Abstract
In prison populations the social factors associated with suicide have been reported to be more prevalent than in the general population [1], with some authors believing that prison in and of itself may be an important risk factor [2].
International perspective
Many international studies report higher rates of suicide in prisoner populations when compared to general community populations [1, 3–5]. A recent study of deaths in custody in England and Wales reported the rate of suicide in prison over a 2 year period to be 133 per 100 000 inmates. That study also found that one-third of all suicides occurred within 7 days of incarceration, with high rates of mental disorder in the total suicide population [6]. Addressing the issue of high rates of mental illness in British prison populations has been directly linked by some authors to suicide prevention [1, 3].
A case–control study in Austrian prisons reports suicidal behaviour among prisoners to be an important risk indicator and one that prison staff need to take seriously. Other important factors in the Austrian prison population were identified as psychiatric diagnosis, violent index offence and placement in single-cell accommodation [7].
Looking more broadly at mortality in Canadian prisons, Wobeser et al. found that those in custody were more likely to die prematurely than the general population [3]. The authors report that for the study period, cause of death tended to be violent, particularly suicide by strangulation and poisoning.
New South Wales context
In the 10 years from 1995 to 2005, the inmate population at census in New South Wales (NSW) prisons has grown from 7749 to 9803, representing a disproportionate increase when compared with the increase in the general population in NSW [4].
In the late 1980s the Royal Commission into Aboriginal Deaths in Custody (RCIADIC) highlighted the extensive problem of suicide in Australian prisons [5]. Since then, suicide in custody has been firmly on political and research agendas. According to the Australian Bureau of Statistics, one-third of all Australian inmates are held in NSW prisons [8].
Methods
This project was conducted as part of a clinical practice improvement project, attempting to gain a better understanding of suicide in NSW prisons, through identifying significant risk factors and subsequently proposing more effective methods of managing those prisoners identified to be at higher risk.
Definitional issues
There are differing opinions within the literature in relation to the connection between self-harming behaviour and suicide. Some authors have put forward the theory that self-harm and suicide are part of the same continuum, beginning with suicidal thinking and sometimes ending with death. Others have postulated that some self-harming behaviour should be viewed as an independent phenomenon. McArthur et al. argue that there is little to be gained in attempting to differentiate, as such a distinction may be ‘illusionary’ and ‘counterproductive’ [9].
In Australia, a death is classified as suicide following a coronial inquest, where it is established that a person committed an act with the intention of taking his or her own life. However, it is difficult to definitively establish intent [10]. Fleming et al. favoured a definition of suicide, as a self-inflicted death regardless of intent [11]. For the purposes of this project, those cases identified as self-inflicted, with a coronial finding of death by suicide or those awaiting a coronial hearing but reported as possible death by suicide, were included.
Identification of cases
Justice Health is the health service responsible for the provision of health care within NSW prisons. When a death in custody occurs Justice Health provides a report to the Commissioner for Corrective Services detailing the health history of that particular inmate and maintains a Death in Custody database for all deaths in NSW prisons. All self-inflicted deaths (with a coronial finding of death by suicide) and those deaths that were reported as possible suicide but awaiting a coronial hearing from 1 January 1995 to 31 December 2005 were identified using the Death in Custody database.
Data collection
The Justice Health medical file was reviewed for all cases (there were two cases for which the medical file was not available), and the Justice Health letter to the Commissioner for Corrective Services detailing each inmate's contact with health services in custody was also reviewed.
