
Abstract
Background
Studies of occupation-associated suicide suggest physicians may be at a higher risk of suicide compared to nonphysicians. We set out to assess the risk of suicide and self-harm among physicians and compare it to nonphysicians.
Methods
We conducted a population-based, retrospective cohort study using registration data from the College of Physicians and Surgeons of Ontario from 1990 to 2016 with a follow-up to 2017, linked to Ontario health administrative databases. Using age- and sex-standardized rates and inverse probability-weighted, cause-specific hazards regression models, we compared rates of suicide, self-harm, and a composite of either event among all newly registered physicians to nonphysician controls.
Results
Among 35,989 physicians and 6,585,197 nonphysicians, unadjusted suicide events (0.07% vs. 0.11%) and rates (9.44 vs. 11.55 per 100,000 person-years) were similar. Weighted analyses found a hazard ratio of 1.05 (95% confidence interval: 0.69 to 1.60). Self-harm requiring health care was lower among physicians (0.22% vs. 0.46%; hazard ratio: 0.65, 95% confidence interval: 0.52 to 0.82), as was the composite of suicide or self-harm (hazard ratio: 0.70, 95% confidence interval: 0.57 to 0.86). The composite of suicide or self-harm was associated with a history of a mood or anxiety disorder (odds ratio: 2.84, 95% confidence interval: 1.17 to 6.87), an outpatient mental health visit in the past year (odds ratio: 3.08, 95% confidence interval: 1.34 to 7.10) and psychiatry visit in the preceding year (odds ratio: 3.87, 95% confidence interval: 1.67 to 8.95).
Interpretation
Physicians in Ontario are at a similar risk of suicide deaths and a lower risk of self-harm requiring health care relative to nonphysicians. Risk factors associated with suicide or self-harm may help inform prevention programs.
Introduction
Suicide is the 13th leading cause of death, with an average of two deaths per minute worldwide. 1 Occupation is an identified risk factor for suicide with physicians being reported to have a higher risk of suicide compared to nonphysicians despite exhibiting better measures of overall physical health.2–15 Numerous survey-based studies identify mental distress, however, there is little contemporary data on death by suicide in physicians in Canada.11, 16–18 High levels of psychosocial stress, burnout, mental health and substance disorders, access to medications, and life-ending knowledge are proposed as putative factors.14, 19–21 This is especially pertinent with recent reported high levels of emotional distress and elevations in mental health services among physicians with the recent coronavirus disease 2019 (COVID-19) pandemic. 22
Many studies reporting a higher risk of suicide among physicians predate 2000, with more recent evidence suggesting that physician suicide occurs at comparable rates to the nonphysician population. 16 The objective of this study was to evaluate the risk of suicide and self-harm among physicians and nonphysicians in Ontario, Canada, using administrative data sources. We hypothesized that the risk of suicide in physicians would be similar to the general population in a more contemporary cohort.
Methods
Design and Setting
This study is part of a broader initiative termed Health Evaluation and Liveliness for Physicians through Meaningful Data (HELP-MD) with the aim to access and analyze large-scale, secondary epidemiological data to study the health and wellness of physicians. We conducted an observational retrospective cohort study of all Ontarian physicians compared with a weighted cohort of nonphysicians from January 1990 to December 2015, followed until 2016. Physicians were identified by registration with the College of Physicians and Surgeons of Ontario (CPSO), a licensing requirement for practicing medicine. Using unique encoded identifiers, we employed deterministic, followed by probabilistic, data linkage based on name, date of birth and sex to link physicians from the database of the CPSO to health databases housed at ICES (Additional methodological details are presented in the Supplemental data and Supplemental Table 1). ICES is a prescribed entity under section 45 of Ontario's Personal Health Information Protection Act. Section 45 authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of the allocation of resources to or planning for all or part of the health system. This project was conducted under section 45 and approved by ICES’ Privacy and Compliance Office. Regional ethics board approval was obtained from the Ottawa Hospital Research Institute; as only deidentified data was analyzed, individual-level consent was waived. The reporting of this study follows guidelines for observational studies (Supplemental Table 2).
