disparities experienced by transgender individuals and to ensure that health-care services are inclusive and affirming.
Background
In Canada, over 100,000 individuals identify as transgender and nonbinary, accounting for ∼0.33% of the total Canadian population aged 15 and over. 1 Transgender is an umbrella term referring to individuals whose gender identity is discordant from their sex assigned at birth, whereas cisgender refers to individuals whose gender identity and sex assigned at birth align. Previous research has shown higher rates of mental and physical comorbidities and higher health service use among transgender individuals compared to cisgender individuals, specifically in relation to chronic conditions, such as asthma, diabetes, HIV, and poor mental health outcomes, including suicidality and self-harm. 2 However, there is limited understanding as to why this is the case, and furthering this understanding will help inform future efforts at improving the health of the transgender population.
Transgender individuals are classified as a health disparity population by the National Institutes of Health. 3 As per a 2019 report, 2-spirit, lesbian, gay, bisexual, transgender, and queer (2SLGBTQ+) people experience significantly higher rates of poverty compared to the general population, and among 2SLGBTQ+ people, transgender individuals experience the highest rates of poverty. 4 Transgender individuals often encounter difficulties accessing housing, employment, and basic goods and services, resulting in disproportionate rates of homelessness and unemployment. 5 Additionally, transgender people experience more social marginalization including discrimination and stigma compared to cisgender people resulting in poorer health outcomes. 6
Marginalization consists of the deprivation of economic resources and lack of knowledge, political rights, capacity, recognition, and power. 7 Marginalization, also referred to as social exclusion, has been associated with poorer physical and mental health outcomes worldwide, likely as a result of minority stress.6,8 Minority stress theory posits that stigma, prejudice, and discrimination create hostile and stressful social environments resulting in poor health. 7 This stress has been directly linked to psychological distress and higher suicide risk among 2SLGBTQ+ individuals and may contribute to the earlier onset of certain chronic diseases in this population.9,10 2SLGBTQ+ individuals tend to have worse health outcomes related to minority stress caused by their marginalization (e.g., lower socioeconomic status (SES), homelessness, unemployment, etc.), including higher rates of depression, anxiety, and substance use; lower screening rates and higher rates of certain cancers and chronic conditions, including HIV.9,11 In the general population, marginalization has been shown to negatively affect both mental and physical health.12–23 For example, lower SES in the general population has been linked with both a higher likelihood of developing asthma, Type 2 diabetes, and their consequences.12,13,17,18 However, minimal research has investigated how marginalization impacts health outcomes among transgender individuals.
Research demonstrates that unstable housing, unmet financial needs, and socioeconomic marginalization are barriers to care, including engagement in HIV care.21,22 Marginalization, in the form of food insecurity, low SES, and unstable housing, has been associated with an increased risk of experiencing a psychiatric condition, self-harm, suicidal thoughts, mood disorders, and generally worsened mental health.14–16,23,24 Transgender people experience significant barriers and challenges accessing and navigating health-care environments, including disrespectful attitudes and being referred to by incorrect names and pronouns. 25 In Canada, 43.9% of transgender people reported unmet health needs in the last year, compared to 10.7% of the cisgender population. 10 Despite these barriers, previous research has identified higher health service use, including emergency department (ED) visits among transgender individuals. 2 The objective of this study is to determine the extent to which neighbourhood-level marginalization mediates mental health service use among transgender individuals.
Methods
Setting and Context
Ontario is Canada's most populated province, with ∼14.8 million people counted in 2021. 26 The 2021 Canadian census reported 39.1% (39,450) of the total transgender population resides in Ontario. 27 However, the actual number of transgender individuals is likely higher due to people feeling uncomfortable and unsafe disclosing their transgender identity for various reasons, including stigma and discrimination. In Ontario, hospital and physician-related care and medically necessary laboratory tests are covered by the Ontario Health Insurance Plan (OHIP) for all legal permanent residents.
Study Design
A matched retrospective cohort study was conducted using administrative health data. Two cohorts were created: one with transgender individuals (n = 2,085) and another with a 1:5 age-matched cohort of the general Ontario population (n = 10,425), which excluded individuals in the transgender cohort. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline. 28
Data Sources
The ICES data repository includes individual-level, linkable, longitudinal data on most publicly funded health-care services for individuals covered by OHIP. The data repository includes physician claims submitted to OHIP, drug claims submitted to the Ontario drug benefit (ODB) Program, discharge abstracts of psychiatric hospital stays and ED visits, and diagnostic and lab tests. We worked with 4 health clinics in 3 cities (Toronto, Ottawa, and Thunder Bay) in Ontario that specialize in offering transgender-inclusive and gender-affirming services to identify a cohort of transgender individuals and link their data with administrative databases held at ICES between January 2015 and December 2019.
