
Abstract
Objectives
Neurocognitive deficits are central in schizophrenia. Cognitive remediation has proven effective in alleviating these deficits, with medium effect sizes. However, sizeable attrition rates are reported, with the reasons still uncertain. Furthermore, cognitive remediation is not part of routine mental health care. We conducted a systematic review to investigate factors that influence access and engagement of cognitive remediation in schizophrenia.
Methods
We systematically searched the PubMed, Web of Science, and PsycINFO databases for peer-reviewed articles including a cognitive remediation arm, access, and engagement data, and participants with schizophrenia spectrum disorders aged 17–65 years old. Duplicates and studies without a distinct cognitive remediation component, protocol papers, single case studies, case series, and reviews/meta-analyses were excluded.
Results
We included 67 studies that reported data on access and engagement, and extracted quantitative and qualitative data. Access data were limited, with most interventions delivered on-site, to outpatients, and in middle- to high-income countries. We found a median dropout rate of 14.29%. Only a small number of studies explored differences between dropouts and completers (n = 5), and engagement factors (n = 13). Dropouts had higher negative symptomatology and baseline self-efficacy, and lower baseline neurocognitive functioning and intrinsic motivation compared to completers. The engagement was positively associated with intrinsic motivation, self-efficacy, perceived usefulness, educational level, premorbid intelligence quotient, baseline neurocognitive functioning, some neurocognitive outcomes, and therapeutic alliance; and negatively associated with subjective cognitive complaints. Qualitative results showed good acceptability of cognitive remediation, with some areas for improvement.
Conclusions
Overall, access and engagement results are scarce and heterogeneous. Further investigations of cognitive remediation for inpatients, as well as remote delivery, are needed. Future clinical trials should systematically explore attrition and related factors. Determining influential factors of access and engagement will help improve the implementation and efficacy of cognitive remediation, and thus the recovery of people with schizophrenia.
Introduction
Neurocognitive dysfunction is a core deficit in schizophrenia. Affected abilities range from processing speed, attention and vigilance processes, verbal and visual learning, problem-solving skills, and memory. 1 Cognitive deficit is found in the majority of this population, with reported rates ranging from 70% to 100%,2,3 alongside increasing evidence of heterogeneity of severity.4,5 Neurocognitive impairments also significantly impact daily functioning, including functional capacity (i.e., the ability to perform skills in optimal conditions) and real-world functioning (i.e., completing day-to-day activities),6,7 and quality of life.8,9
The absence of effective pharmacology to treat cognitive symptoms in schizophrenia 10 has spurred the development of psychosocial interventions, such as cognitive remediation (CR). CR is defined as “an intervention targeting cognitive deficit (attention, memory, executive function, social cognition or metacognition) using scientific principles of learning, with the ultimate goal of improving functional outcomes.” 11 (p.2) Experts recommend the implementation of a supportive environment as well as opportunities to apply the strategies in real life to enhance CR effectiveness (CR Expert Working Group, 2012 in McGurk et al. 12 ). The efficacy of CR on neurocognitive functioning for schizophrenia has been demonstrated in clinical trials, for example, Bryce et al. 13 and Fiszdon et al. 14 and meta-analyses.15–17 Multiple systematic reviews and meta-analyses have been conducted examining what specific CR response factors account for intervention efficacy, with results suggesting the importance of premorbid intelligence quotient (IQ), baseline cognition, course of illness severity, baseline negative symptomatology, and training task progress.14,18,19
Despite evidence for CR efficacy, this intervention is not yet part of routine mental healthcare or national mental health recommendations in most developed countries.20–22 The factors that contribute to poor clinical implementation remain indeterminate. Institutional issues and individual factors regarding consumers and mental health practitioners need to be investigated. It is likely that the wide variety of CR techniques, questions raised about the targeting of consumers, the range of functioning outcomes addressed, as well as therapist strategies used during the intervention contribute to a lack of clarity, especially regarding implementation.17,23 Three recognized barriers involved in the dissemination of evidence-based practices, such as CR, include (1) the lack of staff knowledge and skills, (2) organizational factors that undermine staff potential to implement innovative interventions,24,25 and (3) consumers’ individual barriers. 26 To our knowledge, these factors have not been fully investigated. In a recent meta-analysis, Vita et al. 27 commented on participant and intervention characteristics in relation to acceptability (i.e., dropout rates) of CR for schizophrenia, but did not specifically focus on the quantitative and qualitative data aspects of both access and engagement in CR in schizophrenia; the aim of the current paper. We define access as the means by which an intervention is made available, offered and delivered, such as location and settings. Engagement is defined as participation and perseverance in therapy, it can be measured using dropout rates, session attendance, and homework completion. Indeed, Vita et al. 27 suggested that engagement might be better assessed by combining objective measures, such as dropout rates, with qualitative feedback, which the current study aimed to do. Another recent meta-analysis by the same team examined study and participant characteristics as moderators of CR response or efficacy. 28 In contrast, we looked at these aspects specifically through the lens of their associations with access to and engagement with CR.
Methodology
Search Strategy
Our protocol is registered at the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42020182505), with deviations presented in Supplemental Table 1. It was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. 29 Bibliographic database searches were conducted using PubMed, Web of Science, and PsycINFO up to 5 May 2021. Reference lists of eligible studies and review articles were also searched. The following search string was used: “cognitive” OR “cognit*” AND “remediation” OR “enhancement” OR “intervention” OR “rehabilitation” OR “training” AND “schizophrenia” AND “access*” OR “accessibility” OR “attendance” OR “drop-out rate” OR “response rate” OR “engagement” OR “motivation.”
