
Abstract
Objectives
To examine the effectiveness of group cognitive behavioural therapy (CBT) for postpartum depression (PPD) delivered by public health nurses with little to no previous psychiatric training at improving depression, worry, social support and the mother-infant relationship.
Methods
Mothers (n = 141) living in Ontario, Canada with Edinburgh Postnatal Depression Scale Scores ≥10 and an infant <12 months of age were randomized to receive nine weekly 2-h sessions of in-person group CBT for PPD delivered by two public health nurses plus treatment as usual (TAU; experimental group) or TAU alone (control group). Primary outcomes were change in EPDS score and current major depressive disorder (Mini International Neuropsychiatric Interview) assessed immediately post-treatment (T2). Secondary outcomes included maternal worry, social support, and quality of the mother-infant relationship. All outcomes were assessed again six months post-treatment (T3).
Results
Participants in the experimental group had statistically significantly greater reductions in PPD symptoms immediately post-treatment (T2) (B = -5.35, p < 0.01), were more likely to manifest a clinically significant improvement in EPDS scores (≥4 points; OR = 3.44, 95%CI: 1.49–7.94), and no longer have symptoms consistent with current MDD (OR = 5.31, 95% CI: 1.78–15.83). Six months post-treatment (T3), experimental group participants had higher odds of clinically significant PPD improvement (OR = 5.10, 95%CI: 1.89–13.78), while 25% of the experimental group and 70% of remaining control group participants reported current MDD (p < 0.01). Statistically significant improvements in worry and the mother-infant relationship were also observed, decreases maintained at six months post-treatment.
Conclusions
Public health nurses with little to no previous psychiatric training can be trained to deliver effective group CBT for PPD to improve depression, worry, and the mother-infant relationship. Task shifting PPD treatment with group CBT to public health nurses could improve treatment uptake and lead to better outcomes for mothers, families, and the healthcare system.
(Trial Registration NCT03039530)
Introduction
Postpartum depression (PPD) is one of the most common complications of childbirth, affecting up to one in five mothers. 1 When those with elevated levels of depressive symptoms but not major depressive disorder are included, up to one in three are affected. 2 Postpartum depression is also associated with increased levels of worry and anxiety, 3 reduced social support, 4 and impairments in the mother-infant relationship. 5 While a single case of PPD is estimated to cost $125,000 (CAD) over the lifespan, 6 just 15% of mothers with PPD are able to access evidence-based treatment. 7
Clinical practice guidelines recommend evidence-based psychotherapies (e.g., cognitive behavioural therapy (CBT)) for most mothers with PPD.8–10 Unfortunately, healthcare systems are ill-equipped to treat problems requiring urgent psychotherapy like PPD. Mothers’ preferences for psychotherapy over antidepressant medications, difficulties accessing affordable trained psychotherapy providers, and long waitlists for specialized mental healthcare are barriers.10–12
Task shifting, the process of delegation whereby tasks are moved from specialized experts to those with less training provides a potential solution for addressing the PPD treatment gap. Task shifting has been used around the world to increase access to healthcare and is increasingly common in high-income countries. 13
Given their key role in PPD screening, public health nurses (PHNs) are a frequent first point of contact for those with PPD. Recently, a study that explored the implementation of psychological interventions for PPD found that the majority of mothers with PPD feel that nurses are the optimal non-specialist provider of these types of treatments. 12 Despite generally lacking formal psychiatric training, PHNs are frequently tasked with providing support to mothers with PPD and their infants. 14 These professionals also feel that their role should involve PPD management, particularly the provision of counselling. 15 However, training and a lack of programming for PPD remain key barriers. 16 While their high skill level can enable success, with formal psychotherapeutic training they could play a key role in increasing treatment access.