The participating clinics included 3 community health centers and 1 outpatient hospital clinic. Data extracted from each clinic included health card numbers, date of birth, and self-defined gender identity of all transgender patients (between January 2015 and December 2019). ICES is a prescribed entity under section 45 of Ontario's Personal Health Information Protection Act, which authorizes it to collect personal health information, without consent for the purpose of analysis or compiling statistical information, including the management, evaluation, monitoring, and allocation of resources, for all or part of the health system. The use of the data in this project is authorized under section 45 of Ontario’s Personal Health Information Protection Act and does not require review by a Research Ethics Board. All data sets were linked using unique encoded identifiers and analysed at ICES.
Measures
The outcome of interest was mental health service use, which was a continuous measure, representing the total number of each health service visit. Mental health service use was measured by mental health primary care provider visits using specific OHIP billing codes, psychiatrist visits, mental health, and self-harm ED visits through the National Ambulatory Care Reporting System and mental health hospitalizations through the Ontario Mental Health Reporting System and Discharge Abstract Database. The exposure variable of interest was gender, measured as being in the transgender cohort or general population cohort. Mediators were selected a priori and were derived from the ICES database holdings. The main mediator of interest was marginalization measured using the Ontario Marginalization Index (ON-Marg), an area-based deprivation index created in Ontario, Canada. 29 This index studies marginalization by examining 4 different dimensions: dependency, or the proportion of individuals unable to work due to old age, young age, or disability in a neighbourhood; ethnic concentration, or the concentration of racialized individuals in a neighbourhood; material deprivation, which includes several different indicators of lower SES in a neighbourhood; and residential instability, which measures area-level concentrations of people who experience high rates of family or housing instability. 30
Sociodemographic variables (sex and age) were captured in the Registered Persons Database; migrant status (immigrant, long-term resident, and refugee) was determined using the Immigration, Refugees, and Citizenship Canada Permanent Resident Database; access to drug benefit eligibility based on financial need or social assistance was determined through the ODB Database (in Ontario, eligibility criteria for drug coverage in this demographic include being 65+, unemployment, disability, high prescription drug costs relative to net household income, receipt of home care services, and residence in a long-term care facility); medical comorbidities (arthritis, asthma, cancer, diabetes, HIV, psychosis, etc.) were determined using validated chronic condition algorithms based on physician billings and hospital discharge databases available at ICES31–36; and psychiatric and medical comorbidities were determined using the Johns Hopkins ACG® System Version 10 software, which categorizes codes from the 9th and 10th revisions of the International Classification of Diseases into diagnosis clusters referred to as Aggregated Diagnosis Groups (ADGs), based on 5 clinical dimensions. 37
Statistical Analysis
We used mediation models (using SAS PROC CAUSALMED) to assess the potential mediation effect of marginalization (dependency, ethnic concentration, material deprivation, and residential instability) on the association between gender (transgender vs. general population) and mental health service use. 38
In order to establish significant mediation, the exposure variable (transgender vs. general population) must predict the outcome variable (health service use). The exposure variable must also predict the proposed mediator (marginalization), and the mediator must, in turn, predict the outcome variable (health service use). These relationships are established via regression in the mediation models estimated via SAS PROC CAUSALMED. The SAS PROC CAUSALMED procedure then estimates causal mediation effects (using regression), and confidence intervals (CIs) for the effects based on the maximum likelihood estimates, as well as estimating a p-value regarding the statistical significance of the estimated indirect (mediated) effect compared to zero. In particular, the procedure uses counterfactuals (variation between levels of the exposure variable and proposed mediator) to estimate a 4-way decomposition of the total effect, comprised of the controlled direct, reference interaction, mediated interaction, and pure indirect (PI) effects, using regression. 39 The PI effect designates the mediated effect that is not due to interaction and was the regression estimate used to evaluate mediation. Additionally, percentages of the total effect that are attributed to mediation and the percentage of the total effect eliminated by controlling the mediator level were also calculated. 38 All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Regarding statistical significance, a 2-sided p-value of <0.05 was considered significant. However, the Bonferroni correction was used to account for multiple comparisons and to control the familywise error rate. Analyses generally required 20 comparisons (4 ON-Marg dimensions × 5 outcome variables), such that the adjusted significance level for analyses was 0.0025. The adjusted significance level was 0.01 when evaluating the direct relationship between exposure and outcome variables (transgender vs. general population for health service use) and between exposure and proposed mediator (transgender vs. general population for marginalization), as these analyses required 5 and 4 comparisons, respectively. The mediator variable (marginalization) was dichotomized from quintiles to low marginalization (quintiles 1–3) versus high marginalization (quintiles 4 and 5). Adjusted models included age categories (1–24, 25–44, 45–64, and 65+ years), migrant status, and recipients of ODB as a proxy for financial need (Yes/No). (See Figure 1 for the directed acyclic graph.)