Study Selection
Titles and abstracts were screened against the eligibility criteria by a single researcher (RAEA). Next, full-text screening was conducted by 3 researchers independently (SLR, EJT, and RAEA). Disagreements were then discussed to reach a consensus. Inclusion criteria consisted of (1) studies published in peer-reviewed journals in English, French, and Mandarin (i.e., languages known to the authors); (2) inclusion of a CR intervention arm (as defined by the CR Expert Working Group 1 ); (3) inclusion of at least 1 group of participants with schizophrenia spectrum disorders, as diagnosed using the Diagnostic and Statistical Manual of Mental Disorders IV or 5 2 or the International Classification of Diseases 10 or 11 criteria World Health, 3 and aged between 17 and 65 years old; and (4) inclusion of data about access and engagement, which could be qualitative or quantitative (e.g., dropout rates, themes from qualitative data). We excluded studies focusing only on Cognitive Behavioural Therapy, studies including Cognitive Adaptation Training (e.g., Hansen et al. 30 ) without a CR component, following CR definition, 12 as well as protocol papers, single case studies, case series, and reviews/meta-analyses. All CR papers meeting these criteria were included, independent of design type (i.e., open-label, single-arm, and randomized controlled trials), to maximize available data. Finally, different studies using the same cohorts were included, if they met the inclusion criteria and provided different engagement/access information across publications.
Data Extraction
The following data were extracted: publication year, geographical location, type of intervention and settings, participant information, measures of access and engagement (e.g., dropout rates and attendance rates; see Supplemental Table 2), and main outcomes in neurocognition (see Supplemental Table 3). All data were extracted from the CR arm only. The authors were contacted for further information where appropriate. We reported results in a narrative synthesis summarizing study characteristics, access and engagement data, and precise in the subheadings below for brevity.
Results
Summary of Study Characteristics
Sixty-seven papers were included (see Figure 1), with 3,732 participants and 2,471 receiving CR, in 57 cohorts. Some papers reported on the same cohort, but with distinct engagement and access data. This was the case for 3 Bryce papers,13,31,32 3 Medalia papers,33–35 3 papers from another Medalia cohort,36–38 2 Wykes papers,39,40 2 additional papers from Wykes team,41,42 2 Cavallaro papers,43,44 and 2 Light papers.45,46 Intervention descriptions and neurocognitive outcomes are presented according to a cohort. Supplemental Table 2 summarizes study characteristics. Of 57 unique cohorts, 43 (75.4%) received neurocognition-based interventions, 10 (17.5%) social cognition, 3 (5.3%) a mix of neurocognition and social cognition interventions, and 1 (1.8%) presented 2 distinct interventions, 1 