
Abstract
Objective
Individuals with chronic psychotic disorders are overrepresented in correctional facilities, but little is known about factors that increase the risk of correctional involvement. The objective of this study was to compare individuals with chronic psychotic disorders who were released from correctional facilities in Ontario to individuals with chronic psychotic disorders but no correctional involvement on sociodemographic, clinical, and prior mental health-related health service utilization characteristics.
Method
All individuals with chronic psychotic disorders who were released from a provincial correctional facility in Ontario in 2010 were matched (1:2) by age and sex to Ontario residents with chronic psychotic disorders and no correctional involvement. Covariates included sociodemographic (rural residence, marginalization such as residential instability quintile, material deprivation quintile, dependency quintile, and ethnic concentration quintile) and clinical (duration of chronic psychotic disorder and comorbidities) characteristics, and mental health-related health service utilization characteristics (primary care physician, psychiatrist and emergency department visits, and hospitalizations) 1 and 3 years prior to correctional involvement. The association between correctional involvement and prior health service utilization was measured by estimating incidence rate ratios using Poisson and negative-binomial regressions.
Results
Individuals with correctional involvement (N = 3,197) lived in neighbourhoods with higher material deprivation and residential instability, and had a shorter duration of illness, and more psychosocial comorbidities (e.g., behavioural issues and depression) than individuals without correctional involvement (N = 6,393). Adjusting for sociodemographic and clinical variables, individuals with correctional involvement had a higher rate of mental health-related primary care physician visits, emergency department visits, and hospitalizations but a lower rate of psychiatrist visits prior to correctional involvement, compared to individuals without correctional involvement.
Conclusions
Despite higher mental health-related comorbidities and higher rates of accessing acute mental health services among individuals with chronic psychotic disorders and correctional involvement, visits to psychiatrists prior to involvement were low.
Introduction
In Canada, there are about 250,000 to 400,000 adult admissions into provincial/territorial correctional facilities each year. 1 This population has a poorer health status compared to the general Canadian population, including a higher prevalence of mental illness and substance use disorders across all diagnostic categories.2,3 In particular, individuals with chronic psychotic disorders are overrepresented in correctional facilities, where the prevalence rate of individuals with psychotic disorders in correctional facilities is 3.5% in Canada and other high-income countries, 4 compared to 0.3% in the general population. 5 Individuals with schizophrenia have also been found to experience a greater number of correctional encounters and have an increased risk of reincarceration compared to individuals without schizophrenia. 6
Despite the increased risk of correctional involvement, little is known about the factors associated with involvement among individuals with chronic psychotic disorders. Previous studies have examined potential social, demographic, clinical, and behavioural risk factors or correlates of incarceration among those with and without mental illness but not among individuals diagnosed with chronic psychotic disorders specifically.7,8 It has also been found that many of these sociodemographic risk factors are the same for individuals without mental illness, suggesting that among individuals with mental illnesses generally, there may not be differentiating risk factors associated with incarceration. 8 Given the high rate of correctional involvement among individuals with chronic psychotic disorders, it is important to determine the factors that are associated with the risk of correctional involvement among these individuals.
Although there are similar risk factors, there is a higher incidence of violence among individuals with schizophrenia related to symptoms of psychosis, including experiencing delusions, paranoia, or hallucinations. 9 Therefore, adequate treatment of chronic psychotic disorders is likely to reduce the risk of symptom-driven criminality. 10 Previous studies have examined health service utilization during or following incarceration for individuals with psychotic disorders or other mental illnesses;7,11 however, investigating health service utilization and patterns prior to correctional involvement may be important in a few ways. It can provide a deeper understanding of differences in types of care being accessed by individuals with chronic psychotic disorders who later experience correctional involvement and whether more or better service provision reduces the risk of correctional involvement.
The objective of the present study was to compare adults with chronic psychotic disorders who were released from a provincial correctional facility in Ontario in 2010 to age- and sex-matched adults with chronic psychotic disorders but no correctional involvement in sociodemographic, clinical, and prior mental health-associated health care utilization. Understanding risk factors specific to individuals with chronic psychotic disorders with correctional involvement may help inform targeted interventions to reduce rates of correctional involvement.
