
Abstract
Objectives:
Following recommendations from the Lower Risk Cannabis Use Guidelines, we evaluated how lower risk cannabis use (late initiation and low use frequency) was associated with the risk of developing cannabis abuse/dependence over a 3-year follow-up period compared to 12-month abstinence (controls) or higher risk cannabis use (early initiation and higher use frequency). We also explored the effect of cannabis quantity.
Methods:
Data were obtained from the U.S. nationally representative survey, National Epidemiologic Survey on Alcohol and Related Conditions wave I (2001 to 2002) and wave II (2004 to 2005), which included 31,464 respondents with no lifetime history of cannabis abuse/dependence at the first interview. We applied multiple logistic regression and propensity score matching analyses to examine the association between different use patterns at wave I and cannabis abuse/dependence at wave II, adjusting for covariates. Lower risk cannabis use and the transition to higher use frequency were also assessed.
Results:
For propensity score analysis, lower risk cannabis use at wave I was associated with higher risk of cannabis use/dependence at wave II compared to controls (odds ratio [OR]: 4.27; 95% confidence interval [95% CI], 1.57 to 11.61); however, there was no association with use frequency increase (OR: 2.52; 95% CI, 0.88 to 7.17). Higher risk use had a greater risk of cannabis use/dependence than controls (OR: 6.27; 95% CI, 2.56 to 15.38) and lower risk use (OR: 2.69; 95% CI, 1.12 to 6.47). Logistic regression analyses showed similar results, except that lower risk use was significantly associated with use frequency increase (OR: 2.49; 95% CI, 1.22 to 5.08). For the lower risk use group, 1 to 3 joints/day of use was significantly associated with cannabis abuse/dependence.
Conclusions:
We found that following recommended use patterns can significantly lower one’s risk of cannabis abuse/dependence. However, risk of cannabis abuse/dependence is still 4 times higher than staying abstinent. Updated recommendations on safe cannabis exposure levels are needed to guide cannabis use in the general population after cannabis legalization.
Introduction
As cannabis legalization has gained momentum in Canada and the United States, the public perception toward risks of cannabis has shifted. Statistics Canada followed up on national cannabis use before and after recreational cannabis legalization in October 2018. In 2019, Statistics Canada released results of the National Cannabis Survey, reporting that over 16% of Canadians aged 15 or older have used cannabis in the last 3 months. 1 Among these respondents, about 646,000 people were first-time users. The report also demonstrated that people who used cannabis weekly and occasionally increased after legalization. 1
Although cannabis has been shown to have lower risk than other drugs including tobacco and alcohol, it is associated with multiple acute 2,3 and chronic side effects. 2,4 –6 Long-term use could also lead to cannabis use disorder (CUD), which can be impairing. 7,8 CUD has become one of the most common substance use disorders in North America. 2 About 4% to 8% of adults have been estimated to have CUD during their lifetime. 9 The risk of CUD increases to 16% for those who initiated cannabis use in adolescence and 33% to 50% for daily smokers. 2 Multiple psychosocial treatment approaches have been explored for CUD, some of which have shown efficacy. 7,10 However, available treatments appear to have high relapse rates. 11 Food and Drug Administration approved pharmacologic treatments are currently not available for CUD. At the same time, studies suggest that CUD has increased after cannabis legalization. 3,7,12
As cannabis is becoming more acceptable and available to the public, it is crucial to investigate the health implications of cannabis legalization and mitigate its adverse effects on public health. To control the cannabis market under strict regulations, the Cannabis Act was released. 13 However, the act was not constructed based on public health effects of cannabis use levels. 14 Alternatively, the Lower Risk Cannabis Use Guidelines (LRCUG) was released as an evidence-based tool to lower the health risks of cannabis. To inform cannabis use behaviors with lower adverse health outcomes, Fischer et al. systematically reviewed the modifiable risk factors of cannabis-related health consequences. 15 The guidelines cover recommendations on frequency of use, age of initiation, potency of cannabis, smoking behaviors, driving, and psychiatric risk factors.
