
Abstract
Objective
Individuals with mental illness and addiction are overrepresented in prisons. Few studies have assessed mental health and addiction (MHA)-related service use among individuals experiencing incarceration using health administrative data and most focus on service use after prison release. The objective of this study was to determine the prevalence of MHA-related service use in the 5 years prior to and during incarceration.
Methods
We used linked correctional and administrative health data for people released from Ontario provincial jails in 2010. MHA-related service use in the 5 years prior to the index incarceration was categorized hierarchically into four mutually exclusive categories based on the type of service use: psychiatric hospitalization, MHA-related emergency department (ED) visit, MHA-related outpatient visit (from psychiatrist or primary care physician), and no MHA-related service use. Demographic, diagnostic, and incarceration characteristics were compared across the four service use categories. MHA-related service use during the index incarceration was assessed by category and length of incarceration.
Results
A total of 48,917 individuals were included. Prior to incarceration, 6,116 (12.5%) had a psychiatric hospitalization, 8,837 (18.1%) had an MHA-related ED visit, and 15,866 (32.4%) had an MHA-related outpatient visit. Of the individuals with any MHA-related service prior to incarceration, 60.4% did not receive outpatient care from a psychiatrist prior to incarceration and 65.6% did not receive MHA-related care during incarceration.
Conclusion
Despite a high prevalence of mental illness and addiction among people experiencing incarceration, access to and use of MHA-related care prior to and during incarceration is poor. Increasing the accessibility and use of MHA-related services throughout the criminal justice pathway is warranted.
Introduction
The prevalence of mental illness and substance use disorder (SUD) is higher among individuals experiencing incarceration than the general population.1–3 In Canada, the lifetime prevalence of mental illness, including SUDs, is 2-3 times higher in provincial and federal prisons than in community samples,4,5 and analogous data has emerged from countries around the world.3,6
The overrepresentation of individuals with SUD and mental illness in prison systems is a complex issue shaped by a variety of factors that intersect with mental illness, including lower socioeconomic status, homelessness, stigmatization, and the criminalization of mental illness, an issue that became more pronounced following efforts to deinstitutionalize individuals with psychiatric disorders.3,7,8 The presence of a SUD, mental illness, or a combination of the two (“dual diagnosis”) increases the likelihood of arrest,9–11 increases the risk of negative outcomes during incarceration, 3 and increases the risk of post-release morbidity, mortality, and recidivism.12–14 For example, in the United States (US), a history of alcohol or drug use disorder nearly triples the odds of incarceration, 10 and, in Ontario, individuals with schizophrenia are 40% more likely to be reincarcerated in the 5 years following prison release than individuals without schizophrenia. 15 Inadequate community-based mental health care, limited access to psychiatric hospital beds, and a fragmented health care system in which marginalized populations often fall through the cracks are proposed factors contributing to the overrepresentation of people with mental illness in the Canadian criminal justice system. 8
Given the disproportionate burden of mental illness and SUD and poor health and social outcomes experienced by justice-involved people, improving mental health and addiction (MHA) services for this population is important. It is also a topic that has received recent attention due, in part, to the high rates of suicide and self-harm in prison populations and individuals being injured or killed during police interventions for mental health crises.16–19 Despite the need to improve MHA-related care for this population, patterns of MHA-related health service usage before, during, and after incarceration are not fully understood, and previous studies on this topic (described in detail in the “Discussion” section) are limited by small sample sizes, cohorts restricted to specific demographic or clinical subgroups, data that are more than 15-20 years old, and a reliance on self-reported MHA service use.17,20–22
Recent studies have addressed these limitations by linking data from large cohorts of incarcerated individuals to health administrative records, garnering important insights into the patterns of MHA-related health service use in prison populations.22–28 For example, Al-Rousan et al. 27 linked correctional and health administrative data to determine the prevalence of in-prison service use for mental illness (47.7%), serious mental illness (28.6%), and SUDs (26.1%) among individuals in state prisons in Iowa. Importantly, however, these studies have focused on service use during incarceration and post-release,22,23,25–27 and, to date, none have investigated MHA-related service use prior to incarceration using linked correctional and administrative health data. To address this gap in knowledge, the objective of this study was to characterize MHA-related service use in the 5 years prior to and during incarceration among people who were incarcerated in provincial jails in Ontario, Canada.
Methods
Study Setting and Design
The Ontario provincial jail system is responsible for the detention of all persons on remand (e.g., awaiting trial), and the incarceration of persons serving custodial sentences of <2 years duration. In this paper, we use the term “provincial jails” to represent all provincial correctional facilities, including jails, detention centres, and correctional centres. Ontario has a publicly funded universal health care system that is accessed by virtually all residents, including individuals in provincial jails, which provides a unique opportunity to link administrative provincial health and correctional data to assess MHA-related service use among people who experience incarceration.