Studies that have assessed nurse-delivered psychotherapies for PPD have frequently aggregated outcome data with those of other professionals (e.g., psychologists), and so it is difficult to determine their effectiveness. Murray and colleagues (2001) showed that psychologists, midwives, or nurses could effectively deliver individual CBT for PPD, with clinical improvements that were greater for non-specialist (i.e., nurse/midwife) providers. 17 Milgrom et al. (2011) demonstrated that a psychoeducational program containing CBT elements delivered to individual mothers by nurses and psychologists was more effective than treatment as usual (TAU). 18 In a large cluster RCT, Morrell and colleagues (2009) found that 8 weeks of individually delivered CBT or person-centered therapy by nurses or midwives led to improvements at 6- and 12-months post-intervention. 19 However, the provision of 6-weeks of modified CBT by early childhood nurses was not found to be superior to individual non-directive support. 20 In the only group intervention that appears to have been tested to date, 21 nurses or midwives with specialized training successfully delivered an 8-week psychoeducational group for PPD with a CBT component to 45 mothers. Attendees noted improvements at 6 months compared to TAU. Finally, a recent RCT by Dennis and colleagues showed that Canadian nurses could deliver effective IPT for PPD on an individual basis by telephone, though half of nurses had prior specialized psychiatric training. 22
While these studies suggest that nurses can be trained to deliver effective psychotherapy for PPD to individuals and treatment by nurses is preferred, it is not known if PHNs with little to no prior psychiatric training can deliver effective group CBT for PPD. Group treatments are preferred by many mothers with PPD for the support, symptom normalization, and opportunity to learn via modeling they provide.23,24 Group therapies may also be more cost-effective, treat larger numbers of mothers and reduce waitlists, enabling specialist services to focus on more severely ill individuals.
The primary objective of this randomized controlled trial was to determine if PHNs can effectively deliver a 9-week group CBT for PPD intervention to mothers in community settings to improve PPD immediately post-treatment and six months later. Secondary objectives included assessing its impact on maternal worry, social support, and the mother-infant relationship. We hypothesized that PHNs could deliver group effective group CBT for PPD to improve depression, worry, social support, and the mother-infant relationship.
Method
Trial Design and Procedures
This parallel-group, one-site, randomized controlled trial (RCT) took place in the Niagara Region of Ontario, Canada from April 1, 2017 to January 20, 2020 (prior to the COVID-19 pandemic). Participants were recruited and allocated in a 1:1 ratio to experimental or control groups. The experimental group participated in a 9-week public health nurse-delivered group CBT for PPD intervention in addition to receiving TAU, while the control group received TAU alone. In Ontario, healthcare is universally available and so TAU could involve medications and/or psychotherapy from a physician and/or clinician at a provincially-funded facility/program. Private therapists or any other treatments could also be utilized. Mothers completed questionnaires using REDCap (Research Electronic Data Capture) 25 at baseline (T1), 9-weeks later (immediately post-treatment in the experimental group) (T2), and 6-months after T2 (T3).
Randomization with block sizes of four, six, and eight was conducted by an independent statistician in R 26 and implemented by the study coordinator using REDCap upon participant enrollment, ensuring allocation concealment. While participants, PHNs, and the study coordinator could not be blinded, research assistants completing data collection and data analysts were unaware of group status. The study was approved by the Hamilton Integrated Research Ethics Board and the Niagara Region Public Health Ethics Board and was registered (ClinicalTrials.gov: NCT03039530). Initially, we had planned 12- and 18-months post-treatment follow-ups, but this did not take place (resource limitations). No other study methods changed after trial commencement.
Participants
Mothers self-referred to the study after seeing advertisements on social media (e.g., Facebook) or were referred by a healthcare provider (e.g., physician, midwife) from April 1, 2017 to January 20, 2020. Eligible participants were ≥18 years-old, had an infant <12 months, an EPDS score≥10, and were living in the Niagara Region of Ontario at enrollment. This EPDS score was chosen as it is used in primary care settings to detect PPD 27 and maximizes eligibility and public health relevance (up to 30% of mothers have these symptom levels). 2 Participants were then screened using the Mini International Neuropsychiatric Interview (MINI) 28 and those with bipolar, psychotic, and/or current substance use disorders were excluded.
Public Health Nurse Training
Six public health nurses employed at Niagara Region Public Health were trained to deliver the intervention. 29 Prior to the trial, all six received two days of in-classroom training and then observed the 9-week intervention delivered in the setting in which it was developed. They then delivered the intervention, two at a time, recording sessions and receiving one hour of psychotherapy supervision by the expert therapists.
They had 6–26 years of experience working as a PHN and were all employed in the Family Health Division. In addition to delivering the CBT program as part of the trial, the PHNs were involved in delivery of a variety of services including well-baby clinics, infant sleep workshops, parenting programs, and breastfeeding clinics. None of the PHNs had prior specialized mental health training.