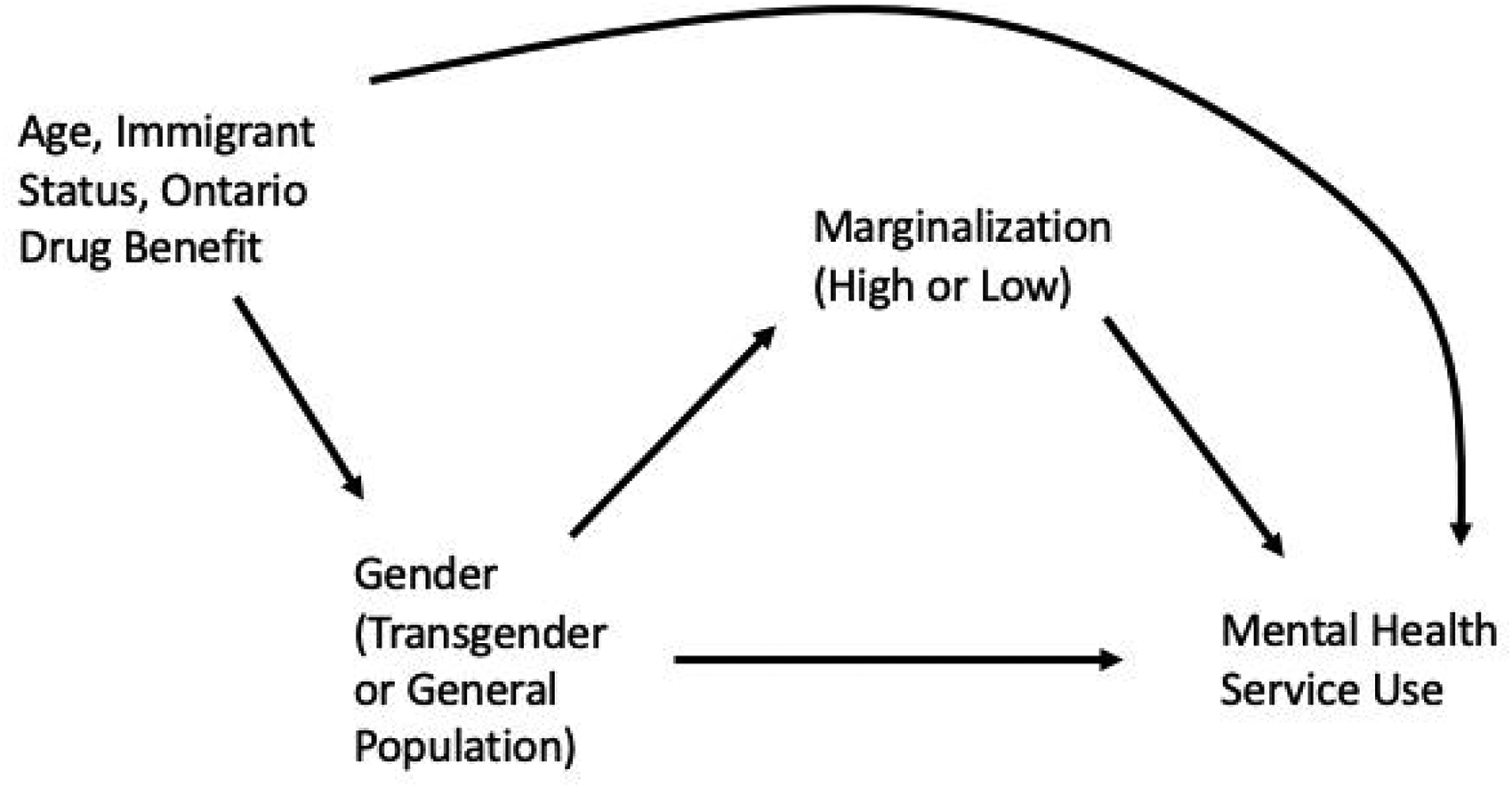
Conceptual framework of data analysis.
