
Abstract
Background
Obsessive-compulsive disorder (OCD) is a major mental health condition with a lifetime prevalence rate of 1.3% among adults. While placebo effects are well described for conditions such as depressive and anxiety disorders, they have not been systematically characterized in OCD.
Objectives
We aimed to determine the impact of placebos in improving different symptom domains in patients with OCD.
Methods
We systematically searched PubMed, EMBASE, Scopus, Web of Science, Ovid, the Cochrane Library, and Google Scholar databases/search engine from inception to January 2021 for randomized controlled trials of treatments for OCD with a placebo arm. A modified Cohen's effect size (ES) was calculated using change in baseline to endpoint scores for different measurement scales within placebo arms to estimate placebo effects and to investigate their correlates by random-effects model meta-analyses.
Results
Forty-nine clinical trials (placebo group n = 1993), reporting 80 OCD specific (153 measures in general) were included in the analysis. Overall placebo ES (95% confidence interval [CI]) was 0.32 (0.22–0.41) on OCD symptoms, with substantial heterogeneity (I-square = 96.1%). Among secondary outcomes, general scales, ES: 0.27 (95%CI: 0.14–0.41), demonstrated higher ES than anxiety and depression scales, ES: 0.14 (95%CI: −0.4 to 0.32) and 0.05 (95%CI: −0.05 to 0.14), respectively. Clinician-rated scales, ES: 0.27(95%CI: 0.20–0.34), had a higher ES than self-reported scales, ES: 0.07 (95%CI: −0.08 to 0.22). More recent publication year, larger placebo group sample size, shorter follow-up duration, and younger age of participants were all associated with larger placebo ES. Egger's test reflected possible small-study effect publication bias (P = 0.029).
Conclusion
Placebo effects are modest in OCD trials and are larger in clinician ratings, for younger patients, and early in the treatment course. These findings underscore the need for clinicians and scientists to be mindful of placebo effects when formulating treatments or research trials for OCD.
Systematic review registration number
PROSPERO CRD42019125979.
Introduction
Obsessive compulsive disorder (OCD) is a major mental health condition with estimated current and lifetime prevalences of 1.1% and 1.3%, with higher rates in women than men (lifetime prevalence 1.5% and 1.0%, respectively). 1 According to a national survey of United States households, the mean age of onset of OCD is approximately 19 years, with younger onset in males, and it rarely onsets after the third decade of life. 2 Beyond the core obsessive and compulsive symptoms, OCD impacts other mental functioning domains such as mood and anxiety. Generally, there is no significant gender difference in treatment response. 3 OCD is a neuropsychiatric disorder with different genetic, neurobiological, immunological, behavioral, and psychosocial factors interplaying in its psychopathology.4–6 Moreover, cultural factors, including religion, education, and ethnicity, have been conceptualized as relevant factors in OCD severity, age of onset, and manifestations. 7 Pharmacotherapy and psychological interventions are effective treatments for OCD in both children and adults. 8
Placebos, inert components of pharmacologic or non-pharmacologic interventions, have been described in the medical literature since the late 18th century and entered into the psychiatric lexicon more than a century later. 9 The placebo effect is defined as the subjective or objective clinical response to placebos or other non-specific benefits observed with treatments. 10 Note that the term placebo response has sometimes been used to refer to all effects seen in subjects receiving placebos while the term placebo effect has sometimes been used to emphasize only the specific impact attributable to the placebo's presumed mechanism of action. 11 However, these terms are often used interchangeably and for the purposes of this study, we will use the term placebo effect to cover both concepts.
Two factors known to drive the placebo effect are positive expectations and rewards. 12 It has been postulated that the neurobiological underpinnings of these mechanisms involve modulation of different neurotransmitters, including endogenous opioids, dopamine, and serotonin, within reward areas of the brain such as the prefrontal cortex, amygdala, and thalamus. 13 Some brain regions, including the dorsolateral prefrontal cortex, orbitofrontal cortex, rostral anterior cingulate cortex, ventrolateral prefrontal cortex, periaqueductal gray matter, and nucleus accumbens, are implicated in placebo effects in pain disorders. 14 Indeed, emotional status or immuno-hormonal responses can contribute to placebo effects.13,15 Person- and condition-specific factors may also play a role in placebo effects. For example, the nature of psychopathology, age, baseline severity, prior treatment trials, and duration of illness were all found to influence subjects’ response to placebo. 16 Study-related factors, such as year of publication, have also been found to impact the placebo effect. Kotzalidis et al. showed a trend of increasing placebo response in patients with OCD between 1991 and 2017. 17 Similar time trends in placebo effects have also been reported in depressive and anxiety disorders (ADs).18,19
Many systematic reviews and meta-analyses have been conducted to estimate the placebo effect in different psychiatric disorders including depression, 20 panic disorder (PD), 21 schizophrenia and schizoaffective disorder,22–24 and attention-deficit/hyperactivity disorder (ADHD). 25 For example, a systematic review of 6778 children and adolescent participants in 36 studies identified a substantial placebo response in ADs, depressive disorders (DDs), posttraumatic stress disorder (PTSD), and OCD. 26 To our knowledge, no systematic reviews have been conducted to delineate placebo effects in OCD according to different symptom domains and measurement types. This systematic review and meta-analysis aims to study placebo effects and their correlates in people with OCD to provide insights which may influence clinical care or research design.
