
Abstract
Background:
Suicide rates are higher in rural compared to urban areas. Although this pattern appears to be driven by higher rates among men, there is limited evidence about the characteristics of rural people who die by suicide in Canada. The objective of this study was to examine the demographics, manner of death, and social and clinical antecedents of people who died by suicide in rural areas compared to urban areas.
Methods:
We conducted an observational study of all suicide deaths that occurred among Newfoundland and Labrador residents between 1997 and 2016 using a linked data set derived from a comprehensive review of provincial medical examiner records. We used t tests and χ2 to assess associations between rural/urban status and variables related to demographics, circumstances, and manner of death, as well as social and medical history. Logistic regression was utilized to assess the independent contribution of any variable found to be significant in univariate analysis.
Results:
Rural people who died by suicide accounted for 54.8% of all deaths over a 20-year period. Overall, 81.6% of people who died were male. Compared to urban, rural people who died by suicide were younger, more likely to use firearms or hanging, and had a higher mean blood alcohol content at the time of death (27.69 vs. 22.95 mmol/L). Rural people were also less likely to have had a known history of a prior suicide attempt, psychiatric disorder, alcohol or substance abuse, or chronic pain.
Discussion:
The demographic and clinical differences between rural and urban people who died by suicide underscore the need for suicide prevention approaches that account for place-based differences. A key challenge for suicide prevention in rural communities is to ensure that interventions are developed and implemented in a manner that fits local contexts.
Introduction
The suicide rate in Canada declined by 24% between 1981 and 2017, 1 though there are still nearly 4,000 suicide deaths each year. 1,2 In Canada and other high-income countries, suicide mortality varies geographically, 3,4 often with higher rates in rural areas compared to cities, 5 –8 especially among males. 5 Risk factors for suicide among rural populations include social isolation, limited access to mental health services, and stigma-related to mental illness. 6,9,10 Globally, access to firearms and agricultural pesticides in rural areas also appear to be factors. 7,11
Previous research on rural suicide in Canada used administrative data 12 –15 such as vital statistics, with limited record-level information about demographic or clinical characteristics. Coroner and medical examiner data can provide an in-depth understanding of the characteristics of people who have died by suicide. Previous Canadian studies with coroner and medical examiner data identified mental illness and problematic alcohol use as common antecedents to suicide 16 –19 and identified elevated risks in specific subpopulations including youth, 20 seniors, 8,21 and Indigenous peoples. 22 –24 However, the majority of these studies focused on cities 16,18 or entire provinces, 25,26 with limited attention to rurality. 17,22
Methodologically, studies utilizing coroner or medical examiner data have also faced challenges related to the brevity of the study period 16,19,25,26 and small sample size. 19,25,26 Our aim was to overcome some of these limitations by using a provincial data set from Newfoundland and Labrador that includes all suicide deaths that occurred over 2 decades.
Historically, Newfoundland and Labrador has had one of the lowest suicide rates in the country. 27 However, since 2000, the rate increased from 8.8 to 12.2 suicide deaths per 100,000 people. 28 Although rural and urban differences in the province have not been examined, a previous study found that there was a 4-fold rate disparity between Labrador, the most rural region of the province, and the island of Newfoundland, which includes the capital city. 29 The objective of the present study was to examine the demographics, circumstances and manner of death, and social and clinical characteristics of people who died by suicide in rural areas compared to urban areas. This was an effort to strengthen contextual knowledge about place-based risks and inform suicide prevention policy.
Methods
Study Design
We conducted a population-based, observational study to examine the characteristics of people who died by suicide in rural areas compared to urban areas between 1997 and 2016. This study was approved by the provincial Health Research Ethics Board (#2018.125). Results are reported based on the Reporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines. 30
Setting
This study was conducted in Newfoundland and Labrador, the eastern-most province in Canada. Newfoundland and Labrador has a large geographic area (370,514 km2) with a relatively small population (519,716 in 2016) of which 39.6% (205,955) reside in or near the provincial capital, St. John’s. 31 The province has a proportionately large rural population (∼60%) with communities ranging in size from remote, fly- or boat-in only communities of a few hundred people up to larger, regional centers such as Gander (11,668 pop.) and Corner Brook (19,806 pop.). 31
Data Source
The primary data source for this study was the Suicide Database developed by the Newfoundland and Labrador Centre for Health Information (NLCHI). 19 This database contains records of all confirmed suicide deaths that occurred in the province between 1997 and 2016. Under the provincial Fatalities Investigations Act, the Chief Medical Examiner is responsible for investigating all unexpected, unexplained, and nonnatural deaths to make a final determination of cause and manner of death. Investigative procedures include physical exam and autopsy, toxicological testing, interviews with key informants and witnesses, and reviews of medical, police, or other pertinent administrative records. In rural areas, the Office of the Chief Medical Examiner (OCME) delegates some responsibilities to family physicians and police and coordinates investigations remotely.