However, the guidelines were only able to provide quantitative recommendations on the age of initiation and frequency of use while making arbitrary suggestions on other exposure measures (e.g., choosing products with lower tetrahydrocannabinol (THC) content). As cannabis has been legalized in Canada, it is worth re-examining the health outcomes of the general population who use recreational cannabis following a less risky use pattern based on the quantitative recommendations in LRCUG (i.e., age of initiation and frequency of cannabis use). Furthermore, quantity is also an important predictor of cannabis use outcomes. 16 Although the quantity measure of cannabis consumption is not standardized, quantifying cannabis use may add more information to the study of the risk of cannabis use. This study primarily aims to determine whether following the suggested cannabis use pattern (i.e., lower risk cannabis use) could protect one from developing cannabis abuse/dependence. We (1) compared the risk of transitioning to a higher frequency cannabis use pattern as well as the risk of developing cannabis abuse/dependence among lower risk cannabis users to 12-month abstainers (i.e., controls); (2) compared the risk of cannabis abuse/dependence in those who did not follow suggested cannabis use pattern (i.e., higher risk use pattern) to 12-month abstainers; and (3) compared the risk of cannabis abuse/dependence among those following higher risk use pattern to those with lower risk use. We hypothesized that no significant association would be found in the first comparison, while a significant association would be found in the second and third comparisons. In this study, we also made an attempt to explore the effect of cannabis quantity on cannabis abuse/dependence by adding the number of joints consumed per day into the outcome analysis.
Methods
Sample
Data were collected from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) wave I (N = 43,093) and wave II (N = 34,653), which has been described in detail elsewhere. 17 The wave I survey data were collected in 2001 to 2002, containing a nationally representative sample of noninstitutionalized U.S. citizens (including Alaska and Hawaii) and noncitizens between 18 and 99 years of age. Black, Hispanic respondents, and young adults (between 18 and 24 years) were oversampled. Weights were adjusted for nonresponse and differential probabilities of participant selection to match demographic distributions in the United States. The wave II survey was completed in 2004 to 2005 as a 3-year follow-up. The response rate of wave II was 86.7%. 18 Research protocol and informed consent procedures have obtained approval from the U.S. Census Bureau and the U.S. Office of Management and Budget. In this study, we only included respondents who participated in both waves with no lifetime cannabis use abuse/dependence at time of wave I interview.
Measures
Cannabis use patterns
Referring to the LRCUG quantitative recommendations, cannabis use patterns were defined according to respondents’ age when they first experimented with cannabis and 12-month cannabis use frequency in wave I interview (i.e., “how often used cannabis in the last 12 months”). The control group included individuals who never used cannabis and those who have abstained for at least 12 months preceding the interview. The lower risk use group consisted of respondents who reported first using cannabis at age 16 or older and consumed cannabis 1 to 2 times/week at most in the past year (i.e., used cannabis once a year to 1 to 2 times/week). The higher risk use group consisted of respondents who reported first using cannabis before age 16 and/or consumed cannabis more than 1 to 2 times/week in the past year (i.e., used cannabis 3 to 4 times/week to every day).
We formed 3 comparison groups: controls versus lower risk use group (treatment exposure), controls versus higher risk use group (treatment exposure), and lower risk versus higher risk use groups (treatment exposure).
Outcomes
The primary outcome is the diagnosis of cannabis abuse/dependence at wave II. Diagnoses of cannabis abuse/dependence as well as other psychiatric disorders were made according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria using Alcohol Use Disorder and Associated Disabilities Interview Schedule 4. For the lower risk use group, the risk of proceeding to higher use frequency (i.e., consuming cannabis 3 to 4 times/week to every day) was also explored.