Results
This study identified 2,085 transgender individuals, who were matched 1:5 to a random 5% sample of the general population (n = 10,425) based on age (see Table 1 for sociodemographic and mental health comorbidities). The cohorts had a mean age of 33.25 (12.86) years with 52.6% of individuals between the ages of 25 and 44 and 28.7% under the age of 24. The transgender cohort was made up of individuals with a variety of gender identities, which were collapsed into the following categories: transgender women (36.90%, n = 770), transgender men (36.50%, n = 761), nonbinary (6.24%, n = 130), and unknown (16.5%, n = 345). The unknown category included transgender individuals whose self-defined gender identity was missing.
Sociodemographic and Clinical Characteristics of Transgender Individuals Compared to Age-Matched General Population as of January 2019.
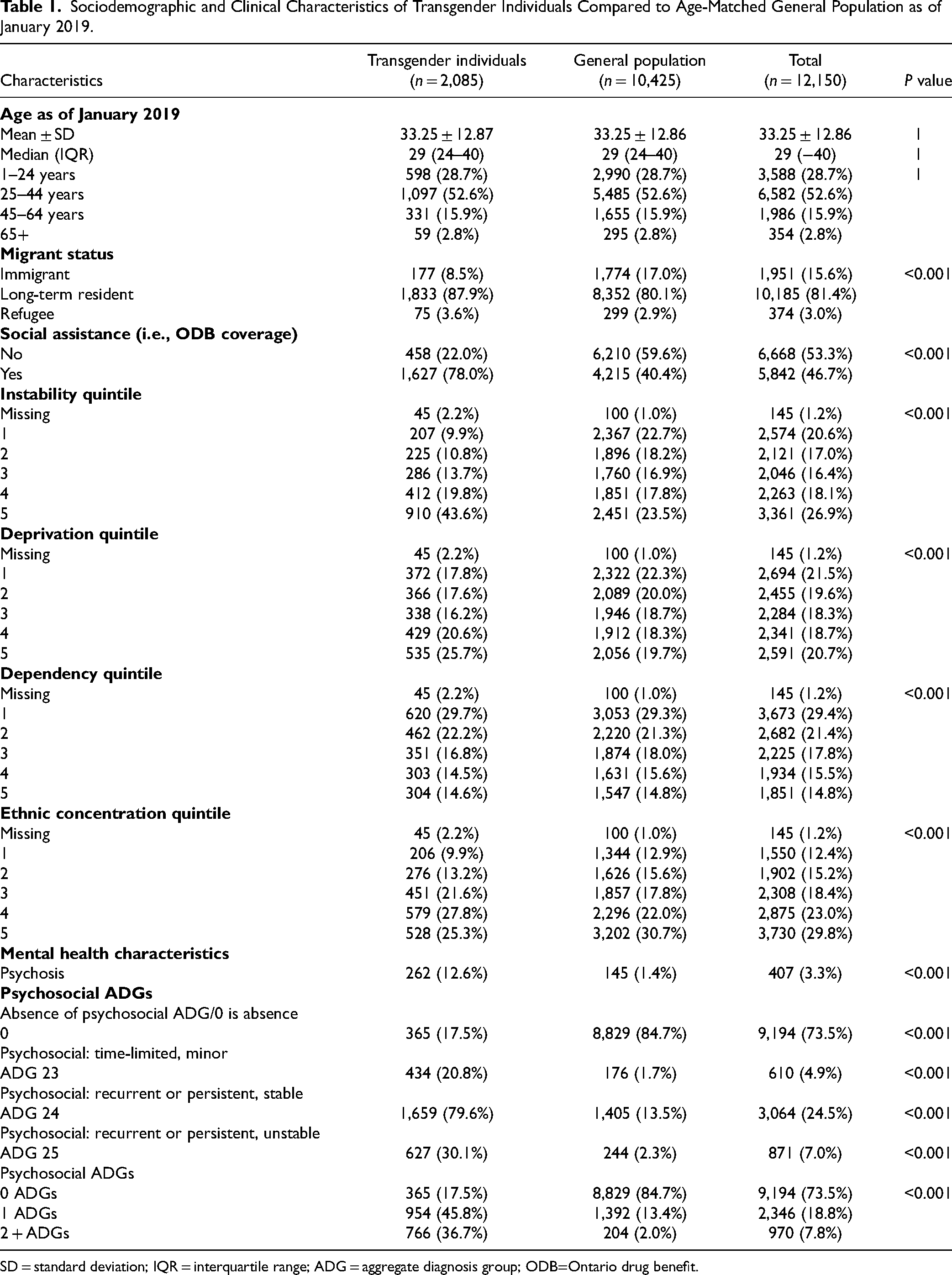
SD = standard deviation; IQR = interquartile range; ADG = aggregate diagnosis group; ODB=Ontario drug benefit.