focusing on neurocognition and the other on social cognition. The majority of studies delivered computer-based cognitive programmes (n = 40; 70.2%). Eleven used paper-and-pencil/manualized interventions (19.3%), 4 (7.0%) used a mixed mode of delivery, 1 study (1.8%) had 1 arm of computerized CR and 1 arm of computer plus paper-and-pencil CR, and 1 study (1.8%) used a smartphone app. Twenty-nine interventions (50.9%) included 1 or several of the following as part of the CR intervention: use of bridging groups, work on personal goals, and transfer to everyday life. The other half (n = 28, 49.1%) did not mention using these features. Interventions were delivered in a group setting for 26 (44.8%) studies, individually for 17 (29.3%), in a group setting but with individual completion and little interaction for 2 (3.4%) and using a mix of group and individual delivery for 3 (5.2%) studies. One study used group delivery with the possibility of individual sessions (1.7%), and 9 (15.5%) studies did not report this information.
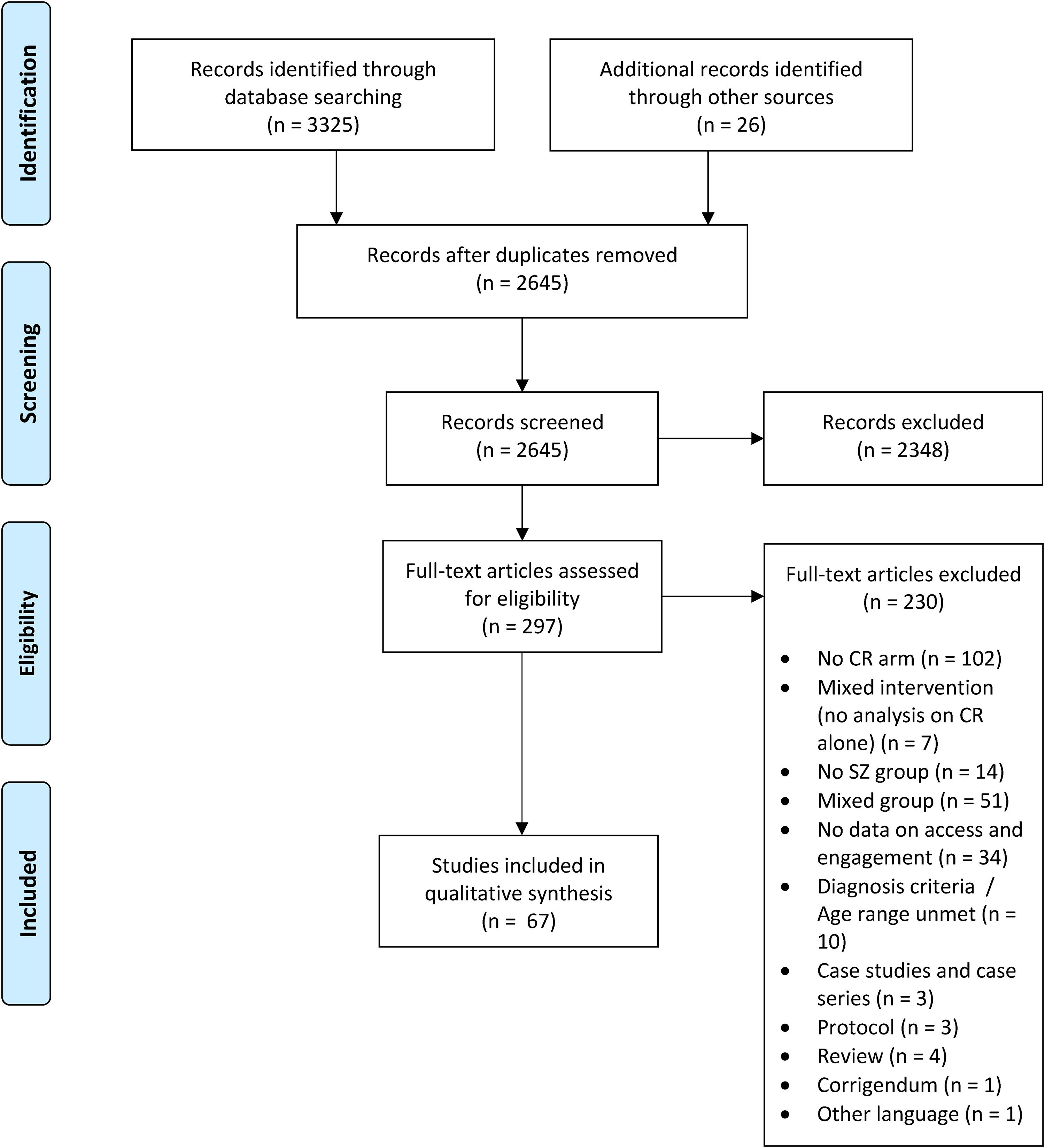
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram.
Access Data
Place of delivery and population
Fifty (87.7%) cohorts received interventions on-site, whereas only 3 (5.3%) received it remotely, and 4 (7.0%) via a mix of on-site and remote delivery. Thirty-two (56.1%) cohorts were composed of outpatients, 6 (10.5%) inpatients, 9 (15.8%) were a mix of in/outpatients, 2 (3.5%) forensic inpatients, 5 (8.8%) were outpatients in supported residential care, and 3 (5.3%) were not specified. Most studies were conducted in Europe (28; 49.1%), with 8 from the UK (14.0%). Seven studies were based in Australia (12.3%), 14 in the US (24.6%), and 1 in Canada (1.8%). In Asia, there were 2 studies from China (3.5%), 2 from Japan (3.5%), and 2 from South Korea (3.5%). One study was multisite: India and the US (1.8%).
Engagement Data
Dropout rates during intervention
Overall, dropout rates ranged from 0% to 47.5% (median = 14.29%). The distribution of dropout rates by the number of CR interventions is presented in Figure 2, excluding those reported as lost to follow-up. Reasons for dropout are reported in Supplemental Table 2.
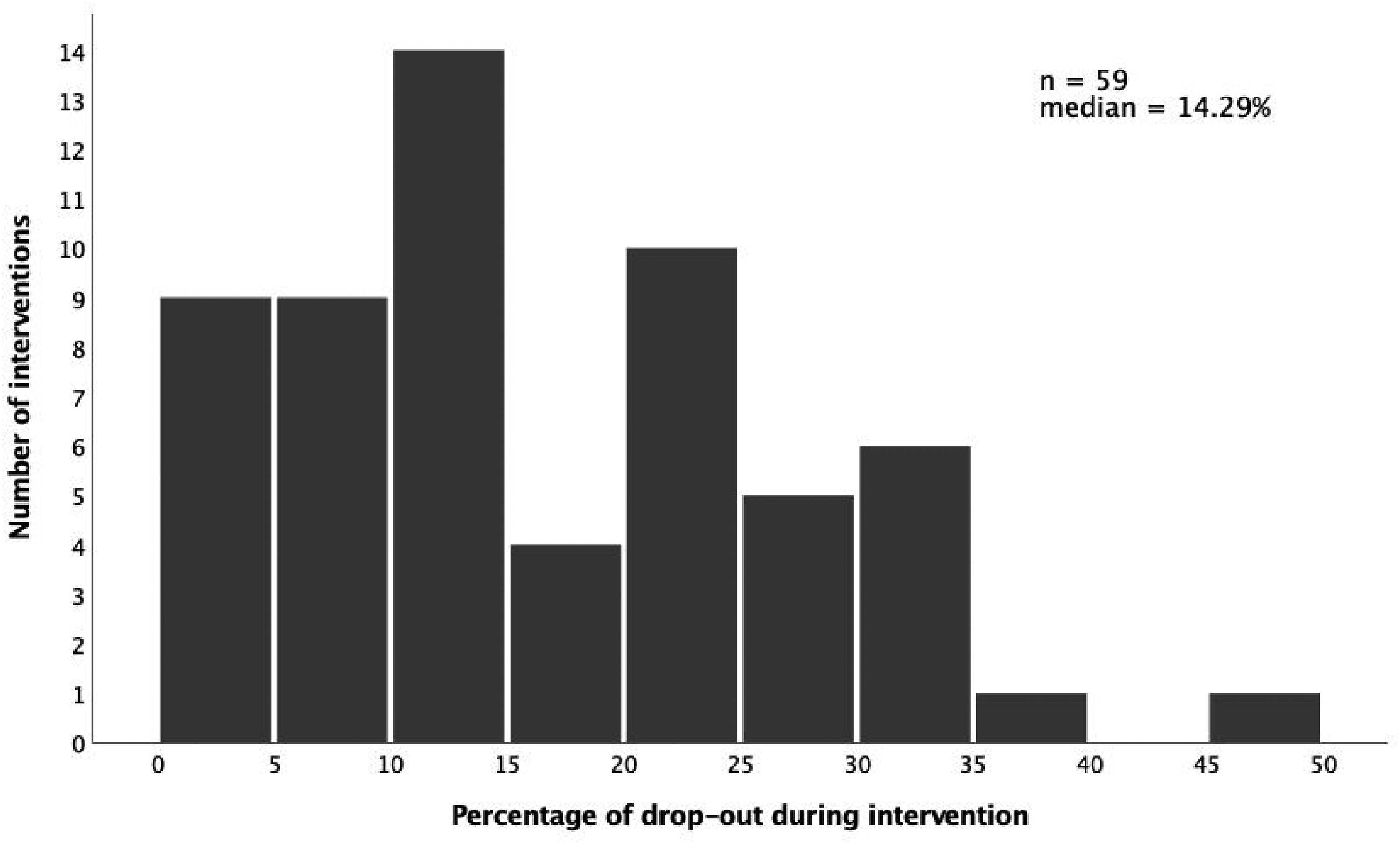
Bar graph of dropout rates during the intervention in 5% increments by a number of cognitive remediation interventions. *Fifty-nine interventions are considered; some studies reported multiple dropout rates because they included different cognitive remediation interventions; 9 papers did not report dropout rates; 10 overlapping cohorts are not represented.
Differences between dropouts and completers
Five papers (7.46%) analysed group differences between dropouts and completers, summarized here by variables investigated.
Demographics (4 Studies)
No significant differences were observed in demographic variables (gender,47,48 age,13,47–49 years of education,13,48 IQ, 13 employment/occupational status,47,49 or living situation 47 ) in all studies comparing dropouts to completers.
