
Abstract
Objective:
To provide the most up-to-date prevalence estimates of alcohol and illicit drug use among individuals with psychosis in Australia, and explore correlates associated with a lifetime diagnosis of both alcohol abuse/dependence and cannabis abuse/dependence.
Method:
This paper uses data from the Survey of High Impact Psychosis (SHIP), conducted as a follow-up to the first Australian National Low Prevalence (Psychotic) Disorders Study (1997–1998). The SHIP was a national study, carried out across five states, in which a sample of 1825 individuals was recruited through a two-phase sampling framework.
Results:
Alcohol and illicit drug use was highly prevalent for the entire sample. There were few significant differences in the prevalence or frequency of use across the diagnostic categories examined. Substantial increases in substance abuse/dependence were noted since the 1997–1998 survey (51% diagnosed with alcohol abuse/dependence, 51% with cannabis abuse/dependence and 32% with other illicit drug abuse/dependence, compared to 28%, 23% and 12% respectively, in the 1997–1998 survey by Kavanagh et al., 2004). Factors significantly associated with both lifetime alcohol and cannabis dependence included male gender, younger age, single marital status, lower educational attainment, shorter duration of illness, lifetime presence of hallucinations, higher negative syndrome score and lower body mass index (BMI). A number of other factors were found to be differentially associated with either lifetime alcohol or cannabis dependence.
Conclusions:
The use of alcohol and illicit substances is common among people with a psychotic illness, with a concerning upward trend in rates of substance abuse/dependence since the 1997–1998 survey. Clinicians should be aware of the potential impact of concurrent substance use and provide integrated treatment for individuals presenting with psychotic illnesses. More research and investment in new intervention programs is required.
Introduction
There is considerable evidence to suggest high rates of co-morbid drug and alcohol problems among individuals with schizophrenia and other psychotic disorders. Estimates from studies conducted in Australia and internationally suggest that 40–50% of all people with schizophrenia will have a ‘dual diagnosis’ with a substance use disorder (SUD) over their lifetime (Blanchard et al., 2000; Kavanagh et al., 2004; Regier et al., 1990); these estimates are some 3–5 times higher than the general population (Australian Bureau of Statistics, 2008; Regier et al., 1990). Furthermore, the co-occurrence of schizophrenia and SUDs has been linked to poorer global functioning, as well as a range of other negative outcomes including criminality, homelessness, re-hospitalisation, unemployment, violence and suicidal behaviour (Blanchard et al., 2000). Tobacco (70–90% lifetime prevalence), alcohol (30–40% lifetime prevalence) and cannabis (20–30% lifetime prevalence) are the most frequently and consistently cited substances of concern among individuals with schizophrenia over their lifetime (Blanchard et al., 2000; Koskinen et al., 2009; Koskinen et al., 2010; O’Daly et al., 2005; Regier et al., 1990).
Causal explanations for the high rates of SUDs among individuals with psychotic illnesses have been widely debated, yet younger age and male sex remain the strongest predictors (Blanchard et al., 2000). Most previous research has focused on assessing current psychiatric symptoms (positive, negative and depressive) to determine whether those with psychotic illnesses misuse substances to relieve symptoms of their disorder, reduce adverse side effects of medication or enhance social interaction (Potvin et al., 2006; Talamo et al., 2006). The evidence, even across meta-analyses, is contradictory, in part reflecting differences in the scales used to assess psychiatric symptoms, or the sample used (i.e. inpatient or outpatient) (Potvin et al., 2006; Potvin et al., 2007; Talamo et al., 2006). Cognitive deficits are considered to be a core feature of schizophrenia (Elvevåg and Goldberg, 2000), and it is widely accepted that individuals with a history of SUD suffer from an excess of cognitive deficits, but the association appears to be less consistent among those with co-morbid substance use disorders and schizophrenia (Potvin et al., 2008). Indeed, some studies of people with schizophrenia have found that cannabis users have better cognitive function than non-cannabis users (Rabin et al., 2011). Inconsistent findings may reflect the heterogeneous nature of schizophrenia, or the need to account for other underlying factors (i.e. age or substance-type preference) (Potvin et al., 2008).
The current study uses data collected as part of the Survey of High Impact Psychosis (SHIP). The SHIP was conducted as an extension to the first Australian National Low Prevalence (Psychotic) Disorders Study, which was conducted in 1997–1998 with a broadly representative sample of people with psychotic illnesses across four urban sites around Australia. The 1997–1998 survey comprehensively documented the prevalence of psychosis, the associated symptom profile, quality of life and service use (Jablensky et al., 2000). The survey found that 40% of individuals with psychosis had a lifetime diagnosis of substance abuse/dependence, with 17% having a lifetime diagnosis of abuse/dependence on more than one substance (Kavanagh et al., 2004). Male sex was the most consistent correlate of a lifetime diagnosis of substance abuse/dependence. Furthermore, certain psychosis-related factors were found to be associated with a lifetime diagnosis of cannabis misuse (e.g. younger age, lower educational attainment and impairment due to medication), but not alcohol, whereas others were associated with a lifetime diagnosis of alcohol misuse [e.g. course of illness (multiple versus single episode), older age at psychosis onset and a premorbid personality disorder], but not cannabis (Kavanagh et al., 2004).
The current study extends this earlier work to provide up-to-date prevalence estimates of alcohol and illicit drug use among Australians with psychotic disorders. In addition, we conducted disorder-specific comparisons of alcohol and illicit substances, and examined a wide range of correlates associated with a lifetime diagnosis of both alcohol abuse/dependence and cannabis abuse/dependence. We do not address tobacco use here; that is the subject of a separate paper in this issue (Cooper et al., 2012).
Method
The second national survey of psychosis covered an area of 62,000 square kilometres and a population of some 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age group. A two-phase design was used. In Phase I, screening for psychosis took place in public specialised mental health services and in non- government organisations supporting people with a mental illness. In Phase II, people who were screen positive for psychosis in Phase I were randomly selected and stratified by age group (18–34 years and 35–64 years) for interview and assessment. The census month was March 2010. Of 7955 people who were screen positive for psychosis and eligible, 1825 were interviewed in Phase II (from 4189 individuals who were contacted for interview). Data were collected on symptomatology, substance use, cognitive ability, functioning, disability, physical health, mental health service use, medication use, education, employment and housing. The study was approved by institutional human research ethics committees at each of the seven study sites and all participants provided written, informed consent. Full details of the survey methodology and measures are given in Morgan et al. (2012).