Mediation Analyses
Direct Relationship
Transgender individuals had higher mental health service use compared to the general population across all outcome variables (see Table 2). Transgender individuals had higher mental health primary care provider visits (b = 6.32; 95% CI [6.01, 6.62], SE = 0.15; z = 40.85, p < 0.001), psychiatrist visits (b = 6.78, 95% CI [6.28, 7.28], SE = 0.26, z = 26.59, p < 0.001), mental health ED visits (b = 1.26, 95% CI [1.14, 1.38], SE = 0.06; z = 20.09, p < 0.001), self-harm ED visits (b = 0.13, 95% CI [0.1142; 0.1154], SE = 0.01; z = 12.82, p < 0.001), and mental health hospitalizations (b = 0.53, 95% CI [0.48, 0.58], SE = 0.02, z = 22.47, p < 0.001) compared to the general population.
Health Service Utilization Among Transgender Individuals and Age-Matched General Population Cohort (2015 to 2019).
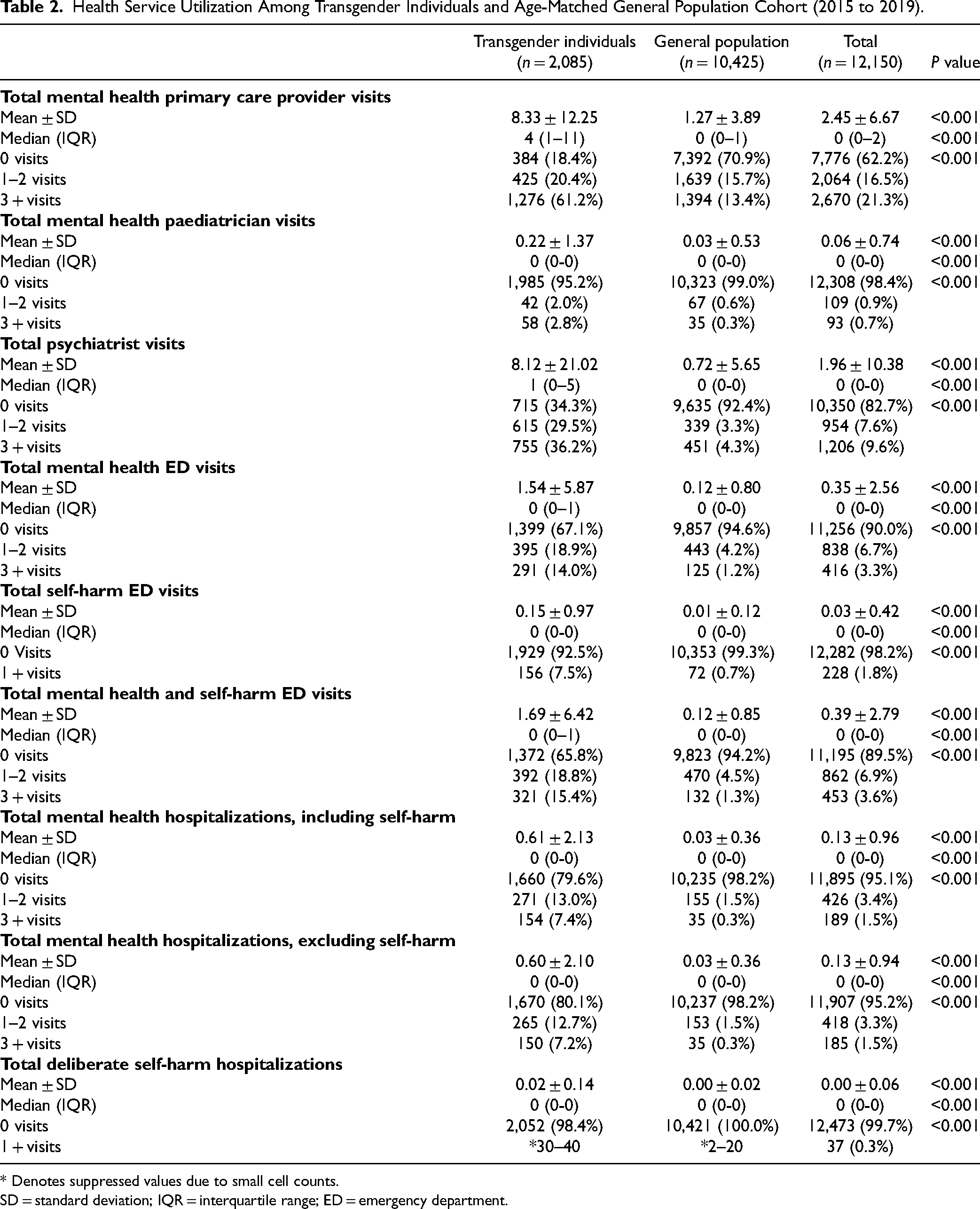
* Denotes suppressed values due to small cell counts.