In provincial jails, a nurse conducts an initial assessment at the time of admission to custody and will liaise with physicians or nurse practitioners to initiate medications prescribed in the community based on their assessment. Patients routinely see a physician or nurse practitioner within weeks of admission. Based on the initial assessment or subsequent interactions, patients may have care and services arranged sooner if indicated, which may include seeing a nurse, family physician, psychiatrist, psychologist, or social worker within the prison, or transfer to a hospital or emergency department (ED) for emergent issues. Ongoing care is typically provided based on patient needs and may include discharge planning to support continuity of medical care.
Population
Individuals released from Ontario provincial jails from January 1, 2010, to December 31, 2010, served as the study population, based on the available data.28,29 Exclusion criteria included individuals aged <18 or >105 years at the time of release from the index incarceration, individuals whose data could not be linked to a valid identifier in the administrative data, 28 individuals missing information on place of residence, individuals who were not Ontario residents for the 5-year time period prior to the admission date of the index incarceration, and individuals who died while incarcerated, were transferred to a federal prison or were deported. For individuals who had multiple incarceration releases in 2010, only the first episode was kept.
Data Sources
For this study, a 5-year look-back period for health service use commenced from the admission date of the index incarceration. The Ministry of the Solicitor General (MSG) provided sociodemographic data including age, sex, and dates of admission and release from provincial custody for the 5-year period prior to index incarceration. Research Ethics Board approval for the use of corrections data was obtained from the Hamilton Integrated Research Ethics Board (REB #4575). MSG data was linked with administrative health data at ICES, Ontario's largest health data repository, using valid ICES Key Numbers, unique identifiers that represent encoded Ontario Health Insurance Plan (OHIP) numbers. ICES is an independent, non-profit research institute whose legal status under Ontario's health information privacy law allows it to collect and analyse health care and demographic data, without consent, for health system evaluation and improvement. The use of ICES data in this project was authorized under section 45 of Ontario's Personal Health Information Protection Act. The linkage rate between MSG and ICES data was 97.5%. ICES datasets provided clinical and demographic data including hospital admissions and discharges, length of stay, ED registrations, and physician outpatient visits, as well as population and demographic data, including date of birth, sex, address, date of death, rurality, income quintile, and OHIP eligibility and status changes. The specific ICES databases used to access this data are outlined in Supplemental Table 1.
Exposure Variable
We used a previously described psychiatric utilization gradient based on MHA service use in the 5 years prior to the index incarceration to create four mutually exclusive categories. 30 The categories were created hierarchically based on whether individuals had a psychiatric hospitalization, an MHA-related ED visit, an MHA-related outpatient visit, or no prior MHA-related service use in the 5 years prior to the index incarceration. Individuals were placed in the hospitalization category if they had at least one psychiatric hospitalization, in the ED visit category if they had no prior psychiatric hospitalization but had at least one MHA-related ED visit, and in the outpatient category if they had no prior psychiatric hospitalizations or ED visits, and had at least one MHA-related outpatient visit in the 5 years prior to the index incarceration. All others, that is, those who had no MHA-related service use in the 5 years prior to the index incarceration, were placed in the “no MHA-related service use” category.
Characteristics
Sociodemographic characteristics included age, sex, neighbourhood income quintile, and urban/rural residence. 31 Rurality was defined using the Rurality Index of Ontario (RIO2008) score, areas that scored 40 or more were considered rural. 32 Variables describing provincial jail involvement, including index incarceration duration, cumulative length of time in custody, and number of incarceration episodes in the 5 years prior to the index incarceration, were obtained from the dataset provided by the MSG.
For each of the MHA-related service use exposure categories (hospitalizations, ED visits, and outpatient visits), we determined the diagnostic category for the service use based on the diagnosis associated with the most recent MHA-related service use event. For hospitalizations and ED visits, the diagnosis is recorded using the International Classification of Disease (ICD)-10 with precise decimal specifiers, whereas outpatient diagnoses rely on ICD-9 and do not have decimal points. Therefore, the diagnostic categories differed for hospitalizations and ED visits compared to outpatient visits. The ICD-9 and ICD-10 codes used to identify particular MHA-related outpatient and hospitalization/ED visit diagnostic categories are detailed in Supplemental Table 2. For outpatient visits both prior to and during incarceration, individuals were hierarchically assigned to diagnostic categories in the following order: (1) psychotic disorders (e.g., schizophrenia), (2) non-psychotic disorders (e.g., personality disorders and depressive disorders), (3) substance-related disorders, (4) social disorders (e.g., social adjustment problems), and (5) other disorders (e.g., substance-related psychosis and child and adolescent behavioral disorders).
We also measured the number of MHA-related primary care physician (PCP) visits and outpatient psychiatrist visits in the 5 years prior to incarceration, including PCP visits by diagnostic group (non-psychotic disorders, psychotic disorders, and substance-related disorders). Visits to PCPs were categorized as mental health-related and non-mental health-related visits based on a validated algorithm. 33 Finally, for each service use exposure category, we measured MHA-related service use during the index incarceration, including hospitalizations, ED visits, and outpatient service use, both overall and stratified by the duration of the index incarceration. The duration categories were created based on the skewed distribution of incarceration duration in the sample.