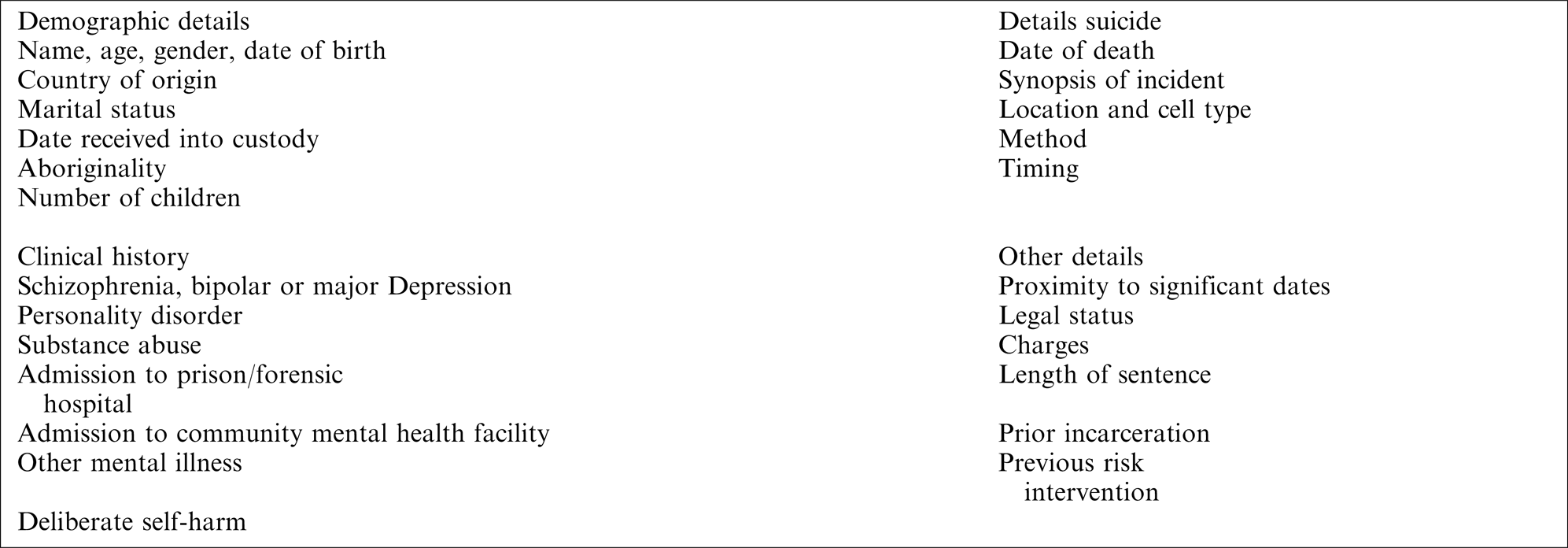
A data set was collected on each case and entered into a database. The data set consisted of information outlined in Appendix I.
Data analysis
Results are presented as proportions with 95% confidence intervals (95%CIs) presented for each of the main variables.
Results
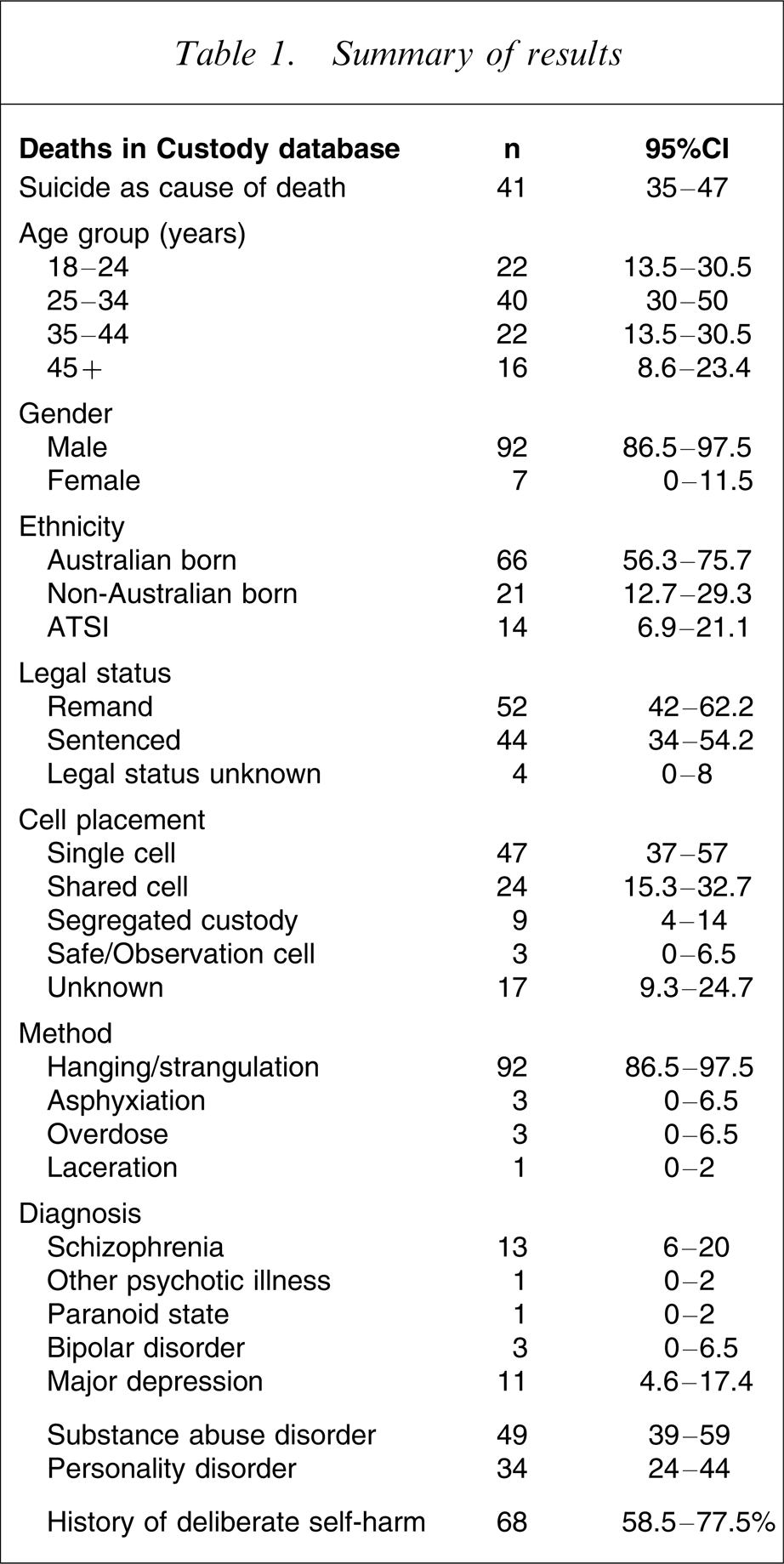
Table 1 provides a summary of the main findings. There were a total of 224 deaths in custody from 1 January 1995 to 31 December 2005. A total of 92 cases were identified as deaths by suicide (41%, 95%CI = 35–47%). Two cases were reviewed but excluded because the coronial inquest was incomplete and on review of documentation available the cause of death was not clear. A decision was made to track those two cases for possible inclusion at a later date should more information become available. One case was excluded because the suicidal act occurred prior to incarceration.
Summary of results
Rates of suicide
The rate of suicide is represented here as the rate per 100 000 inmates and calculated based on the number of inmates in custody at the time of prison census each year and are shown in Figure 1. The rate of suicide in the total Australian prison population is calculated likewise based on the number of self-inflicted deaths in Australian prisons and the population of inmates in Australian prisons.