Methods
The study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 27
Search Strategy
We systematically searched PubMed, EMBASE, Scopus, Web of Science, Ovid, the Cochrane Library databases, as well as Google Scholar search engine for potentially eligible studies up to 31 January 2021. The implemented search strategy for each database is described in Appendix 1. We applied searches for these keywords: “placebo” OR “nocebo” OR “placebo effect” OR “nocebo effect” OR “sham” AND “OCD” OR “obsessive-compulsive disorder” OR “obsessive disorder” OR “compulsive disorder” AND “randomized clinical trial” OR “clinical trial” OR “randomized trial.” Results were imported to EndNote 17.8 citation manager software (Thomson Reuters, Clarivate Analytics, Philly, USA), which was then used to remove duplicate citations. We implemented no search limits such as time or type of publication. We contacted corresponding authors to obtain additional study details necessary for the analysis that were unavailable within the manuscript.
Study Selection
We included randomized controlled trials (RCTs) published in English, which had at least one placebo arm, one or more biological intervention arm(s), and applied at least one standardized outcome measurement at baseline and end of the trial. The eligible studies included patients with OCD diagnosed based on the Diagnostic and Statistical Manual of Mental Disorders (DSM)-III, DSM-III-R, DSM-IV, DSM-IV-TR, and DSM-5. We excluded studies with no reported outcome data for OCD symptoms in placebo group or no placebo-only group. For this study, we have selected studies that have at least one biological (pharmacological or other, such as brain stimulation) intervention arm, therefore, the corresponding placebos in this review include pill placebos or sham placebos, corresponding to an ineffective intervention analogue.
Two reviewers independently screened the titles or abstracts of potentially eligible studies. In case of any discrepancies, they consulted with a third reviewer. The full texts of the included articles from the previous step were then reviewed by two authors with the third reviewer again resolving any disagreements regarding data extraction (see below for details).
Data Extraction
Two authors independently extracted data from the included studies, including study identifiers (name of the first author and year of publication), study attributes (study start year, study design, country in which the study was conducted, blinding status, and sampling setting), sample characteristics (total sample size, sample size of intervention and placebo arms, total and placebo group completion rate, number of subjects who withdrew/were lost to follow-up, duration of follow-up, percentage of males, mean age of placebo group, and ethnicity/race), disorder characteristics (type of OCD, i.e., first episode, recurrent, or treatment-resistant), characteristics of intervention(s) and placebo, and outcomes measurements (type and name of measurement tools, frequency of measurements, and baseline and endpoint mean and standard deviation [SD] of outcomes).
Quality Assessment
To evaluate the quality of included studies, a modification of the Cochrane tool for assessing the risk of bias in randomized trials-version 2 (RoB 2) 28 was used, without including the intervention group items.
Statistical Analysis
To calculate effect size (ES) estimates, we used baseline and endpoint means, and SDs in the placebo group for every outcome measurement tool. For studies using more than one outcome measurement, each measurement's statistics was considered as a separate entry in the analysis. If endpoint values were not reported separately, we calculated the endpoint mean from the pre-post value change, and used baseline SD as an estimate of endpoint SD.
29
As baseline and endpoint values were not independent, we used a modified Cohen's d formula to calculate effect size. This formula is as follows:

Results
Study Selection
The initial search identified 5,765 articles (see Figure 1 for details of the study selection process). After removing 3,521 duplicate records, 2,244 articles were included for title/abstract screening, which resulted in the exclusion of a further 1,970 articles. Among the remaining 274 articles, 225 did not fulfill the eligibility criteria, with 49 articles ultimately included in the meta-analysis.
Study selection process. OCD = obsessive compulsive disorder; RCT = randomized controlled trial.
Study Characteristics
Overall, the 49 eligible articles (published between 1980 and 2020) included 1,993 participants in their placebo arms. Studies followed up the participants for a range of one to 80 weeks with a mean of approximately 13 weeks. Across the studies, the overall mean age ± SD of participants in the placebo groups was 31.8 ± 10.5 years old and with a relatively even distribution of sexes (almost half of the participants, 48.2 ± 12.0%, were male). In terms of study completion, 83.6 ± 16.3% of the participants in placebo arms completed their respective trials. Mean follow-up duration and number of measurements were 13.3 ± 13.2 weeks and 6.4 ± 3.3, respectively (Figure 2).