Covariates
We included demographic characteristics, preliminary factors, substance use, and lifetime Axis I and II psychiatric diagnoses, which were evident risk factors of cannabis use and/or cannabis abuse/dependence. 19 –25 Demographic characteristics consisted of age, sex, race/ethnicity (White or non-White), education, and marital status. Preliminary factors included parental absence (did not live with biological parents before age 18 or parents not living together before age 16), parental loss (death of parents before age 16), parental violence (frequency of parents fighting before age 18), childhood sexual abuse (frequency of sexual abuse before age 18), childhood maltreatment (frequency of physical abuse or neglect experience before age 18), history of family economic challenge (family received money from government assistance program before age 18), social deviance (number of conduct disorder or antisocial personality disorder behaviors before age 15), family history of alcohol or drug use disorder, and early substance use (any substances use before age 16). Lifetime Axis I and II psychiatric diagnoses consist of mood disorders (major depressive disorder, dysthymia, manic, and hypomanic disorders), anxiety disorders (panic disorder, social phobia, specific phobia, and generalized anxiety disorder), personality disorders (conduct disorder, antisocial, avoidant, dependent, obsessive-compulsive, paranoid, schizoid, histrionic personality disorders), and drug use disorders (any substance use disorders except alcohol, tobacco, and cannabis abuse/dependence). Lifetime use of other substances (excluding cannabis) at wave I was also included in the analyses. Among the covariates, the demographic characteristics (sex and race/ethnicity) and the preliminary factors (parental absence, parental loss, childhood sexual abuse, childhood maltreatment, history of family economic challenges, family history of alcohol or drug use disorders, social deviance, low self-esteem, and early substance use) are baseline covariates that occurred before the initiation of cannabis use among those in the lower risk use group (or before age 16 or 18 in other study groups).
Statistical Analyses
We first examined the association between cannabis use patterns and the outcomes of interest using multivariate logistic regression, adjusted for covariates mentioned above. Odds ratios (ORs) and 95% confidence intervals (CIs) of cannabis abuse/dependence at wave II by past year cannabis use at wave I were obtained. For the controls versus lower risk use comparison, the OR of proceeding to higher frequency cannabis use was also computed. The cutoff for significance was P = .05.
Second, we adopted a propensity score method to derive a robust prediction model for cannabis use patterns. We estimated the average treatment effect on the treated, 26 in which we compared the average effect on risk of outcomes for individuals in the exposure group with controls. We performed regression-based propensity score matching on the previously listed baseline covariates. 27 The sampling weight of each respondent was also added in the propensity score model as a baseline covariate to account for the complex survey design of NESARC. 28
For the lower risk use versus controls and the higher risk use versus controls comparisons, we performed optimal matching by pairing each exposure with 8 controls. Both matchings were done without control sample replacement to avoid impacting the weighting design of NESARC data. Therefore, each control was only matched once. For the higher risk versus lower risk use comparison, we performed optimal matching with a 1:2 pairing ratio. As sample sizes of these 2 groups were similar, the “replacement” option was chosen so that 2 respondents in the lower risk group were matched more than once. According to Stuart, this method can decrease bias. 26 Numerical and graphical summaries were used to examine the balance in covariate distribution between exposure and control groups. The propensity score models were adequately specified when standardized differences in means of all covariates were less than 0.2.
We compared covariates between the 3 use pattern groups using χ2 tests, setting the level of significance at P < 0.05. We performed multivariate logistic regression analyses on the propensity score matched comparison groups to assess outcomes of interest. Effect sizes (i.e., ORs and 95% CIs) were obtained, adjusted for residual covariates that were not baseline covariates. Propensity score matching procedures were conducted using the “MatchIt” package in R. 29 Logistic regression analyses were performed using SUDAAN 11.0.1 to account for weights and other complex survey design features of the NESARC. 30
Results
There were 31,646 respondents with no lifetime history of cannabis abuse/dependence. The control group consisted of 31,127 individuals, who abstained from cannabis use for at least 12 months. The lower risk cannabis use group contained 317 respondents, who initiated cannabis use at or over 16 years of age and consumed cannabis 1 to 2 times/week at most in the last 12 months before wave I interview. The higher risk use group contained 202 respondents, who initiated cannabis use before 16 years of age or consumed cannabis more than 1 to 2 times/week in last 12 months before wave I interview.