NLCHI epidemiologists use a standardized data collection procedure to conduct annual file reviews of all suicide deaths investigated by the medical examiner. 19 The data set is then cleaned and linked with the Annual Mortality Files provided by Vital Statistics, NLCHI’s Client Registry, and the Postal Code Conversion File to allow for integration with other demographic and clinical data. The database is available for surveillance and research purposes following institutional approval from NLCHI.
Rural/Urban Status
For the purpose of our analysis, a variable for rural/urban status was derived from the first three characters of the Canadian postal code, the Forward Sortation Area (FSA), based on the last known address of residence for each individual. The second character in the FSA designates an area as rural (0) or urban (1 to 9). This definition classifies regional population centers outside metropolitan areas as urban and has been used in other studies on rural health. 32 –34 Previous studies have shown that outcomes vary depending on the definition of rurality that is used. 34 Therefore, we included a sensitivity analysis with an alternative definition of rural based on the Statistical Area Classification (SAC). 14,15 For this broader definition, rural was defined as any community of residence in a census subdivision outside of the St. John’s metropolitan area (Online Supplement 1). 35
Variables
We obtained data on all suicide deaths that occurred between January 1, 1997, and December 31, 2016. This was the largest period of data available. The following variables were included:
Demographics: sex (female/male), age at time of death, marital status (married/not married), living arrangement (living alone/living with someone), employment status (student, employed, unemployed, and retired), and education level (less than high school/high school or more);
Circumstances related to the manner of death: suicide note (yes/no), suicide method (self-poisoning, firearms, hanging, strangulation, or suffocation, cutting and piercing, drowning, self-poisoning by carbon monoxide, jumping from a high place, and all other methods), blood alcohol content (BAC; mmol/L), and legally intoxicated (yes/no based on threshold of 17.36 mmol/L);
Social history, including stressors present at time of death (yes/no): recent heavy drinking, financial problems, trouble with the law, marital/relationship problems, interpersonal conflict, history of gambling, and family history of suicide loss; and
Clinical characteristics (yes/no): past suicidal thoughts, past suicide attempt, history of mental illness, history of alcohol abuse, history of substance abuse (prescription drugs, illicit drugs, or nonillicit drugs), psychiatric drugs in the chart at the time of death, history of a chronic disease, and history of pain.
Similar to other studies with comparable data, 18,36 variables related to social and clinical characteristics were included in the medical examiner records and subsequently in the NLCHI Suicide Database if they were known to be present. That is, they were coded as “yes, present” if there was confirmation from any investigative materials that the individual had previous experience or exposure to the factor. In some instances, the medical examiner specified that a factor was not present, such as for past suicide attempts. For example, the medical examiner report may have indicated that “there was no known history of suicide attempt(s) by the deceased.” However, the absence of a factor was often not recorded by the medical examiner and therefore was coded as “missing” or “unknown” in the NLCHI Suicide Database. In cases where a response of no or unknown/missing both denoted the absence of a condition or factor, these categories were combined. As a result, estimates of the prevalence of social and clinical factors are likely to be underestimates.
Analysis
Descriptive and comparative analyses were performed using SPSS Version 21.0. Frequency analyses were used to provide a general description of the data; t tests were used to compare continuous variables (age, blood alcohol level), and χ2 tests were used to assess associations between rural/urban status and all demographic, manner of death, social, and clinical categorical variables. We used a P value threshold of 0.05 to determine overall statistical significance. Post hoc differences were assessed via inspection of standardized residuals. The Bonferroni adjustment was also used, where applicable. 37 Logistic regression was utilized to assess the independent contribution of any variable found to be significant in univariate analysis.
Results
We identified 972 suicide deaths among the residents of Newfoundland and Labrador between 1997 and 2016. Data on rural/urban status were available for 919 (94.5%) decedents. Based on the FSA definition, 504 (54.8%) people who died by suicide were from rural areas of the province and 415 (45.2%) were from urban areas. A majority (81.2%) were male, and the mean age of decedents, regardless of sex, was 42.6 years.
The demographic characteristics of rural and urban people who died by suicide are shown in Table 1. Overall, a larger proportion of people who died were male; however, the percentage was greater in rural areas than in urban areas. On average, people from rural areas were younger (M = 41.29, SD = 17.82) than those from urban areas (M = 44.20, SD = 15.37). There was a significant association between age-group and rural/urban status, with a higher proportion of people from rural areas aged 10 to 19 years old. No significant association was found between rural/urban status and marital status, though people from rural areas were less likely to live alone. There was a significant association between rural/urban status and both employment and education (Table 1). With the exception of differences in the average age, the analysis based on the SAC definition of rurality yielded similar results (Online Supplemental Table 1).