Methods
Study Setting and Design
The Ontario provincial correctional system is responsible for the detention of all people on remand (i.e., those held in custody and awaiting trial) and people serving custodial sentences of <2 years. Provincial correctional facilities include jails, detention centres, and correctional centres.
This study used a matched case-control design. Cases were defined as individuals diagnosed with chronic psychotic disorders who were released from Ontario's provincial correctional facilities between 1 January 2010 and 31 December 2010.11,12 The index event was the date of first incarceration release in 2010. The maximum time period for a provincial correctional event is 2 years, although this does not include presentence or pretrial custody that may extend beyond the 2 years. The index admission was the specific incarceration admission date that led to the index release. Controls were defined as individuals from the general Ontario population diagnosed with chronic psychotic disorders prior to 1 January 2010, and without correctional involvement. It is assumed that controls (i.e., those not released from a correctional facility in 2010) had no other correctional involvement. The index event for controls was 1 January 2010, given that controls did not experience correctional involvement during the 2010 period. The data are retrospective to 2005, so to ensure the same correctional and health service utilization observation period for every case, regardless of index event duration, the look back period was 3 years prior to the index event. All cases were matched 1:2 by age (±6 months from birthdate) and sex (male or female) to controls (except 1 case was matched to 1 control) to investigate how both groups differed on characteristics of interest.
Data Sources
The Ontario Ministry of the Solicitor General provided data on individuals released from provincial correctional facilities from 2005 to 2015. This included demographic data on age, sex, and address of residence on correctional entry as well as correctional data on admission dates, release dates, and reasons for release. The corrections data were linked to health administrative data contained within ICES. ICES is an independent, nonprofit research institute whose legal status under Ontario's health information privacy law allows it to collect and analyse health care and demographic data, without consent, for health system evaluation and improvement. The corrections data were linked to ICES data using ICES Key Numbers, which are based on health card numbers or other direct personal identifiers. The linkage rate was approximately 97%. 11 This study was approved by the Hamilton Integrated Research Ethics Board (Study 4575).
The Registered Persons Database (RPDB) is a population-based registry maintained by the Ontario Ministry of Health (MOH) and was used to obtain population and basic demographic data on Ontario residents who use the provincial health care system. These data included birthdate, sex, address, date of death, and Ontario Health Insurance Plan (OHIP) eligibility and status changes. This database also provided each resident's postal code of residence, which was used to obtain data on neighbourhood-level information, including the rurality of residence and the degree of area-level marginalization. The Ontario Marginalization Index is a geographically (census) based index developed to quantify the degree of neighbourhood-level marginalization occurring across the province, 13 sourced from The Ontario Community Health Profiles Partnership. It combines a large range of demographic indicators into 4 distinct dimensions thought to underlie the construct of marginalization: residential instability (high rates of family or housing instability), material deprivation (poverty and inability to access and attain basic material needs), dependency (not having income from employment), and ethnic concentration (recent immigrants and/or belonging to “visible minority” group). The collection of indicators for each dimension is determined based on the postal code.
Data for mental health-associated health service utilization were acquired from data sources held at ICES. Several health care databases were accessed to obtain data on administrative, sociodemographic, and clinical data on all healthcare encounters covered by Ontario's public health care system. The OHIP billing codes from the claims database provided data on the number of primary care physician (PCP) and psychiatry visits. The ICES Physicians Database was used to identify physical specialties to accurately differentiate between PCP and psychiatrist visits. For hospital-based care data, the Canadian Institute for Health Information (CIHI) Discharge Abstract Database provided data on all acute psychiatric hospitalizations in nonpsychiatric designated beds, and the Ontario Mental Health Reporting System provided data on all psychiatric hospitalizations in psychiatric designated beds. The National Ambulatory Care Reporting System provided data on emergency department visits. These datasets were linked using unique encoded identifiers and analysed at ICES.