Statistical Analysis
Health service use encounters were calculated in the 5-year period before the entry date of the index incarceration and during the index incarceration. The number and duration of incarceration episodes in the 5 years prior to the entry date of the index incarceration were also calculated. Descriptive data were summarized using frequencies and proportions for categorical data and using mean (standard deviation) or median (interquartile range [IQR]) for continuous data depending on the distribution (normal vs. skewed). Differences between groups were assessed using chi-square tests for independence (categorical variables) and analysis of variance (continuous variables). All analyses were performed in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). 34
Results
Characteristics of the Study Population
In 2010, 54,772 individuals ≥18 years old accounted for 71,295 incarceration releases in Ontario. There were 16,523 (23.2%) individuals who had multiple releases in 2010, and only the first incarceration was kept. The following individuals were excluded: 2,741 (3.8%) were transferred to federal prisons, 1,751 (2.5%) individuals had a missing health card number, 1,350 (1.9%) were deported out of Canada, 7 (<0.1%) died during incarceration, and 6 (<0.1%) individuals who were not matched due to missing year of birth or age <18 years at index event. The final sample included 48,917 individuals ≥18 years old who had an incarceration release in 2010.
The characteristics of the cohort, stratified by MHA service use exposure category, are listed in Table 1. In total, 63.0% of incarcerated individuals had at least one MHA-related contact prior to index incarceration, with 12.5% having at least one psychiatric hospitalization, 18.1% having at least one MHA-related ED visit, and 32.4% having at least one MHA-related outpatient visit. The average age of incarcerated individuals was similar across the service use categories (33-35 years). Females were overrepresented in MHA-related hospitalization (21.4%) and ED visit (18.0%) service use categories, relative to the outpatient (11.8%) and no service use (7.5%) categories. Individuals from low- relative to high-income neighbourhoods were overrepresented overall, and the proportion of individuals from the lowest income quintile was slightly higher among those with MHA-related service use (hospitalization: 35.3%; ED visits: 38.0%; outpatient visits: 34.8%) than without (no MHA-related service use: 30.0%). Individuals with MHA-related hospitalizations and ED visits were less likely to be immigrants (5.4% and 4.5%, respectively) compared to those with MHA-related outpatient visits (8.0%) or no MHA-related service use (10.9%).