Rate of suicide.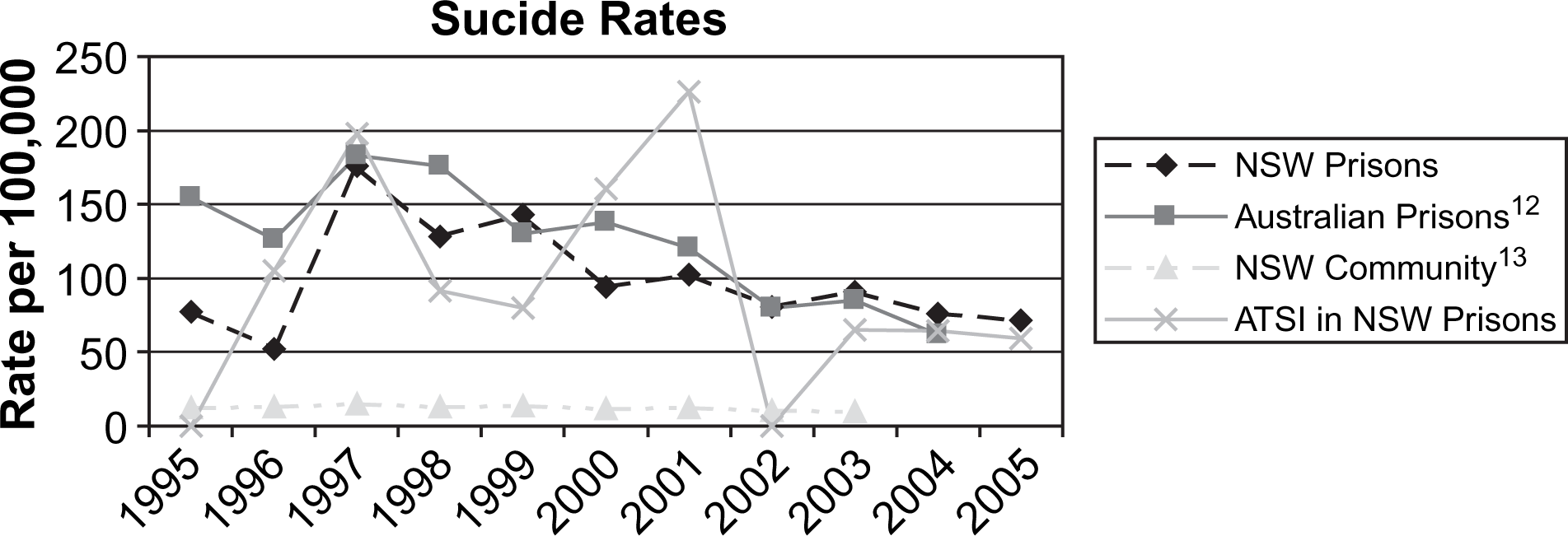
Method of suicide
The most common method of suicide was asphyxiation by hanging or strangulation (92%, 85 cases, 95%CI = 86.5–97.5%). There were a further three cases (3%, 95%CI = 0–6.5%) of asphyxiation involving the use of a plastic bag. There were three cases (3%, 95%CI = 0–6.5%) involving overdose, and one death (1%, 95%CI = 0–2%) resulting from the laceration of a major blood vessel.
Cell placement
Of the total group 43 cases (47%, 95%CI = 37–57%) subjects were in single cells; 22 (24%, 95%CI = 15.3–32.7%) were in shared cells; eight cases (9%, 95%CI = 4–14%) were in segregated custody (single-cell placement in a dedicated segregation unit, with closer levels of monitoring); three cases (3%, 95%CI = 0–6.5%) were in ‘safe cells’ or ‘observation cells’ (cells designed for continuous indirect monitoring and to limit opportunities for self-harm, of inmates identified as at risk). In a further 16 cases (17%, 95%CI = 9.3–24.7%) the nature of the individual's accommodation was not identifiable.
Demographics
Age
Twenty individuals (22%, 95%CI = 13.5–30.5%) were in the 18–24 age group, the majority were in the 25–34 age bracket (37 cases, 40%, 95%CI = 30–50%). Twenty individuals (22%, 95%CI = 13.5–30.5%) were in the 35–44 age group and 15 individuals (16%, 95%CI = 8.6–23.4%) were in the over-45 age group.
Gender
Male subjects represented 92% (95%CI = 86.5–97.5%) of the group while 7% were female; there was one transgender inmate in the group.
Ethnicity
The majority of individuals were born in Australia (66%, 95%CI = 56.3–75.7%), with Aboriginal and Torres Strait Islanders representing 14% (13 cases, 95%CI = 6.9–21.1%) of the total group. A further 21% (95%CI = 12.7–29.3%) of the group were born outside Australia, with a broad representation of nationalities, the largest subgroup being those identified as born in the Pacific Islands (4 cases, 4%, 95%CI = 0–8%). In 12 cases (12%, 95%CI = 5.4–18.6%), the country of origin or place of birth was not identified.
Legal status and sentence
Forty-eight individuals (52%, 95%CI = 42–62.2%) were on remand at the time of suicide. Of the 40 inmates who were sentenced (44%, 95%CI = 34–54.2%), 28% (11 cases, 95%CI = 14–42%) were sentenced to a term of incarceration of ≤6 months. When combined, those serving a sentence of ≤6 months (n = 11) and those on remand (n = 48) represent 64% of the total group.