Population
All persons included in this study received a primary diagnosis of psychotic disorder including schizophrenia, schizoaffective disorder, or psychotic disorder not otherwise specified (NOS), prior to 1 January 2010. These individuals were identified using a validated, nonspecific algorithm using OHIP billing codes and hospitalizations. 14 A diagnosis of psychotic disorder NOS was also included because the addition of psychotic disorder NOS to the health administrative data algorithm that included schizophrenia and schizoaffective disorder improved the test characteristics of the algorithm and there is evidence that most individuals who receive this diagnosis often later receive a schizophrenia or schizoaffective disorder diagnosis.14,15
Exclusion criteria for cases included individuals whose data could not be linked to a valid identifier in the administrative data, 11 who had missing data on postal code information, age, and sex, and whose ages <18 or >105 years at the time of index admission date, who had not been an Ontario resident for at least 5 years prior to index admission date, and who died prior to correctional release as of 1 January 2010. Only the first incarceration release in 2010 was used in analyses for individuals with multiple incarceration releases. Data of individuals in the control group were acquired from the RPDB from a pool of individuals diagnosed with chronic psychotic disorders by applying the same exclusion criteria used for the case group, except the age and Ontario residence criteria had to be met prior to 1 January 2010.
Characteristics
This study compared individuals with and without correctional involvement on several characteristics. Sociodemographic characteristics included urban/rural residence and neighbourhood marginalization dimensions. Rurality was defined using the Rurality Index of Ontario score where scoring 0 to 39 was considered urban and scoring 40 or more was considered rural. 16 The 4 neighbourhood marginalization dimensions included the residential instability quintile, material deprivation quintile, dependency quintile, and ethnic concentration quintile. Quintiles were ranked from 1 (least marginalized) to 5 (most marginalized).
Clinical characteristics included duration of psychotic disorder diagnosis and medical and psychosocial comorbidities. The duration was defined as the period between the first diagnosis of a chronic psychotic disorder and the index admission date for cases and the first diagnosis of a chronic psychotic disorder on 1 January 2010, for controls. The ACG® System Aggregated Diagnosis Groups (ADGs) from the John Hopkins ACG® System Version 10 were used as a proxy measure of comorbidities. 17 ADGs have been shown to predict mortality in the province of Ontario in the general population 18 and in a population of individuals with schizophrenia. 19 The ADGs were obtained 2 years prior to the index date.
Finally, characteristics of mental health-related health service utilization were divided into 4 categories: PCP visits, psychiatrist visits, emergency department visits, and hospitalizations. The categorization of mental health-related visits was based on a validated algorithm using OHIP billing codes. 20 All health service utilization characteristics were assessed for the 1- and 3-year period prior to the index admission date. This look back period was selected to ensure the same observational period for correctional and health service utilization data for all cases, irrespective of time spent in a correctional centre.
Statistical Analysis
Descriptive data on baseline sociodemographic, clinical, and prior mental health-related health service utilization characteristics for cases and controls were summarized using frequencies and proportions for categorical data and means (standard deviation) and medians (interquartile range) for continuous variables. Between-group differences were assessed using standardized differences, where a standardized difference of 0.1 or greater was considered significant. 21
Health service utilization visits were calculated for all participants in the 1- and 3-year periods before the index admission date. Two sets of regression models were constructed to estimate the association between correctional involvement and various prior mental health-related health service utilization for the 1- and 3-year periods prior to the index admission. Poisson regression was conducted for a number of hospitalizations and due to concerns of dispersion, negative-binomial regression was conducted for PCP, psychiatrist, and emergency department visits. For each set of regression models, unadjusted and adjusted models were constructed, where adjusted models controlled for all sociodemographic and clinical variables including sex, age, rural residence, four marginalization dimensions, duration of diagnosis, and total number of comorbidities. All analyses were completed in SAS version 9.4. 22
Results
In 2010, a total of 3,280 individuals with chronic psychotic disorders were released from a provincial correctional facility. After excluding individuals with missing demographic information (N = 50) and those who had not resided in Ontario for at least 5 years prior to the index admission date (N = 32), 3,197 individuals were identified and included as cases. Cases had a mean age of 37 years; most were males (83.6%) and lived in urban settings (91.0%). All cases, except for one, were age- and sex-matched to 6,393 controls (Table 1).