Clinical characteristics (4 Studies)
Dropouts presented higher levels of negative symptoms (P = 0.019). 13 Conversely, no significant group differences were observed in overall symptomatology, 49 medication13,47 (in a number of people treated with clozapine), and duration of illness. 47
Neurocognitive functioning (2 Studies)
Bryce et al. 13 found lower baseline global neurocognitive functioning in dropouts at trend-level significance (P = 0.064). However, another study reported no such differences when examining neurocognitive outcomes (data not reported). 48
Self-efficacy (1 Study) and intrinsic motivation (1 Study)
Compared to completers, dropouts exhibited significantly higher baseline self-efficacy (P = 0.011) 13 and reported significantly lower task interest (P = 0.02) and task value (P = 0.001) on the Intrinsic Motivation Inventory for Schizophrenia Research (IMI-SR) regarding their allocated programme. 32
Differences in engagement variables between CR intervention types
Twelve papers (17.91%) analysed differences in intervention engagement between multiple interventions. First, comparing individual and group CR, Cella et al. 50 found a trend for participants attending more sessions in individual CR (P = 0.057). Fiszdon et al. 51 compared CR (i.e., a brief, computerized math-learning programme) delivered using motivational interviewing (CR + MI) with CR using a control interview (CR + CI). Session attendance was higher in CR + MI than in CR + CI (P < 0.001). Investigating 2 different social cognition interventions, Marsh et al. 52 highlighted higher attendance for Emotion Recognition Training (85.71%) compared to the Mental-State Reasoning Training (67.86%). Andreou et al. 53 found better attendance in the metacognitive therapy (MCT+) group compared to the CogPack intervention (P = 0.001), and lower early dropout rates (i.e., participation <4 sessions; P = 0.006). Conversely, 8 studies reported non-significant differences between interventions in terms of dropout/attrition rates (Mahncke et al. 48 : CR vs control, P = 0.12; Mueller et al. 54 : Integrated Neurocognitive Therapy vs treatment as usual (TAU), P = 0.46; Thomas et al. 45 : Targeted Cognitive Training vs TAU, P = 0.10; Jahshan et al. 55 : BrainFitness vs CogPack vs Sporcle control group, P = 0.31; Lim et al. 56 : Social Cognitive Skills Training + TAU vs TAU, P = 0.55) and/or average completed sessions/completion rates/weekly training time (D'Souza et al. 57 : CR alone vs CR + D-Serine vs D-Serine alone vs control video watching, P = 0.66; Jahshan et al. 55 : BrainFitness vs CogPack vs Sporcle control group, P = 0.22; Nahum et al. 58 : SocialVille vs control computer games, P = 0.34; Medalia et al. 59 : remote + on-site CR (hybrid CR) vs all on-site CR, P = 0.81).
Predictors of engagement and associations with other variables
Thirteen studies (19.40%) examined predictors of dropout or associations between engagement variables (e.g., session attendance) and other variables.