Clinical assessments
The Diagnostic Interview for Psychosis (DIP) (Diagnostic Module) is a semistructured clinical interview used to generate both Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) and International Classification of Diseases, 10th revision (ICD-10) diagnoses (Castle et al., 2006). The DIP assesses family history of schizophrenia, lifetime prevalence of hallucinations and delusions, duration and course of illness, as well as measures of lifetime suicidal behaviour (attempts and ideation), and alcohol and illicit drug abuse/dependence. In the DIP respondents are asked a range of questions covering lifetime (e.g. ‘Have you ever . . .’) and past year (‘In the past 12 months have you . . .’) use of alcohol and other illicit substances. Interviewers were instructed to code ‘no’ to alcohol use if the respondent reported only ever having an alcoholic drink on a rare occasion. In addition, respondents were asked whether a number of consequences from substance use occurred at any time in their lives including, but not limited to, tolerance, withdrawal, feelings of guilt, inability to control use and legal/work/social problems. This information on substance use is used to provide a DSM-IV lifetime diagnosis of alcohol abuse/dependence as well as lifetime cannabis abuse/dependence. Substance use was also assessed using a number of established validated measures, namely: the Alcohol Use Disorders Identification Test (AUDIT) (Babor et al., 2001), the Drug Abuse Screening Test (Skinner, 1982), the CAGE Questionnaire (Mayfield et al., 1974) and the Fagerström Test for Nicotine Dependence (Heatherton et al., 1991). Amphetamine and cocaine use were combined into a ‘stimulant’ use category, and heroin, tranquilliser, inhalant, ecstasy and hallucinogens were combined into an ‘other illicit drugs’ category.
The DIP also assessed sociodemographics, childhood experiences (including occurrence of distressing or traumatic events), social participation and functioning, physical health (including family history of illness), psychopathology (negative symptoms, as well as worry, panic, anxiety and obsessions), cognitive function, service use and perceived need for services.
Statistical analyses
Analyses were conducted using the Stata version 11.2 software (StataCorp LP, College Station, Texas, USA). Means and standard deviations were calculated for continuous variables and frequencies were measured for categorical variables. For categorical variables, differences between diagnostic groups were analysed by chi-square or Fisher exact tests as appropriate; the Fisher exact tests were applied in case of an expected frequency of less than five. For all statistically significant chi-square analyses, follow-up multinomial logistic regressions were conducted using schizophrenia/schizo-affective disorder as the reference category.
For continuous variables, diagnostic group differences were examined using one-way analyses of variance (ANOVAs). Welch’s ANOVA was used when the homogeneity of variance assumption was violated. A series of logistic regression models were conducted to determine predictors of a lifetime diagnosis of alcohol abuse/dependence and a lifetime diagnosis of cannabis abuse/dependence, respectively. For all analyses, a value of p < 0.05 was considered statistically significant.
Results
Sample characteristics
Table 1 presents the characteristics of the sample. The majority of the sample was male, with an average age of 38 years. Just fewer than 50% of the sample reported a post-school qualification and slightly more than half were unemployed at the time of the interview (53%). Nearly all participants reported deterioration from their premorbid level of functioning (90%). Just under two-thirds of the sample was diagnosed with schizophrenia/schizo-affective disorder (63%), 17% with bipolar disorder (mania), 15% with other psychotic disorders and 4% with psychotic depression, according to the ICD-10 criteria.
Characteristics of the sample (N = 1825).
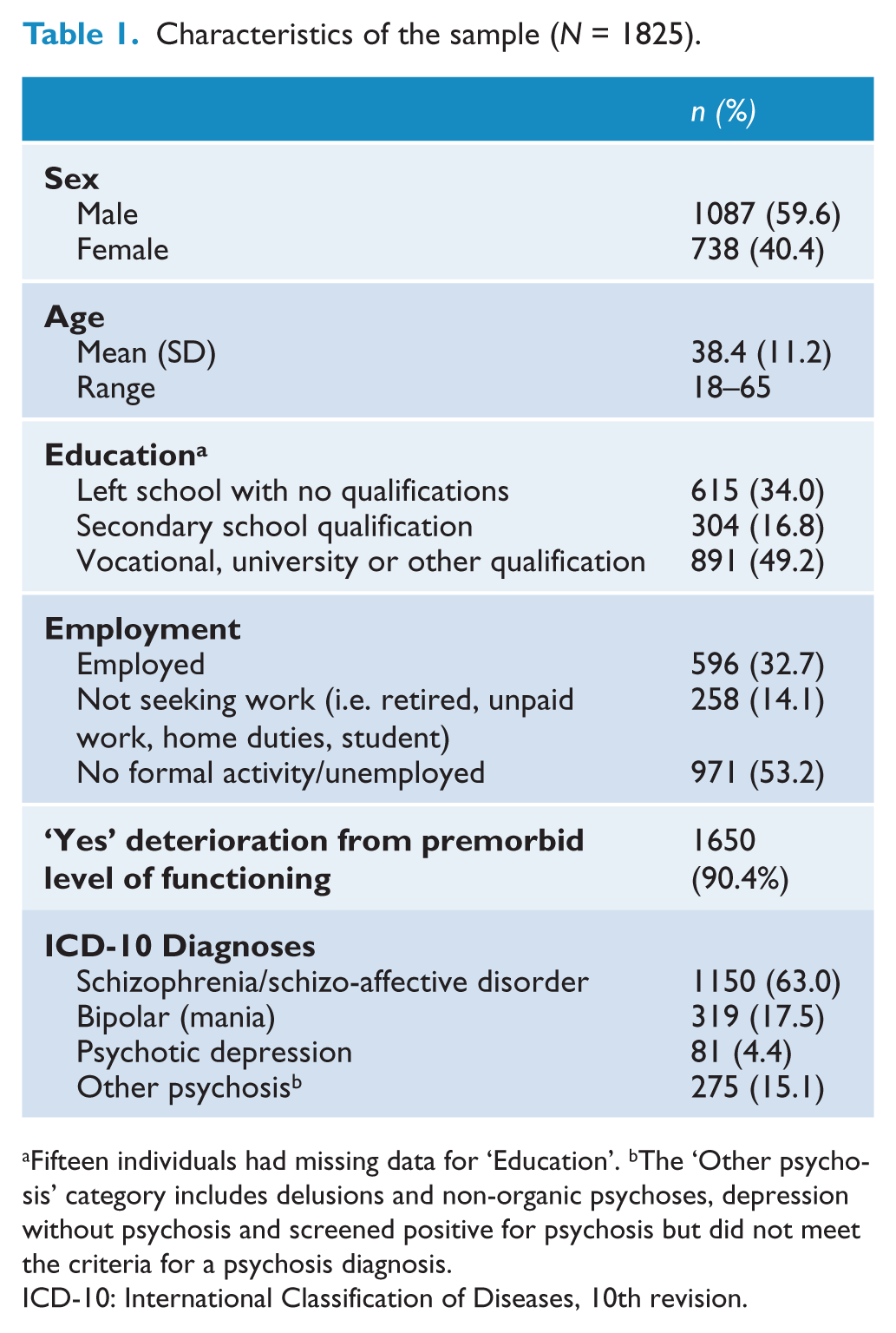
Fifteen individuals had missing data for ‘Education’. bThe ‘Other psychosis’ category includes delusions and non-organic psychoses, depression without psychosis and screened positive for psychosis but did not meet the criteria for a psychosis diagnosis.
