
Abstract
Objectives:
Individuals with schizophrenia are overrepresented in correctional facilities relative to their population-based prevalence. The purpose of this study was to determine the rate and predictors of reincarceration of individuals with schizophrenia after release from correctional facilities.
Methods:
This was a retrospective cohort study that included all people released from Ontario’s provincial correctional facilities from January 1 to December 31, 2010. Individuals with schizophrenia were identified using a population-based algorithm. The primary outcome was time to reincarceration. Covariates included sociodemographic characteristics (age, sex, neighborhood income quintile, urban/rural residence), health service utilization (primary care physician visits, psychiatrist visits, psychiatric and nonpsychiatric hospitalizations, emergency department visits), and other clinical comorbidity. Survival analysis was used to examine the association between schizophrenia and reincarceration.
Results:
Among 46,928 individuals, N = 3,237 (7%) had a diagnosis of schizophrenia. Approximately 67.5% of these individuals were reincarcerated within 5 years following their first release in 2010, compared to 58.8% of individuals without schizophrenia. Individuals with schizophrenia were 40% (HR = 1.39, 95% CI, 1.33 to 1.45) more likely to be reincarcerated following release than the control group after adjusting for demographic characteristics. This association reduced to 8% (HR = 1.08, 95% CI,1.03 to 1.14) after adjusting for prior health service utilization, prior correctional involvement, and comorbidities.
Conclusion:
Individuals with schizophrenia were more likely to experience reincarceration after release from correctional facilities. This risk is partly explained by prior correctional involvement, health service utilization, and comorbidities. Future research should focus on risk factors predicting the higher reincarceration rate and interventions to reduce correctional involvement.
Introduction
Individuals with schizophrenia are at higher risk of incarceration compared to individuals without serious mental illness. 1,2 This higher rate of incarceration has translated into a schizophrenia prevalence in correctional facilities that is 3 to 6 times the population prevalence. 3 Estimates from Canadian studies similarly suggest a higher prevalence of schizophrenia and other psychotic disorders in custodial populations. 4,5
The higher rate of incarceration among individuals with schizophrenia may be due in part to higher rates of recidivism and potential reincarceration or effects of criminal justice interventions. For instance, reoffending after correctional facility release is increased by 40% among individuals with severe mental illnesses 3 compared to those without. In particular, a significant factor for higher risk of reincarceration for individuals with schizophrenia in contrast to those without is technical violation. Technical violations arise from criminal justice sanctions (court appearances, probation, and parole requirement). Individuals with schizophrenia may have challenges adhering to probation and parole requirements resulting in a greater likelihood of getting new charges for these violations. The high rate of incarceration and reincarceration among individuals with schizophrenia may also be partially due to poor access to treatment, 6 and evidence suggests that timely access to care among individuals with schizophrenia who have been released from correctional facilities can reduce the likelihood of reincarceration. 7,8
The objective of this study was to determine the prevalence of schizophrenia in persons released from Ontario correctional centers in 2010 and to estimate reincarceration rates among these individuals with schizophrenia compared to those without a diagnosis of schizophrenia. We used comprehensive population-based correctional and health administrative data for all Ontario residents who were released from provincial correctional facilities in 2010.
Methods
Study Setting and Design
The Ontario provincial correctional system is responsible for the detention of all persons on remand and sentenced inmates subject to sentences of less than 2 years. Sentenced people have an average length of stay of approximately 60 days, and people on remand of approximately 40 days, although the median remand length of stay is closer to 1 week.
Individuals who were released from Ontario’s provincial correctional facilities from January 1 to December 31, 2010, served as the study population, based on available data 9,10 Exclusion criteria included individuals whose age was less than 18 and greater than 105 at the time of the first correctional facility release data in 2010 (the index event), individuals whose data could not be linked to a valid identifier in the administrative data, 10 individuals who were missing information about their place of residence, and individuals who were not residents of Ontario for the 3 years prior to the admission date of the index incarceration—as health service utilization data would not be available for these individuals.
Data Sources
The Ministry of Community Safety and Correctional Services data set provided data for individuals within this cohort from 2005 to 2015. The index release was the first release in 2010, and the maximum period of time for a provincial correctional event is 2 years. Since the data are retrospective to 2005, 3 years prior to correctional center was the lookback duration that ensured the same correctional and health service utilization observation period for each subject regardless the duration of index correctional event duration. Subjects were followed from the index release in 2010 to a maximum follow-up date of December 31, 2015, to capture correctional involvement and health service utilization.
The Ministry of Community Safety and Correctional Services provided sociodemographic data including age, sex, self-reported race, address on correctional entry (data on income quintile and rurality of residence were accessed at ICES, Toronto-Ontario’s largest health data repository, using the address provided), and dates of entry and release from provincial custody from 2005 to 2015. These data were linked with health administrative data contained within ICES using valid ICES Key Numbers, which are unique person identifiers that are encoded Ontario Health Insurance Plan (OHIP) numbers. The linkage rate was approximately 97%.