Demographic Characteristics of Rural and Urban People Who Died by Suicide in Newfoundland and Labrador, 1997 to 2016.
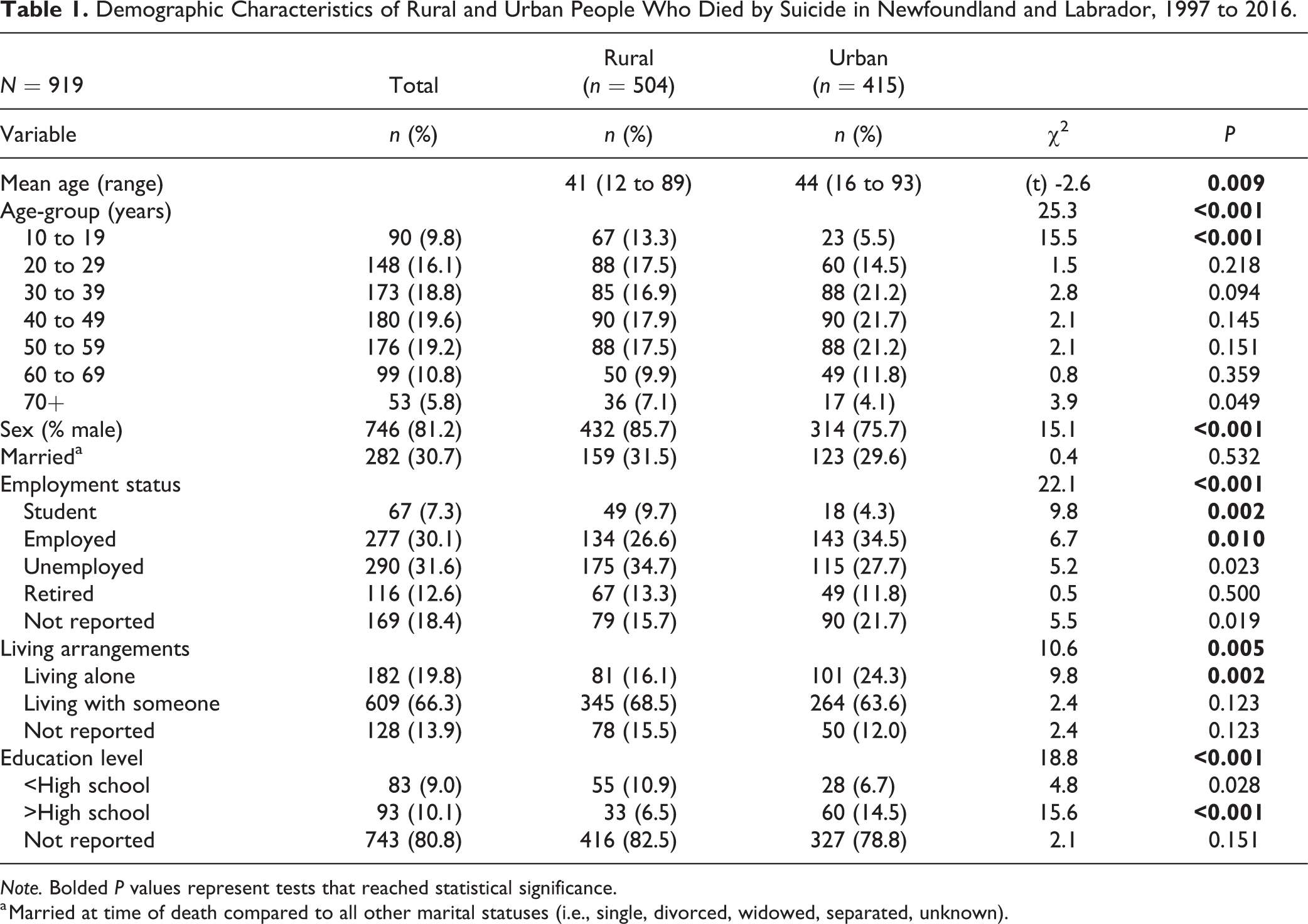
Note. Bolded P values represent tests that reached statistical significance.
a Married at time of death compared to all other marital statuses (i.e., single, divorced, widowed, separated, unknown).