Data Sources
Physician demographic, specialty, medical school, and level of training information were obtained from CPSO registration data. Relevant data were obtained from encoded, linked databases housed at ICES (Supplemental Table 3). Additional physician specialty information was obtained from the ICES physician database, which uses billings and workforce information to assign specialties based on the proportion of specialty billing codes used.
Study Population
All newly registered physicians and nonphysicians aged 25 or older from January 1990 to December 2015 were included in the study cohort (Supplemental Table 4). The age cut off was chosen as it is the average age of completion of medical school in Canada. Physicians who were newly registered with the college entered the cohort (i.e., index date) when deemed ready to practice, which we defined as either the initial registry date with the college or initial date of eligibility with the Ontario Health Insurance Plan, whichever came later, to avoid an immortal time bias. 23 We assigned nonphysicians a random index date proportional to the distribution of index dates among physicians. 24 Health care utilization was determined using the Canadian Institute for Health Information Discharge Abstract Database for hospital admissions, National Ambulatory Care Reporting System for emergency room visits and physician billing information (all codes and definitions are presented in). Cause of death and death date were obtained from the Ontario Registrar General Death vital statistics. Income quintiles and location of residence were obtained from postal code conversion files based on Statistics Canada census data. The databases were complete for all variables used except for income quintile and rural location, which were missing in less than 5% of individuals. Physicians or nonphysicians were lost to follow-up on the first date they became ineligible for OHIP (i.e., due to emigration or missed OHIP renewal, 0.2% total cohort).
Covariates
We obtained physician information including age, sex, location of residence, specialty (family medicine, psychiatry, anesthesia, internal medicine, surgery, radiology, missing or other), medical school location (Canada vs. international), and health care use. Health care use medical visits for mental health, psychiatric care, and all-cause admissions to hospital in the year before the index date, and mental health comorbidities (defined as 2 outpatient physician visits or 1 admission to hospital within the prior 2 years using a relevant mental health diagnostic code based on International Classification of Diseases, 9th Revision [ICD-9] and International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10] codes). Income quintiles and place of residence were from Statistics Canada and determined using geospatial data based on an individual's postal code. Individuals were assigned with neighborhood-level income quintiles based on the census metropolitan area for the closest census year to the index.
Outcomes
Our primary study outcomes were death by suicide and an episode of self-harm presenting to the emergency room or requiring hospitalization as defined by ICD codes (Supplemental Table 5). 25 Our secondary outcome was the composite of suicide or self-harm events. An episode of self-harm is among the strongest predictors of future suicide in the general population. 25 The ICD-9 and ICD-10 codes for suicide we employed in this study showed strong concordance (sensitivities of greater than 96%) with coroner reported suicide when validated in Ontario. 26 In Canada, self-harm was only captured from ICD-10 onwards (implemented in Ontario from April 1, 2002, onwards). We defined an episode of self-harm by an ICD code for a self-harm event and a mental health disease. 26
Statistical Analysis
Characteristics of physicians/nonphysicians were compared pre- and post-inverse probability treatment weighting. 27 The weights were calculated using all covariates listed previously. We used standardized differences to assess covariate balance pre- and post-weighting between physicians and nonphysicians. 28 This measurement assesses differences between group means relative to the pooled standard deviation, with a significant difference considered to be 0.10 or greater. We calculated crude and age/sex direct standardized rates (standardized to the Ontario Census population 2016) for the total cohort (n = 6,621,186) for suicide, self-harm, and their composite for physicians and nonphysicians per 100,000 person-years. We examined the association of being a physician and suicide, self-harm, and the composite outcome using weighted, cause-specific Cox proportional hazards models. 27 Physicians and nonphysicians were censored at death, loss to follow-up or end of the study period. Physicians with missing income or location (n = 1,535) were excluded. Interaction terms for age, sex, and a history of a mental health disorder with the composite outcome of suicide or self-harm were evaluated. Lastly, we explored risk factors associated with suicide and the composite of suicide or self-harm using univariate logistic regression. Odds ratios (ORs) with 95% confidence intervals (CIs) were determined for variables of interest (age, sex, rural residence, medical school, health care use, and physician specialty). We evaluated risk factors for suicide at index date (registration to practice) and upon death. As self-harm was captured from April 2002 onwards, we performed a sensitivity analysis, limiting our cohort from April 2002 to the last date of follow-up. We conducted all analyses with SAS software, SAS Enterprise guide version 7.1 (SAS Institute Inc., Cary, NC, USA). We deemed p values <0.05 or CIs that did not overlap with 1 statistically significant. All analyses were conducted at ICES.