Characteristics and calculated OCD-specific placebo effect sizes for the included RCTs (n = 1945, using 80 measurements) in patients with OCD. Age = in placebo group, years; CBT = cognitive behavioral therapy; CI = confidence interval; CR = controlled release; F/U = duration of follow-up in weeks; HR = high risk; ITT = intention-to-treat; LR = low risk; male (%) = in placebo group; measurements# = number of outcome measurements during the study; N = placebo group sample size; NAC = N-acetyl cysteine; OCT = obsessive compulsive disorder; PP = per-protocol analysis; quality = study quality for risk of bias, based on Cochrane tool for assessing risk of bias in randomized trials (RoB 2); RCT = randomized controlled trials; rTMS = repetitive transcranial magnetic stimulation; SC = some concerns; Tools# = number of different tools for outcome measurement in each study; Tx-Resistant = treatment-resistant OCD as the target of the study.
Pooled Placebo Effect Size
There was a total of 28 different outcome measurement tools (mean ± SD: 3.12 ± 1.95 tools utilized per study), corresponding to four outcome/symptom groups: OCD (8 tools), anxiety (6 tools), depression (7 tools), and general scales (7 tools). There was total of 80 OCD-specific outcome measure values(1.63 ± 1.01 OCD-specific tools per study). The overall estimated OCD specific placebo effect size was 0.32 (95%CI: 0.22–0.41) ranging from −0.03 to 0.58 across different measurement tools (Figure 3). Among individual tool types, Y-BOCS was the most used questionnaire to evaluate changes in obsessions and compulsions (in 38 studies, with an overall ES of 0.31 (95%Ci: 0.16–0.46) while the Children Y-BOCS (CYBOCS) showed the largest ES (0.57; 95%CI: 0.38–0.77, Figure 3). Notably, there were 24 different interventions were investigated in included studies. The pooled interventions effect size across all studies for OCD-specific outcome measures was 0.64, 95%CI: 0.53–0.75 (YBOCS intervention ES: 0.62, 95%CI 0.43–0.81) (Figure 3). In terms of other outcome measurements, interventions had a pooled effect size of 0.51 (95%CI: 0.10–0.92), 0.38 (95%CI: 0.27–0.50), and 0.35 (95%CI: 0.21–0.49) on anxiety, depression, and general scales, respectively.
Forest plot of the effect sizes of placebo effect by measurement tools. *The effect size for intervention group has been presented only for the purpose of comparing with the placebo effect size, and it does not reflect the efficacy of interventions in OCD due to heterogenous and diverse group of intervention types. **Sample size in placebo group. The sum of sample sizes outnumbers total sample size of studies as some studies have used more than one measurement tools. BAI = Beck Anxiety Inventory; CASS = Covi Anxiety Scale Schedule; CDI = children's depression inventory; CGAS = Children's Global Assessment Scale; CGI = clinical global impression; CPRS = comprehensive psychopathological rating scale - OCD subscale; GSI = General Symptom Index; HAM-A = Hamilton Anxiety Scale; HAM-D = Hamilton Depression Scale; LOI-CV = Leyton Obsessional Inventory-Child Version Symptom/Resistance/interference; MDRS = Montgomery-Asberg Depression Rating Scale; MOCI = Maudsley Obsessional Compulsive Inventory; NIMH-Anxiety = National Institute of Mental Health-Anxiety Scale; NIMH-Depression = National Institute of Mental Health-Depression Scale; NIMH-GI = National Institute of Mental Health-Global Impairment. NIMH-OC = National Institute of Mental Health-Obsessive-Compulsive Scale; OCD = Obsessive-Compulsive disorder; OCI = Obsessional Compulsive Index; OCR = obsessive-compulsive (OC) rating scale; BDI = Beck Depression Inventory; PGI = Patient Global Impression; PSCL = Physical Symptom Checklist; R = test–retest Reliability of each tool (used in calculation of modified effect size); RCMAS = Revised Children's Manifest Anxiety Scale; SAR-SR = Social Adjustment Scale-Self Rating; SCL-90 = 90-items Symptom Checklist (SCL −90 includes the whole scale and/or GSI/OCI subscales); SDS = Self-rating Depression Scale/Zung; STAI = State-Trait Anxiety Inventory; Studies No. = Number of studies using each tool/measurement; YBOCS = Yale-Brown Obsessive-Compulsive Scale.
Effect Size Based on Different Measurement Tools
The included studies utilized 153 outcome measure values (change from baseline), which were derived from 28 different measurement tools. The combined placebo effect, with aggregate data from all primary and secondary measurement tools in each study, was 0.24 (95%CI: 0.18–0.31), ranging from −0.56 to 1.45 across the studies and from −0.46 to 0.96 across different measurement tools (Figures 2 and 4). Among non-OCD tool groups, general scales (0.27; 95%CI: 0.14–0.41) had higher effect size values compared to anxiety scales (0.14; 95%CI: −0.04 to 0.32) and depression scales (0.05; 95%CI: −0.05 to 0.14) (Figure 3).