Table 2 includes a summary of suicide methods and other characteristics related to the circumstances of death. There was a significant association between suicide method and rural/urban status: A greater proportion of people from urban areas died from self-poisoning compared to rural areas, whereas firearms and hanging were more common among people from rural areas. An alcohol toxicology screen was completed for a total of 734 (79.9%) people who died by suicide, with varying levels of alcohol detected in 345 (47.0%) cases. Among people who died with alcohol in their system, the average BAC was significantly higher among people from rural areas (M = 27.69 mmol/L, SD = 21.34) compared to those from urban areas (M = 22.95 mmol/L, SD = 18.60; t = 2.16, df = 343, P = 0.031). Based on the SAC definition, we detected slight but statistically significant changes in rural/urban differences related to suicide method, BAC, and the presence of a suicide note (Online Supplemental Table 2).
Circumstances and Manner of Death among Rural and Urban People Who Died by Suicide in Newfoundland and Labrador, 1997 to 2016.
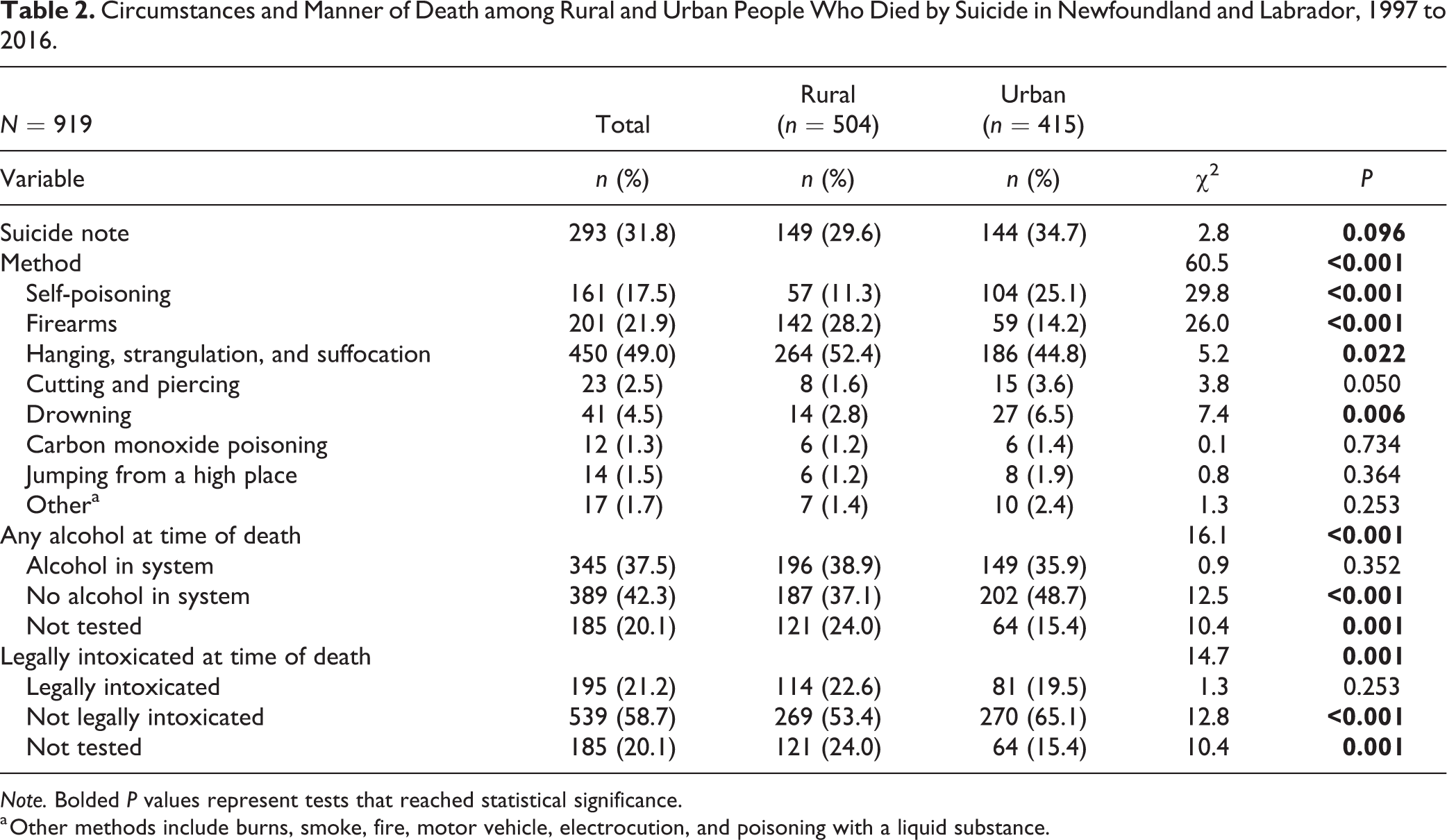
Note. Bolded P values represent tests that reached statistical significance.
a Other methods include burns, smoke, fire, motor vehicle, electrocution, and poisoning with a liquid substance.