Results
We included 35,989 physicians and 6,585,197 nonphysicians in our study cohort. Compared with nonphysicians, a higher proportion of physicians were male (57.2% vs. 47.9%) and physicians were younger (mean age 32 vs. 55 years). Physicians were less likely to live in a rural setting and more likely to live in higher income neighborhoods. Physicians also had fewer medical comorbidities and fewer health care visits (Table 1). After statistical weighting, a total of 34,454 physicians were included (1,535 were excluded due to missing data) and the two groups were balanced on baseline characteristics. The median (25th, 75th percentiles) follow-up time was 10 (5–16) and 8 (4–14) years for physicians and nonphysicians, respectively.
Baseline Characteristics of Physicians and Nonphysicians Before and After Inverse Probability Treatment Weighting.
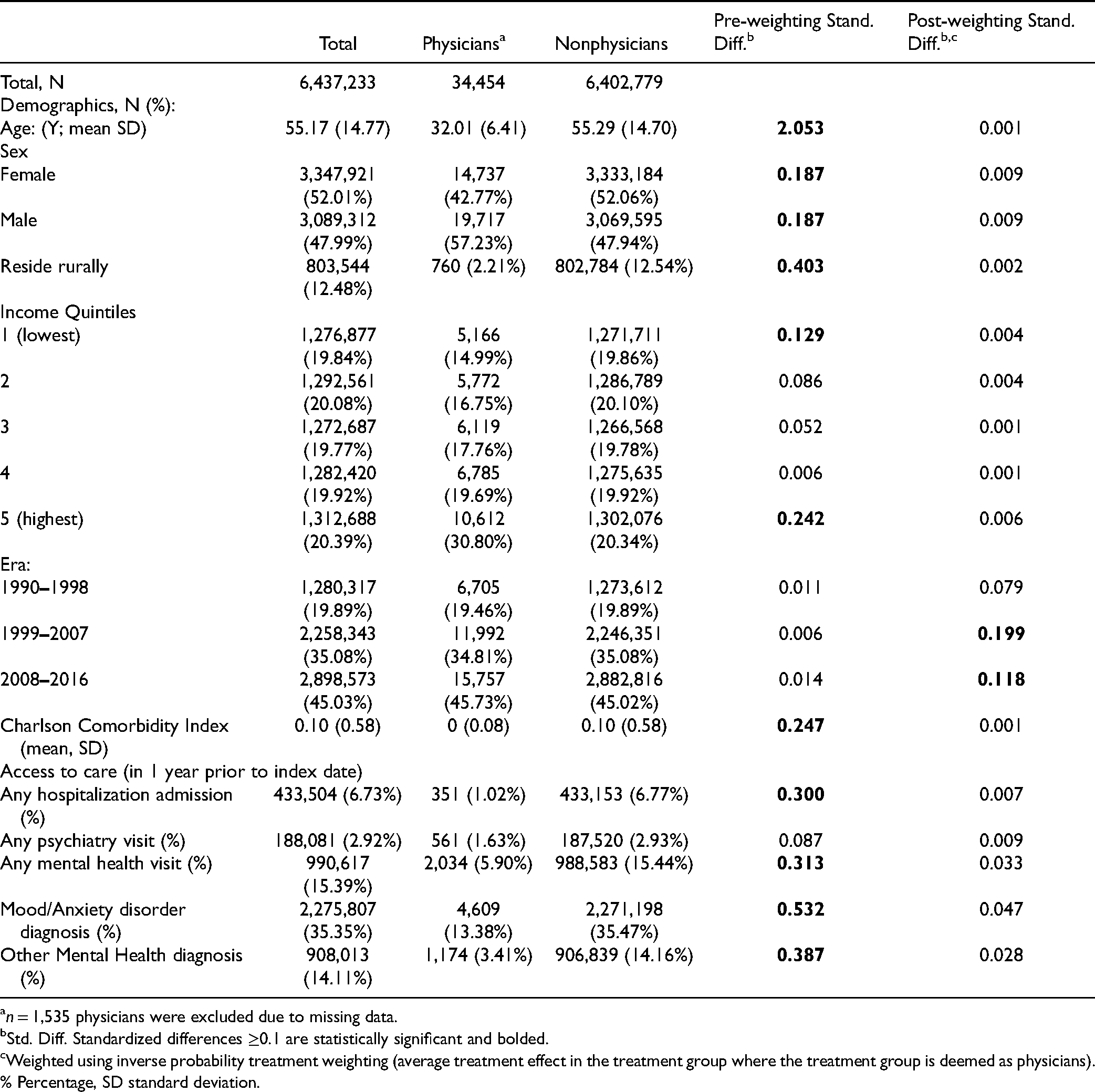
n = 1,535 physicians were excluded due to missing data.