Engagement, motivation, and self-efficacy
Four papers described significant results for motivation assessments. Bryce et al. 32 and Fiszdon et al. 51 both reported that intrinsic motivation, assessed by the IMI-SR, was significantly positively associated with session attendance. Fiszdon et al. 51 supported associations with both the total IMI-SR score (P < 0.001) and all the subscales (all P < 0.05), while Bryce et al. 32 only observed a correlation with the value/usefulness subscale (P = 0.01). Conversely, a study by Saperstein et al. 37 reported no significant association between baseline IMI-SR score and session attendance. However, a significant correlation between higher baseline Perceived Competency (PC; i.e., a measure of self-efficacy) and shorter time to treatment completion (P = 0.025) indicated greater engagement. Furthermore, PC was found to fully mediate the relationship between subjective awareness of deficits or insight (Measure of Insight into Cognition-Self-Report [MIC-SR]) and perceived value of treatment (IMI-SR) at post-treatment (MIC-SR ≥ PC: P = 0.025; PC ≥ IMI-SR: P < 0.001). 37 Saperstein et al. 37 found treatment intensity, in the same cohort, to be significantly positively correlated with PC (P = 0.003) but not with IMI-SR scales (all P > 0.10). Using another measure of motivation-related perceptions of the training environment (i.e., the MUSIC® Model of Motivation Inventory), they showed that attendance was significantly positively correlated with usefulness (P = 0.02) and success (P = 0.048) subscales. 38 Finally, Gooding et al. 60 found that intrinsic motivation, PC, and perceived autonomy were not significantly related to CR treatment utilization (TU; i.e., average session attendance calculated as the ratio of attended sessions to scheduled sessions; all P > 0.10).
Engagement, demographics, and clinical variables
Gooding et al. 60 reported that education (P = 0.006) and estimated premorbid IQ (P = 0.046) were positively and significantly correlated with TU. Conversely, 2 studies found no significant predictor of dropout when looking at participant baseline characteristics,61,62 and 1 found no significant association between attendance and change in positive and negative symptoms. 42
Engagement and baseline neurocognitive functioning
In Gooding et al., 60 higher TU was significantly correlated with better global neurocognitive functioning (P = 0.007). Specifically, higher TU correlated with better attention and working memory (P = 0.03), processing speed (P = 0.01), verbal learning (P = 0.07), and executive functioning (trend-level; P = 0.058). Moreover, controlling for premorbid IQ, more self-reported neuropsychological complaints (MIC-SR) were associated with lower TU (P = 0.008). Finally, the authors conducted 2 hierarchical regression analyses to explore the combined and individual contributions of self-reported and objective neuropsychological variables to TU, controlling for premorbid IQ. Both objective (ß = 0.51, P = 0.001) and subjective neuropsychological assessments (ß = −0.44, P = 0.002) provided unique contributions to the model, accounting for 44% of TU variance (P < 0.001). The second model that included the different neurocognitive domain scores, attention/working memory (ß = 0.40, P = 0.041) and MIC-SR total score (ß = −0.45, P = 0.002) were unique contributors to the model, accounting for 48% of TU variance (P < 0.001). 60
Harvey et al. 63 examined the single effects and interaction of diagnosis and cognitive status (i.e., BACS <41 and BACS >41) on training engagement and found no significant effects (all P > 0.20).
Engagement and cognitive outcomes
Four papers investigated links between engagement and cognitive outcomes of the intervention. First, better improvement rates (mean = 68.1%, SD = 8.96, range = 46–87) significantly correlated with a higher total number of completed tasks (r = 0.36, P < 0.05), but did not significantly correlate with session attendance (r = 0.29, P > 0.1). 64 Second, better session attendance was associated with greater non-verbal executive improvement (r = −0.31) at 12 weeks, and better task completion and a higher number of useful strategies were associated with improvement in visual memory (r = 0.39 and 0.24, respectively). 41 Analysis of a subsample of this latter study found similar results. Greater task practice (i.e., the average number of tasks per session) was associated with improvements in non-verbal memory (r = −0.4, P < 0.05) and executive functions (r = −0.38, P < 0.05), and the average number of useful strategies with non-verbal memory improvements (r = −0.29, P < 0.05). 42 Finally, 1 paper found no significant correlation between their social cognition outcome and any of the training data (i.e., total level count (P = 0.123); days of training (P = 0.292); levels completed by day (P = 0.672)). 58
Engagement and therapeutic alliance
Two studies examined associations between therapeutic alliance and treatment engagement. Results showed that client-rated therapeutic alliance was significantly and positively correlated to CR duration (P < 0.01), 65 but no significant correlations were found between therapeutic alliance and either total number of tasks or average task per session completed. 42
Qualitative Data and User Experience
Of 67 papers, 15 evaluated user experience (22.39%), either qualitatively (interview, qualitative survey, or clinicians’ notes analysis; n = 7) or with a satisfaction questionnaire (n = 7), and 1 used both. Features of access and engagement are reported in Supplemental Table 4. Overall, the majority of papers reported good tolerance and satisfaction, with some negative comments such as feelings of frustration, 66 challenges to staying focused, 67 anxiety during tasks, 68 security concerns, 69 or general difficulties related to attending sessions. 50 The 4 papers that examined the therapist role all reported positive feedback.50,59,66,70 Some programme features were valued such as guidance, feedback, environment and shared experience, 70 programme attractiveness,67,69,71 the wide variety of exercises, 31 and enjoyment at improving on tasks. 66 Hybrid CR participants in Medalia et al. 59 also valued the sense of independence. Negative aspects included some level of programme use difficulty, 69 difficulties of tasks,50,66 and leading to a sense of failure. 66 Suggestions for improvement included a more interactive structure, 50 the use of more updated and varied exercises 31 and less repetitive exercises.31,68
Regarding computers, most studies reported good acceptability and ease of use66,69,70 with a few participants reporting difficulties. 66 However, computer access and proficiency were major barriers in Medalia et al. 59 Comments on a group format were mixed. While a large majority of participants valued the group format,50,70 reported beneficial aspects such as engaging with peers 59 and sharing with people having similar issues, 72 others encountered difficulties in discussing their issues 72 within groups, leading to distraction, feelings of insecurity and competitiveness. 70 Some appreciated the “quiet time” to complete their homework alone, emphasizing improved concentration. 59 (p. 4) Some participants would have preferred individual sessions,31,72 whereas some would have liked bigger groups. 50 Finally, intervention duration was the most negatively rated area, but also less often evaluated (6 of 15 studies). Participants reported the intervention as “too intense” 50 (p. 7) and the total duration required commitment 70 or was too long/disliked the time commitment.31,68,71 Positive feedback was given in 1 study only, with some participants preferring more sessions. 66 Additionally, 1 study explored qualitative trajectories using clinicians’ weekly notes on inpatient participation in CR. Their results showed that most improved over time (7 of 9 participants), with 2 participants showing deterioration. The CR group showed greater variability in their participation trajectories, compared to the TAU group. However, these variations did not seem to impact the trajectories of other themes (i.e., social functioning and symptom severity). 46
Discussion
The current study aimed to systematically review available data on access and engagement of CR in schizophrenia. We aimed to determine the factors that impact access and engagement, and establish barriers and facilitators of CR implementation. We identified the following access data across the included studies: place of delivery, setting, and intervention characteristics. For most studies, engagement variables were dropout rate, reasons for dropout, session attendance, and CR duration or time to completion. Both access and engagement were also assessed with available qualitative data.