Table 1 summarizes the covariate distributions of the 3 cannabis use pattern groups and includes demographic characteristics, early life adversities, substance use, and lifetime Axis I and II psychiatric diagnoses. Current cannabis use groups tended to be younger than controls, with a higher proportion of male respondents. Compared with the other 2 groups, the lower risk use group had more respondents with higher educational levels (some college or higher). Cannabis use groups had more respondents who were never married. Individuals in cannabis use groups were more likely to experience early life adversities (parental absence, parental violence, childhood sexual abuse, childhood maltreatment, history of family economic challenge) than controls. Individuals in cannabis use groups also reported a family history of alcohol or drug use disorders more often than controls.
Comparisons of Demographics, Early Life Adversities, Clinical Diagnoses, and Drug Use between 3 Cannabis Use Patterns: Controls, Lower Risk Cannabis Use, and Higher Risk Cannabis Use.
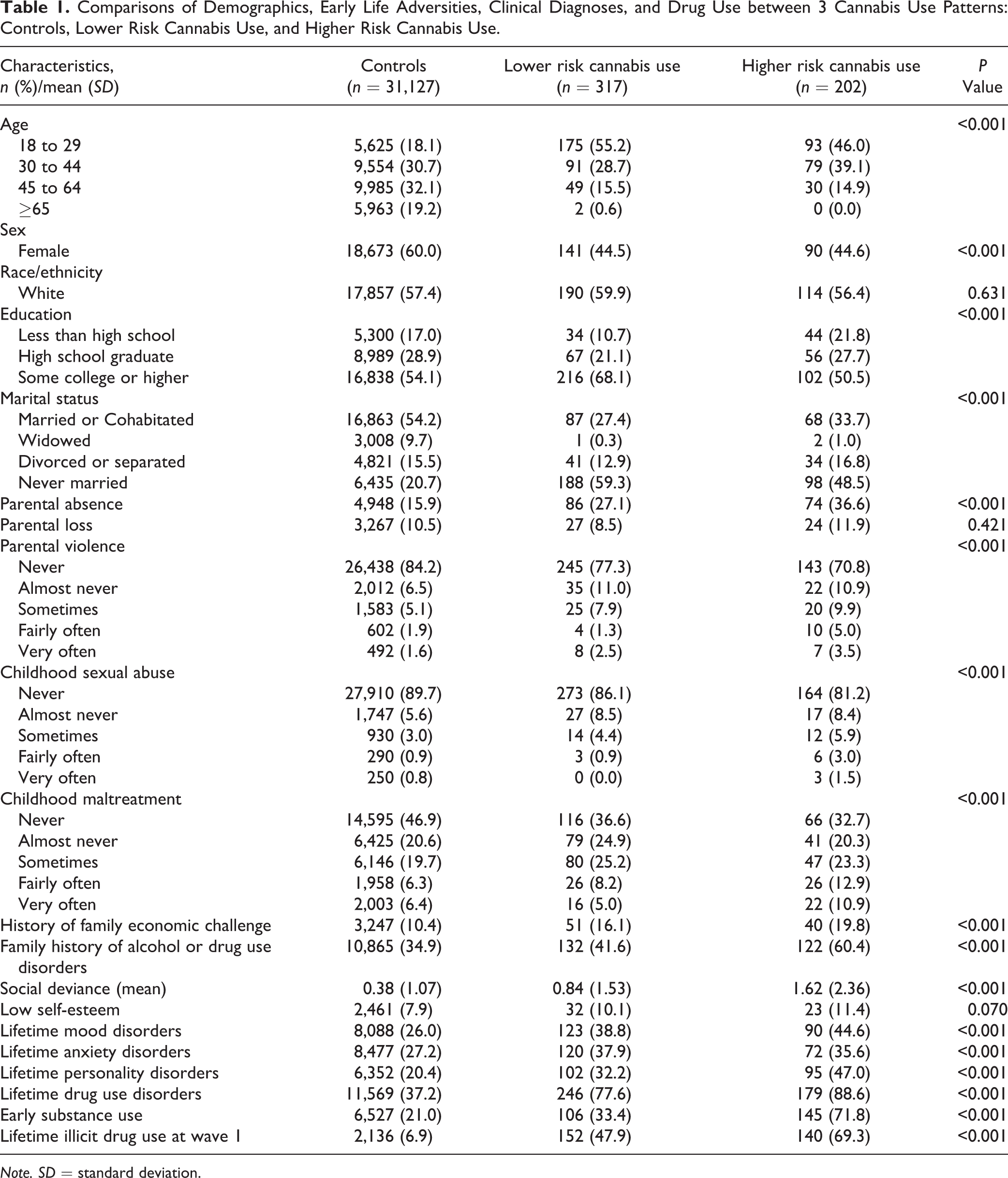
Note. SD = standard deviation.