Std. Diff. Standardized differences ≥0.1 are statistically significant and bolded.
Weighted using inverse probability treatment weighting (average treatment effect in the treatment group where the treatment group is deemed as physicians).
% Percentage, SD standard deviation.
About 1 in 1,300 (0.08%, 27 events) physicians died by suicide between 1990 to 2016. Between April 2002 to 2016, 1 in 400 died by suicide or had a self-harm event (62 events). We did not find a statistically significant difference in the crude (9.44 vs. 11.55 per 100,000 person-years, p = 0.3) and age- and sex- standardized (6.66 vs. 11.37 per 100,000 person-years, p = 0.3) rates for suicide in physicians compared to nonphysicians (Table 2). We found that age- and sex-adjusted rates of self-harm (53.85 vs. 52.15 per 100,000 person-years), and the composite of suicide or self-harm (61.26 vs. 60.73 per 100,000 person-years) were statistically similar between physicians and nonphysicians.
Crude and Age-sex Standardized Rates of Suicide, Self-Harm and the Composite of Suicide and Self-Harm in Ontario Physicians Compared to the Nonphysician Population From 1990 to 2016.
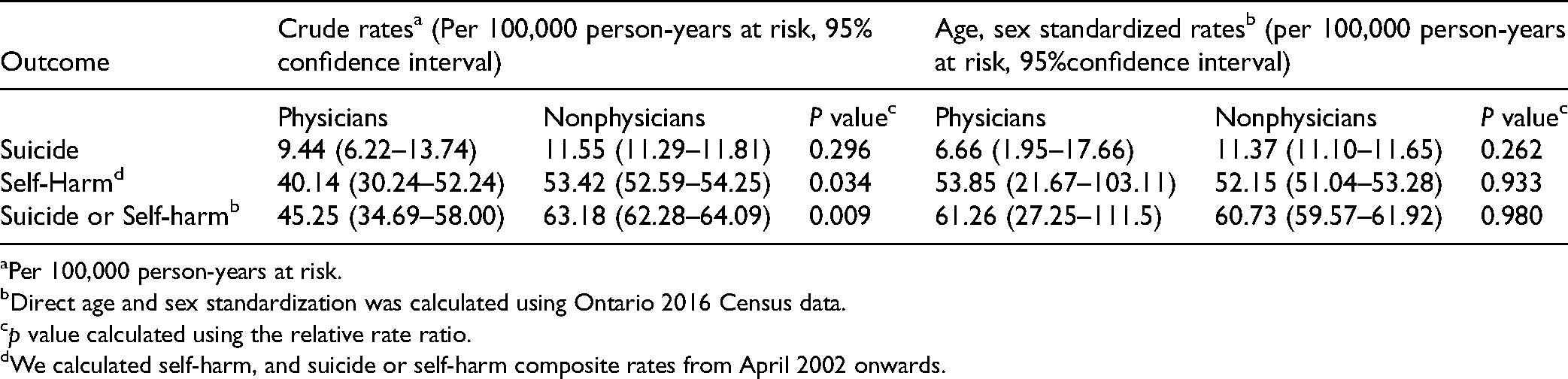
Per 100,000 person-years at risk.
Direct age and sex standardization was calculated using Ontario 2016 Census data.
p value calculated using the relative rate ratio.