Characteristics of Study Cohort.
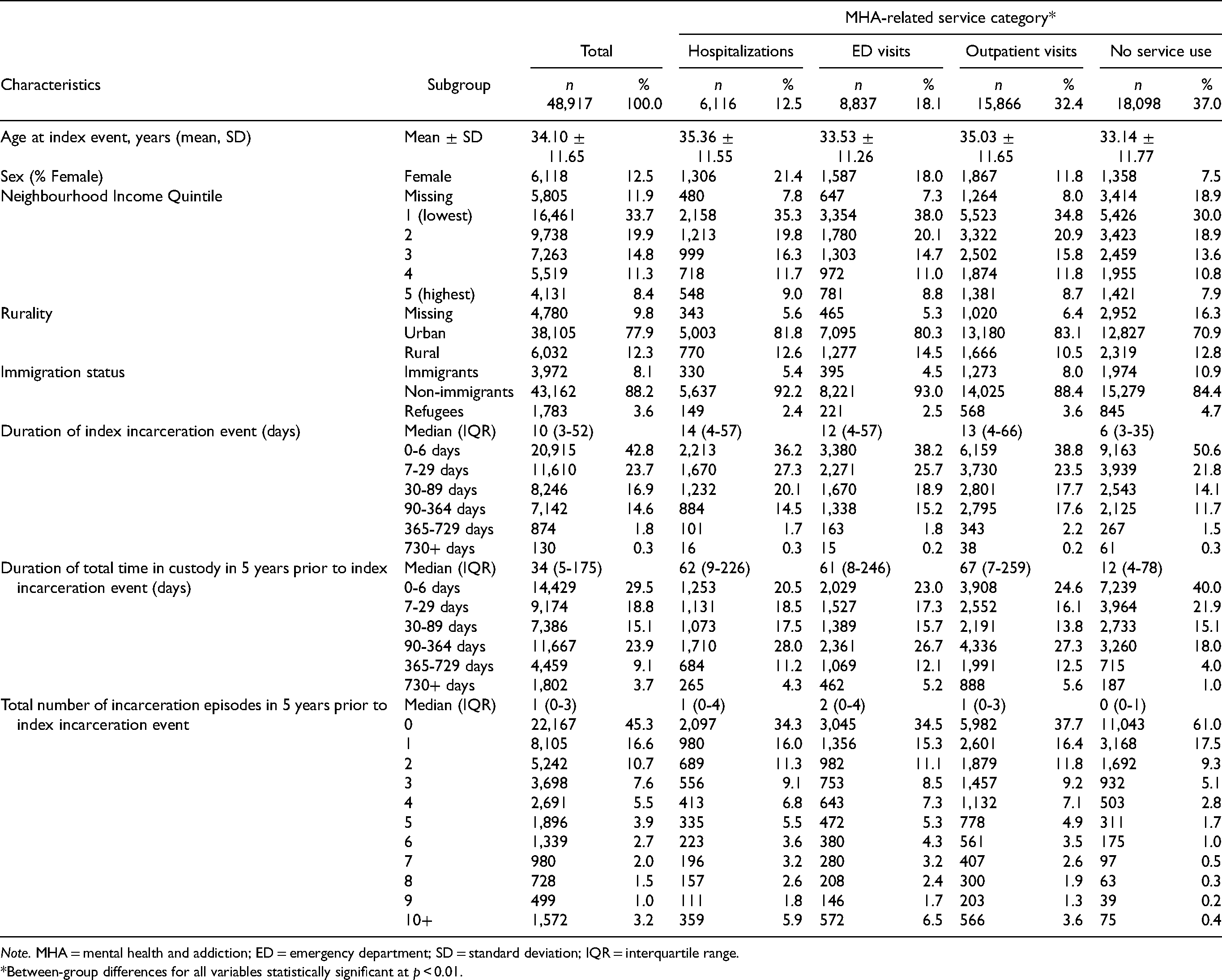
Note. MHA = mental health and addiction; ED = emergency department; SD = standard deviation; IQR = interquartile range.
Between-group differences for all variables statistically significant at p < 0.01.
The median duration of the index incarceration was longer for those with MHA-related service use prior to incarceration (hospitalization: 14 days [IQR: 4-57], ED visits: 12 days [IQR: 4-57], outpatient visits: 13 [IQR: 4-66]) than without (no MHA-related service use: 6 days [IQR: 3-35]). Individuals with MHA-related service use prior to incarceration also had a greater total of incarceration days (hospitalization: 62 [IQR: 9-226], ED visits: 61 [IQR: 8-246], outpatient visits: 67 [IQR: 7-259]) and episodes (hospitalization: 1 [IQR: 0-4], ED visits: 2 [IQR: 0-4], outpatient visits: 1 [IQR: 0-3]) in the 5 years prior to the index incarceration compared to individuals without (median total incarceration days: 12 [IQR: 4-78], median incarceration episodes: 0 [IQR: 0-1], Table 1).
Diagnostic Categories of Service Use Prior to Incarceration
Among those with an MHA-related hospitalization prior to the index incarceration, the three most common diagnostic categories were substance-related disorders (33.6%), mood disorders (19.1%), and psychotic disorders (17.9%, Table 2), with 10.0% hospitalized for self-harm (Table 2). The most commonly assigned diagnoses for outpatient visits in the hospitalization group were non-psychotic disorders (44.8%) and psychotic disorders (44.6%, Table 2). Among those with an MHA-related ED visit prior to the index incarceration, the most common diagnostic category was substance-related disorders (54.3%), followed by anxiety disorders (11.9%) and self-harm (11.0%, Table 2). The most commonly assigned diagnoses for outpatient visits in this group were non-psychotic disorders (55.2%) and psychotic disorders (15.6%, Table 2). Finally, among those who only had outpatient MHA-related service use prior to the index incarceration, the most common diagnostic group was non-psychotic disorders (75.3%), followed by substance-related disorders (12.6%) and psychotic disorders (9.3%, Table 2).
Diagnostic Subgroups of Service Use Prior to Incarceration.