The social and clinical characteristics of rural and urban people who died by suicide are shown in Table 3. People from rural areas were significantly more likely to have engaged in recent heavy drinking compared to those from urban areas, though they were less likely to have had recent financial problems or a recent history of gambling. There were no significant differences in other social factors (Table 3).
Social and Clinical Characteristics of Rural and Urban People Who Died by Suicide in Newfoundland and Labrador, 1997 to 2016.
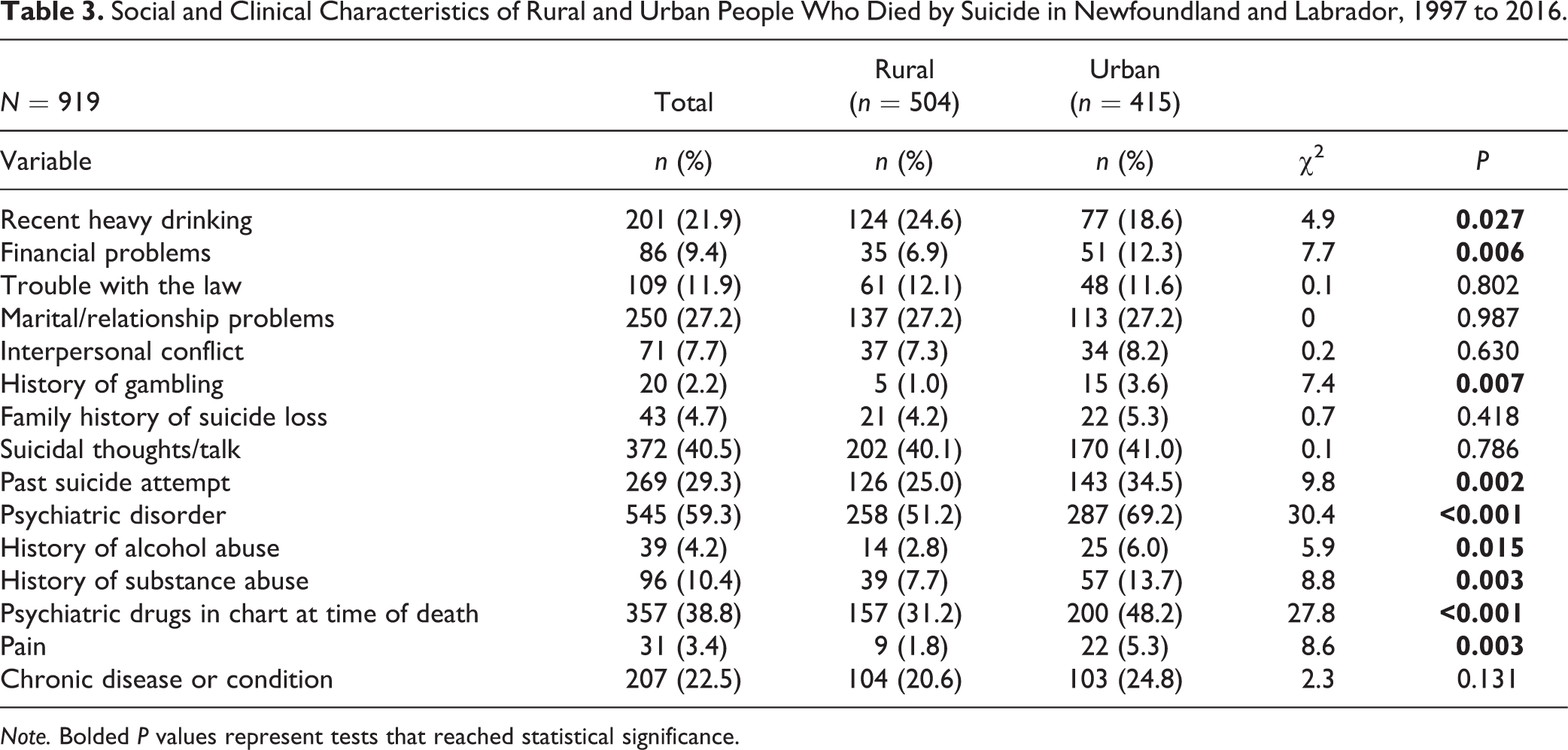
Note. Bolded P values represent tests that reached statistical significance.