Intervention
The intervention was based on a previously validated treatment 30 and consisted of nine weekly 2-h sessions. No formal psychotherapy supervision took place during the trial, but a perinatal psychiatrist was available to provide support for emergencies. Each group was delivered by two nurses. The first half of each session consisted of core CBT content (e.g., cognitive restructuring), and the second half included psychoeducation and/or a discussion of topics relevant to PPD (e.g., sleep, supports) and co-led by mothers and PHNs.29,30 Each participant was provided with a copy of the CBT manual which detailed each week's content and included homework forms for practicing skills. The groups took place face-to-face in community locations including community centres and schools. Free childcare was offered.
Outcome Measures
Participants’ self-reported sociodemographic characteristics at enrollment including age, infant age, country of birth, number of children, marital status, years of education, household income, past psychotherapy, current antidepressant use, and mental health care visits in the previous 9 weeks. Participants provided data on our primary (depression) and secondary (worry, social support, mother-infant relationship) outcomes at T1, T2, and T3.
The primary outcome (depression) was assessed using the EPDS, a 10-item (α = 0.78) measure of maternal depression that assesses symptoms over the previous seven days. 31 Total scores range from 0–30, with scores of ≥10 indicating possible PPD. 31 Based on Jacobsen and Truax's reliable change index 32 and consistent with the work of others, 33 a change of ≥4 points was deemed indicative of a clinically significant change in depressive symptoms. 34 The MINI, a structured diagnostic interview, was also administered at T1, T2, and T3 to assess changes in current major depressive disorder (MDD) diagnosis.
The Penn State Worry Questionnaire (PSWQ) 35 is a 16-item scale (α = 0.86) that measures worry, a common PPD comorbidity, 3 with each item scored on a five-point scale (higher scores indicate greater severity). The PSWQ has good psychometric properties in adults. 35
The Social Provisions Scale (SPS), a 24-item (α = 0.91) questionnaire, assessed the degree to which an individual perceives their current social relationships to provide support. 36 Social support is a key risk factor for PPD development and persistence, 37 and its total scale score was used.
The Postpartum Bonding Questionnaire assesses the mother-infant relationship on four subscales: impaired bonding (α = 0.86), rejection and pathological anger towards the infant (α = 0.82), infant focused anxiety (α = 0.81), and incipient abuse. 38 The incipient abuse scale was not examined owing to past performance issues. 39
Sample Size and Statistical Analysis
We used SAS PROC POWER to estimate sample size and power requirements in longitudinal or repeated measures study designs. Our sample size was based on a type one error of 0.05 and 90% power to detect a difference between experimental and control arms of medium effect size in EPDS scores from T1 to T2 of 0.45 (Cohen's d). 40 Anticipating 35% attrition of enrolled women, the target sample size was 136 (68 per arm).
Statistical Analysis
The characteristics of participants in experimental and control groups were compared using t-tests and chi-square tests for continuous and dichotomous variables, respectively. All were examined as potential predictors of attrition, where we compared those who completed the study versus those who did not complete treatment and/or their T2 and/or T3 questionnaires.
This study follows an intention-to-treat (ITT) approach in which all available participant data is utilized regardless of treatment non-compliance, protocol deviation, or withdrawal following randomization. In keeping with ITT, all follow-up data obtained were analyzed according to participant randomization at the outset of the study. This yields a conservative estimate of treatment effect. 41
Continuous outcomes were analyzed using linear mixed models (LMM) with restricted maximum likelihood estimation. As the intervention was delivered between T1 and T2, T3 served to assess the stability of treatment effects. Models therefore compared change in score between T1 and T2, and then T2 to T3 independently, allowing us to quantify changes in symptom scores immediately following workshop completion, then separately assess the stability of treatment effects at T3.
A two-level hierarchy was employed in which continuous outcomes at each timepoint (level 1) were nested within participant (level 2). Group assignment was included as a fixed effect predictor, allowing us to assess the effect of the intervention over time between experimental and control groups. A random-effects intercept was also included in the model to adjust for unobserved heterogeneity at the level of the individual participant. As LMMs include observations of participants at T1 but who were subsequently lost to follow-up, this approach is more powerful than traditional repeated-measures techniques using listwise deletion.