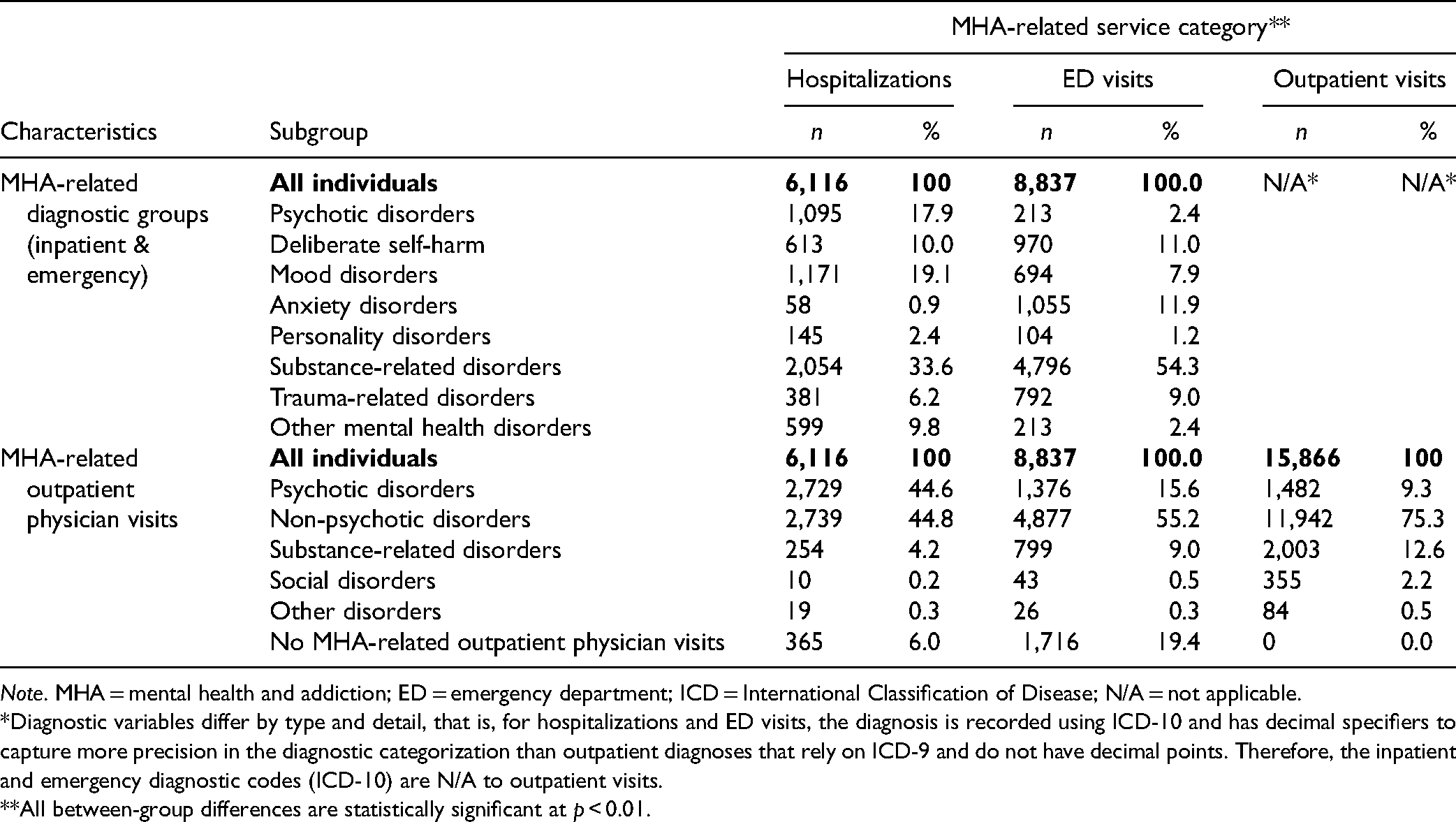
Note. MHA = mental health and addiction; ED = emergency department; ICD = International Classification of Disease; N/A = not applicable.
Diagnostic variables differ by type and detail, that is, for hospitalizations and ED visits, the diagnosis is recorded using ICD-10 and has decimal specifiers to capture more precision in the diagnostic categorization than outpatient diagnoses that rely on ICD-9 and do not have decimal points. Therefore, the inpatient and emergency diagnostic codes (ICD-10) are N/A to outpatient visits.
All between-group differences are statistically significant at p < 0.01.
MHA-Related Outpatient Service Use Prior to Incarceration
Overall, individuals with any MHA-related service use prior to incarceration had a median number of MHA-related PCP visits of 3 during the 5-year look-back (IQR: 1-10), but the number followed a gradient, with the highest frequency among individuals in the hospitalization category (median: 7, IQR: 2-20), followed by the ED visit category (median: 3, IQR: 1-11) and the outpatient visits category (median: 2, IQR: 1-7, Table 3). Similar gradients were observed in PCP diagnostic subgroups (Table 3). In terms of outpatient psychiatrist visits, a substantial proportion of individuals in the hospitalization (30.3%), ED visit (61.8%) and outpatient categories (71.3%) had no psychiatrist visit in the 5 years prior to the index incarceration (Table 3).
Volume and Type of Outpatient Service Use Prior to Incarceration.