We calculated self-harm, and suicide or self-harm composite rates from April 2002 onwards.
Physicians were associated with a similar weighted rate of suicide as nonphysicians [0.07% vs. 0.11%, respectively; hazard ratio [HR]: 1.05, 95% CI: 0.69 to 1.60) (Table 3). Self-harm events (0.22% vs. 0.46%; HR: 0.65; 95% CI: 0.52 to 0.82) and the composite of suicide or self-harm (0.28% vs. 0.55%; HR: 0.70; 95% CI: 0.57 to 0.86) were lower in physicians compared to nonphysicians. This was consistent in a sensitivity analysis limiting follow-up from 2002 onwards (Supplemental Table 6). No effect modification was detected by age (p = 0.6) or sex (p = 0.1) with the composite outcome of suicide or self-harm, however, effect modification was detected by the history of a mental health disorder (p < 0.01).
Incidence of Suicide, Self-Harm and Suicide or Self-Harm for Physicians Compared to Nonphysicians.
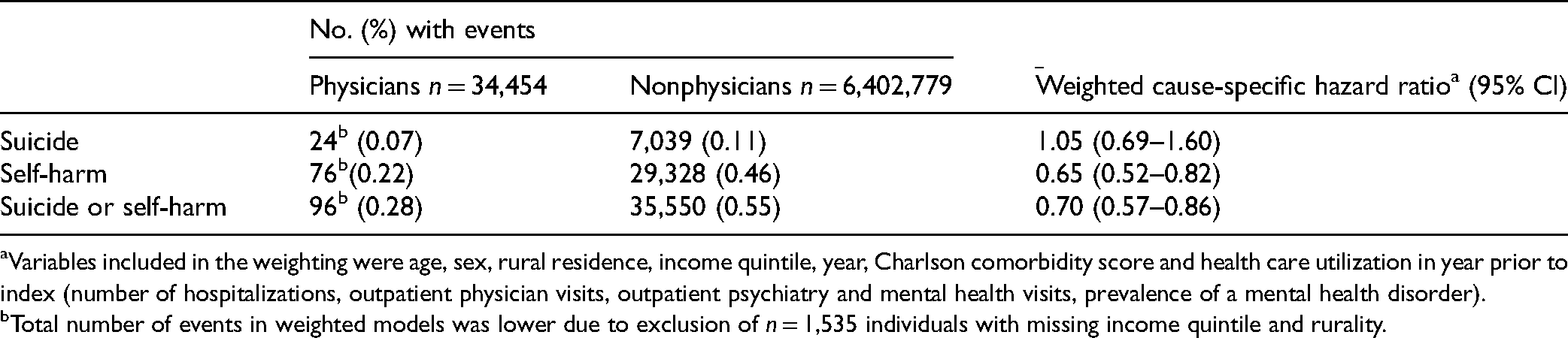
Variables included in the weighting were age, sex, rural residence, income quintile, year, Charlson comorbidity score and health care utilization in year prior to index (number of hospitalizations, outpatient physician visits, outpatient psychiatry and mental health visits, prevalence of a mental health disorder).
Total number of events in weighted models was lower due to exclusion of n = 1,535 individuals with missing income quintile and rurality.