The 2 cannabis use groups had higher proportions of individuals reporting social deviance behaviors and Axis I and II psychiatric diagnoses including mood disorders, anxiety disorders, personality disorders, and drug use disorders in their lifetime but not low self-esteem. Early substance initiation (initiation of alcohol, tobacco, and other illicit drugs before age 16) and experience with illicit drug use at wave I interview were more common in the cannabis use groups.
Logistic regression results in Table 2 show that the lower risk use group was more likely to increase their 12-month frequency of use at wave II (OR: 2.49; 95% CI, 1.22 to 5.08), compared to controls. Lower risk cannabis use was also significantly associated with cannabis abuse/dependence at wave II (OR: 2.92; 95% CI, 1.50 to 5.69). Higher risk use was associated with significantly higher odds of cannabis abuse/dependence (OR: 8.43; 95% CI, 4.25 to 16.72). As expected, odds of cannabis abuse/dependence in the higher risk use group was significantly higher than those in the lower risk group (OR: 3.63; 95% CI, 1.67 to 7.91).
Associations (ORs, 95% CI) between Cannabis Use Pattern in the Past 12 Months at NESARC Wave I and High Frequency Cannabis Use or Cannabis Use Disorder Outcome at NESARC Wave II.
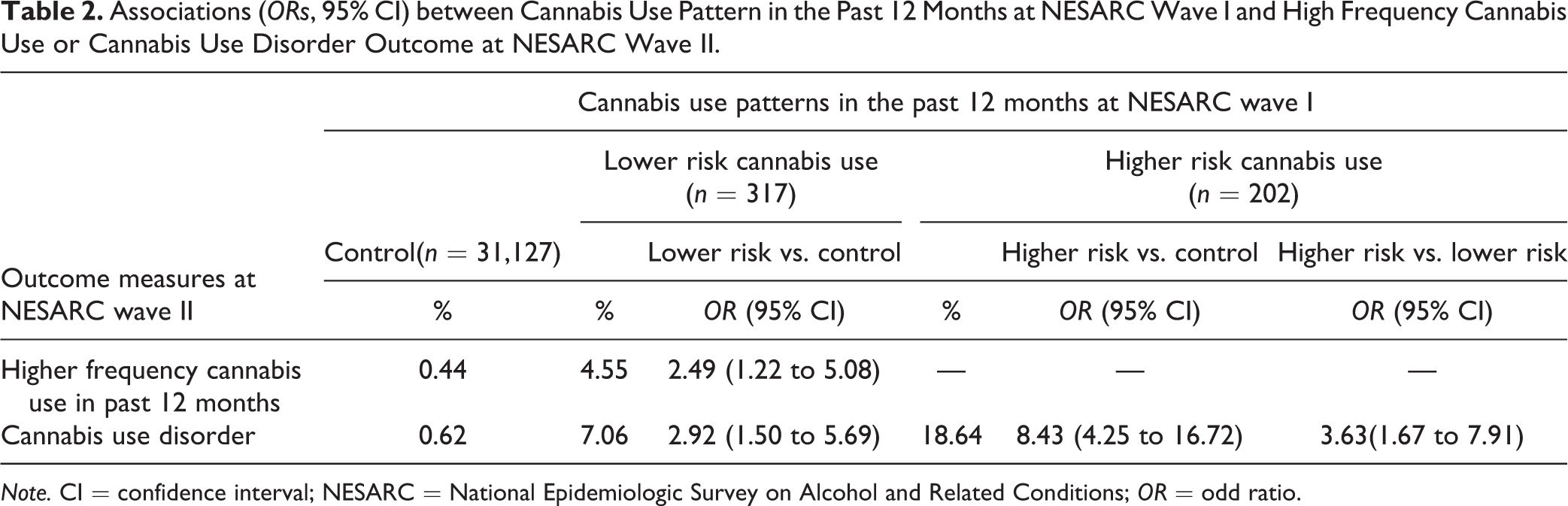