(a) The OCD-specific placebo effect in patients with OCD based on outcome measurement type, analysis protocol, placebo type, and participants’ characteristics. Age = studies on only 17 + year-old subjects have been categorized as adult; CI = confidence interval; ITT = intention-to-treat analysis or last observation carried forward (LOCF); K = number of measurements in each group; PP = per-protocol analysis; Tx-resistant = only Treatment-resistant OCD subjects were included in the study; based on the study's definition. (b) The all-measure placebo effect in patients with OCD based on outcome measurement types, analysis protocol, placebo type, and participants’ characteristics. K = number of measurements in each group; CI = confidence interval; ITT = intention-to-treat analysis or last observation carried forward (LOCF); OCD = obsessive-compulsive disorder; PP = per-protocol analysis; age = studies on only 17 + year-old subjects have been categorized as adult. Tx-resistant = only treatment-resistant OCD subjects were included in the study, based on the study's definition.
Placebo Effect Correlates
Almost all of the OCD-specific measurements (78 out of 80) were clinician-administered. However, among all primary and secondary measurement tools, more than half were clinician-rated (16 of 28 individual tools, including 129 of the 153 measurement values in the meta-analysis). Considering the administration type, two self/patient-rated OCD-specific measurements showed lower, but not significant, placebo effect size than the clinician-rated tools (0.11 ; 95%CI: −0.37 to 0.58 vs. 0.32; 95%CI: 0.23–0.42, P = 0.39, respectively). On the other hand, the all-measure placebo effect estimate using clinician-rated scales was significantly higher than that observed for self/patient-rated tools (0.27; 95%CI: 0.20–0.34 vs. 0.07; 95%CI: −0.08 to 0.22, P = 0.02) (Figure 4(a) and (b)).
Measurements derived using ITT analysis also provided a significantly larger placebo effect size compared to those using a PP approach (0.43; 95%CI: 0.28–0.58 vs. 0.20; 95%CI: 0.11–0.29, respectively, P = 0.01). A similar discrepancy in placebo effects based on the analysis type was found among all measure placebo effects estimates (0.37; 95%CI: 0.27–0.47 vs. 0.12; 95%CI: 0.05–0.19, for ITP and PP, respectively, Figure 4(a)). Moreover, there were no significant difference between pill placebo effect (n = 74, ES: 0.33) and sham intervention (n = 6, ES: 0.20), P = 0.42, (Figure 4(a)). RCTs with child/adolescent participants demonstrated higher placebo ES, 0.45, than those with adult participants (ES: 0.24, P = 0.02). Findings on different placebo effect sizes based on placebo type (pill vs. sham), and participants’ age group were also replicated for all-measure placebo effect estimates (Figure 4(b)). In contrast, there were no significant differences in placebo effect among studies with treatment-resistant OCD subjects and other studies, for both OCD-specific and all-measure placebo effect estimates (P = 0.63 and P = 0.97, respectively Figures 4(a) and (b)).