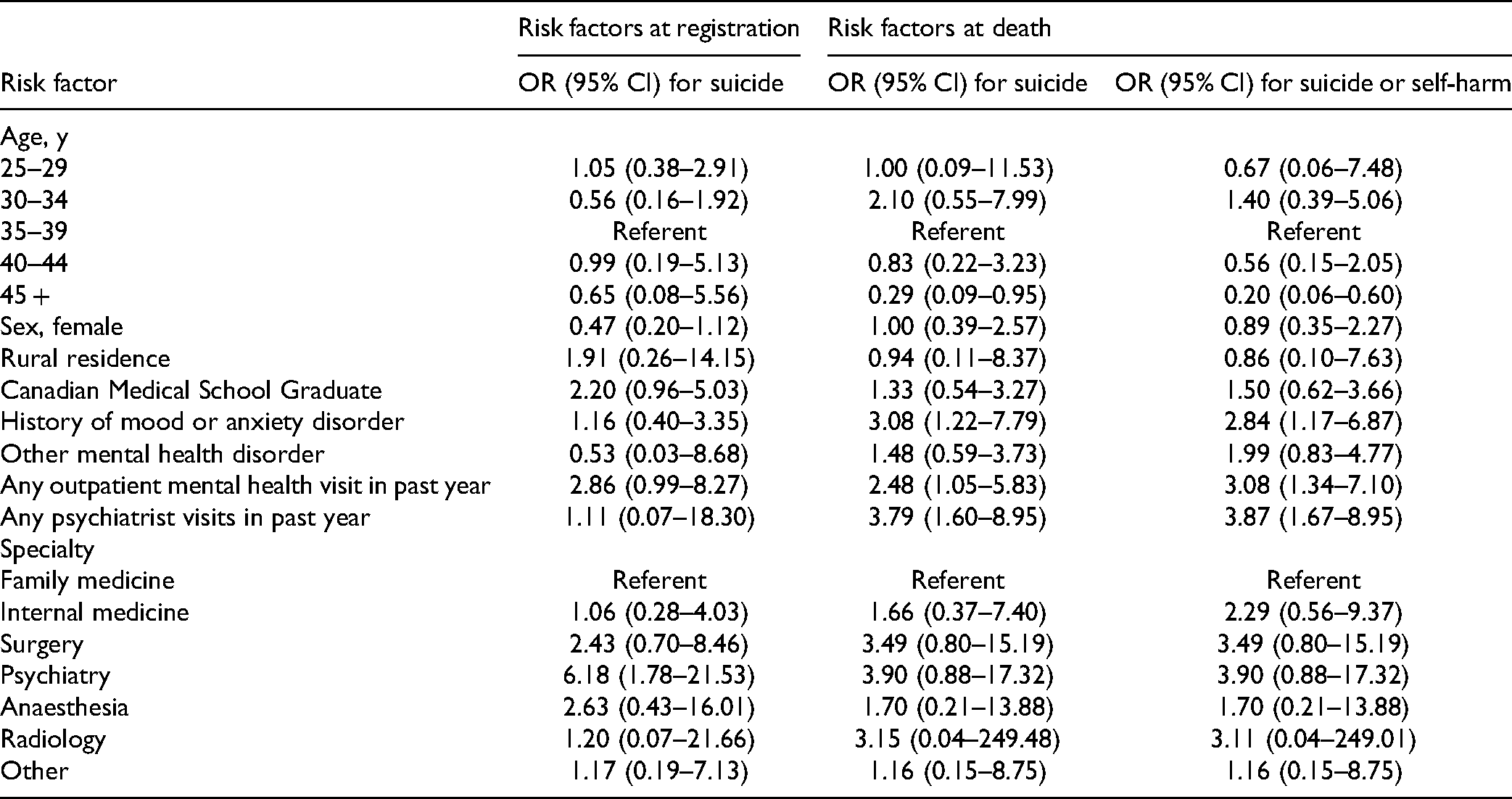
Among physicians who died in the follow-up, psychiatry as a medical speciality was associated with a higher risk of suicide (Table 4). When examining risk factors at the time of death, suicide and suicide or self-harm were associated with age > 45 years, history of a mood or anxiety disorder, an outpatient mental health visit in the past year and any psychiatry visit in the past year.
Univariate Association Risk Factors for Suicide at Registration With the College of Physicians and Surgeons and Risk Factors for Suicide and the Composite of Suicide or Self-Harm at Death.
Discussion
We observed 27 physician deaths by suicide over a 26-year period (roughly 1 in 1,300), a rate similar when compared to nonphysicians. Furthermore, self-harm and the composite of suicide or self-harm were lower in physicians relative to nonphysicians. Physicians with a history of a mood or anxiety disorder and a psychiatry visit in the preceding year were associated with the composite of suicide or self-harm.