ICD-10: International Classification of Diseases, 10th revision.
Prevalence and frequency of alcohol and illicit substance use
Table 2 presents data on the prevalence and frequency of alcohol and cannabis use. Ninety-two per cent of the sample reported lifetime alcohol use, with the majority also reporting alcohol use in the past year (81%). A third of the sample reported monthly or weekly alcohol use in the year prior to illness onset (36%), and 58% of the sample reported daily/almost daily alcohol use during their heaviest use period. Almost all of the individuals assessed reported cannabis use at some point in their life (97%), with past-year cannabis use reported by just under half the sample (49%). The majority of the sample reported either daily/almost daily (47%) or monthly/weekly (17%) cannabis use in the year prior to illness onset, and 75% of those who reported ever using cannabis had used daily/almost daily during their heaviest use period. Around three quarters of the sample reported stimulant use (including amphetamines or cocaine) and/or other illicit drug use (including heroin, tranquilliser, inhalant, ecstasy and hallucinogens) over their lifetime, with daily/almost daily use common during their heaviest use period (42% for stimulants, 36% for other illicit drugs).
Prevalence and frequency of alcohol and cannabis use.
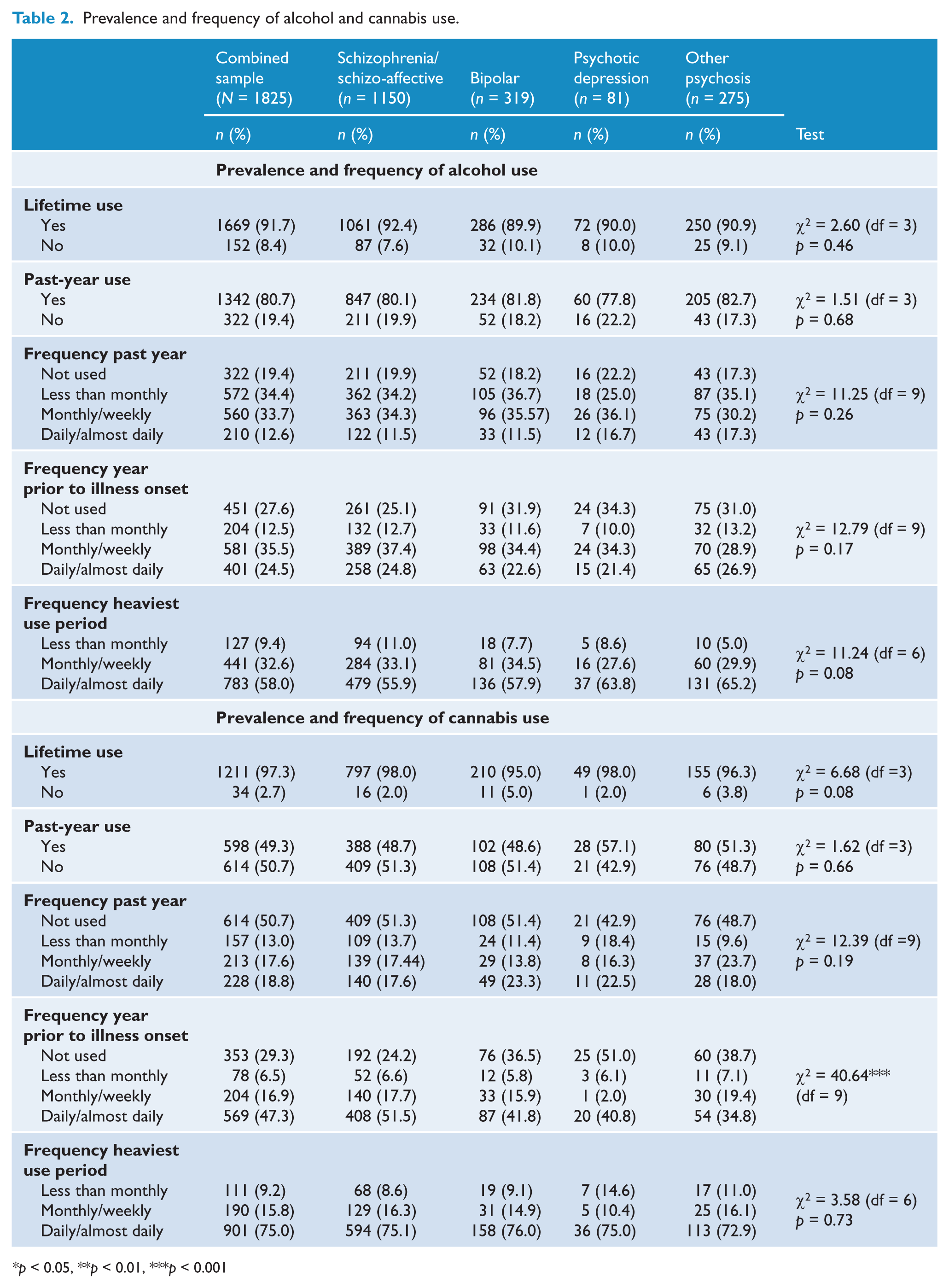
p < 0.05, **p < 0.01, ***p < 0.001
Prevalence and frequency of substance use by diagnostic subgroup
For alcohol, there were no significant diagnostic subgroup differences in lifetime use, past-year use, frequency of past-year use or frequency during their heaviest use period for alcohol (Table 2). The only significant group differences identified in the prevalence and frequency of illicit drug use was for use in the year prior to illness onset (Tables 2 and 3). Individuals with schizophrenia/schizo-affective disorder were significantly more likely to have used cannabis daily or almost daily (versus not at all) compared to each of the other three diagnostic groups [bipolar disorder: odds ratio (OR) 1.85, 95% confidence interval (CI) 1.30–2.63, p < 0.01; psychotic depression: OR 2.63, 95% CI 1.45–5.00, p < 0.01; other psychoses: OR 2.38, 95% CI 1.59–3.57, p < 0.001] (Table 3). In addition, individuals with schizophrenia/schizo-affective disorder were significantly more likely to report stimulant use, compared to those with bipolar disorder [monthly/weekly use (versus not at all): OR 1.89, 95% CI 1.09–3.23, p < 0.01; daily/almost daily (versus not at all): OR 2.27, 95% CI 1.25–4.17, p < 0.01] and those with other psychoses [monthly/weekly use (versus not at all): OR 2.70, 95% CI 1.43–5.88, p < 0.001]. Similarly, individuals with schizophrenia/schizo-affective disorder were more likely to report using other illicit substances weekly/monthly (versus not at all), compared to those with bipolar disorder (OR 2.13, 95% CI 1.22–3.57, p < 0.01) and those with psychotic depression (OR 5.26, 95% CI 1.20–20.00, p < 0.05).