Factors Influencing CR Access
Most interventions were delivered in middle- to high-income countries. This aligns with previous research showing a greater treatment gap in low-income countries,73,74 and emphasizes the need to address international disparities in mental health care provision. The majority of interventions were delivered on-site, which could itself be a barrier to CR uptake. Considering the recent COVID-19 global pandemic, the need for digital remote interventions is increasing.75–77 While circumventing restricted movements outside the home due to the pandemic, allowing remote access to CR could increase uptake in individuals living in remote areas and experiencing transport difficulties. 57 In contrast, access to technology was identified as a major barrier to remote CR delivery. 59 Future research should aim to further trial remotely delivered CR to establish its feasibility, explore design conditions for its implementation and explore engagement factors. Finally, access to CR was mainly limited to outpatients. Broadening CR access to a range of illness stages, while adapting delivery to the targeted population, could increase the functional recovery of people with schizophrenia. This reflects a recent finding showing lower dropout rates in inpatients compared to outpatients. 27
Factors Influencing CR Engagement
Dropout rates and reasons for dropout
Dropout rates in this review (range = 0 to 47.5%; median = 14.29%) were similar to those reported in another recent systematic review (mean dropout rate = 16.58%). 27 Trial validity, and thus the credibility of a clinical trial, can be affected by attrition rates. 78 This is relevant to CR, compromising intervention benefits, especially considering the intensity threshold of CR. 28 Varied reasons for dropout included symptom exacerbation, change of residence, lack of interest, lack of perceived relevance, travel burden, time constraints, etc. (see Supplemental Table 2). Despite some studies showing high attrition rates, qualitative data revealed overall good acceptability, further supporting intervention utility. No major differences were observed in study characteristics of interventions presenting low versus high attrition rates (see Supplemental Material 1). Notably, only half of the included studies mentioned using bridging groups, transfer techniques, or work on personal goals, which could impact participants’ engagement. Although we did not find a significant difference in dropouts depending on the presence/absence of bridging groups, previous research showed the importance of including all core aspects of CR, as presented in Bowie, 23 to improve acceptability. 27 These should be systematically implemented when delivering CR.
Predictors of dropout
The small number of studies examining differences between dropouts and completers, and associations with or predictors of engagement, reported heterogeneous results. Dropouts had higher negative symptomatology and baseline self-efficacy, and lower baseline cognitive functioning and intrinsic motivation. Limited data suggest positive associations between engagement and intrinsic motivation, self-efficacy, educational level, and premorbid IQ. In contrast, Vita et al. 27 showed better acceptability of CR in participants with lower education and premorbid IQ. Further work is thus needed to understand the factors influencing both dropout and acceptability and their intricacies. Additionally, our results showed lower CR engagement in individuals with lower neurocognitive functioning and those with higher neurocognitive insight. Therefore, completing a comprehensive neurocognitive assessment alongside CR delivery is essential to ensure that clinicians explicitly implement strategies to keep lower functioning participants interested and engaged. More careful work is perhaps also needed on the therapeutic alliance, as the presence of an active and trained therapist is a core moderator of CR efficacy. 28 Our synthesis presented here shows an active and trained therapist could also be a core aspect of CR engagement. Our results on attrition differences between interventions suggest that, rather than location or delivery format, the use of techniques to increase engagement, such as motivational interviewing, could be key in preventing dropout.
Neurocognitive Outcomes and CR Engagement
Finally, a few papers have proposed links between engagement and neurocognitive outcomes. If the neurocognitive outcome is indeed related to training engagement, it means that engagement could be essential to achieving CR goals. Factors associated with improvements/CR efficacy have been identified in previous studies, including lower education, lower premorbid IQ and higher baseline symptom severity. 28 In the current review, lower education, lower premorbid IQ, and higher negative symptomatology were associated with poorer engagement. Ultimately, this suggests that individuals at higher risk for dropout should not be denied a CR intervention, especially since these risk factors could be facilitators of efficacy. Contrarily, CR should be offered to clients at higher risk but with ongoing support from the therapist and other strategies to ensure adherence (e.g., motivational interviewing and work on personal goals).