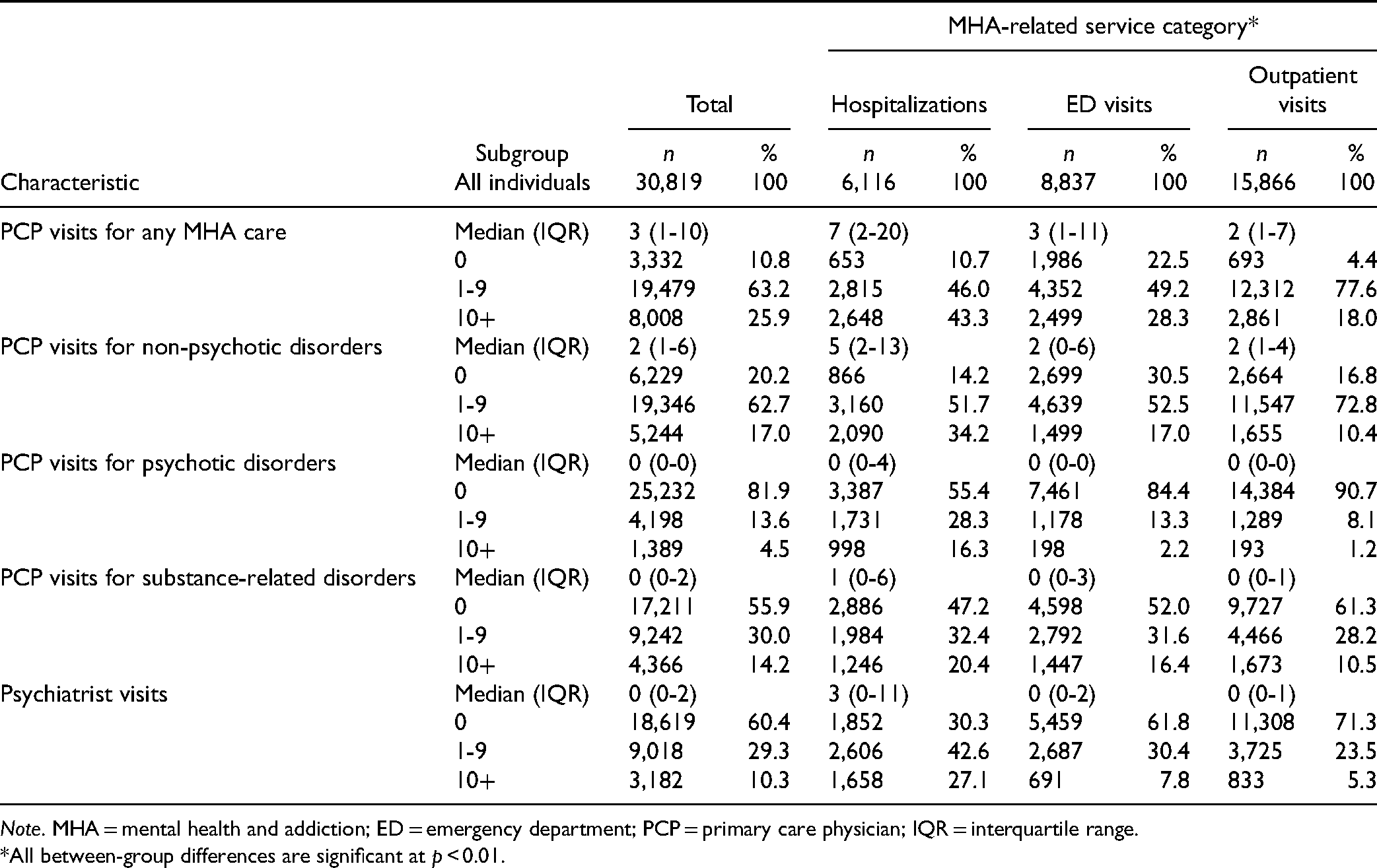
Note. MHA = mental health and addiction; ED = emergency department; PCP = primary care physician; IQR = interquartile range.
All between-group differences are significant at p < 0.01.
MHA-Related Service Use During Incarceration
Among those who had at least one psychiatric hospitalization prior to the index incarceration, 5.6% had a psychiatric hospitalization, 4.2% had an MHA-related ED visit, and 42.1% had an MHA-related outpatient visit during the index incarceration (Table 4). Among those who had at least one MHA-related ED visit prior to the index incarceration, 1.0% had a psychiatric hospitalization, 2.2% had a MHA-related ED visit, and 31.9% had an MHA-related outpatient visit during the index incarceration (Table 4). Among those who had at least one MHA-related outpatient visit prior to the index incarceration, 0.4% had a psychiatric hospitalization, 0.7% had an MHA-related ED visit, and 26.4% had an MHA-related outpatient visit during the index incarceration (Table 4). The proportion of individuals who had psychiatric hospitalizations, MHA-related ED visits, and MHA-related outpatient visits during incarceration increased with the increasing length of index incarceration (Table 4).
MHA-Related Service Use During Incarceration.