There were some significant differences in clinical factors. People from rural areas who died by suicide were significantly less likely to have a known history of previous suicide attempts, a psychiatric disorder or treatment with psychiatric medication, alcohol or prescription drug abuse, or chronic pain. There were no significant differences with other clinical variables. Overall, many social and clinical factors appeared to be significantly less prevalent among rural people who died by suicide. Recent heavy drinking was no longer significant when the alternative definition of rurality was utilized; all other differences remained significant (Online Supplemental Table 3). Based on the logistic regression, employment, method (firearm and self-poisoning), and history of gambling made significant independent contributions (Table 4). Similar results were found for the SAC definition of rural/urban (Online Supplemental Table 4).
Regression Model of Demographic Predictors of Suicide Death among Rural and Urban People in Newfoundland and Labrador, 1997 to 2016.
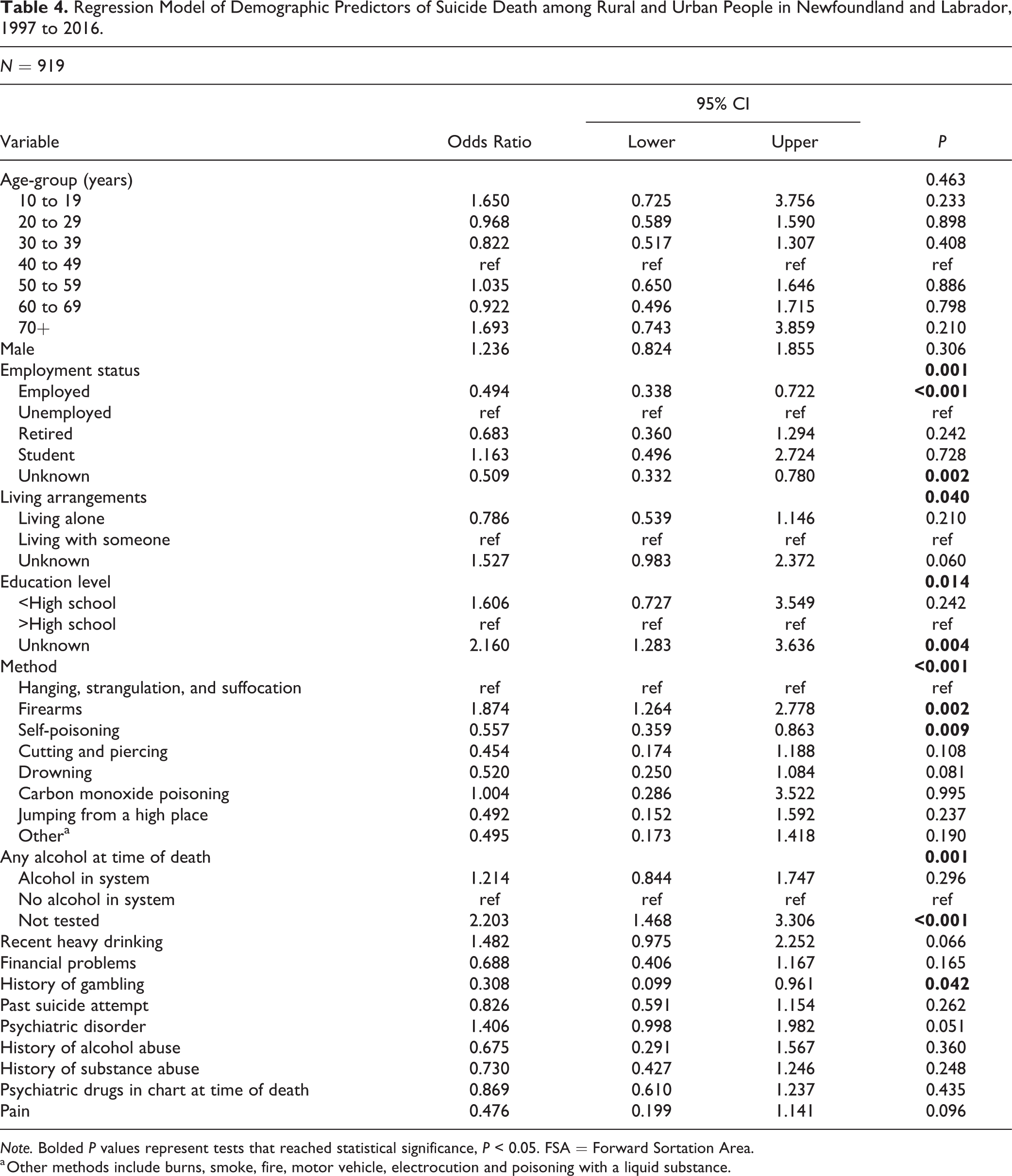
Note. Bolded P values represent tests that reached statistical significance, P < 0.05. FSA = Forward Sortation Area.
a Other methods include burns, smoke, fire, motor vehicle, electrocution and poisoning with a liquid substance.