Diagnosis
On review of the medical file, in 12 cases the subjects had documented symptoms consistent with a diagnosis of schizophrenia (13%, 95%CI = 6–20%); one individual with an unspecified psychotic illness (1%, 95%CI = 0–2%); one reported to present in a paranoid state (1%, 95%CI = 0–2%); 3% of the group had documented symptoms consistent with a diagnosis of bipolar disorder (3 cases, 95%CI = 0–6.5%) and a diagnosis of major depression was evident in 10 cases (11%, 95%CI = 4.6–17.4%).
Forty-five individuals had a documented substance abuse (SA) disorder (49%, 95%CI = 39–59%) while 34% of the group (95%CI = 24–44%) had a personality disorder (n = 31). The most commonly abused substances were cannabis (49%, 95%CI = 39–59%); opioid (48%, 95%CI = 38–58%); alcohol (47%, 95%CI = 37–57%)) and amphetamines (35%, 95%CI = 25–35%).
In 15 cases (16%, 95%CI = 8.5–23.5%) the subject had a major mental illness (MMI), that is, psychotic illness, bipolar disorder or major depression with comorbid SA disorder; 10 subjects (11%, 95%CI = 5–17%) had an MMI with comorbid personality disorder (PD), while the same number, 10 subjects (11%, 95%CI = 5–17%) had a diagnosis of MMI with SA disorder and PD.
History of deliberate self-harm
Sixty-three subjects, representing 68% (95%CI = 58.5–77.5%) of the total population had a documented history of deliberate self-harm (DSH). The remaining 29 (32%, 95%CI = 22.5–41.5%) did not have a reported history documented in the Justice Health medical file.
Timing
Figure 2 illustrates the time from reception to suicide in days. The date of reception into custody was not available in one case and therefore it was not possible to determine the length of time from incarceration to suicide in that case. Of the remaining 91 cases, nine subjects (10%, 95%CI = 4–16%) committed suicide within 24 h of incarceration; 20 (22%, 95%CI = 13.5–30.5%) occurred between 24 h and 1 week; nine (10%, 95%CI = 4–16%) between 1 week and 1 month of incarceration; 29 (32%, 95%CI = 22.5–41.5%) between 1 month and 6 months of incarceration, and the remaining 24 cases (26%, 95%CI = 17–35%) took place >6 months after incarceration.
Time from reception to suicide.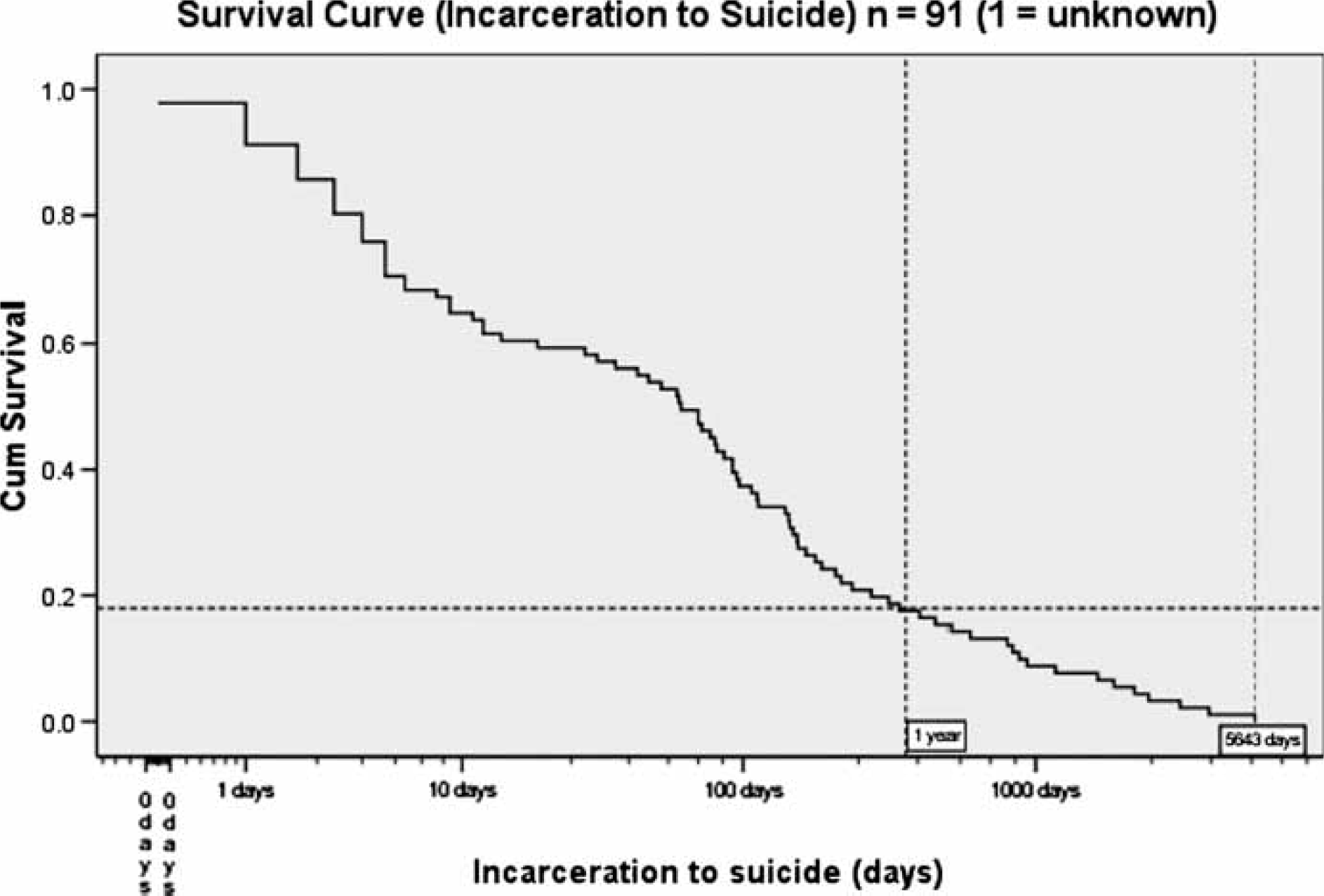
In the 10 year period from 1995 to 2005, 32% (95%CI = 22.5–41.5%) of suicides in NSW prisons occurred within one week of reception into custody with a total of 74% (95%CI = 65–83%) of suicides taking place within 6 months of incarceration.