Prevalence and frequency of stimulants and other illicit substance use.
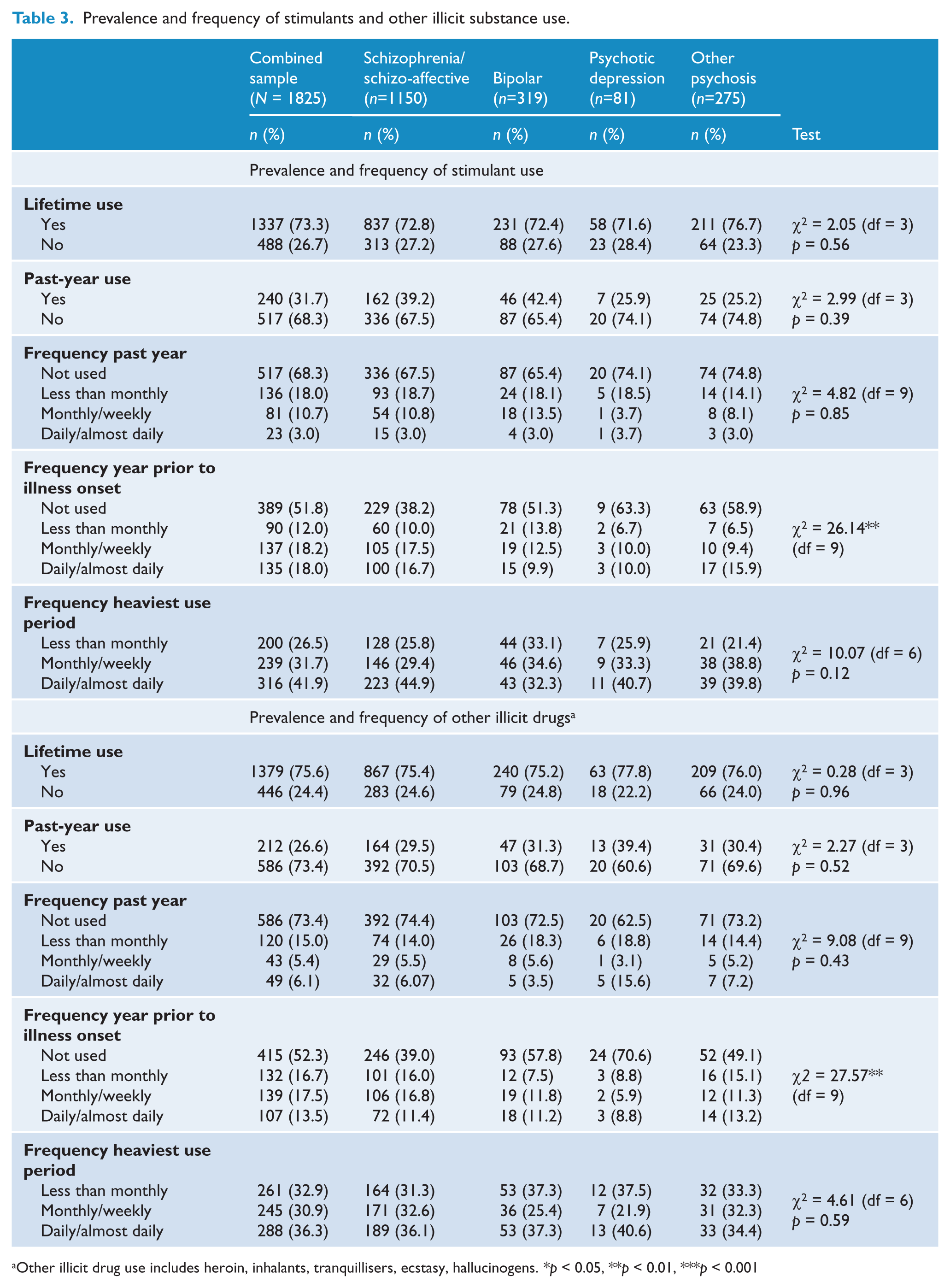
Other illicit drug use includes heroin, inhalants, tranquillisers, ecstasy, hallucinogens. *p < 0.05, **p < 0.01, ***p < 0.001
Consequences of alcohol and other illicit drug use
Cannabis was cited most often as the primary drug of concern (i.e. the one that has caused the most problems) (44%), followed by alcohol (24%) and amphetamines (19%). In addition, participants were asked to report whether they experienced a number of specific potential consequences from substance use over their lifetime, either never, in the previous 12 months or at some point in their lives, but not in the previous 12 months (‘outside of the previous 12 months’).
Table 4 presents data on the consequences of alcohol use. Most commonly reported were: unable to recall the night before due to drinking (62.1% over lifetime), wanting to cut down or not being able to cut down on alcohol (60.5% over lifetime) and experiencing an impaired capacity to control alcohol use once they started drinking (46.8% over lifetime). The consequences reported least often were experiencing nervous or medical problems as a result of alcohol (21.3% over lifetime), seeking help to reduce alcohol use (21.8%) and experiencing withdrawal symptoms (28.4%).
Consequences of alcohol use.