SD = standard deviation; IQR = interquartile range; ED = emergency department.
Indirect Relationship
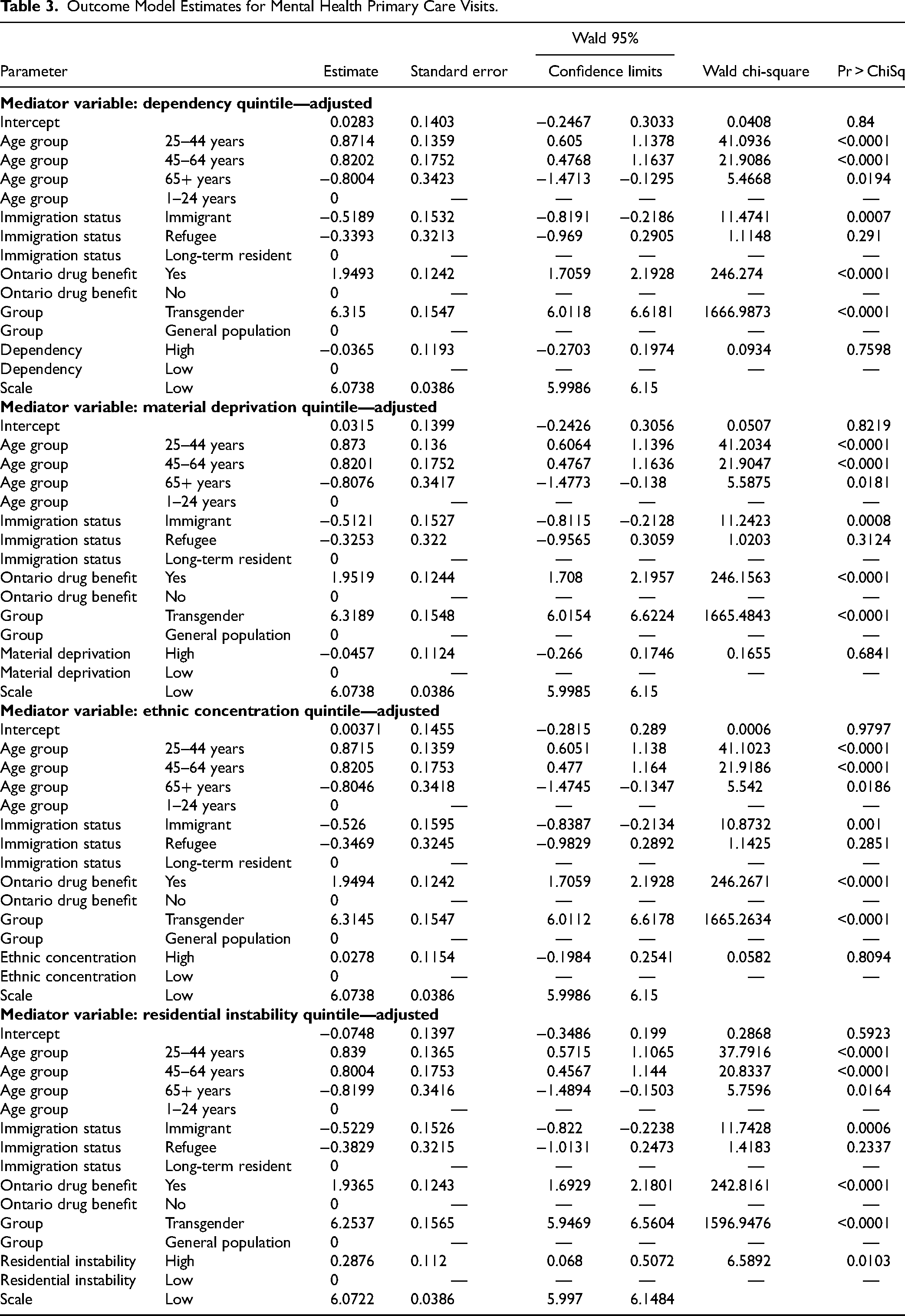
No ON-Marg dimension emerged as a significant mediator across the 5 outcome measures. Transgender individuals showed higher ON-Marg scores across all dimensions, as they lived in neighbourhoods with higher dependency (p < 0.001), ethnic concentration (p < 0.001), material deprivation (p < 0.001), and residential instability (p < 0.001; see Table 1) when compared to the general population. However, ON-Marg dimensions did not predict outcome measures, except in only 3 cases. Living in a neighbourhood with higher ethnic concentration predicted a higher number of psychiatrist visits, b = 0.61, 95% CI [0.24, 0.99], SE = 0.19, z = 10.39, p = 0.001. Ethnic concentration also predicted ED visits due to self-harm, such that living in a neighbourhood with higher ethnic concentration predicted lower ED visits due to self-harm, b = −0.02, 95% CI [−0.03, −0.004], SE = 0.008, z = 6.07, p = 0.0125. Residential instability also predicted mental health primary care provider visits, b = 0.29, 95% CI [0.07, 0.51], SE = 0.11, z = 6.60, p = 0.01. Estimates of the mediated (indirect) effect based on maximum likelihood estimates were not significant (see Tables 3 to 5 for model estimates).
Outcome Model Estimates for Mental Health Primary Care Visits.
Outcome Model Estimates for Psychiatrist Visits.
Outcome Model Estimates for Emergency Department Visits and Hospitalizations.
Discussion
There were significant differences in rates of marginalization between transgender individuals and the general population.
We hypothesized that neighbourhood-level marginalization would mediate mental health service utilization among transgender individuals; however, this was not the case in our study. Dependency, ethnic concentration, material deprivation, and residential instability measured at the neighbourhood-level did not mediate mental health service utilization. Even though the current sample constitutes the largest sample of Canadian, transgender health data, there may not have been sufficient statistical power to detect mediation effects due to a large number of multiple comparisons (m = 20). Other forms of marginalization may explain the discrepancies in mental health service use, as well. Other forms of marginalization that may be contributing to the higher rates of mental health service use include stigma and minority stress. The higher rates of psychiatrist visits by individuals in higher ethnic/racial minority communities may be a result of minority stress and marginalization at the individual level. Prior research has found that members of stigmatized minority groups, specifically racialized transgender individuals experience higher levels of stress due to stigmatization resulting in poor mental health. 