Meta-regression analyses further revealed that the placebo effect size had no significant correlation with baseline measurements (values and variance, as indicators of symptom severity), gender ratio among participants, number of measurement tools, and the intervention effect size. However, year of publication (r = 0.0114, P = 0.018), placebo group sample size (r = 0.0035, P = 0.003), participant mean age (r = −0.0074, P = 0.024), and duration of follow-up (r = −0.0115, P < 0.001) significantly correlated with placebo effect size (Figure 5). Notably, there were no significant age-related differences in placebo effect among studies with adult participants (37 studies, mean age: 36.4 ± 4.3 years old, P = 0.183).
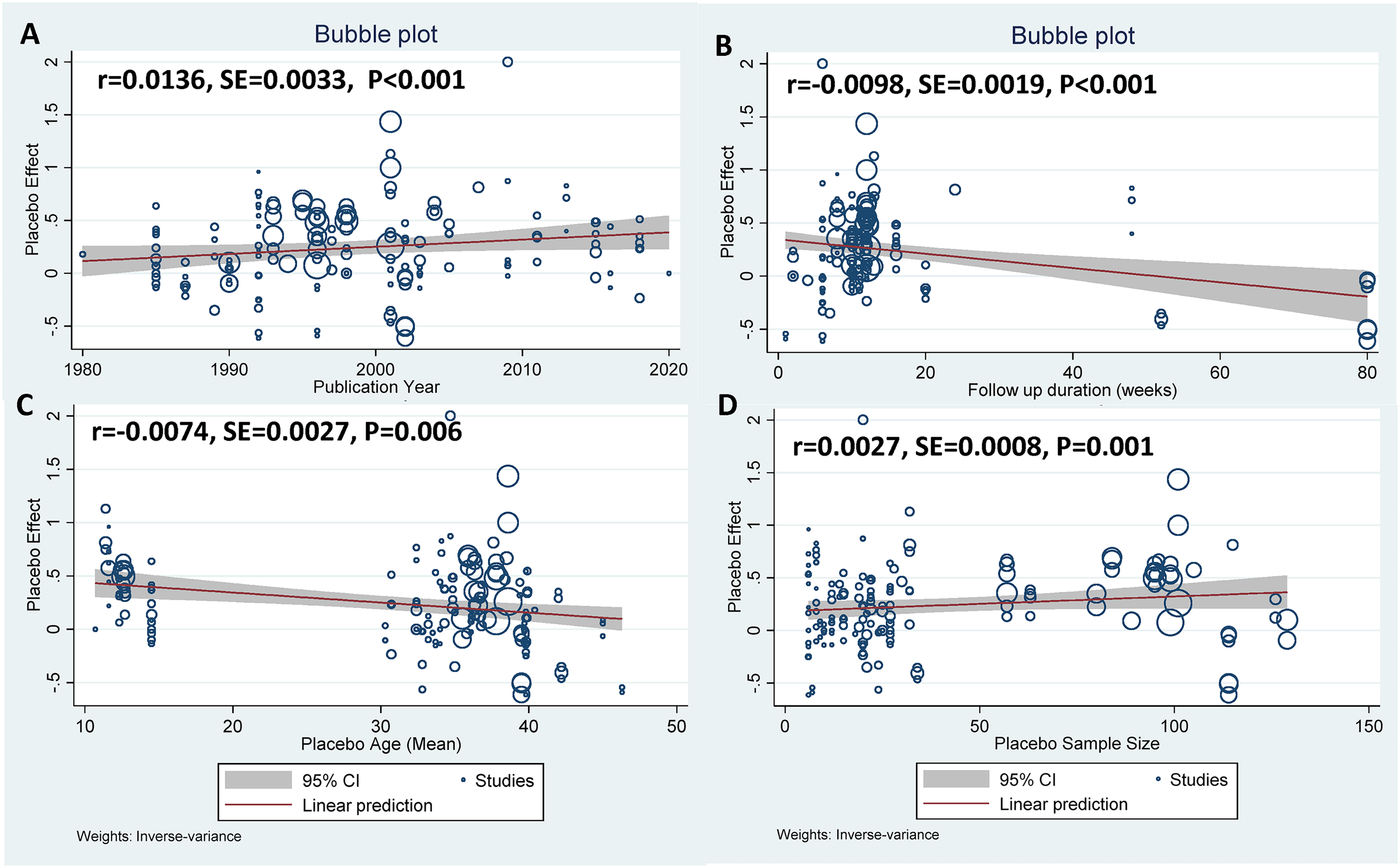
Meta-regression analyses on placebo effects in OCD based on: (a) publication year, (b) follow-up duration (weeks), (c) placebo group mean age (years), and (d) placebo group sample size. OCD = obsessive-compulsive disorder; r = regression coefficient; SE = standard error of r; CI = confidence interval; bubble's size correlated with the weight of each measurement based on inverse-variance.
Publication Bias
There was a significant small-study effect in this meta-analysis (Egger's test P = 0.029), which might indicate a publication bias of small studies (with higher standard error of measurements) being less likely to be published in OCD clinical trials with a placebo arm.
Discussion
In this systematic review and meta-analysis of RCTs, we found that treatment with placebos produced a modest overall effect size in patients with OCD compared to placebo effect sizes reported for other major psychiatric conditions such as DDs (ES: 1.57 19 ), ADs in general (ES: 1.03 18 ), and PD (ES: 0.56 21 ). Arguably, the effect size based on OCD scales, ES: 0.32, or more specifically based on YCOBS and CYBOCS, ES: 0.39 and 0.58, respectively, should be considered as a principal estimate of placebo effect in OCD. They are higher than the all-measure placebo effect, based on aggregated OCD-specific, ES: 0.32, and -non-specific measures, ES: 0.24. Nevertheless, it is sufficiently large to be meaningful both from a clinical and research design standpoint and, notably, there was substantial heterogeneity in placebo effect measurements across clinical trials in OCD. Compared to the interventions’ effect size (ES:0.64 on OCD scales), placebos are about 50% as effective as the intervention in people with OCD. Findings here suggest that several factors may lead to larger placebo effects in OCD trials. These include younger participants (who are known to be more susceptible to placebo effects 31 ), larger samples (who may be less carefully selected), and shorter studies (which may be more vulnerable to transient expectancy effects or random changes). Our findings also contribute to the literature showing that placebo effects may be increasing over time in research trials. 32
The placebo effect is a complex phenomenon that arises through the interaction of multiple factors including participant characteristics, the condition under study, and study-specific factors. Each of these broad factors consists of numerous sub-variables, many of which are not measured or reported in clinical trials. Therefore, systematic reviews have inherent limits in analyzing them. However, they can identify potential factors that can be the subject of further investigations as described above.