For outcomes where statistically significant group by time interactions were observed, models were then stratified by intervention group to identify the magnitude of score change following group completion by the experimental group. Estimated marginal means of scale scores within each group at T1, T2, and T3 were reported to optimize the clinical interpretability of our results.
We also created logistic regression models to assess the odds of participants experiencing a clinically significant improvement in EPDS scores between groups, as well as change in current MINI major depressive disorder (MDD) status. Analyses were performed in SPSS 24 (IBM SPSS Statistics).
Results
A total of 234 participants were assessed for eligibility and 141 were randomized (experimental = 70, control = 71). Most participants were recruited through social media (62%) or public health (25%). Twenty-two participants declined to participate prior to the start of the intervention, and so 119 (experimental n = 57, control n = 62) completed baseline (T1) measures (Figure 1). The characteristics of experimental and control group participants are summarized in Table 1. There were no statistically significant differences between groups at baseline. Participants were approximately 31 years of age and most were married/living common-law. Their infants were an average of 5.5 months of age. The self-reported gender identity of all participants was female. An average of six participants attended each CBT group and they attended an average of seven sessions.
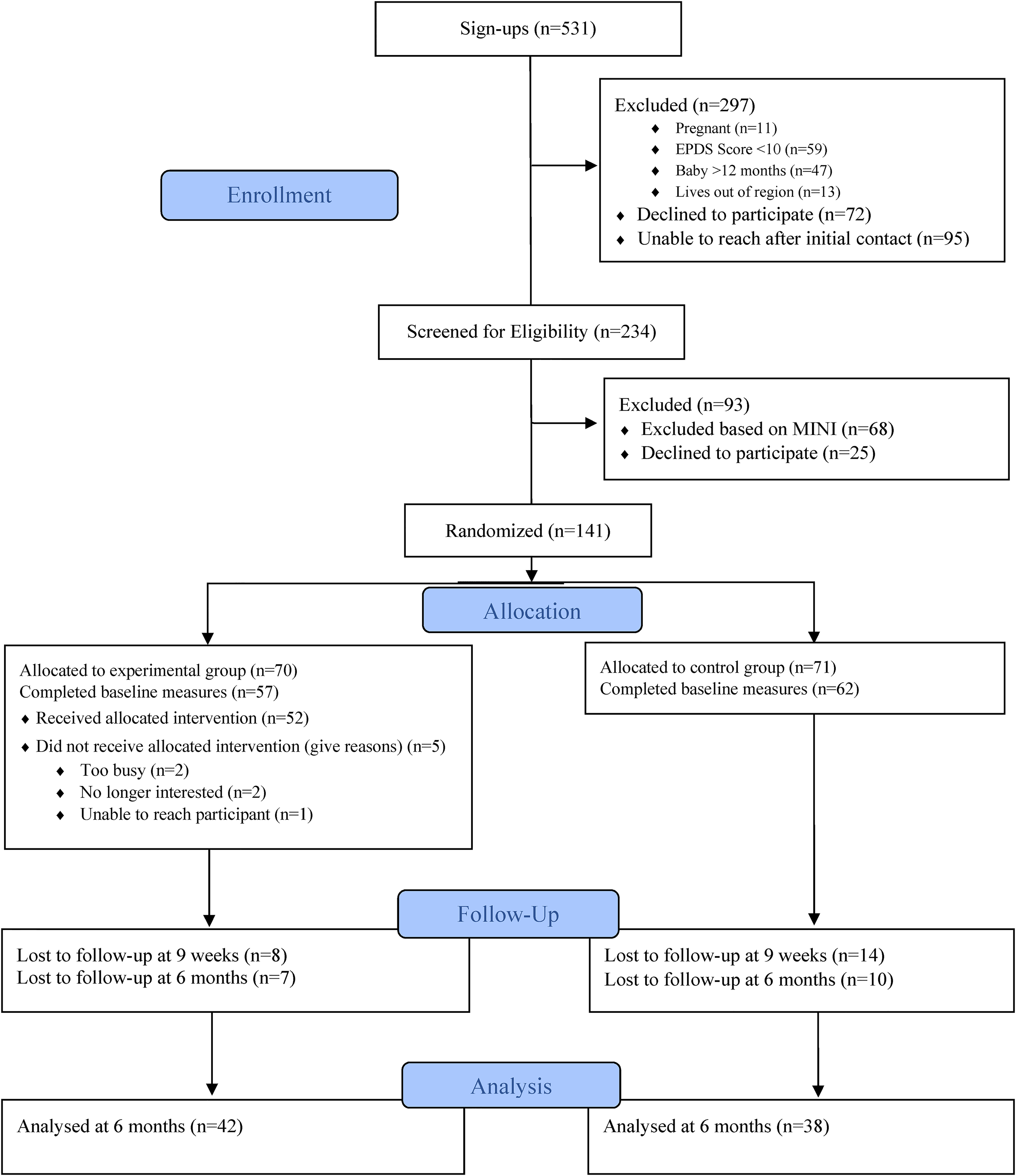
Flow of participants through the trial.