8 Primary care provider visits for mental health were higher among individuals who experienced residential instability. Housing has been shown to be an important determinant of health and poor housing is associated with a variety of health conditions including poor mental health. 40 The lower likelihood of mental health- and self-harm-related ED visits may be a result of distrust in the health-care system due to discrimination and marginalization. Prior research shows that racialized transgender people experience significantly higher levels of transphobic discrimination compared to their White counterparts in accessing health services. 41 These results may reflect emerging research that ethnic/racial minority status may decrease ED visits due to self-harm.42,43 Similarly, a study of Chinese-Canadian women found that individuals would rather endure their emotional distress than seek help, which exemplifies cultural factors that can lead to a lower likelihood of presenting for care in neighbourhoods of greater ethnic concentration. 44
For instance, they also found that there were no differences in racial/ethnic minority status with regard to self-harm-related ED visits in the United States, even though Hispanic and African American respondents experience higher rates of self-harm in nationwide data sets, such that ethnic/racial minority communities may be underutilizing services. 42 Prior research has also found that Indigenous subscribers to a Canadian text service reported higher rates of suicidal ideation when compared to peers. 44 However, Canadian medical records often do not include data on race/ethnicity, such that these are unavailable for later analysis in Canadian studies of service utilization.45–47 Further research may consider base rates of suicidal behaviour and attempts among racial/ethnic minorities in Canada, as well as associated ED visits, insofar as the current study is one of the first in Canada to suggest that living in communities with higher ethnic concentration may actually depress rates of ED visits due to self-harm (though rates of self-harm behaviour were not evaluated). Future studies may further consider the consequences of fewer ED visits due to mental health and self-harm among racialized transgender Canadians. Additionally, future research on marginalization and mental health service utilization may be better studied using primary data collection, particularly qualitative methods.