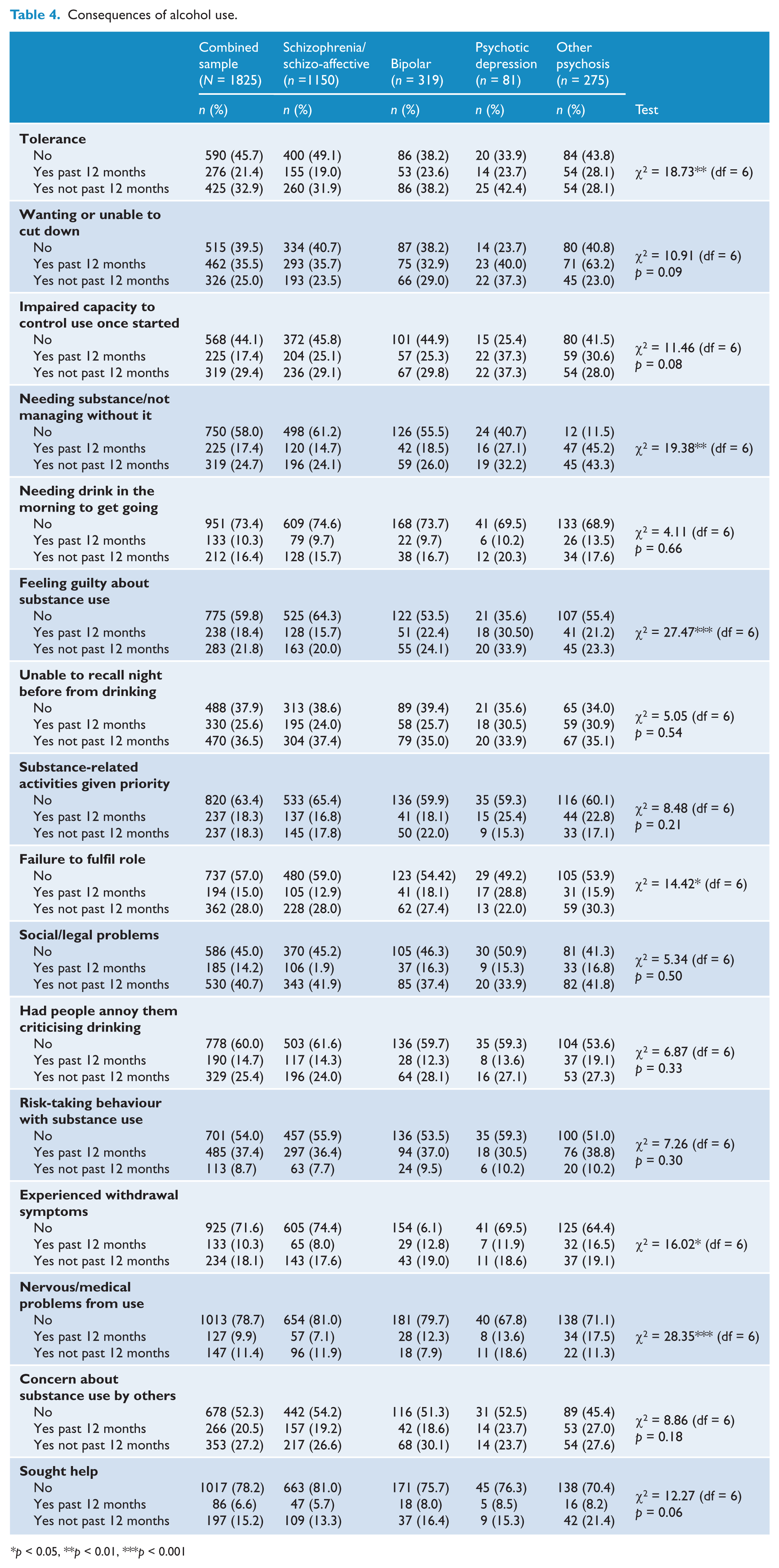
p < 0.05, **p < 0.01, ***p < 0.001
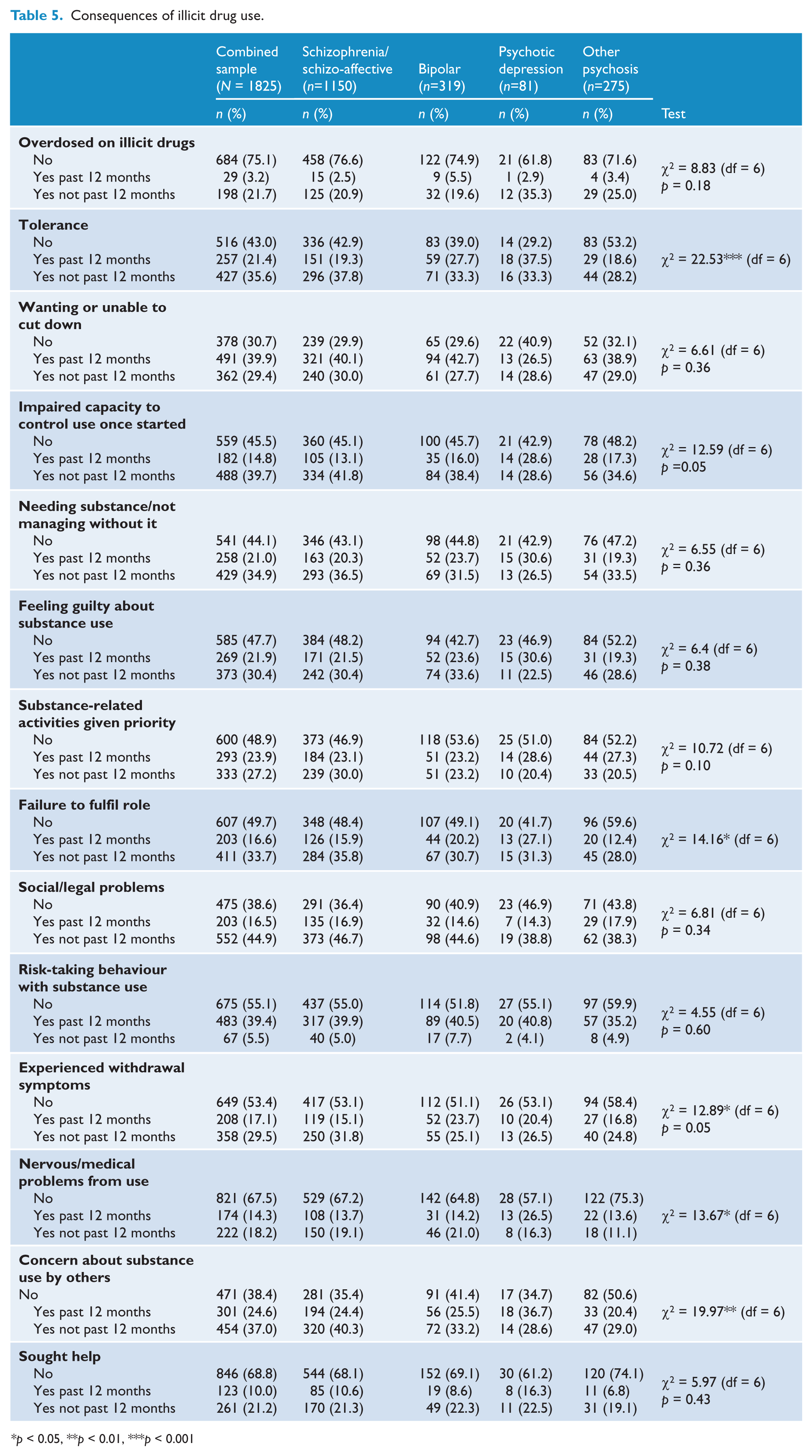
Table 5 presents data for the consequences resulting from illicit drug use. Having a desire to cut down or being unable to cut down on illicit drug use (69.3%) was the most commonly reported consequence, followed by experiencing concern about illicit drug use from others (61.6% over lifetime) and having social/legal problems as result of illicit drug use (61.4% over lifetime). Consequences reported least often were experiencing an overdose from illicit drug use (24.9% over lifetime), seeking help to reduce illicit drug use (31.2%) and developing nervous or medical problems as a result of illicit drug use (32.5% over lifetime).