Summary of Participant Characteristics.
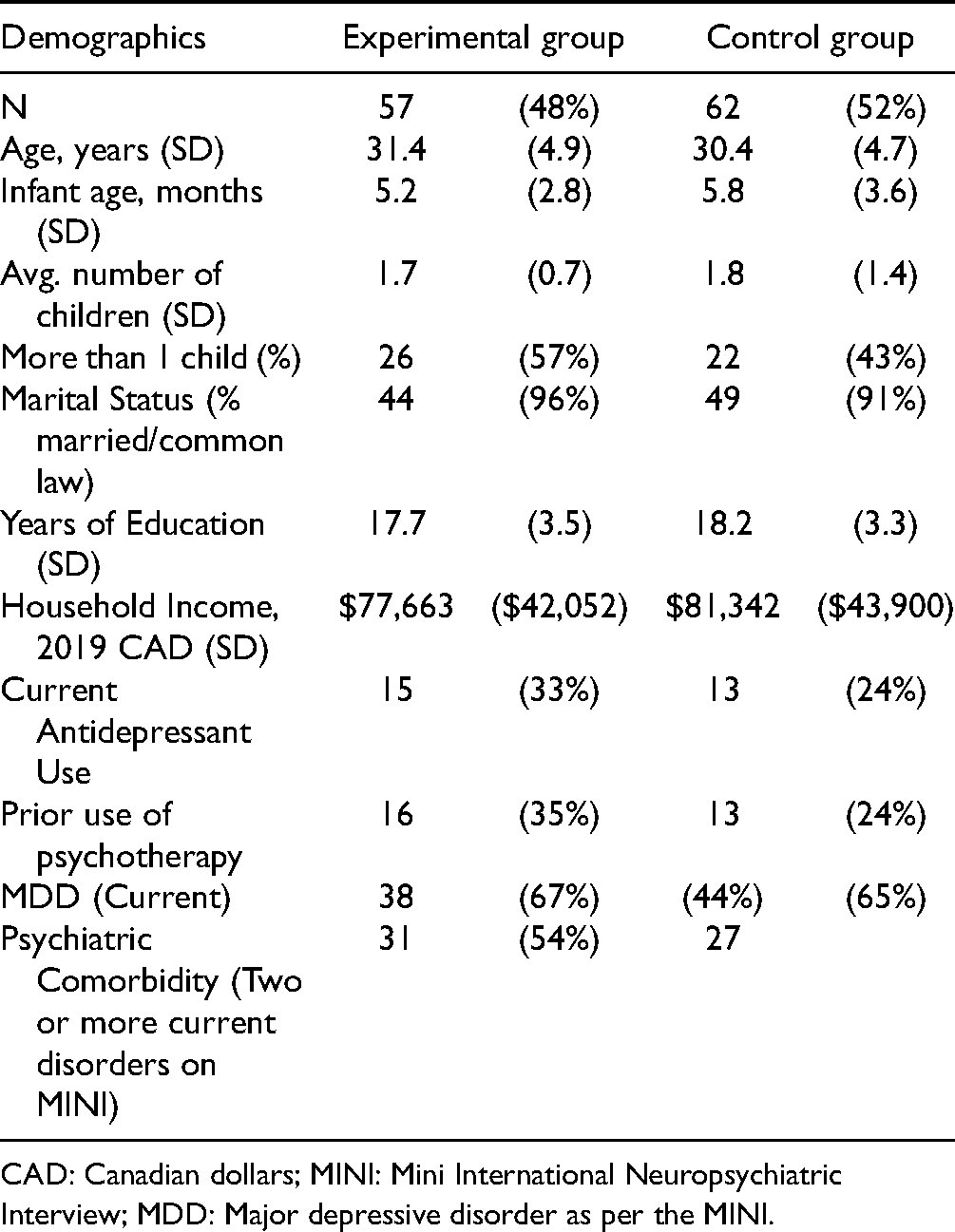
CAD: Canadian dollars; MINI: Mini International Neuropsychiatric Interview; MDD: Major depressive disorder as per the MINI.