Suggestions for Future Research
Future research should seek to determine moderators of engagement alongside efficacy to optimize intervention designs. For example, thresholds for duration and intensity should be investigated for both efficacy and engagement. Similar to Vita et al. 27 meta-analyses, we did not find a significant association between intervention duration and dropout rate (see Supplemental Material 1), but qualitative data suggest that duration could be an engagement barrier, supporting further research in this area. These data stress a need to personalize CR interventions as much as possible, titrate task difficulty appropriately, and work on personal goals to maintain intrinsic motivation and PC. Intervention duration, variety of tasks, programme attractiveness and interactivity are all factors that need to be considered. Working with consumer feedback on adapting CR programmes will help with engagement and identify areas for improvement.
Some aspects remain underinvestigated as possible consumer factors impacting engagement, such as metacognitive skills that are essential for goal setting and behaviour change, as well as self-stigma and insight. Internalized stigma can lead to self-esteem decline and has been linked to poorer psychosocial treatment engagement.79–81 Individuals with poorer self-esteem tend to have increased feelings of hopelessness, thus believing less strongly in rehabilitation benefits. 82 Insight into cognitive functioning, and the broader illness, is intrinsically related to the perceived usefulness of rehabilitation. 83 The benefits of combining multiple rehabilitation interventions can counteract these issues. For example, CR has been shown to lead to better functional outcomes when delivered in conjunction with other psychosocial rehabilitation interventions.84,85 It has even been suggested that CR could enhance engagement in adjunctive psychosocial treatment. 45 Finally, the specifics of intervention delivery (e.g., individual vs group format) could impact engagement/adherence. 86 Further research is needed to clarify which and how intervention characteristics influence participant engagement.
Methodological Considerations
There are 5 major methodological considerations. First, we noted some assessment heterogeneity for similar concepts across publications. Second, future research should maintain distinctions between their intervention versus control groups during data analyses, notably with dropouts, to avoid limiting their conclusions. Third, the inter-relationships between engagement factors remain unclear and should be investigated. Most studies included in our review examined simple correlations, preventing further conclusions on the nature of these relationships. Fourth, participant compensation is an important engagement factor that could not be investigated due to a large proportion of studies not reporting whether participants were reimbursed (see Supplemental Table 2). Despite evidence that reimbursement does not significantly affect dropout, 27 we could argue that participant compensation in research impacts the scalability of results, because most clinical settings would not pay patients to complete a rehabilitation programme or assessments. 87 In the current review, almost all studies looking at intrinsic motivation provided payment to participants for completing assessments. Considering that intrinsic motivation occurs, by definition, when task performance is in itself rewarding, without any external reward, 88 a bias might arise in these studies. Finally, it is worth noting that the current findings are not entirely representative of clinical contexts, especially given most CR research receives funding or is directly affiliated with CR programmes. In our review, 29.8% of studies either received funding directly related to the CR (e.g., the programme is supplied for free), or authors were affiliated with or developers of the programme they used. Conversely, 1 study mentioned having to limit the duration of CR due to funding limitations. 67 Funding plays a crucial role in accessibility, and this may limit the clinical generalizability of our results.
Caveats