Consequences of illicit drug use.
p < 0.05, **p < 0.01, ***p < 0.001
Consequences of alcohol use by diagnostic subgroup
Individuals with schizophrenia/schizo-affective disorder were significantly less likely to report experiencing tolerance to alcohol at some point in their lives, compared to each of the other three diagnostic groups (bipolar disorder: previous 12 months OR 0.63, 95% CI 0.43–0.93, p < 0.05, and outside of previous 12 months OR 0.65, 95% CI 0.46–0.90, p < 0.05; other psychoses: previous 12 months OR 0.35, 95% CI 0.17–0.75, p < 0.01; psychotic depression: outside of the previous 12 months OR 0.52, 95% CI 0.28–0.95, p < 0.05). Similarly, individuals with schizophrenia/schizo-affective disorder were significantly less likely to report needing alcohol/not managing without it, compared to those with psychotic depression (previous 12 months OR 0.36, 95% CI 0.19–0.70, p < 0.01; and outside of the previous 12 months OR 0.50, 95% CI 0.27–0.93, p < 0.05) and other psychoses (previous 12 months OR 0.52, 95% CI 0.35–0.78, p < 0.01). Individuals with schizophrenia/schizo-affective disorder were also significantly less likely to report feeling guilty about alcohol use at some point in their lives, compared to each of the other diagnostic groups (bipolar disorder: past 12 months OR 0.58, 95% CI 0.40–0.85, p < 0.01, and outside of the previous 12 months OR 0.69, 95% CI 0.48–0.99, p < 0.05; psychotic depression: past 12 months OR 0.28, 95% CI 0.15–0.55, p < 0.001, and outside of the past 12 months OR 0.33, 95% CI 0.17–0.62, p < 0.01; other psychoses: past 12 months OR 0.64, 95% CI 0.42–0.96, p < 0.05).
Compared to the other diagnostic categories, individuals with schizophrenia/schizo-affective disorder were significantly less likely to report (in the past 12 months) a failure to fulfil their role due to alcohol use (bipolar disorder: OR 0.66, 95% CI 0.43–0.99, p < 0.05; psychotic depression: OR 0.37, 95% CI 0.20–0.70, p < 0.01), experience symptoms of alcohol withdrawal (bipolar disorder: OR 0.57, 95% CI 0.36–0.92, p < 0.05; other psychoses: OR 0.42, 95% CI 0.26–0.67, p < 0.05) and suffer physical and mental health problems due to alcohol use (bipolar disorder: OR 0.56, 95% CI 0.35–0.91, p < 0.05; psychotic depression: OR 0.44, 95% CI 0.19–0.97, p < 0.05; other psychoses: OR 0.35, 95% CI 0.22–0.56, p < 0.001).
Consequences of illicit drug use by diagnostic subgroup
Individuals with schizophrenia/schizo-affective disorder were significantly less likely to report experiencing a tolerance to drug use in the past 12 months compared to those with bipolar disorder (OR 0.63, 95% CI 0.43–0.93, p < 0.05) and those with psychotic depression (OR 0.35, 95% CI 0.17–0.72, p < 0.01); however, outside of the previous 12 months they were more likely to report drug tolerance compared to those with other psychoses (OR 1.66, 95% CI 1.11–2.50, p < 0.05). Likewise, individuals with schizophrenia/schizo-affective disorder were significantly more likely to report that drug use interfered with their ability to fulfil their role outside of the previous 12 months, compared to those with other psychoses (OR 1.59, 95% CI 1.08–2.33, p < 0.05). Physical and mental health problems as a result of drug use were significantly less likely to be reported by individuals with schizophrenia/schizo-affective disorder in the previous 12 months compared to those with psychotic depression (OR 0.44, 95% CI 0.22–0.88, p < 0.05), while more likely to be reported by participants with schizophrenia/schizo-affective disorder outside of the previous 12 months compared to those with other psychoses (OR 1.92, 95% CI 1.14–3.23, p < 0.05). Additionally, compared to the other diagnostic categories, individuals with schizophrenia/schizo-affective disorder were significantly more likely to report that others expressed concern about their drug use in both the previous 12 months (other psychoses: OR 1.72, 95% CI 1.10–2.70, p < 0.05) and outside of the previous 12 months (bipolar disorder: OR 1.43, 95% CI 1.00–2.00, p < 0.05; other psychoses: OR 2.00, 95% CI 1.33–3.33, p < 0.01).
Correlates of lifetime alcohol and/or cannabis dependence/abuse
Problematic use (abuse, dependence) of alcohol and cannabis was examined. Half the sample was diagnosed with DSM-IV lifetime alcohol abuse/dependence (50.5%) and/or DSM-IV lifetime cannabis abuse/dependence (50.8%). A third of the sample was diagnosed with DSM-IV lifetime other illicit drug abuse/dependence (31.6%).
No significant group differences were identified in the (lifetime) prevalence of alcohol abuse/dependence. There were, however, significant differences in AUDIT scores across diagnostic groups for schizophrenia/schizo-affective disorder (M = 6.34; SD = 7.30), for bipolar (M = 6.52; SD = 7.81), for psychotic depression (M = 7.86; SD = 9.13) and for other psychoses (M = 7.78; SD = 9.95); Welch’s F(3, 453.54) = 2.70, p < 0.05, with planned contrasts indicating that patients with schizophrenia had significantly lower mean AUDIT scores than the combined bipolar, psychotic depression and other psychoses groups (t = 2.48, p < 0.05). In addition, individuals with schizophrenia/schizo-affective disorder were significantly more likely to be diagnosed with lifetime cannabis abuse/dependence, compared to other psychoses (no significant pairwise differences were noted for bipolar disorder or psychosis with depression) (Table 6).
Correlates of lifetime alcohol and cannabis dependence.