Of the 119 participants, another 22 (19%) were lost to follow-up between T1 and T2. Of these, eight were in the experimental group (χ2 = 1.14, p = 0.23). Seventeen (14%) additional participants were lost to follow-up before they could complete T3. There were no statistically significant predictors of attrition among all sociodemographic characteristics assessed in this study in either group.
The MINI was completed by participants at each study visit. Current MDD was the most common diagnosis identified by the MINI, with 38 (67%) experimental and 40 (65%) control mothers endorsing these levels of symptoms at time of recruitment. Additionally, 86% of experimental participants and 84% of control participants reported a lifetime history of MDD (χ2 = 0.10, p = 0.75). Current generalized anxiety disorder was the most common comorbidity reported (50.4%).
Change in antidepressant usage did not differ between groups from baseline to T2 (χ2 = 1.73, p = 0.19), or T2 to T3 (χ2 = 0.03, p = 0.87). Likewise, the average number of mental health service visits did not differ between groups at T1 (1.00 vs.1.03, t = 0.07 p = 0.94), T2 ((0.75 vs.0.67, t = 0.67 p = 0.24), or T3 (2.00 vs.2.12, t = 0.13 p = 0.89).
Statistically significant group × time interactions predicted change in EPDS (B = -3.44, p < 0.01), PSWQ (B = -7.31, p < 0.01), PBQ-Bonding (B = -2.83, p = 0.01), PBQ-Rejection (B = -1.54, p = 0.03) and PBQ-Anxiety (B = -0.96, p = 0.03) scores from T1 to T2 (Table 2).
Scale Scores for Treatment and Control Groups at Each Study Visit.
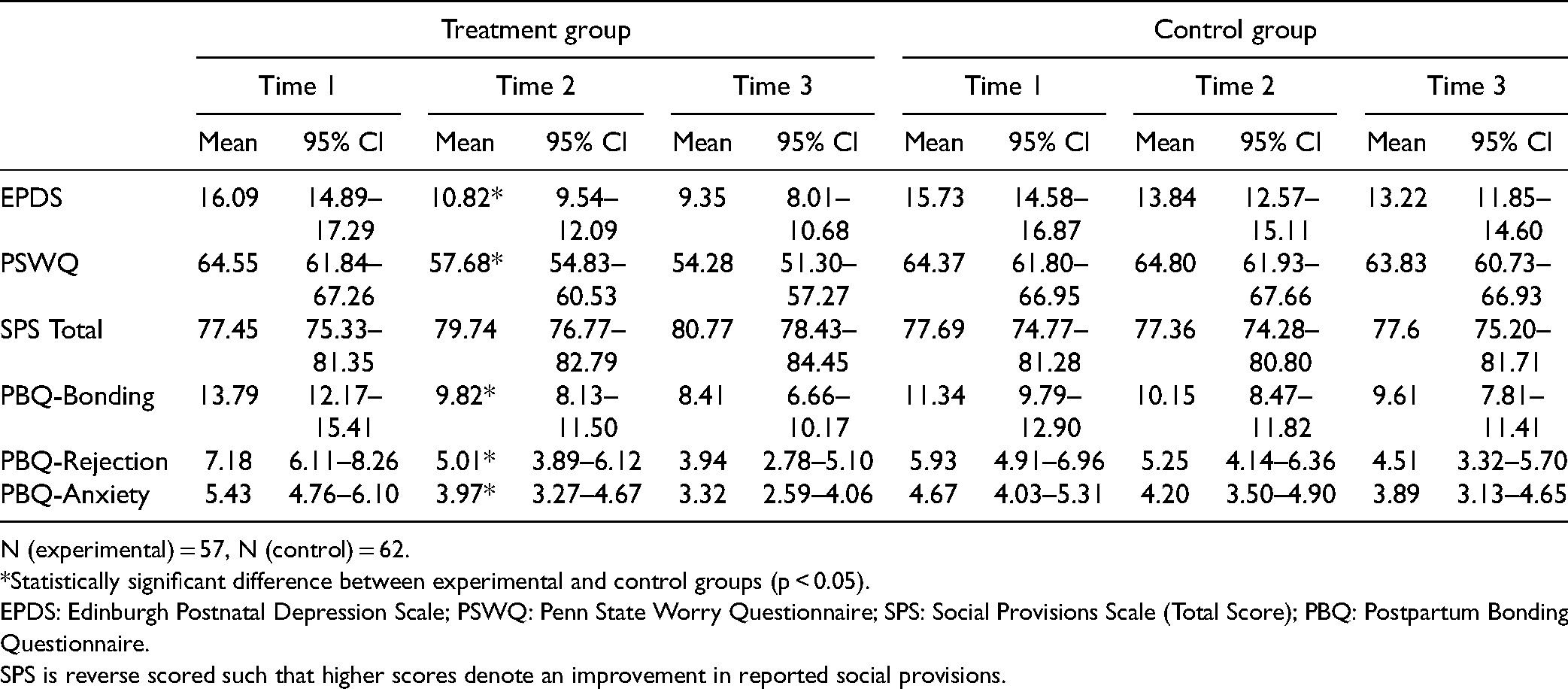
N (experimental) = 57, N (control) = 62.
*Statistically significant difference between experimental and control groups (p < 0.05).
EPDS: Edinburgh Postnatal Depression Scale; PSWQ: Penn State Worry Questionnaire; SPS: Social Provisions Scale (Total Score); PBQ: Postpartum Bonding Questionnaire.
SPS is reverse scored such that higher scores denote an improvement in reported social provisions.
For our primary outcome (PPD), participants who received group CBT reported EPDS scores that decreased from 16.1 at T1 to 10.8 at T2 (B = -5.35, p < 0.01), a clinically significant decrease from T1 to T2. They were also had three and a half times the odds of a clinically significant reduction in EPDS scores (≥4 points) compared to control participants (63.3% of