Discussion
The retrospective nature of this review leads to a number of limitations. These include variable quality and quantity of information available and a limited capacity to corroborate data. The descriptive nature of the project and the lack of a control group limit the capacity to definitively examine the factors associated with suicide in this population.
The strength of this review lies in the complete nature of the sample and the fact that detailed reports to the Commissioner of Corrective Services were prepared by Justice Health (formerly Corrections Health Service) following each of these suicides in custody. These reports were prepared in a standardized format and were available in all but seven cases. However, the medical files were available in those cases in which the report to the Commissioner could not be located. In two cases the medical files were not available for review, but in those cases the reports to the Commissioner were accessible. Additionally, the authors are confident that all suicides in prison custody in NSW from 1 January 1995 to 31 December 2005 were included in this review.
Camilleri et al., in their review of the literature in relation to suicide in prisons, discuss the inherent difficulty when calculating rates of suicide in this population, noting that calculations vary greatly depending on whether the rate is based on an average prison population or annual reception rates [14]. The rate of suicide is represented here as the rate per 100 000 inmates and calculated based on the number of inmates in custody at the time of prison census each year. Rates of suicide in the NSW community and the total Australian prison population are presented here merely to provide a context in which to view the NSW prison rates. Rates of suicide in NSW prisons have been declining over the past 10 years, while over the same period the number of people in custody has grown [5, 15]. However, this reduction should not lead to complacency because rates in NSW prisons remain approximately 10-fold that of the general population. Caution should be exercised when comparing rates of suicide in prison and community populations [16]; nonetheless such a large discrepancy cannot be ignored.
The first week of incarceration represents a significant risk period. Those on remand or serving a sentence of ≤6 months are significantly overrepresented in the suicide group.