Baseline Characteristics as of index Admission Date of Individuals With Chronic Psychotic Disorders by Correctional Involvement.a,b
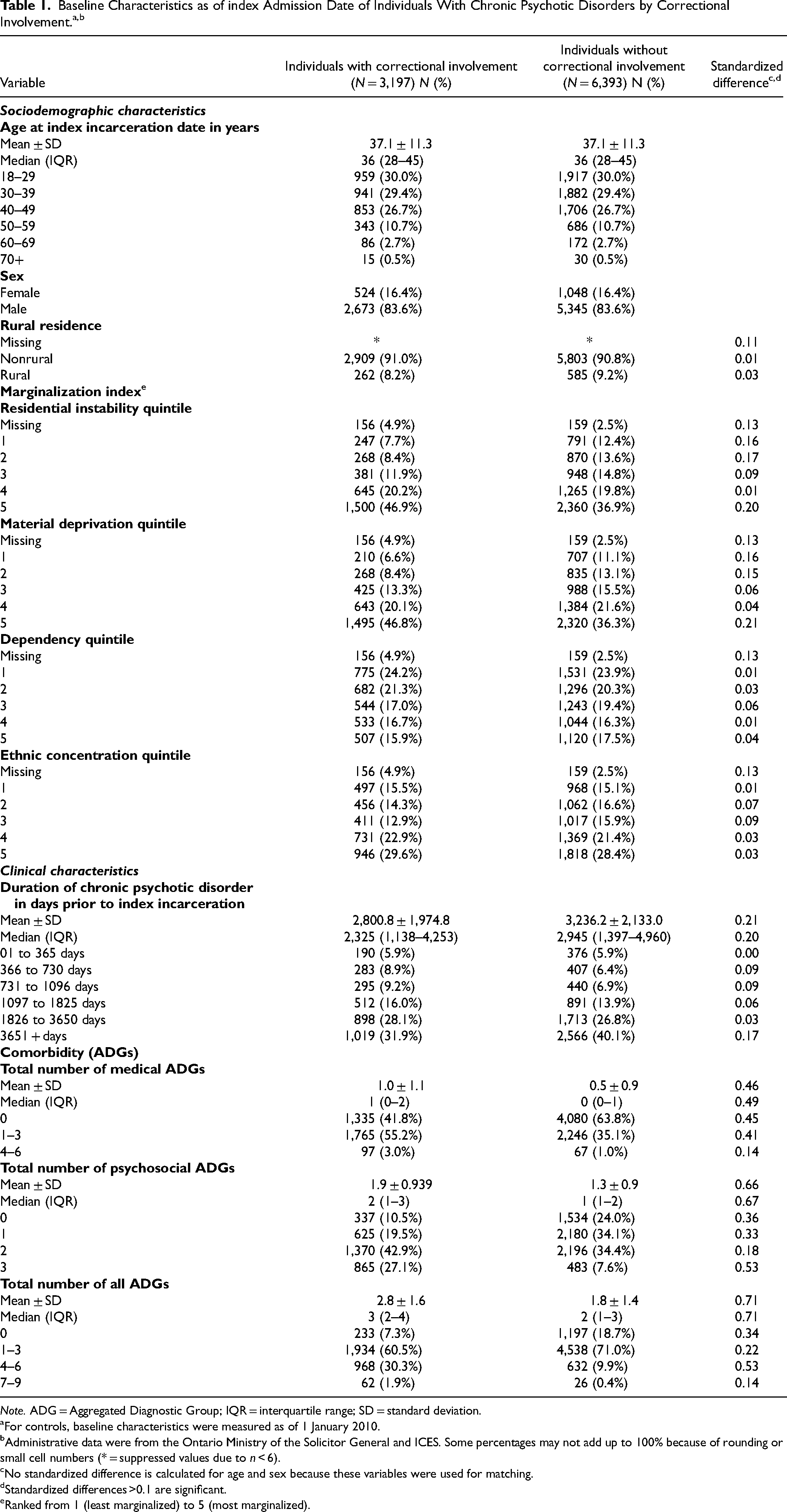
Note. ADG = Aggregated Diagnostic Group; IQR = interquartile range; SD = standard deviation.
For controls, baseline characteristics were measured as of 1 January 2010.
Administrative data were from the Ontario Ministry of the Solicitor General and ICES. Some percentages may not add up to 100% because of rounding or small cell numbers (* = suppressed values due to n < 6).
No standardized difference is calculated for age and sex because these variables were used for matching.
Standardized differences >0.1 are significant.
Ranked from 1 (least marginalized) to 5 (most marginalized).