Little information exists on suicide among Canadian physicians. A case-control study from Quebec identified 36 physician suicides (29 male, 7 female, median age 50 years old) between 1992 and 2009. 11 In a study of occupational suicide in Canada, physicians were not identified as an occupation with high suicide risk. 27 We observed a crude rate of physician suicide of 9.44, and an age- and sex-standardized rate of 6.66 that was statistically similar to that of the nonphysician population. Country-level physician rates of suicide relative to the general population were reported from the United States, Europe, and Australia, with consistently higher rates among physicians.3–10, 12, 13 Physician cohorts from pre-2000 reported significantly higher crude rates of 31.2 in the United Kingdom, and 26.1 for women and 43 for men in Norway, with a declining trend over time.3, 28 The United Kingdom reported a 63% reduction in physician suicide from the early 1980s to 2001–2005. 29 A 2016 retrospective mortality study in Australia reported age- and sex-standardized suicide rate of 12.2 per 100,000 person-years. 6 The lower rate of physician suicide in Ontario may be specific to the Canadian physician population, as our nonphysician population had a comparable suicide rate to previous studies from Canada.1, 30 Furthermore, the low age- and sex-standardized rate we report may reflect our study cohort construction because we accrued mostly newly graduating registered physicians from 1990 onwards, with fewer older physicians.
Self-harm is an important risk factor for future suicide in the nonphysician population; however, its importance as a causal factor in physicians is unclear. Studies on clinically identified self-harm events in physicians are limited to highly specific cohorts (e.g., admitted psychiatric in-patients, decedents only) precluding a determination of true risk.14, 21 A high number of Canadian physicians report self-harm or similar behaviors in self-reported survey studies. Just under 3% of family medicine residents from British Columbia reported suicide attempts, a more specific term encompassing self-harm with intent for suicide, during residency. 18 Suicidal ideations within the last 12 months were reported among 8% of 2,735 physicians surveyed by the Canadian Medical Association. 29 In the current study, self-harm occurred in roughly 1 in 450 physicians, compared with about 1 in 200 nonphysicians. Possible explanations for lower physician rates include underreporting by the treating physician, self-treatment of salient risk factors (such as mental health disorders), or not seeking out health care by physicians for suicidal thoughts. Stigma-related to illness, particularly mental health disorders, persists among physicians and is especially prevalent in medical students and residents. 21 Because of their in-depth medical knowledge and access to medications, physicians may be more likely to die with an episode of self-harm. Especially lethal methods such as firearms (US only) and poisoning/drug overdoses are more common among physicians. 9 Self-harm and related behavior's such as suicide attempts among physicians require further study and should be regarded as a particularly high-risk warning sign for potential suicide, invoking appropriate intervention.
We examined several risk factors associated with suicide, self-harm, and their composite. First, no clear differences were observed based on gender despite a large body of literature identifying women and younger age groups being at a higher risk.4–10, 14, 15, 21, 28, 31 In a recent meta-analysis of 46 studies reporting death by suicide among physicians, the standardized mortality ratio was 1.44 (95% CI: 1.16 to 1.72) with a high degree of heterogeneity in the findings based on sex. 19 The male and physician pooled ratios were 1.24 and 1.94 relative to the general population, respectively. 19 Second, a history of a mental health disorder, mental health visits and psychiatric care were associated with both suicide and the composite of suicide and self-harm, underpinning their importance as risk factors. The link between mental health disorders, suicide, and related behaviors is well established in the nonphysician population. 32 In a case-control study from Quebec, physicians and nonphysicians with psychiatric illness had similarly elevated suicide risks. 11 This suggests that physicians with any mental health disorder or requirement for psychiatric care should be viewed as being at higher risk for suicide and to a similar degree as a nonphysician under comparable circumstances. Third, we found nonlinear associations between physician age and risk of suicide and self-harm but that older age (45+) appeared to be protective. These findings are consistent with conflicting prior evidence on the role of age and physician suicide.3, 14, 15, 29 Last, we did observe a higher risk of suicide among psychiatrists at registration. A recent meta-analysis of physician suicide identified psychiatrists at elevated suicide, along with anesthesia, family physicians and general surgeons, relative to other medical specialties. 16 A survey study of 174 psychiatrists provides insight into the traumatic feelings of responsibility and a loss of clinical confidence in response to the death of one of their patients by suicide, potentially acting as a driver of suicide in psychiatrists themselves.33, 34
Our findings unify and contemporize many previous observations with substantial clinical implications. First, our results directly challenge the narrative that suicide risks are currently higher among physicians. Second, by examining self-harms and the composite of suicide or self-harms, interventions and awareness programs can be developed with the goal to prevent the loss of life. Third, as our study cohort included residents and fellows, the early introduction to wellness programs, screening, and individualized treatment programs, incorporated directly into medical school or training programs, may be beneficial. Fourth, an increase in health care use by a physician with a mental health disorder should prompt concern among caregivers. As physicians at risk may underuse health care resources, as suggested by the low self-harm rates, education, and a culture shift away from viewing illness as a weakness, and training physicians specifically on how to identify a colleague in distress (crisis training) may also be beneficial. Lastly, our findings using objective, administrative data complement emerging data in Canada around physician health outcomes.