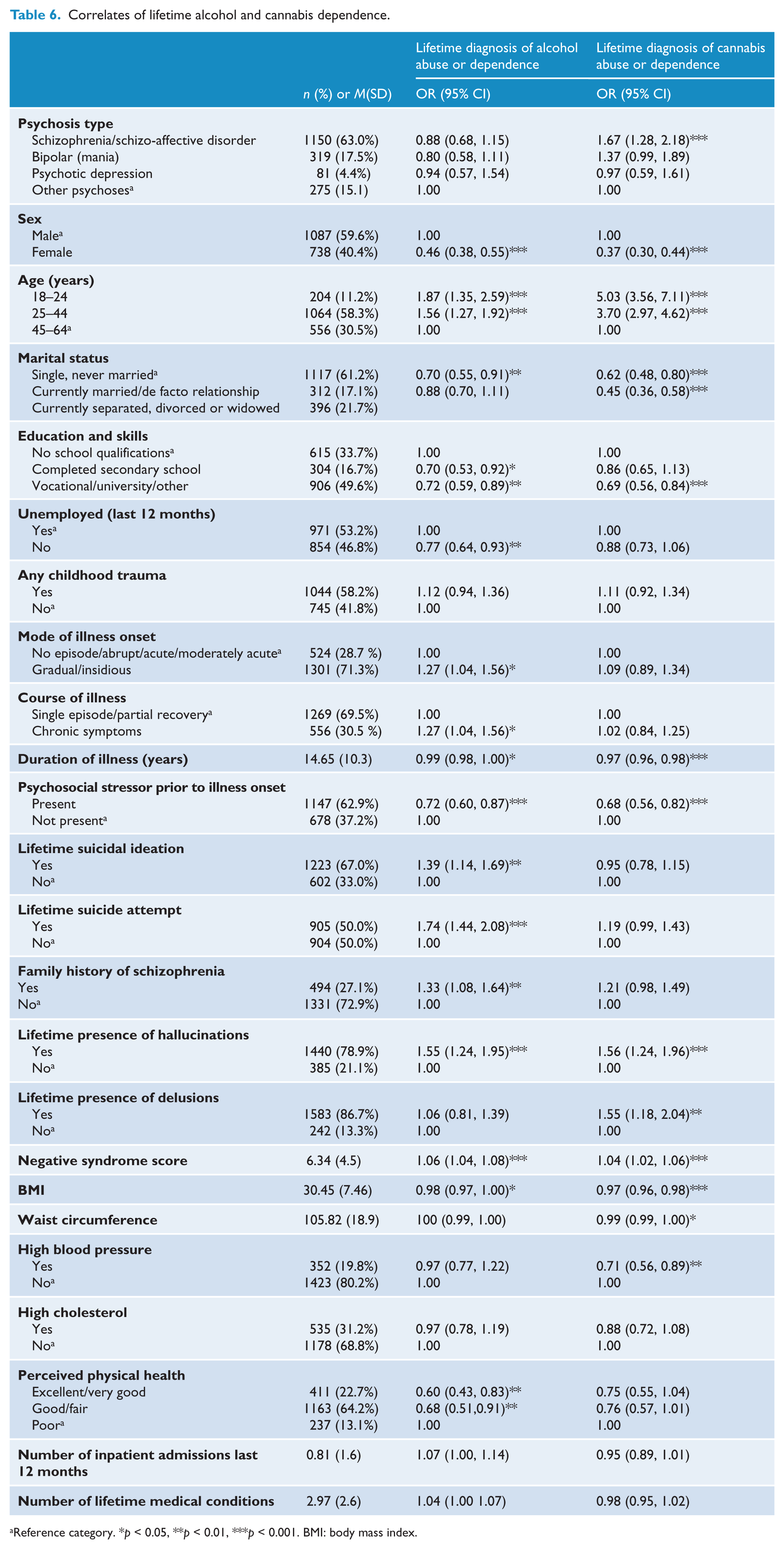
Reference category. *p < 0.05, **p < 0.01, ***p < 0.001. BMI: body mass index.
A number of factors were found to be associated with an increased risk of both lifetime alcohol and cannabis dependence/abuse (Table 6). These are:
male gender;
younger age;
being single (vs currently married/de facto relationship);
no school qualification (vs vocational/university/other qualification);
shorter duration of illness;
not having a psychosocial stressor present prior to illness onset;
lifetime presence of hallucinations;
a higher negative syndrome score; and
lower body mass index (BMI).
A number of other variables were associated with an increased risk of lifetime alcohol dependence/abuse only (Table 6):
unemployed in the previous year;
mode of illness onset (gradual/insidious vs no episode/abrupt/acute);
course of illness (chronic symptoms vs single episode/partial recovery);
lifetime suicidal behaviour (ideation and attempts);
family history of schizophrenia;
reduced quality of life [lower assessment of quality-of-life (aqoL) score]; and
poor perceived physical health (vs excellent/very good and good/fair).
Other factors associated with an increased risk of lifetime cannabis dependence/abuse only (Table 6) were:
no school qualification (vs completed secondary school);
lifetime presence of delusions; and
smaller waist circumference.
Discussion
The current study replicates and extends earlier work to provide up-to-date prevalence estimates of alcohol and illicit drug use among Australians with a psychotic illness. We also conducted disorder-specific comparisons on prevalence (and frequency of use) of alcohol and illicit substances, and examined a wide range of correlates associated with a lifetime diagnosis of substance abuse/dependence.
Alcohol and cannabis use were found to be highly prevalent for the entire sample. In fact, a larger proportion of the sample reported lifetime cannabis use compared to alcohol use (97% vs. 92%). Few significant differences in the prevalence or frequency of use were identified across the diagnostic categories examined. Cannabis was most frequently cited as the primary drug of concern (i.e. the substance which had caused them the most problems) by just fewer than half the sample, followed by alcohol and amphetamines. This finding is consistent with previous research which suggests that, aside from tobacco, cannabis and alcohol are the most frequently and consistently cited substances of concern among individuals with schizophrenia (Blanchard et al., 2000; Koskinen et al., 2009; Koskinen et al., 2010; O’Daly et al., 2005; Regier et al., 1990). International comparisons highlight jurisdictional differences in patterns of substance use, perhaps reflecting the availability of particular drug types (i.e. cocaine is less frequently cited as a drug of concern in Australia compared to North America and Europe) (Fowler et al., 1998; Kavanagh et al., 2004; Talamo et al., 2006). Compared to the other diagnostic groups, individuals with schizophrenia/schizo-affective disorder reported lower levels of tolerance to alcohol despite still experiencing numerous psychosocial problems (e.g. social/legal problems, being unable to recall the previous night due to alcohol use). This is consistent with other research suggesting that alcohol problems among individuals with schizophrenia are less likely to be characterised by a physical dependence, which may suggest an increased sensitivity (or ‘supersensitivity’) to alcohol and other substances (Mueser et al., 1998).