The sociodemographic and clinical characteristics of individuals with chronic psychotic disorders with and without correctional involvement are shown in Table 1. Of the 4 marginalization dimensions, individuals with correctional involvement tended to experience greater residential instability (46.9% vs. 36.9% in the most marginalized quintile, standardized difference: 0.20) and material deprivation (46.8% vs. 36.3% in the most marginalized quintile, standardized difference: 0.21) than individuals without correctional involvement. The distributions of quintiles for dependency and ethnic concentration were not significantly different between individuals with and without correctional involvement. Furthermore, cases were more likely, on average, to have a shorter mean duration of illness (2,800 [SD=1,975] vs. 3,236 [SD=2,133] days) and a higher mean total number of comorbidities (2.84 [SD=1.63] vs. 1.78 [SD=1.36]), mean medical comorbidities (0.97 [SD=1.08] vs. 0.52 [SD=0.85]) and mean psychosocial comorbidities (1.86 [SD=0.93] vs. 1.25 [SD=0.91]).
Mental health-related health service utilization 1 year and 3 years prior to the index admission date is outlined in Table 2. In both the 1- and 3-year prior periods, the number of PCP visits, emergency department visits, and hospitalizations were all higher among those with correctional involvement than those without correctional involvement. However, there was no significant difference among the higher number of psychiatrist visits.
Mental Health-Related Health Service Utilization 1 Year and 3 Years Prior to Index Admission Date.a
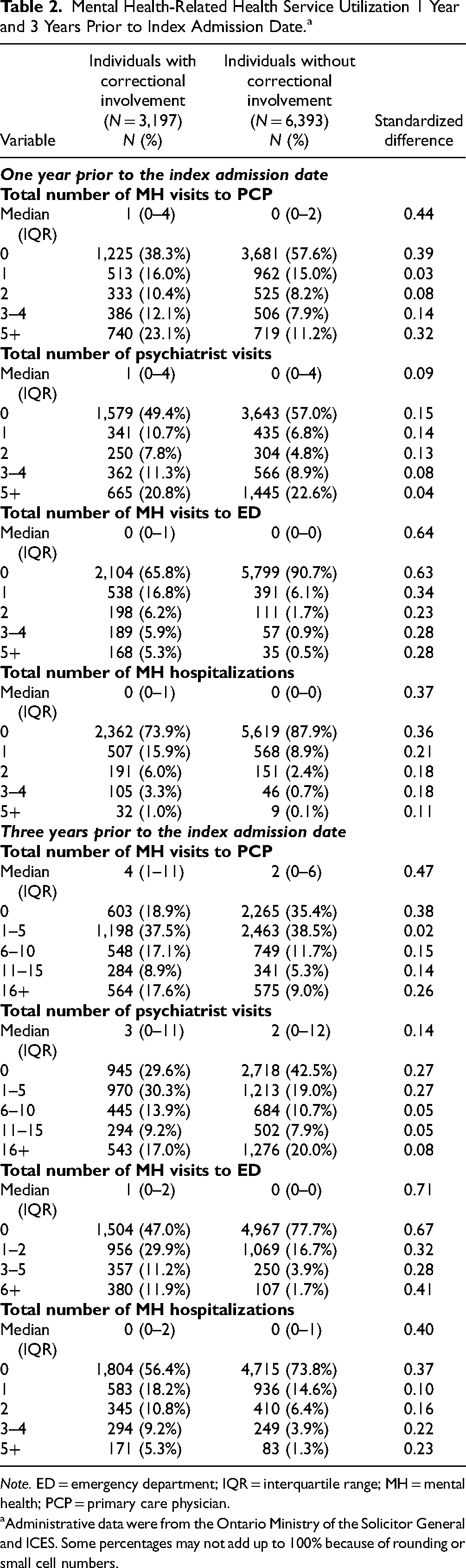
Note. ED = emergency department; IQR = interquartile range; MH = mental health; PCP = primary care physician.
Administrative data were from the Ontario Ministry of the Solicitor General and ICES. Some percentages may not add up to 100% because of rounding or small cell numbers.
Unadjusted and adjusted incidence rate ratios (IRRs) have been provided for each type of mental health-related health service use for 1 and 3 years prior to the index admission date in Figure 1 and Supplemental Tables 1 and 2. The adjusted rates are summarized below.