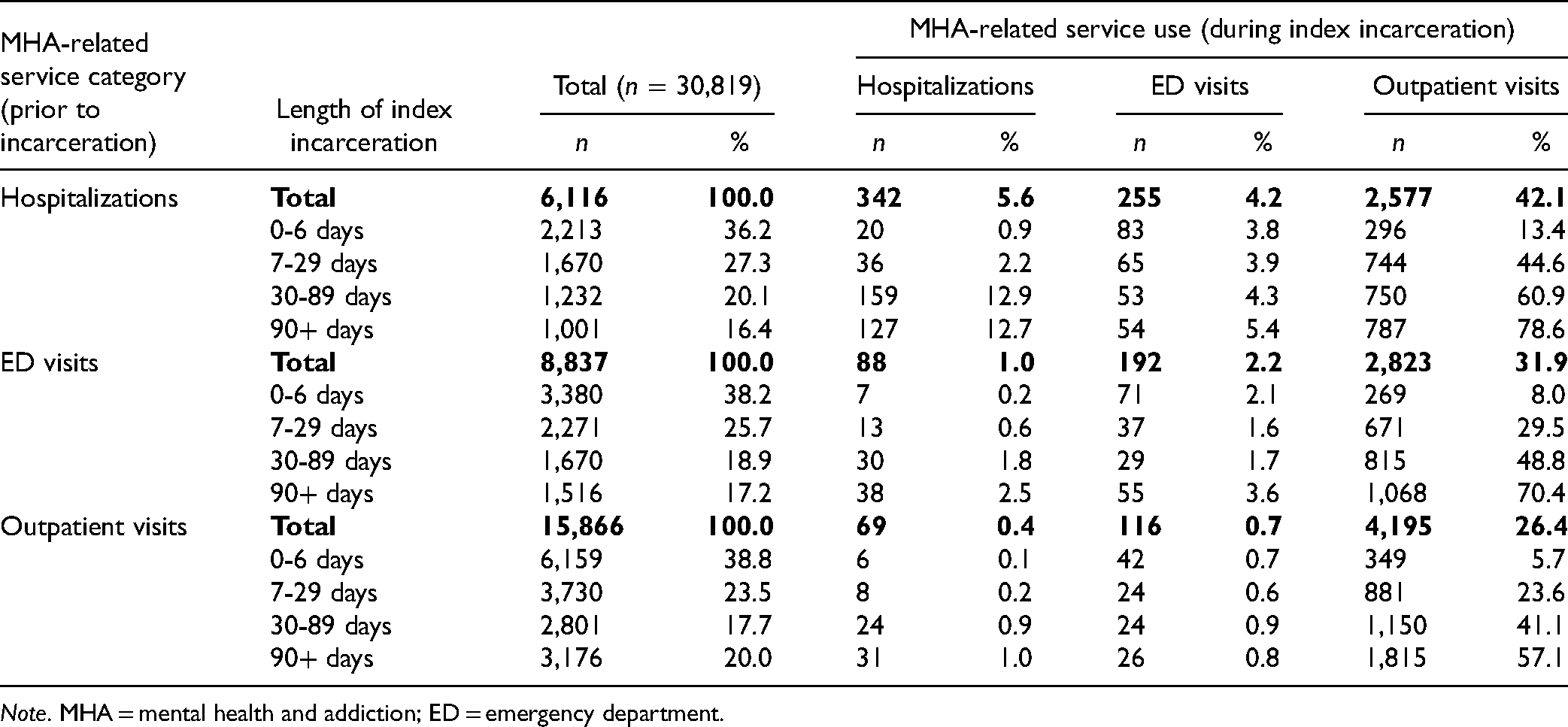
Note. MHA = mental health and addiction; ED = emergency department.
Discussion
In this population-based study of individuals released from Ontario provincial jails in 2010, the majority (63.0%) had some form of MHA-related service use in the 5 years prior to incarceration. Previous studies on MHA-related service use prior to incarceration have generally relied on self-reported lifetime service use and have found varying rates of use. For example, Brochu et al. 21 found that 6.3%, 36.9%, and 39.8% of men in Quebec reported receiving psychiatric, alcohol use, and drug use services, prior to incarceration and Nicholls et al. 20 found that 8.2%, 28.9%, and 57.7% of women in British Colombia reported receiving inpatient mental health, outpatient mental health, and SUD services prior to incarceration.
The results of our study align with this previous data insofar as we observed (1) higher rates of service use for SUDs than other psychiatric disorders and (2) higher rates of outpatient than inpatient care prior to incarceration. However, beyond the advantages of using linked correctional and health administrative data, our study built on this previous work by evaluating the specific types of psychiatric illnesses that were being treated in ED, hospital, and outpatient settings. We found that SUDs were most prevalent among individuals with MHA-related ED visits, whereas individuals with psychiatric hospitalizations had a relatively high prevalence of mood and psychotic disorders, and individuals with MHA-related outpatient visits had a relatively high prevalence of non-psychotic disorders. This suggested that individuals presenting to hospital, ED, or outpatient settings require different intervention strategies to promote positive downstream outcomes in the criminal justice system. For example, given that SUDs increase the risk of incarceration, 10 the high prevalence of SUD-related ED use indicates that EDs may be an important point of contact to initiate or facilitate SUD treatment to reduce the risk of incarceration and SUD-related morbidity and mortality.