Of interest was the finding that individuals with schizophrenia were more likely to report regular cannabis, stimulant and other illicit drug use in the year prior to illness onset compared to some of the other diagnostic categories. Individuals with schizophrenia were also more likely to report some negative consequences from illicit drug use (at some point in their lives), including experiencing drug tolerance, being unable to fulfil their role due to drug use and experiencing physical or mental health problems as a result of drug use, compared to the other diagnostic categories. Moreover, people with schizophrenia were significantly more likely to be diagnosed with lifetime cannabis dependence. While it is not possible from these findings to draw conclusions regarding any causal associations between drug use and schizophrenia, it does suggest that individuals presenting to treatment services for problems with substance use should be carefully screened for psychosis. It should be noted that high rates of virtually all substance-related adverse consequences were reported by the sample. While experiencing a drug overdose was one of the least commonly reported consequences, it was still reported by a substantial proportion of the sample (24%). The experience of these adverse consequences is likely to have a huge impact on rehabilitation and recovery from psychotic disorders, particularly in individuals with co-morbid SUDs.
Half the sample was diagnosed with either lifetime alcohol abuse/dependence or cannabis abuse/dependence, and a third with lifetime other illicit drug abuse/dependence. While these estimates of co-morbidity (substance use disorder among individuals with schizophrenia) are consistent with other reports from studies conducted both in Australia and internationally (Blanchard et al., 2000; Regier et al., 1990), they are substantially higher than rates identified among the general population (e.g. 25% ‘any substance use disorder’ in the latest Australian National Survey of Mental Health and Wellbeing) (Australian Bureau of Statistics, 2008). Moreover, the estimates of problematic substance use are considerably higher than those reported in the first Australian National Low Prevalence (Psychotic) Disorders Study conducted in 1997–1998 (Kavanagh et al., 2004). Kavanagh et al. (2004) identified lifetime alcohol abuse/dependence for 28% of their sample, lifetime cannabis abuse/dependence for 23% and lifetime other illicit drug abuse/dependence for 12%, compared to 51% (each for alcohol and cannabis) and 32% (other illicit drugs), in the current study. This is a very concerning trend. While it is possible that the increase is due to a cohort effect, other explanations are also possible. A recent Australian general population survey showed illicit drugs were perceived as more easily available and accessible in 2010 compared to 2007, which may, at least in part, help explain the observed increase (Australian Institute of Health and Welfare, 2011). There is also evidence to suggest individuals with psychotic disorders are spending more time in the community with fewer and briefer inpatient hospital stays common, which may allow more time to access alcohol and illicit drugs (SANE Australia, 2002).
In line with previous research, including the earlier Australian National Low Prevalence (Psychotic) Disorders Study, male gender and younger age were strong predictors of both alcohol and cannabis abuse/dependence (Blanchard et al., 2000; Kavanagh et al., 2004). Compared to those aged 44–64 years, individuals aged 18–24 were five times more likely, and those aged 24–44 were over three times more likely, to be diagnosed with lifetime cannabis abuse/dependence.
Consistent with the findings of Kavanagh et al. (2004), course of illness (chronic symptoms vs single episode/partial recovery) was found to be associated with alcohol but not cannabis abuse/dependence. The experience of lifetime hallucinations and a higher negative syndrome score were associated with both alcohol and cannabis abuse/dependence. In addition, a number of other correlates, not assessed in the 1997–1998 survey, were found to be associated with either alcohol abuse/dependence only (including gradual/insidious onset of disorder, lifetime suicidal behaviour, family history of schizophrenia, poorer perceived quality of life, poorer perceived physical health) or cannabis abuse/dependence only (including lifetime delusions and smaller waist circumference). While some of these correlates have been identified in previous research, this study extends our knowledge by examining a wider range of factors not previously assessed within a single sample (Blanchard et al., 2000). It is important to note, however, that many of the measures used were assessing lifetime occurrence and it is therefore not possible to make causal associations with substance misuse.
The finding that individuals with a higher negative syndrome score were more likely to have an alcohol and/or cannabis use disorder is somewhat surprising. A number of other studies of schizophrenia have documented that individuals with pronounced negative symptoms are less likely to have substance use disorders (Kirkpatrick et al., 1996; Mueser et al., 1990; Salyers and Mueser, 2001). It is likely that the diagnostically heterogenous nature of the sample (i.e. the sample consists of individuals with a diagnosis of schizophrenia/schizo-affective disorder, bipolar disorder, psychotic depression or other psychoses) played a role in this unexpected finding. Another way of looking at this, though, is that people tend to use substances to alleviate ‘negative affect’, and this is particularly relevant to people with schizophrenia and related disorders (Spencer et al., 2002).
While the current study is limited in its ability to establish cause and effect between symptoms and substance use, it provides the most up-to-date estimates of alcohol, cannabis and other illicit drug use among individuals with psychotic disorders in Australia. Reliance on self-report in the current study could be identified as a limitation; however, the reliability and validity of self-report among individuals with substance use disorders is well established (Darke, 1998). The study moves beyond previous work by using a large national sample and examining correlates for alcohol and cannabis abuse/dependence separately.
While it was beyond the scope of the current study, future work would benefit from assessing the best predictors of alcohol and/or cannabis abuse/dependence among individuals with psychosis. Overall, the findings suggest the use of alcohol and illicit substance is common among people with a psychotic illness, and is associated with a number of adverse outcomes. Rates of harmful use of these substances seem to be increasing. Future research would benefit from exploring possible socialisation motives for using substances. In addition, clinicians should be aware of the potential impact of concurrent substance use among individuals presenting for treatment for a psychotic illness. In doing so, it is important to explore why individuals with a psychotic illness are using alcohol and illicit drugs (e.g. it may be to counteract the effects of medication, improve negative affect or relieve stress) in determining the most appropriate treatment approach (Spencer et al., 2002). The results also suggest individuals with psychotic disorders may benefit from treatment services which concurrently address co-morbid substance use disorders (Drake et al., 2007; Mueser et al., 2003). More research and investment in new intervention programs is required given that current initiatives appear to be having little success in reducing consumption. In fact, recent research suggests that public health initiatives aimed at the general population to reduce tobacco smoking are ineffective among those with psychotic disorders (Thornton et al., 2011). There is a need for more research to examine if this is also occurring for alcohol and other illicit drugs, and if so, strategies specifically targeting people with serious mental illness are needed.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V Morgan (National Project Director), A Jablensky (Chief Scientific Advisor), A Waterreus (National Project Coordinator), R Bush, V Carr, D Castle, M Cohen, C Galletly, C Harvey, B Hocking, A Mackinnon, P McGorry, J McGrath, A Neil, S Saw, H Stain.
The authors would like to thank Professor Vaughan Carr, Professor John McGrath and Professor Andrew Mackinnon for providing comments on earlier drafts. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
The study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.