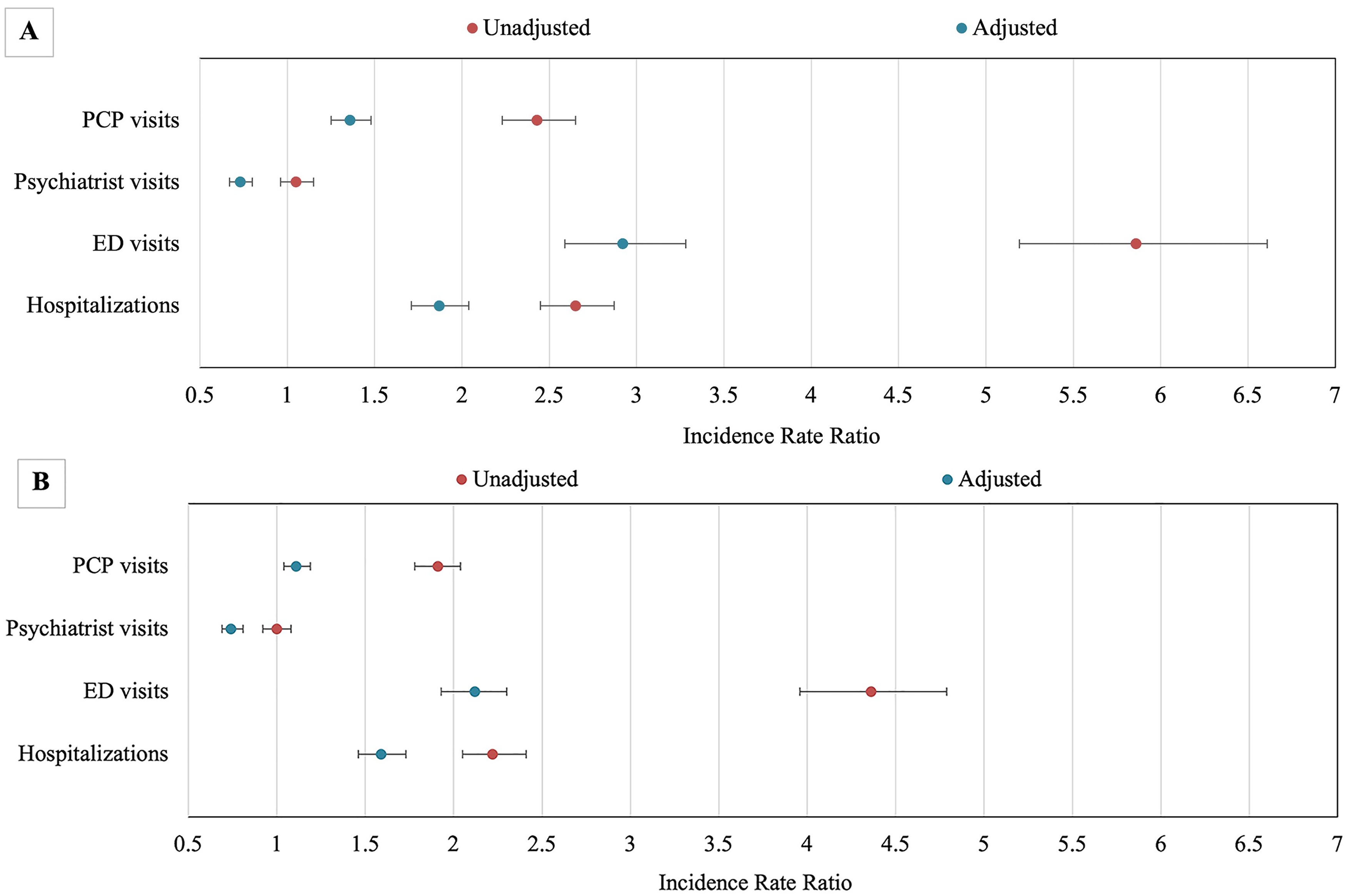
IRRs of mental health-related health service utilization among individuals with chronic psychotic disorders with versus without correctional involvement (A) 1 year prior to index admission date and (B) 3 years prior to index admission date.a
One year prior to correctional involvement, and adjusting for sociodemographic and clinical variables, individuals with correctional involvement had a higher rate of prior PCP mental health-related visits (IRR 1.36, 95% CI, 1.25 to 1.48), but a lower rate of psychiatrist visits (IRR 0.73, 95% CI, 0.67 to 0.80) 1 year prior to index admission. Individuals with correctional involvement also had higher rates of both mental health-related emergency department visits (IRR 2.92, 95% CI, 2.59 to 3.28) and mental health-related hospitalizations (IRR 1.87, 95% CI, 1.71 to 2.04) (Figure 1A and Supplemental Table 1). Adjusting for sociodemographic and clinical variables, individuals with correctional involvement had a higher rate of 3 years prior PCP mental health-related visits (IRR 1.11, 95% CI, 1.04 to 1.19), but a lower rate of psychiatrist visits (IRR 0.74, 95% CI, 0.69 to 0.81) 3 years prior to the index admission. Individuals with correctional involvement also had higher rates of both mental health-related emergency department visits (IRR 2.11, 95% CI, 1.93 to 2.30) and mental health-related hospitalizations (IRR 1.59, 95% CI, 1.46 to 1.73) (Figure 1B and Supplemental Table 2).