Note. CI = confidence interval; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions; OR = odd ratio.
Table 3 shows results from analyses using propensity score-matched data. After balancing for distribution differences in baseline covariates, the association between lower risk use and frequency of use at wave II was no longer significant (OR: 2.58; 95% CI, 0.88 to 7.17). Compared to controls, the odds of developing cannabis abuse/dependence among lower risk (OR: 4.27; 95% CI, 1.57 to 11.61) and higher risk use (OR: 6.27; 95% CI, 2.56 to 15.38) groups remained significant. Significant association also remained in the high risk versus lower risk comparison (OR: 2.69; 95% CI, 1.12 to 6.47). We also explored interaction effects of cannabis use patterns by adding the interaction of cannabis use pattern and age or sex to the regression models. Based on Wald F test results (setting level of significance as P < 0.05), we did not find strong evidence that cannabis use patterns were moderated by age or sex.
Association between Cannabis Use Patterns in the Past 12 Months at NESARC Wave I and High Frequency Cannabis Use or Cannabis Use Disorder Outcome at NESARC Wave II after Baseline Covariate Adjustment Using Propensity Score Matching Method.
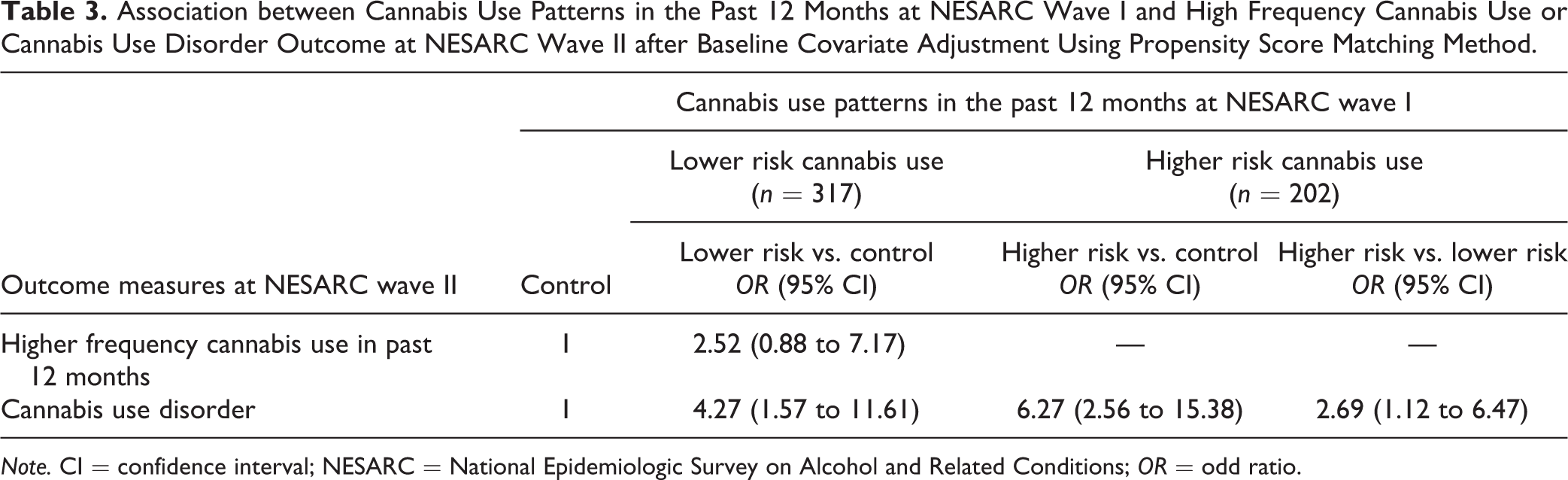
Note. CI = confidence interval; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions; OR = odd ratio.