A systematic review by Cohen et al. compared the placebo response rate between patients with major DD (MDD), OCD, and ADs other than OCD . Theyreported that the placebo response rate in OCD was lower than the other disorders (31% in OCD compared to 49.6% and 39.6% in MDD and AD, respectively). 33 The study also found a positive relationship (Spearman rank correlation [ρ] = 0.1) between publication year and placebo response which was not significant. 33 The fact that this finding was significant in our study may arise from the difference in sample size (49 studies included here vs. six studies in Cohen et al.) and possibly the longer interval of published trials (1980–2020 of ours vs. 1992–2004 of Cohen et al.). 33 The results of another meta-analysis on PD by our group, with a similar methodology, likewise showed a higher effect size for placebo effects in PD compared to OCD (Cohen's d = 0.56; 95%CI: 0.50–0.63 in PD). 21 In that study, participants’ characteristics and type of outcome measures also impacted the placebo effect. In their systematic review, Breilmann et al. reported that the placebo effect in people with depression is correlated with baseline depression severity and the active intervention used. 34 In a meta-analysis of antidepressants response, Kirsch et al. also highlighted that the initial severity is correlated with lower placebo effects, which results in a wider drug-placebo difference in participants with higher initial severity scores. 35 In our review, meta-regression analysis did not find any significant correlation between participants’ baseline severity (and its variance) with the placebo effects. It is not clear what factors may contribute to the discrepancy in findings about the impact of initial severity on the placebo effects. Further research, especially with individual patient data (IPD) meta-analysis, could help identify potential factors.
A systematic review of 61 RCTs with 1,328 participants with MDD comparing the efficacy of sham repetitive transcranial magnetic stimulation (rTMS) on an acute depressive episode showed a significant effect size (Hedges’ g = 0.8, 95%CI = 0.65–0.95). 36 In their review, Razza et al. found publication year and treatment-resistant depression status to be positively and negatively associated with placebo effects, respectively. 36 Notably, sham rTMS has been found to have a significant effect, comparable to the active intervention, in treatment-resistant depression. 37 Our study did not find any significant differences in placebo effect estimates (both OCD-specific and all-measure ES) between studies with pill placebos and sham (rTMS or surgery). Inherently, placebo response involves factors beyond the placebo type per se, which includes potential shared and specific factors for different placebo types. Our study lacks reliable data to explore contributing factors in placebo effect based on the nature of placebos.
The lower placebo effects observed in patients with OCD compared to other psychiatric disorders such as MDD, AD, and PD might be related to the psychopathologic mechanisms of these disorders. Reportedly, people with OCD have lower response rates to different treatment modalities in general compared to depressive and ADs. For example, the response rates to serotonin-specific reuptake inhibitors (SSRIs) are lower in OCD. 38 Moreover, the suggested neurobiological mechanisms of placebo effects are alterations in dopamine and opioid neurotransmitters in addition to functional alterations in some brain regions, including rostral anterior cingulate, insula, nucleus accumbens, amygdala, thalamus, hypothalamus, and periaqueductal grey, along with orbitofrontal and dorsolateral prefrontal cortices.39,40 Comparing the regions affected by placebos with those implicated in psychiatric disorders shows that OCD had the fewest areas of overlap that potentially could be affected by placebo, which may result in a lower placebo effect in OCD. While these brain regions, mostly involved in the limbic system, are shown to be functionally and structurally impacted in MDD and AD,41,42 OCD generally lacks direct involvement of the insula, nucleus accumbens, amygdala, and periaqueductal grey area.43,44
The correlation between publication year and the placebo effect is an interesting finding that is challenging to interpret. Our review demonstrated a slight, significant increase in placebo effect size across OCD trials over the last three decades (at approximately 0.14 increments in placebo ES per decade). Some other studies, for example, systematic reviews of the placebo effect in antidepressant trials,19,32 anti-psychotic trials, 45 rTMS trials,36 among people with dementia, 46 or major ADs, 18 have also shown similar incremental trends in placebo effect by publication year. However, these findings are not consistent. 47 For example, a systematic review by Furukawa et al. examining placebo effects in depression, over a 25-year period, showed a consistent rate/no change over time.34,48 It has been argued that the sample characteristics, such as age and baseline symptom severity profile, and study characteristics, such as sample size, follow-up duration, and frequency of assessments may impact the placebo effect.45,46,49 Changes in these factors in trials over time might influence time trends in the placebo effect. In our study, however, we did not find any significant correlation between the study's publication year and many of these factors, including subjects age, sample's sex ratio, baseline symptoms severity, follow-up duration, frequency of measurements, or sample size. On the other hand, some of these factors, (e.g. age, follow-up duration, and sample size) showed an independent, significant impact on the placebo effect size in the meta-regression analysis. Specifically, the ES was higher in more recent studies, those with larger sample size, with younger participants, and shorter follow-up duration (Figure 5). Another speculative explanation for the time trends observed in placebo response is that in earlier OCD research, occurring in the 1980s or before, pharmacotherapy was focused almost exclusively on a single medication (clomipramine) and, therefore, many people in RCTs were treatment naïve. Later OCD studies, for example examining SSRIs, particularly by the late 1990s and beyond may have included more patients who had previously failed other agents. This might have led to increased urgency for participants and clinicians to observe a therapeutic response in those randomly allocated into trial arms, and hence perhaps a higher placebo response.