Discussion
This study compared individuals with a diagnosis of chronic psychotic disorders with and without correctional involvement. Individuals with correctional involvement were more likely to live in neighbourhoods with high rates of residential instability (family or housing) and deprivation of basic material needs (poverty), and were more likely, on average, to have a shorter duration of illness and higher total, medical, and psychosocial comorbidities than individuals without correctional involvement. Individuals with correctional involvement also had higher rates of mental health-related primary care and acute care (emergency department visits and hospitalizations) utilization, but lower rates of psychiatric care utilization both 1 year and 3 years prior to the index admission date.
Higher rates of prior mental health-related acute care among individuals with correctional involvement have been previously reported. Constantine et al. 23 found that individuals with serious mental illness with emergency room or inpatient mental health services contact in the previous 90 days had an increased likelihood of misdemeanour and felony arrests. Although individuals with correctional involvement had higher rates of 1- and 3-year prior mental health-related PCP visits, emergency department visits, and hospitalizations, the incidence rates of these prior mental health-related PCP and acute health service utilization were largely attenuated after controlling for sociodemographic and clinical characteristics. This suggests that these characteristics may be important factors associated with the use of these mental health-related services. Specifically, the total number of comorbidities largely attenuated the relationship between correctional involvement and health service utilization, which aligns with prior research that has found that psychiatric comorbidities for individuals with schizophrenia are associated with frequent hospitalizations and emergency services. 24 Given that individuals with correctional involvement also had a higher number of comorbidities than individuals without correctional involvement and that the high prevalence of medical and psychiatric comorbidities among individuals with schizophrenia is associated with adverse outcomes such as decreased quality of life and lifespan,24-29 frequent interactions with the health care system may present opportunities for intervention, including treatment of schizophrenia and comorbidities. Given the higher rates of mental health-related acute and primary care visits among those with correctional involvement, it is unclear what is required to mitigate rates of correctional involvement. Further research is required to determine what type of health service interventions might reduce correctional involvement.
Interestingly, the unadjusted rates of 1- and 3-year prior psychiatry visits were not significantly different for individuals with chronic psychotic disorders with and without correctional involvement. This could suggest that access to psychiatrists for individuals with chronic psychotic disorders is challenging, regardless of correctional involvement. However, as highlighted above, individuals with correctional involvement were more likely to experience greater residential instability, material deprivation, and medical and psychosocial comorbidities. If these sociodemographic and clinical variables are proxies for need, this suggests there is a greater need for psychiatric involvement among individuals with correctional involvement. The lower rates of psychiatrist visits for people with correctional involvement after including these variables in the model suggest that although the absolute rates of psychiatrist visits are equivalent, there may be an unmet need for psychiatric care among individuals with correctional involvement assuming that individuals without correctional involvement are receiving adequate care. However, as mentioned above, frequency of care may be an inadequate proxy for quality care and meeting mental health care needs, so this conclusion must be interpreted with caution. Prior US studies have also reported similar trends in specialist mental health care.23,30 Along with examining acute care contact, Constantine et al. 23 also examined mental health outpatient contact and found that among adults with serious mental illness in Florida, not having contact with outpatient mental health services 90 days prior to correctional involvement increased the odds of misdemeanour and felony arrests and spending additional days in jail. Wilper et al. 30 analysed national survey data and reported lower rates of psychiatric treatment (medication or counselling) in the year prior to incarceration than during incarceration among people in prison and jail with schizophrenia or bipolar disorder. Overall, the results of this study may indicate poor continuity or lack of access to community psychiatric care among those that become involved with correctional centres. Although the present study does not elucidate reasons for limited ongoing psychiatric management, the results suggest that the needs of individuals with correctional involvement are not being met, resulting in adverse outcomes. Since previous studies have found that poorer stability of mental health may lead to offending behaviour, 9 further research on access or barriers to psychiatric care is required.