This research has numerous policy implications. First, efforts are required to implement and strengthen gender-inclusive and race/ethnicity data collection tools in health care. This will provide critical information on how transgender individuals access mental health services. This study also highlights the need to better understand the higher rates of mental health service use among transgender individuals, and whether there are marginalization measures that are not captured by ON-Marg which contribute to this. Lastly, more efforts are necessary to ensure that health care services, particularly mental health services, are transgender-inclusive and affirming of transgender individuals, which will be essential in order to support and improve the mental health of this population.
Strengths and Limitations
A strength of our study is that we identified a large sample of transgender individuals allowing for unprecedented power to examine mediation and differences in marginalization between transgender individuals and the general population. Unlike previous studies on transgender health that relied on medical transition and diagnostic definitions to identify transgender individuals, our study used self-reported gender identities to identify transgender individuals which is more representative of the larger transgender population.48,49
Our study has several limitations. A large number of multiple comparisons (m = 20) reduced statistical power, despite the large sample size, increasing the likelihood of Type II error, which is a general concern when conducting structural equation modeling. 50 The participating health clinics were situated in urban centers in Ontario, with a limited representation of individuals from rural settings. This may limit the generalizability of our findings. Additionally, we were only able to identify individuals who had access to primary care, meaning that those who are so marginalized that they cannot access primary care are not included in our sample. As explained above, more marginalized individuals in the general population appear to access the ED for nonurgent reasons more often than less marginalized individuals, and the inability to capture this population may partially explain why marginalization did not appear to mediate health service use in our study. Most hospitals in Ontario still do not collect gender identity data and only record sex designation listed on people's OHIP cards, and therefore, are unable to identify transgender patients and link their OHIP numbers to ICES databases, making it nearly impossible to examine health service use among transgender individuals who do not have a primary care provider. It is important to note that due to the stigmatization faced by 2SLGBTQ+ populations and difficulties accessing gender-affirming health care, many transgender individuals do not feel safe disclosing their transgender identity and socially and/or medically transitioning—these individuals may also be marginalized and access health care but would not be captured by the methods utilized in this study. Another limitation of the study is that it focuses on health-care services covered under the public health-care system and does not include health service use in the private health-care system. A limitation of using OBD as a proxy for social assistance is that we are unable to determine the financial needs of individuals 65+. Additionally, it is important to note that individuals who are categorized as not receiving ODB could be covered but have not filled a prescription during the analysis period resulting in the overestimation of the number of people who are not covered under the ODB program. Likewise, we are unable to determine why individuals were receiving ODB. Thus, limiting ODB as a proxy for financial need. The data collected also does not include community care which transgender individuals are known to utilize. While there are many benefits of being able to use ICES administrative health data, including the breadth and quality of data, there are limitations in using secondary data but it is still valuable for understanding more about transgender health in Ontario.
Conclusion
Our study found higher rates of mental health service use among transgender individuals compared to the general population in Ontario. However, we found that the mental health service utilization differences were not clinically mediated by the ON-Marg Index (although 2 emerged as marginally significant). Our study highlights the need for additional research to better understand the mental health outcomes and the factors (e.g., stigma) that mediate the mental health disparities experienced by transgender individuals. Possible directions for future research include the use of primary data collection methods, particularly qualitative research, to understand these issues and provide deeper insight. Creating a better understanding of the source of these disparities will inform public health and health service interventions to reduce health-care disparities.
Footnotes
Acknowledgments
Parts of this material are based on data and information compiled and provided by the Ministry of Health (MOH), CIHI, Cancer Care Ontario (CCO), and Immigration, Refugees, and Citizenship Canada Current of May 17. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. We thank IQVIA Solutions Canada Inc. for the use of their Drug Information File. CCO (now known as Ontario Health): parts of this material are based on data and information provided by Ontario Health (OH). The opinions, results, views, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of OH. No endorsement by OH is intended or should be inferred.
Data Access
We are unable to make our dataset publicly available for ethical and privacy reasons. This study involves sensitive administrative health data, which cannot be shared publicly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Centre for Addiction and Mental Health Discovery Fund.