In this systematic review, we extracted data from all 28 different individual tools utilized as outcome measurements to explore the potential differences in placebo effect size across a range of target outcomes. To our knowledge, most, if not all, of the systematic reviews of the placebo effect have confined their analyses to one main outcome measure. Considering the complexity of symptom domain in psychiatric conditions, including OCD, which could generally impact other symptom domains (such as mood, anxiety, and overall function), we pooled the data from all reported outcome measurement values. Our findings highlight the significant heterogeneity between not only different scale categories, but also individual scales (Figures 3 and 4(a) and (b)). In our study, the main placebo effect in people with OCD was derived from OCD-specific symptom domains. This might at least in part be explained due to the studies’ inclusion criteria that usually excluded patients with comorbid and treatment-resistant conditions. Therefore, participants would be less likely to have underlying depressive or anxiety symptoms amenable to the placebo effect. Furthermore, in studies on OCD, the main treatment goal is about OCD-specific symptoms, which could expectedly result in more improvement in the target symptoms, compared to other concurrent conditions, by either placebo or the interventions. The variable placebo effect on the symptom domains can be a point of consideration in clinical practice where patients with OCD would have a different clinical picture with up to 75.8% and 63.3% comorbid anxiety and mood disorders, respectively. 2 Additionally, our study did not aim to and does not have all data to investigate all sources of heterogeneity in placebo effect among different OCD trials, but we believe that the diverse range of placebo efficacy, at some level, may be related to the differences in placebo's mode of action on a variety of symptom domains. We suggest that future systematic reviews on placebo effects (focused on overall efficacy of trials in general) specify the source of outcome measurement data to avoid combining data from heterogeneous sources and to provide tool-specific analyses findings.
Regarding the source of data for outcome measures, most tools in the studies included in our review (78 out of 80 in OCD-specific tools; 129 out of 153, 83.8% of all measurement tools) were clinician rates scales. Our findings showed that clinicians were more likely than participants themselves to identify larger benefits of placebos. While clinician-rated measurements showed a substantial placebo effect, the placebo effect based on self-report outcomes was not significantly different than zero. Keeping in mind the limitation for generalizability of patient-rated effect size, due to the small sample size, the higher placebo effect size based on clinician ratings may suggest that clinicians are overestimating and/or that participants are underestimating non-specific improvements in OCD treatment, which may be related to differences in interpreting patients’ subjective experiences between clinicians and patients themselves. To our knowledge, comparisons between placebo effect estimates driven from clinician- or patient-data sources have not been published in most similar systematic reviews.However, a similar pattern of significantly higher placebo effect based on clinician-rated scales has been found in PD. 21 A discrepancy between clinician's and patient's assessment of mental health disorders, for example in depression, has also been reported in some other studies. 50 Few systematic reviews of placebo effects have differentiated between those measured by clinician versus patient-rated scales. While studies examining placebo effects in MDD indicate similar findings of higher placebo effects in clinician-based measures,19,51 Hodgins et al. reported no difference in placebo effects across patient and clinician-rated scales in people with PTSD. 52 A poor correlation between patient and clinician ratings has been reported by Dunlop et al. for the response rate of depression treatments, 50 however they did not include a placebo arm in their trial. On the other hand, while research may suggest better validity of clinician-rated tools, 53 some argue that clinicians may be more susceptible to observers’ bias, especially when the integrity of the blinding process is questionable.51,54 Notably, systematic reviews of the placebo effect in psychiatric conditions have typically used a single outcome measure in meta-analyses, usually a clinician-rated tool, for example, Hamilton Depression Rating Scale (HAM-D) for depression. 55 In summary, it is not clear, based on the present literature, if this discrepancy in placebo effect findings based on data source is attributable to the underlying condition (MDD, PTSD, or OCD), study characteristics (such as inclusion criteria, sample size, and response definition), the mere nature of clinician-rated tools (such as clinician optimism, the role of the clinical encounter, which is inevitable for the administration, and/or bias in translating participants’ subjective reports), or some combination of these factors. This topic deserves further investigation as each of these circumstances has potentially important implications for clinical practice and research design.