We further explored the relationship between cannabis exposure and cannabis abuse/dependence. Based on the interview question: “number of cannabis joints usually smoked in a day in the last 12 months,” we included lower risk users with certain quantities of cannabis use to the lower risk versus controls model. We found that lower risk users who reported smoking 1 to 3 “joints”/day (or 1 to 6 joints/week; n = 312) encountered significantly higher odds of cannabis abuse/dependence than the 12-month abstainers (or 0 joints/week; OR: 5.17; 95% CI, 2.11 to 12.69).
Discussion
Consistent with previous literature, cannabis use is associated with being young, male, single, early life adversities, and more social deviance behaviors. 19,24 As expected, Axis I and II diagnoses and cannabis use are closely related. Family history of substance use disorders and personal experience with other illicit drugs were also related to cannabis use. The higher risk use group has a particularly higher proportion of other illicit drug consumption. This finding aligns with the observation that both early initiation and regular cannabis use are strongly associated with other illicit drug use. 31
As expected, respondents in the higher risk use group were most likely to experience cannabis abuse/dependence in the 3-year follow-up. This finding is in line with the quantitative recommendations of the LRCUG. Starting cannabis use later in life and consuming cannabis with a lower frequency can significantly lower one’s risk of cannabis abuse/dependence. 2,32
However, we also found that respondents in the lower risk group had a greater risk of cannabis abuse/dependence than controls. We applied the propensity score matching method to match cannabis use groups with controls based on their baseline demographic characteristics and early life experience, while controlling for other covariates. Findings remained significant with the exception that the association between lower risk cannabis use and the transition to higher use frequency lost significance. The results suggest that those who use cannabis with a lower risk use pattern may not practice higher use frequency overtime. However, they are still more vulnerable to cannabis abuse/dependence.
Research suggests that the harms of cannabis depend on age of initiation, frequency of use, and quantity of exposure. 33 Compared with controls, the significantly high risk of lower risk users developing cannabis abuse/dependence could possibly be explained by the inclusion of individuals who consumed cannabis with a high THC content or at a high dose. Therefore, we took into consideration the daily number of cannabis joints consumed. We found that smoking 1 to 3 joints/day is significantly associated with cannabis abuse/dependence. Estimating an average amount of 0.32 g in a typical joint based on data from 2000 to 2010, this group was exposed to up to 0.96 g cannabis in an average day. 34 This confirms that quantity of use is another important predictor of cannabis-related health outcomes, further suggesting the need to foster future research in quantity measures and include such findings in cannabis use guidelines and policies. 16
In this survey, we were not able to accurately quantify cannabis exposure. In fact, it is always challenging to determine the dose and potency of the substance due to the large number of cannabinoids in cannabis plants, 32 variations in strains, growing methods, and manufacturing processes. 35 Nonetheless, the study results should still raise concerns, taking into consideration a consistent increase of average THC content in cannabis over the last 2 decades (1995 to 2014). 36,37
With lots of unanswered questions remaining, a focus on public health education is crucial at this current stage. The LRCUG serves as an important source of education for those who are considering consuming cannabis for recreational purposes. As stated in the guidelines, staying abstinent is the best way to avoid any risks from cannabis use. The lower risk use pattern in this study does not protect one from cannabis abuse/dependence, rather it causes a 4 times increased risk of developing cannabis abuse/dependence than staying abstinent. A precautionary approach with lower threshold may be more protective to public health as the availability and acceptability of cannabis increases following legalization in Canada. 15 As more research evidence evolves, we will be able to generate a more detailed LRCUG with more information on exposure measures. Therefore, it is important to foster research on the harmful effects of cannabis use in the general population as well as to keep re-examining and updating the recommendation items of the LRCUG.