Discussion
This study identified differences between rural and urban people who died by suicide in a Canadian province with a proportionately large rural population. Similar to studies in other high-income countries, 3,6,7 males accounted for the majority of suicide deaths. Rural people who died by suicide were younger, more likely to be students or unemployed, had less education, and were more likely to be living with someone at the time of their death. Rural people were also more likely to use firearms or hanging and less likely to use poison than those from urban areas, as was found in a recent systematic review. 6 Rural people were also less likely to have a known history of prior suicide attempt, mental illness, alcohol or substance abuse, treatment with psychiatric medication, or chronic pain. However, some variations were evident when an alternative definition of rurality was used. Broadly, our results align with previous reviews 6,9 and studies of rural suicide in high-income countries. 7,38
Our finding that rural males accounted for 47% of all suicide deaths in Newfoundland and Labrador is likely related to a combination of factors that are specific to rural communities. Rural communities have poorer access to mental health services, and rural men in particular are less likely to seek professional help or social support for mental health problems. 38,39 Qualitative research has shown that not seeking treatment for depression and suicidality is influenced by conceptions of rural masculinity that value stoicism and silence in response to distress. 39 Rural health systems may be able to offset barriers in local access to mental health services by scaling up telepsychiatry, which has been shown to be feasible, acceptable, and effective, 40 though is underused in some areas. 41 The acceleration of digital mental health interventions during the COVID-19 pandemic 42 may also provide new opportunities for reaching rural men where in-person services have been ineffective or in short supply. Increasing access to virtual care, especially for rural men, may be complemented by public messaging about treating depression and destigmatizing mental health care. 43 –45
Suicidality among rural men may also be related to occupational and economic factors. Men from rural communities in Newfoundland and Labrador often work in industries with the highest suicide rates such as agriculture, resource extraction, and construction. 46,47 The “fly-in, fly-out” workforce model that is present in some of these industries may also contribute to increased psychosocial stresses 48,49 and risks for mental illness 50 that disproportionately impact rural workers. Suicide risks associated with economic recession, job insecurity, and unemployment may also have a differential impact on rural men.
Rural men may also face elevated risks due to exposure to environmental factors. This includes extreme weather events and unpredictable climatic conditions, which may have disruptive impacts on men in farming 51,52 or Indigenous communities. 53 Examining sex differences and sex-specific characteristics of rural people who die by suicide may help to identify opportunities for interventions that address differential risks.
Suicide method was another factor that distinguished rural and urban populations in our study. Hanging accounted for nearly half of all deaths, as is the case nationally, 2 though the proportion in rural communities in Newfoundland and Labrador was higher than that observed in urban areas. A recent study from Ontario found marked disparities in firearm-related injuries between rural and urban areas. 54 Although we could not discern the types of guns used in firearm-related suicides, the elevated prevalence of firearm deaths among rural people who died compared to urban people (28.2% vs. 14.2%) is similar, though not as prominent, as the pattern in the United States. 5,7
Rural–urban differences in firearm use are likely related to several factors. Hunting is a key aspect of food security in rural areas, 55,56 and household firearm ownership is common in many rural communities. 8,57 Access to guns and unsafe storage practices increase risk of suicide 58,59 and may partially explain geographic differences in firearm-related mortality.
Access to an emergency department and trauma care may also be a factor in the higher proportions of firearm and hanging-related suicide deaths in rural areas. People who attempt suicide in rural communities may be more likely to die from their injuries than those in cities because it takes longer to be transported to the emergency department. Indeed, a higher proportion of trauma deaths occur prehospital in rural compared to urban settings, and excess deaths may be related to delays in prehospital care. 60 A recent study found that 92% of suicide deaths occurred on site before medical personnel arrived, and 68% of suicide deaths occurred within an hour of the attempt. 61 Examining the role of prehospital trauma care following a suicide attempt in rural settings is a valuable direction for future research.
This is one of the few Canadian studies to examine the social and clinical characteristics of rural people who died by suicide. 6,22,24 The prevalence of most factors was either lower for people in rural areas or equivalent, with the exception of recent alcohol use and blood alcohol level at time of death, which were higher in rural areas. Alcohol is a known risk factor for suicide at both the population and individual level. 62 Among adolescents, alcohol consumption tends to be higher in rural areas, 63,64 and heavy drinking is more common among men and in rural communities. 65 Geographic patterns in alcohol use may have a role in the distribution of risk for suicide, especially in Newfoundland and Labrador where rates of heavy and risky drinking are elevated. 66 Alcohol may also be an upstream risk factor for suicide through prenatal exposure.