The high prevalence of MHA-related service use prior to incarceration is also indicative of a high psychiatric illness burden among Ontarians experiencing incarceration, which parallels the existing Canadian and international literature. A recent international systematic review found good consistency in the reported prevalence of psychotic illness (4% in both men and women), major depression (10% in men, 14% in women), alcohol misuse (18-30% in men, 10-18% in women) and drug misuse (10-48% in men, 30-60% in women) within reports on prison populations globally. 3 Similarly, in Canada, 5% of men incarcerated in British Colombia have a self-reported history of psychotic disorders, 14% have a self-reported history of major depression, and 76% have a self-reported history of SUDs. 5
Our study does not directly align with these previous reports as it assessed MHA-related service use in the 5 years prior to incarceration rather than the lifetime prevalence of psychiatric diagnoses determined via self-report or chart review. Nonetheless, 5.7% of our cohort received care for psychotic disorders and 18.1% received care for SUDs prior to incarceration, which resembles these previous reports. The lower prevalence of service use for SUDs in our cohort (18%) relative to the high prevalence of SUDs reported in these previous studies (sometimes as high as 70-90%5,17,20,35–37) may reflect that many incarcerated individuals do not receive care for SUDs. This concept has been well established. For example, in 2004, only 14.8% of individuals in US state prisons who met Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria for drug abuse or dependence received addiction treatment. 38
Finally, nearly 1 in 3 individuals who had a prior psychiatric hospitalization and nearly 2 in 3 individuals who had an MHA-related ED visit did not see a psychiatrist in an outpatient setting in the 5 years prior to index incarceration. Furthermore, more than half of individuals with MHA-related service use prior to incarceration did not receive MHA-related services during their index incarceration. Together, these findings suggest that individuals with pre-existing SUDs or mental illness have difficulty accessing MHA-related services, particularly outpatient psychiatric care, both prior to and during incarceration. This aligns with and builds upon previous US studies that found that only ∼15-20% of individuals with pre-existing addictions and mental illness receive MHA-related care while incarcerated,38,39 and indicates that improved access and use of MHA-related services among justice-involved individuals is required.
Limitations
This study did not capture non-physician-based mental health services such as private addiction facilities and visits to non-physician MHA care providers, such as psychologists. If these types of services were preferentially accessed within provincial jails, this may partially explain the reduction in MHA-related service use we observed during incarceration. Most of these services require private payment, however, making this potential limitation less applicable to this marginalized population.
The use of administrative data also comes with the risk of misclassified diagnoses. This concern is partially mitigated by the fact that the coding algorithm used to identify MHA-related outpatient service use has been previously validated 33 ; however, its applicability to prison populations has not been specifically evaluated. Furthermore, there can be missing data within Ontario health administrative databases, which can bias results if this missingness is not random. The impact of this limitation is likely small in the current study, as only ∼2.5% of our cohort had to be discarded due to missing data. This study was also limited by using data from 2010, as these were the most recent data available. While the results of this study are likely representative of the current reality in the Ontario jail system, updated analyses will be warranted when more recent data become available. Finally, while a most responsible diagnosis was assigned to each MHA-related event, some will have been related to combined substance-related and psychiatric illnesses, which are known to increase the risk of negative outcomes and were not specifically evaluated in this study.
Conclusion
In this large, population-based study of individuals incarcerated in Ontario prisons, nearly two-thirds of individuals had evidence of prior MHA-related service use, and therefore illness burden, in the 5 years prior to incarceration. The substance-related disorder was the most frequent diagnosis among individuals with MHA-related hospitalizations and ED visits, but hospitalizations and ED visits for psychotic disorders, mood disorders, and self-harm were also common. Most individuals who used MHA-related services prior to incarceration never visited a psychiatrist and did not use MHA-related services during their index incarceration. These findings highlight that individuals experiencing incarceration with SUDs and mental illness have trouble accessing MHA-related care both prior to and during incarceration. Increasing the accessibility and use of MHA-related services throughout the criminal justice pathway is warranted and may help to reduce the overrepresentation of individuals with substance use disorders and mental illness in prisons.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437211055414 - Supplemental material for Prevalence of Mental Health and Addiction Service use Prior to and During Incarceration in Provincial Jails in Ontario, Canada: A Retrospective Cohort Study
Supplemental material, sj-docx-1-cpa-10.1177_07067437211055414 for Prevalence of Mental Health and Addiction Service use Prior to and During Incarceration in Provincial Jails in Ontario, Canada: A Retrospective Cohort Study by Paul Kurdyak, Erik L Friesen, Jesse T Young, Rohan Borschmann, Javaid Iqbal, Anjie Huang and Fiona Kouyoumdjian in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The use of ICES data in this project was authorized under section 45 of Ontario's Personal Health Information Protection Act. Research Ethics Board approval for the use of corrections data was obtained from the Hamilton Integrated Research Ethics Board (REB #4575).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH). It was also supported by the Mental Health and Addictions Scorecard and Evaluation Framework grant from the MOH (04601A14-19). The opinions, results, and conclusions reported in this paper are those of the authors and are independent of the funding sources. Dr Kurdyak received funding from the Canadian Institutes of Health Research. Dr Young receives salary and research support from a National Health and Medical Research Council Investigator Grant (NTG1178027). No endorsement by ICES or the Ontario MOH is intended or should be inferred.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.