Strengths and Limitations
The present study has the following strengths. It uses unique data linkage between provincial correctional data and health administrative data to examine sociodemographic, clinical, and health service utilization characteristics in individuals with chronic psychotic disorders who experienced correctional involvement in Ontario. This is also the first study in Canada to examine differences in prior health service utilization among individuals with chronic psychotic disorders with and without correctional involvement.
However, this study has several limitations. Although individuals in provincial correctional facilities are sentenced for a maximum period of two years, individuals may have also spent time in jail prior to being sentenced. Since this was not accounted for in the present study, individuals may have spent slightly varying times in correctional facilities. Relatedly, individuals in the control group may have had legal involvement during the timeframe used for this study. There were limited data on important individual-level sociodemographic characteristics that have been previously identified that could not be examined in the present study including race, educational attainment, marital status, and housing status. 8 Neighbourhood-level factors were examined using the marginalization index to assess important sociodemographic characteristics in the study population. Future research and policies should also consider the compounding impact of social conditions (e.g., poverty) among individuals with chronic psychotic disorders as these factors may be of specific importance for predicting correctional involvement. 8 Furthermore, the identification of individuals with chronic psychotic disorders was ascertained through clinical codes in the health administrative dataset and not formal clinical assessments, potentially resulting in misclassification of psychotic disorders diagnosis status. However, the algorithm developed to identify individuals with chronic psychotic disorders has been validated using health administrative databases in Ontario. 14 Relatedly, specific diagnoses known to contribute to correctional involvement, such as substance use disorders, may have accounted for some of the group differences observed. However, ADGs were used as a proxy measure due to concerns regarding the accuracy of specific diagnoses in this study population. Finally, this study used data from 2010 as these were the most recent correctional involvement data available. Future studies should conduct updated analyses and examine any changes over time.
Conclusion
Individuals with chronic psychotic disorders are overrepresented in correctional facilities compared to the general population. Individuals with chronic psychotic disorders and correctional involvement resided in neighbourhoods with higher residential instability and material deprivation and have higher medical and mental health-related comorbidities than individuals with chronic psychotic disorders and no correctional involvement. Individuals with correctional involvement had higher rates of mental health-related primary and acute care utilization, but lower rates of psychiatric care utilization. Future studies are needed to closely examine whether individuals with chronic psychotic disorders receive timely access to specialist outpatient care to improve mental health care for this marginalized population.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437231189468 - Supplemental material for Chronic Psychotic Disorders and Correctional Involvement: A Population-Based Matched Case-Control Study in Ontario, Canada
Supplemental material, sj-docx-1-cpa-10.1177_07067437231189468 for Chronic Psychotic Disorders and Correctional Involvement: A Population-Based Matched Case-Control Study in Ontario, Canada by Ruchi Vijh, Fiona G. Kouyoumdjian, Tomisin Iwajomo, Alexander I. F. Simpson, Roland Jones, Claire de Oliveira and Paul Kurdyak in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() . The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification. Parts of this material are based on data and information compiled and provided by the Ontario MOH and the CIHI. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification. Parts of this material are based on data and information compiled and provided by the Ontario MOH and the CIHI. We thank the Toronto Community Health Profiles Partnership for providing access to the Ontario Marginalization Index. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health. This study was funded by a grant from the Canadian Institutes for Health Research (CIHR).
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.