The presence of an MMI, PD, SA disorder and history of DSH have been shown to be linked to suicide in custody [1, 3–5, 8, 11]. This review highlights these factors as associated with suicide in NSW prisons. Butler and Allnutt estimated the prevalence of MMI in NSW prisons to be 8.8% for psychotic illness, 14.6% for major depression, 2.8% for bipolar disorder, 53% for SA and 40.6% for PD [17]. In the present population the prevalence of major depression, bipolar disorder, SA and PD is in keeping with the Butler and Allnutt findings, but psychotic illness appears to be overrepresented. The authors acknowledge the inherent difficulties of attempting to retrospectively determine the presence of an MMI, SA disorder or PD, but a diagnosis was not recorded for an individual unless substantial documentary evidence existed to support such a diagnosis. In this regard, MMI could even be underreported here.
As discussed earlier there are inherent difficulties in defining and categorizing self-harming behaviour. For the purpose of this review no attempt has been made to determine intent or lethality of self-harming behaviour, rather all self-harming behaviour has been grouped together under the heading of DSH. It is difficult to determine with any certainty the extent to which inmates self-harm. In the population described here DSH was a prominent feature, with 68% of the total group having a documented history. This figure may in fact represent an underestimation of the prevalence of DSH in the group because it relies on documented evidence in the Justice Health medical file or self-report at the time of reception into custody.
The methods by which those in custody in NSW commit suicide are more violent then those in the community [13], with hanging as the means of suicide in 92% of cases in custody. This may in part be explained by the lack of access to less violent means.
Other studies have highlighted single-cell accommodation as a factor to be taken into consideration when reviewing suicide in custody [10]. In NSW prisons the majority of suicides occurred in single-cell placement, but of concern are the number of suicides that have occurred in shared accommodation or in cell placements with high levels of indirect observation.
Based on population estimates (1.8% of NSW population [13]), Aboriginal and Torres Strait Islanders (ASTI) are overrepresented in NSW prisons, accounting for 11.5% of the total inmate population in NSW in 1995, 17.1% of the population in 2005 and averaging at 15% of the NSW prison population for the 10 years from 1995 [6]. For the period of the present review ASTI represent 14% of the suicide deaths in custody.
In the wider Australian community 28% of the adult population are born outside of Australia. This group represents 21% of the NSW prison population and account for one-fifth of suicides in custody.
Conclusion
Suicide was the leading cause of death among NSW inmates between 1995 and 2005, accounting for 41% of all deaths in custody. The rate of suicide in NSW prisons has been declining over the past 10 years but remains approximately 10-fold that of the NSW community. Mental illness, substance abuse and personality disorder appear to be important factors contributing to higher rates of suicide in custody. Although it is difficult to determine the extent of previous episodes of DSH in custody, the majority of those who committed suicide in custody had a documented history of DSH, making it an important marker in the assessment and management of suicide risk.
Shared accommodation and cells with higher levels of indirect observation should not be seen to protect completely against the risk of suicide. The first week following reception represents a significant risk period and increased monitoring during this period may be an effective intervention.
Those on remand or serving a sentence of <6 months accounted for 64% of all suicides in custody in NSW from 1995 to 2005, with 74% of all suicides occurring within 6 months of incarceration. Consideration should be given to the length of time spent on remand and the value of custodial sentences of ≤6 months.
Suicide is a rare event, making its prediction a difficult task, with the prison environment a further compounding factor. This review highlights a number of factors, which appear to be common in many cases. Further study and examination of those factors will enhance our understanding of suicide in custody; its precipitants and assist in the identification of people at higher risk.
Footnotes
Appendix I
| Demographic details | Details suicide |
| Name, age, gender, date of birth | Date of death |
| Country of origin | Synopsis of incident |
| Marital status | Location and cell type |
| Date received into custody | Method |
| Aboriginality | Timing |
| Number of children | |
| Clinical history | Other details |
| Schizophrenia, bipolar or major Depression | Proximity to significant dates |
| Personality disorder | Legal status |
| Substance abuse | Charges |
| Admission to prison/forensic hospital | Length of sentence |
| Admission to community mental health facility | Prior incarceration |
| Other mental illness | Previous risk intervention |
| Deliberate self-harm |