This study has included respondents who experimented cannabis before 16 years old in the control group, which may compromise the effect sizes of outcomes. Therefore, we performed additional analyses by excluding controls with early onset cannabis use and conducted the same regression tests. For lower risk versus controls, we found that the odds of higher use frequency (OR: 2.00; 95% CI, 0.70 to 5.75) and cannabis abuse/dependence (OR: 4.53; 95% CI, 1.79 to 11.42) were similar to previous models. On the other hand, the odds of cannabis abuse/dependence (OR: 11.59; 95% CI, 3.48 to 38.59) were higher for the higher risk versus controls comparison, indicating that the effect size was compromised by the inclusion of respondents with early onset cannabis use. However, the overall findings were consistent with previous model, which did not change our study conclusions.
The results of this study should be interpreted under the consideration of several limitations. First, due to the limitation of available data, this study only directly examined 2 items of the LRCUG (i.e., age of initiation and frequency of use) and could not cover the entire cannabis use guidelines. For example, NESARC surveys only focus on cannabis plant smoking, while less harmful ways of use recommended by the LRCUG (e.g., extracts vaporizing, edibles consumption) were neglected. However, the study findings should still apply to most cannabis users, as cannabis plant smoking still accounts for over 90% of overall cannabis use in Canada. 36 Second, our study does not establish a causal relationship between cannabis use pattern and new onset of cannabis abuse/dependence due to possible residual confounding factors that were not collected in this survey. Third, some early life adversities may include events occurring after cannabis initiation, meaning the risk of reverse causality could not be eliminated. Fourth, the validity of self-reported data may be compromised by social desirability and recall biases. Recall bias is most possible in the age of cannabis initiation and early life experience. Fifth, NESARC wave I and II were conducted 15 years ago, when DSM-IV criteria were used instead of the new Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria. This means that the current study may overestimate the effect size of CUD. Furthermore, multiple cannabis-related policy changes have taken place in the United States after the NESARC survey was conducted. Therefore, changes in social desirability bias as well as use patterns of different demographic groups should be taken into consideration while interpreting our study findings. Lastly, the data used for this study were based on the U.S. population and may diminish the generalizability to the Canadian population. Nonetheless, our study provides prospective evidence from a large nationally representative cohort, which serves as a strong source to re-examine the current cannabis use guidelines for the public.
Conclusions
In this study, we confirmed that late cannabis initiation and lower use frequency can significantly lower one’s risk of developing cannabis abuse/dependence. However, following these quantitative recommendations from the LRCUG is still associated with a 4 times increased risk of cannabis abuse/dependence than staying abstinent. There is still limited evidence on safe levels of cannabis exposure. However, as cannabis is legalized in Canada, a precautionary approach on public health education with lower exposure threshold is needed to guide safe cannabis use in the general population. It is also expected that national scale longitudinal surveys containing use of various cannabis products and more standardized determination of safe cannabis exposure measures can be conducted in Canada.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Le Foll has received research support from Bioproject, Alkermes, Canopy, ACS, and Aurora. Ms Chen has received grants from MITACS accelerate program (in partnership with Canopy Growth Corporation). The supporting sources had no role in the research, authorship, and/or publication of this article.