experimental group vs. 33.3% of control group OR = 3.44, 95%CI: 1.49–7.94 (Risk Difference (RD) = 30%, Number needed to treat (NNT) = 3.3). Following treatment, 12 (25%) experimental group participants reported current MDD, while 26 (65%) control participants did (χ2 = 18.89, p < 0.01). Among participants who met the diagnostic criteria for current MDD at T1, those in the experimental group had five times greater odds of not reporting it after treatment (T2) compared to control participants (OR = 5.31, 95% CI: 1.78–15.83, RD = 40%, NNT = 2.5).
At T3 (six-months post-treatment), remaining experimental group participants had odds five times greater of a clinically significant improvement in EPDS scores (81% vs. 46%, OR = 5.10, 95%CI: 1.89–13.78, RD = 35%, NNT = 2.9). Nine (25%) experimental group participants and 23 (70%) control group participants reported current MDD (χ2 = 13.83, p < 0.01) at T3 (percentage changes are due to study attrition).
Treatment was associated with improvements in several secondary outcomes. Worry (PSWQ scores) decreased from 64.6 to 57.7 (B = −6.86, p < 0.01) following intervention. PBQ-Bonding scores in the experimental group improved from 13.79 to 9.82 (B = 4.08, p < 0.01) from T1 to T2, as did PBQ-Rejection (7.18 to 5.01, B = -2.25, p < 0.01), and PBQ-Iinfant-focused anxiety (5.43 to 3.97; B = −1.49, p < 0.01). Social support improved in the experimental group after treatment though the group × time interaction was not statistically significant (Table 2).
Between T2 and T3 (6-month follow-up), there were no significant group × time interactions to predict change in symptom scale score (Table 2), suggesting that the decrease in self-reported symptom severity following the completion of the CBT program was stable through six-months.
Discussion
Public health nurses with little to no previous formal psychiatric or psychotherapy training may be capable of delivering effective group CBT for PPD that leads to statistically and clinically significant improvements in PPD, as well as reductions in worry, infant-focused anxiety, anger and rejection, and improved mother-infant bonding, findings that remain stable up to six months post-treatment. This intervention respects women's treatment preferences and has potential for scalability (including online) to increase treatment access.