This study has some important limitations. First, our review has only considered placebo effect of biological interventions and has not included psychological placebos. We did not search the PsycINFO database, a database which focuses on journals with an emphasis on publishing trials of psychological interventions. Second, despite our best efforts, including emailing the corresponding authors, we could not access the full text of five studies. Third, due to the lack of reported data, we could not evaluate factors contributing to the placebo effect in different types of placebos, such as sham, and pill placebos. IPD meta-analysis, with data on participants, setting measurement tool characteristics,and their sub-scales, could be potentially helpful to address this limitation in future. Fourth, our overall effect size estimates are pooled together from all outcome measures of the placebo arms regardless of their methodologies, including their inclusion criteria and washout period, as well as tool characteristics, such as psychometric characteristics and their target symptom domain. Besides the inevitable concerns with aggregate-data meta-analysis from different sources, this may have contributed to the heterogeneity of the findings. Nevertheless, we tried to overcome this by reporting meta-analysis findings for individual and grouped measurement tools to provide readers with a broader perspective. Fifth, we did not extract the data to assess the effects of the type of randomization (balanced vs. unbalanced) on the ES, which has been shown to be an important factor for placebo response in RCTs. 56 Lastly, this study identified a significant potential for publication bias that may have resulted in missing trials with small sample size studies or a larger placebo effect. This could have impacted the overall effect size estimates
Relevant to clinical practice, our findings indicate that patients with OCD can derive modest benefits from placebo effects, though to a lesser extent than in anxiety and mood disorders for example. Based on an experts’ consensus opinion, to leverage this benefit in routine patient care, recommendations include patient education and the potential use of open-label placebos. 11 The latter may enhance placebo effects by allowing patients to participate more knowledgeably in their care. Furthermore, practitioners may need to consider implementing specific care routines employed in clinical trials including, for example, efforts to enhance the clinician-patient relationship, frequent follow-ups, and measurement-based care.11,57
Further Directions
Despite an ever-growing number of systematic reviews highlighting a significant but heterogenous placebo effect in different health conditions, the nature and the correlates of the placebo effect has still been the subject of insufficient study.45, 46 Systematic reviews, including our study, generally lack the ability to identify sources of placebo effect heterogeneity over time and in different studies due to insufficient detailed data. A greater focus on the placebo effect in future trials, for example, through open-label placebo trials or placebo-oriented designs embedded in conventional RCTs, can be a reasonable strategy for increasing our understanding of the placebo effect across the different diseases. Research priorities going forward include characterizing the sources of heterogeneity in the placebo effect, the interactive dynamic between placebos and interventions, and demographic and clinical correlates of the placebo effect. Furthermore, researchers should consider the placebo effect in the interpretation of the treatment effectiveness. For example, a high placebo effect could hypothetically impact intervention effect, especially in trials where the intervention and placebo share a similar presumed mode of action, 58 for example when the brain areas that contribute to the placebo effect also are the target of intervention. 40 In clinical practice, on the other hand, placebos can be considered a cost-effective and evidence-based therapeutic tool in the management plan, which contributes to the desired care goals. 37
Conclusions
This review demonstrated that (pill/sham) placebos have a modest effect on patients with OCD, mainly in improving core symptoms of OCD, albeit to a lesser extent than placebo effects in other major psychiatric conditions such as depressive and ADs. This effect can be leveraged by clinicians who should be mindful of potential contributors including patient expectations. We also recommend that researchers consider how better to utilize and investigate placebo-related factors in future clinical trials and to carry out network meta-analyses to characterize the impact of placebo effect correlates including placebo type, study factors, and subjects’ characteristics.
Supplemental Material
sj-pdf-1-cpa-10.1177_07067437221115029 - Supplemental material for Systematic Review and Meta-Analysis of the Placebo Effect and its Correlates in Obsessive Compulsive Disorder
Supplemental material, sj-pdf-1-cpa-10.1177_07067437221115029 for Systematic Review and Meta-Analysis of the Placebo Effect and its Correlates in Obsessive Compulsive Disorder by Safoura Mohamadi, Masoud Ahmadzad-Asl and Seyed Aria Nejadghaderi, Roxana Jabbarinejad, Seyed Hamidreza Mirbehbahani, Mark Sinyor, Margaret A. Richter, Farnoush Davoudi in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437221115029 - Supplemental material for Systematic Review and Meta-Analysis of the Placebo Effect and its Correlates in Obsessive Compulsive Disorder
Supplemental material, sj-docx-2-cpa-10.1177_07067437221115029 for Systematic Review and Meta-Analysis of the Placebo Effect and its Correlates in Obsessive Compulsive Disorder by Safoura Mohamadi, Masoud Ahmadzad-Asl and Seyed Aria Nejadghaderi, Roxana Jabbarinejad, Seyed Hamidreza Mirbehbahani, Mark Sinyor, Margaret A. Richter, Farnoush Davoudi in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
Authors would like to thank Sara Savaheli, MD; Sadaf Saneh, MD; Morteza Naserbakht, MD, Farzaneh Farhadi, MD; Sarvenaz Salahi, MD; Pegah Derakhshan, MD; Ali Kabir, MD; Fatemeh Hadi, MD; Ahmadreza Shamshiri, MD, PhD; and Mona Goodarzi, MD for their assistance in the screening process and data extraction.
Registration and Protocol
This study was reviewed and approved by the Research Ethical Review Board of Iran University of Medical Sciences (Reg. No.: 9511286016) and Research Ethical Review Board. It is also registered in the International Prospective Register of Systematic Reviews (PROSPERO) as CRD42019125979.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. M. Sinyor receives salary support from Academic Scholars Awards from the Departments of Psychiatry at Sunnybrook Health Sciences Centre and the University of Toronto.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Contribution
M.A.A., F.D., and S.M. contributed to idea development, proposal preparation, data collection and analysis, manuscript draft preparation, and finalization. S.A.N., S.H.M., and R.J. were involved in finalizing the study protocol, data collection, manuscript draft preparation, and finalization. M.S. and M.A.R. contributed to idea development, data analysis, and manuscript finalization.
Availability of Data,Code,and Other Materials
The data used in this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.