Our study has a few limitations. Our study cohort comprised newly registered physicians from 1990 onwards, thereby limiting the number of individuals over 60 years of age and potentially leading to an underestimate of the true total risk of death from suicide and self-harm. Whether the risk of physician suicide increases over the age of 60 is controversial, with disparate findings from the literature.3, 9, 10, 12 Death by suicide is a well-validated outcome; however, our self-harm outcome only captures more sever presentations and did not capture ambulatory visits. As such it may be subject to misclassification and underreporting and likely greatly underestimates the prevalence of self-harm episodes in physicians.26, 35 Despite our large dataset, there remained a limited number of events that prevented multivariate adjustment when evaluating risk factors and reduced our power to detect subgroups. Roughly 1 in 4 physicians lacked specialty information. We did not have access to data on the method of suicide which could be relevant when considering interventions to reduce suicide in physicians. We did not include medical students, a group in which suicide may be increasing. We used only one-time point, 2016 census data, for standardization of age and sex, which may not reflect changes over time. Because our study cohort included newly registering physicians only, we were unable to examine temporal trends. Further research using a cohort of all physicians in Ontario could investigate whether rates of suicide and self-harm have been changing over time
Suicide and self-harm in physicians, albeit uncommon events, are important, potentially preventable, and pertinent physician health issues. In a large cohort from 1990 to 2016, we found a similar rate of suicide in physicians relative to nonphysicians and a lower risk of self-harm. Key risk factors such as a mental health disorder should prompt a high index of concern.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437221099774 - Supplemental material for Suicide and Self-Harm Among Physicians in Ontario, Canada
Supplemental material, sj-docx-1-cpa-10.1177_07067437221099774 for Suicide and Self-Harm Among Physicians in Ontario, Canada by Manish M. Sood, Emily Rhodes, Robert Talarico, Caroline Gérin-Lajoie, Christopher Simon, Edward Spilg, Taylor McFadden, Kwadwo Kyeeremanteng, Daniel T. Myran, Nicholas Grubic and Peter Tanuseputro in The Canadian Journal of Psychiatry
Footnotes
Data Sharing
Data from this study is not publicly available as per ICES policy.
Acknowledgments
The opinions, results, and conclusions are those of the authors and are independent of the funding sources. Parts of this material are based on data and/or information compiled and provided by CIHI. However, the analyses, conclusions, opinions, and statements expressed in the material are those of the author(s), and not necessarily those of CIHI. Parts of this report are based on Ontario Registrar General (ORG) information on deaths, the original source of which is ServiceOntario. The views expressed therein are those of the author and do not necessarily reflect those of ORG or the Ministry of Government Services. No endorsements by ICES, the University of Ottawa, the Ottawa Hospital Research Institute, the Canadian Institutes of Health Research, or the MOHLTC are intended or should be inferred.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Manish Sood received speaker fees from AstraZeneca and is supported by the Jindal Research Chair for the Prevention of Kidney Disease. Peter Tanuseputro is supported by a Physicians’ Services Incorporated Graham Farquharson Knowledge Translation fellowship. CGL, CS, TM: The opinions and conclusions expressed are the writers’ own and are not those of the Canadian Medical Association.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ottawa Hospital Academic Medical Organization, Canadian Medical Association, Ottawa Hospital Innovation Project, Bruyère Centre for Individualized Health, ICES that is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC)
Ethical Approval
Regional ethics board approval for this study was obtained from the Ottawa Hospital Research Institute.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.