The changes that accompany PHN-delivered group CBT for PPD are similar in magnitude to trials of other evidence-based psychotherapies for PPD delivered by experts in individual or group format.40,42 The results of the current study also complement the recent work of Dennis and colleagues (2020) that showed that nurses can deliver IPT successfully by telephone. 22 Since CBT can be successfully delivered online, 43 group delivery by PHNs could increase treatment uptake during and after the COVID-19 pandemic.
Improvements were also noted in maternal worry, changes that persisted six months after the intervention. While the group CBT program did not specifically target worry or anxiety, it contained a number of CBT strategies that could have helped (e.g., cognitive restructuring, relaxation techniques, problem solving). The findings of this work are consistent with previous trials of structured psychotherapies for PPD, 42 important findings given increasing recognition of high rates of postpartum anxiety, particularly among those with PPD. 3
Stable improvements were also reported in the mother-infant relationship. Such changes are important given their long-term effects on offspring emotional and behavioural functioning. 44 While our findings were based on maternal reports alone, bonding, infant-focused anxiety and rejection and anger all improved. These may have been due to mothers’ utilization of CBT skills in their interactions with infants, improvements in depression and/or anxiety, or the informal teaching of skills by PHNs, all of whom had experience with public health messaging around mother-infant attachment.
Surprisingly few RCTs of maternal PPD treatment have examined its impact on the mother-infant relationship. Studies of IPT alone have not consistently led to improvements in mother-infant attachment,36–38 but interventions focused on the mother-infant relationship have showed more promise.45–47 Murray and colleagues’ RCT comparing three different psychotherapies (including CBT) to routine care showed that objective measures of the mother-infant relationship improved immediately post-treatment (4.5 months), but not at 18 or 60 months. 17 While the improvements observed in our study remained stable to six months, it is unclear how much longer they persist.
Despite being conducted in group format, no statistically significant group by time interaction was observed for social support. However, a post-hoc analysis of the experimental group did suggest a statistically significant improvement. Trials of IPT for PPD have frequently shown that individual or group treatment can increase social support. 42 However, this may be due to the fact that the core goals of IPT include depressive symptom improvement and enhanced social support.
One limitation of this trial is that it was conducted at a single centre. Given the public health focus of this study, our main eligibility criterion (EPDS≥10) was intentionally inclusive, though on average, participants had at least moderate levels of depression, and two-thirds endorsed current MDD at baseline. While not every participant in the study met full diagnostic criteria for current MDD, since mothers with subsyndromal levels of PPD also have poor outcomes (because they often fail to seek treatment and are ineligible for clinical services),48,49 these findings could still have important implications. Participants were mainly white, married, and educated, and had access to universal healthcare, so our results may not generalize to samples in all settings. While PHNs did utilize a structured manual and underwent rigorous training prior to the trial, a formal measure of adherence to the CBT model was not utilized. Moreover, since no other active control (e.g., psychoeducation) group was included, improvements in participants could have been contributed to by factors other than CBT alone. Future studies should formally assess therapist adherence and competence. While participant attrition rates are consistent with those in the literature,40,42 they were higher at T3, and could affect the generalizability of our results. Groups generally contained six participants and so it is not known how larger numbers of participants might affect effectiveness. Since changes in PPD and ratings of mother-infant outcomes tend to be correlated, changes noted in the mother-infant relationship could reflect improvements in maternal depression alone. It also remains to be seen if PHN-delivered group CBT for PPD can have a positive impact on offspring outcomes, and if it is cost-effective.
Women with elevated levels of symptoms of PPD are in urgent need of timely, accessible, equitable, and effective psychotherapeutic treatments. Public health-nurse delivered group CBT for PPD is a scalable treatment that could be delivered in-person or online to improve access to effective treatment for mothers with PPD around the world, with significant potential benefits for them, their families, and healthcare systems.
Footnotes
Acknowledgments
The authors would like to acknowledge the Public Health Nurses who facilitated the CBT groups and the participants who participated in this study.
Data Access
The data that support the findings of this study are available from the corresponding author (RV) upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Hamilton Academic Health Sciences Organization (HAHSO) AFP Innovation Fund (grant number HAH-16-05) and PSI Foundation Mental Health Grant (grant number 16-49).