Fetal alcohol spectrum disorder (FASD) has an estimated prevalence of between 1% and 5% 67,68 and may be higher in rural areas. 69,70 There is a high burden of mental illness among people with FASD, 71 and adolescents in particular have higher rates of suicidal thoughts and attempts than the general population 72 and a higher rate of suicide than those without FASD. 73 FASD is not routinely documented in medical examiner reports and therefore was not available in the data set we used. However, it is possible that a higher incidence of FASD in rural areas may be part of the constellation of risk for suicide.
Suicide Prevention in Rural Communities
Although our study found that there were many similarities between rural and urban people who died by suicide, the differences between these groups underscore the need for clinical and population-based approaches to suicide prevention that account for place-based differences. 74 Given the prominence of firearms as a prevalent suicide method in rural communities, there may be value in developing interventions to promote the safe storage of guns, 10,75 –77 especially when people with access are in distress or at elevated risk. Rural “means safety” 77 initiatives would be complemented by community-based interventions 43 and clinical care focused on problematic alcohol use and engaging at-risk men in follow-up care. A key challenge for suicide prevention in rural communities is to ensure that interventions are developed and implemented in a manner that fits local contexts. 74 Mixed methods research may be particularly useful in understanding the social and cultural factors that influence the relationships between gender, suicide methods, and alcohol in rural communities.
Indigenous communities in Canada and globally have experienced persistent disparities in suicide rates, 78 including those in rural areas of Newfoundland and Labrador. 29 Consequently, many communities have prioritized prevention and developed innovative approaches to promoting mental health. 79 –81 A foundation of many of these interventions is that they reflect local culture and way of life and are designed by local stakeholders around community assets. These types of community-led approaches to suicide prevention may help to target specific subgroups and risk factors that are prominent in rural settings.
Limitations
This study had several limitations due to its descriptive nature and the use of secondary data. Although we examined a relatively large data set over a 20-year period, the study was cross-sectional. While we were able to identify social and clinical differences between geographic contexts, the lack of a control group comprised of people who did not die by suicide meant we could not discern the extent to which social and clinical factors contributed to suicide risks. This challenge was compounded by threats to the quality and accuracy of the data that may have occurred because of inconsistencies in variable definitions and data collection procedures over time.
Relatedly, for some variables, a larger proportion of unknowns were recorded for decedents from rural areas versus urban areas, which raises questions about systematic differences in data collection process and documentation practices. As such, the prevalence of factors related to social and clinical history should be considered underestimates. 36 To strengthen the quality, reliability, and comprehensiveness of data on suicide, additional sources and collection strategies could be used including record linkage, comprehensive medical chart reviews, or surveys of primary care physicians. 82,83
The results may have also been impacted by our definitions of rural. 84 The definition based on FSA treated regional population centers as urban; conversely, the SAC definition included them as rural. The sensitivity analysis revealed some differences between these definitions. Analyses with granular categories that represent rurality along a continuum may add additional insight into differences in suicide mortality between rural areas of varied size and in comparison to urban areas.
Conclusion
This study identified important differences between rural and urban people who died by suicide. These results highlight an urgent need for suicide prevention efforts to focus on specific rural populations such as younger and working-age men. Public health and clinical interventions need to account for place-based differences in both community strengths and suicide risks. To do so, rural stakeholders need to be collaborators in the planning, design, and implementation of interventions 74 and must have a role in “rural proofing” 85 evidence-based preventative strategies. Achieving a nuanced and effective approach to rural suicide prevention will also be determined by the extent to which resources are distributed equitably to the communities that are most impacted by suicide.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743721990315 - Rural–Urban Differences in Suicide Mortality: An Observational Study in Newfoundland and Labrador, Canada: Différences de la Mortalité Par Suicide en Milieu Rural-Urbain: Une Étude Observationnelle à Terre-Neuve et Labrador, Canada
Supplemental Material, sj-docx-1-cpa-10.1177_0706743721990315 for Rural–Urban Differences in Suicide Mortality: An Observational Study in Newfoundland and Labrador, Canada: Différences de la Mortalité Par Suicide en Milieu Rural-Urbain: Une Étude Observationnelle à Terre-Neuve et Labrador, Canada by Charlene Reccord, Nicole Power, Keeley Hatfield, Yordan Karaivanov, Shree Mulay, Margo Wilson and Nathaniel Pollock in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The Suicide Database is available from the Newfoundland and Labrador Centre for Health Information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Newfoundland and Labrador Support Unit for People and Patient-Oriented Research and Trials (NL SUPPORT). Administrative support was provided by Eastern Health and Memorial University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.