Our conclusions on access were limited by the lack of data. Some implementation research exploring organizational and structural barriers to CR access such as staff training21,25,89 are highly relevant, but could not be included in the present review because they did not meet our inclusion criteria (e.g., no schizophrenia spectrum disorders group). To our knowledge, only a few studies have directly investigated the accessibility of CR26,89 and further research is needed. For the current review, it remains possible that we missed some relevant studies. Current terminology for dropout and engagement variables is heterogeneous, therefore we chose only the most commonly used term for our search string (i.e., dropout). The influence of publication bias on our results is plausible. Non-significant CR results might not be published as consistently as significant ones, thus some information about access and engagement could remain inaccessible; although the large number of studies included in this review represents a strength. Finally, our inclusion/exclusion criteria were limited to adults with schizophrenia spectrum disorders, so studies with mixed groups or that did not present distinct results for schizophrenia diagnosis could not be included (e.g., Best et al. 90 ). We also did not explore access and engagement of CR for youth with psychosis/first-episode. This is a highly important area for future research, considering that cognitive impairment often exists prior to the onset of psychotic symptoms and the importance of early intervention.5,91,92
Conclusion
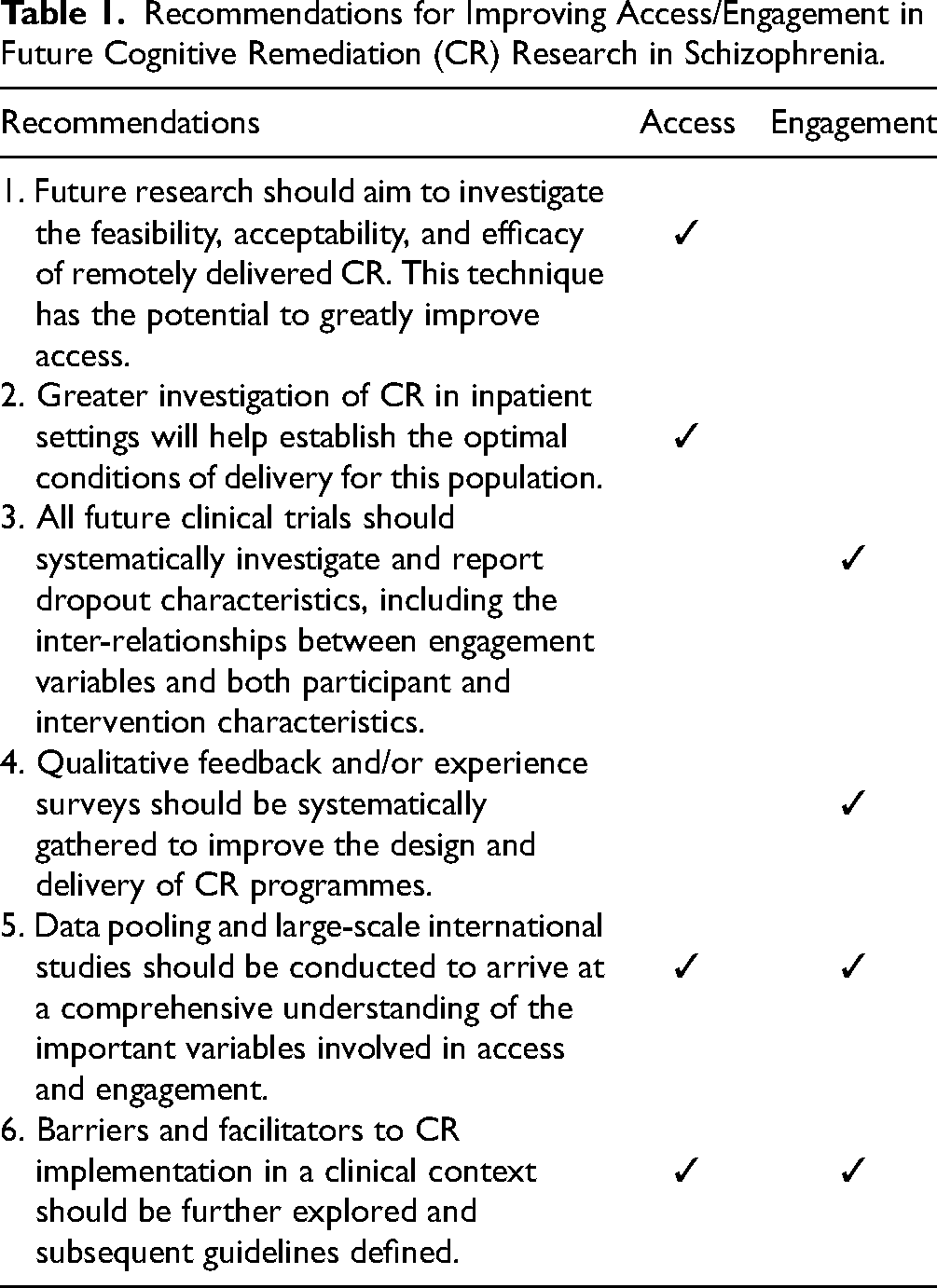
While treatment discontinuation in pharmacological approaches is consistently investigated; to our knowledge, this is the first systematic review investigating dropout rates and associated factors in CR, looking at both quantitative and qualitative data. Access to CR remains largely underinvestigated. Factors pertaining to participant and intervention characteristics have been identified as influencing engagement or adherence to CR. Implementing techniques to ensure participant engagement is essential, as engagement might also play an important role in efficacy. Future research recommendations are summarized in Table 1. Given the heterogeneity of the results, data pooling and large-scale international studies should be conducted to arrive at a comprehensive understanding with regard to the important variables involved in access and engagement.
Recommendations for Improving Access/Engagement in Future Cognitive Remediation (CR) Research in Schizophrenia.
Supplemental Material
sj-doc-1-cpa-10.1177_07067437221129073 - Supplemental material for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review
Supplemental material, sj-doc-1-cpa-10.1177_07067437221129073 for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review by Rosalie Ariane Eva Altman, Eric Josiah Tan and Susan Lee Rossell in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437221129073 - Supplemental material for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review
Supplemental material, sj-docx-2-cpa-10.1177_07067437221129073 for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review by Rosalie Ariane Eva Altman, Eric Josiah Tan and Susan Lee Rossell in The Canadian Journal of Psychiatry
Supplemental Material
sj-doc-3-cpa-10.1177_07067437221129073 - Supplemental material for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review
Supplemental material, sj-doc-3-cpa-10.1177_07067437221129073 for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review by Rosalie Ariane Eva Altman, Eric Josiah Tan and Susan Lee Rossell in The Canadian Journal of Psychiatry
Supplemental Material
sj-doc-4-cpa-10.1177_07067437221129073 - Supplemental material for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review
Supplemental material, sj-doc-4-cpa-10.1177_07067437221129073 for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review by Rosalie Ariane Eva Altman, Eric Josiah Tan and Susan Lee Rossell in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-5-cpa-10.1177_07067437221129073 - Supplemental material for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review
Supplemental material, sj-docx-5-cpa-10.1177_07067437221129073 for Factors Impacting Access and Engagement of Cognitive Remediation Therapy for People with Schizophrenia: A Systematic Review by Rosalie Ariane Eva Altman, Eric Josiah Tan and Susan Lee Rossell in The Canadian Journal of Psychiatry
Footnotes
Data Access
The data that support the findings of this study are available from the corresponding author, RAEA, upon reasonable request.
Author Contributions
RAEA, EJT, and SLR designed the study and wrote the protocol. RAEA conducted the literature search and title and abstract screening. RAEA, EJT, and SLR conducted the full-text screening. RAEA extracted data. RAEA wrote the first draft of the manuscript and all authors contributed to and have approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Swinburne University of Technology (Faculty Scholarship to RAEA); an Early Career National Health and Medical Research Council Fellowship (GNT1142424 to EJT); and a Senior National Health and Medical Research Council Research Fellowship (GNT1154651 to SLR). All funding sources had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.