Data related to health service utilization were obtained using administrative health information data sets including the Canadian Institute for Health Information Discharge Abstract Database (CIHI DAD), the Ontario Mental Health Reporting System (OMHRS), the National Ambulatory Care Reporting System (NACRS), and OHIP Claims Database. These health databases capture and report administrative, clinical, and demographic data such as hospital admission and discharge, length of stay, emergency department registrations, and ambulatory encounters. The Registered Persons Database (RPDB) was used to obtain population and demographic data. The RPDB is a population-based registry maintained by the Ministry of Health and Long-term Care in Ontario. The data set has demographic information on individuals that use the health system including date of birth, sex, address, date of death, and OHIP eligibility and status changes. All these data sources are held at ICES. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. These data sets were linked using unique encoded identifiers and analyzed at ICES. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board.
Exposure Variable
The provincial correctional sample was stratified based on the presence of a diagnosis of schizophrenia prior to the index event. Persons with a schizophrenia diagnosis were identified using a validated nonspecific algorithm using OHIP billing codes, emergency department visits, and hospitalizations. 11 Psychosis not otherwise specified is often indistinguishable from schizophrenia, and therefore, we included this diagnosis. The definition was ≥1 hospitalization (DAD/OMHRS) or ≥3 OHIP claims in a 3-year period with DSM-IV/ICD9 dx 295, 298, ICD10 F20, F25, F29. 11
Outcomes
The primary outcome of this study was reincarceration, measured as time to first readmission to a provincial correctional facility after the date of first release in 2010. Secondary outcomes of this study were measures of correctional events and health service utilization. Outcomes included the number of admissions to provincial correctional facilities within 5 years of the index event, the total number of days in custody in provincial correctional facilities within 5 years of the index event, and the time to first contact for each of the following health services after release: primary care physician (PCP) contact (including total, mental health–related, and non-mental health–related contact), psychiatrist contact, emergency department visit (for all causes and mental health reason), medical hospitalization, and psychiatric hospitalization.
Covariates
Sociodemographic characteristics included age, sex, neighborhood income quintile, and urban/rural residence. Age was divided into 6 categories (18 to 29, 30 to 39, 40 to 49, 50 to 64, 65 to 74, and 75+ years). Neighborhood income levels were obtained using Census Canada information provided by Statistics Canada (May 2006). Neighborhood income levels were divided into 5 categories based on distribution, in which income level 1 was defined as the lowest income quintile and level 5 as the highest based on dissemination areas. 12 Rurality was defined using the Rurality Index of Ontario score, areas that scored 0 to 39 were considered urban and areas that scored 40 or more were considered rural. 13 Self-reported race and variables describing provincial correctional involvement were obtained from the data set provided by the Ministry of Community Safety and Correctional Services. These categorical variables included the cumulative length of time in custody from all correctional admissions in 3 years prior to the index incarceration, length of the index incarceration event, and the number of prior correctional events in 3 years prior to the index incarceration.
PCP visits were defined as the total number of visits for all reasons for the periods mentioned above. Visits to PCPs were further categorized as mental health–related and non-mental health–related visits based on a validated algorithm using OHIP billing codes. 14 The total number of psychiatry visits were also identified in OHIP billing codes. To differentiate between PCP and psychiatrist visits, the ICES Physician Database was used to identify physician specialties for accuracy. Total hospitalizations and psychiatric hospitalizations were identified in CIHI DAD and OMHRS. The total number of emergency department visits was captured using NACRS. Clinical characteristics of the sample were captured using the ACG® System Collapsed Adjusted Diagnosis Groups (CADGs) from the John Hopkins ACG® System Version 10, which has 12 categories. 15 CADGs were used as a proxy measure of morbidity and have shown good prediction of mortality in the general population 16 and in a population of individuals with a diagnosis of schizophrenia. 17
Statistical Analysis
Health service utilization encounters were calculated for each participant in the 3-year period before the entry date of the index incarceration and in the 5-year period after the index release—defined as the first release in 2010. Health care utilization was also measured during the index incarceration. We examined episodes in custody in the 3 years prior to the entry date of the index incarceration and 5 years after the index event.
The descriptive data were summarized using frequencies and proportions for categorical data and defined based on the data distribution. The distribution of continuous variables was measured using mean (standard deviation) and median (interquartile range) to measure the variations. Cox proportional hazards model was selected as the most appropriate modeling method to reflect our interest in the time to event and to be able to include other covariates in the time to event model. Violation of the Cox PH proportionality assumption was tested using Schoenfeld residuals and time-dependent covariates in the analysis. All analyses were performed in SAS version 9.4 (SAS Institute, Cary, NC). 18
Results
In 2010, there were 51,013 individuals released from Ontario’s provincial correctional facilities. After excluding individuals who were missing information about their location on residence (N = 3,448), missing age variable (
The characteristics of individuals released from correctional facilities with and without schizophrenia are outlined in Table 1. Individuals with schizophrenia were older, more likely to be female, more likely to live in a neighborhood in the lowest neighborhood income quintile, and less likely to reside in rural regions.
Characteristics of Study Cohort, by Schizophrenia Diagnosis.
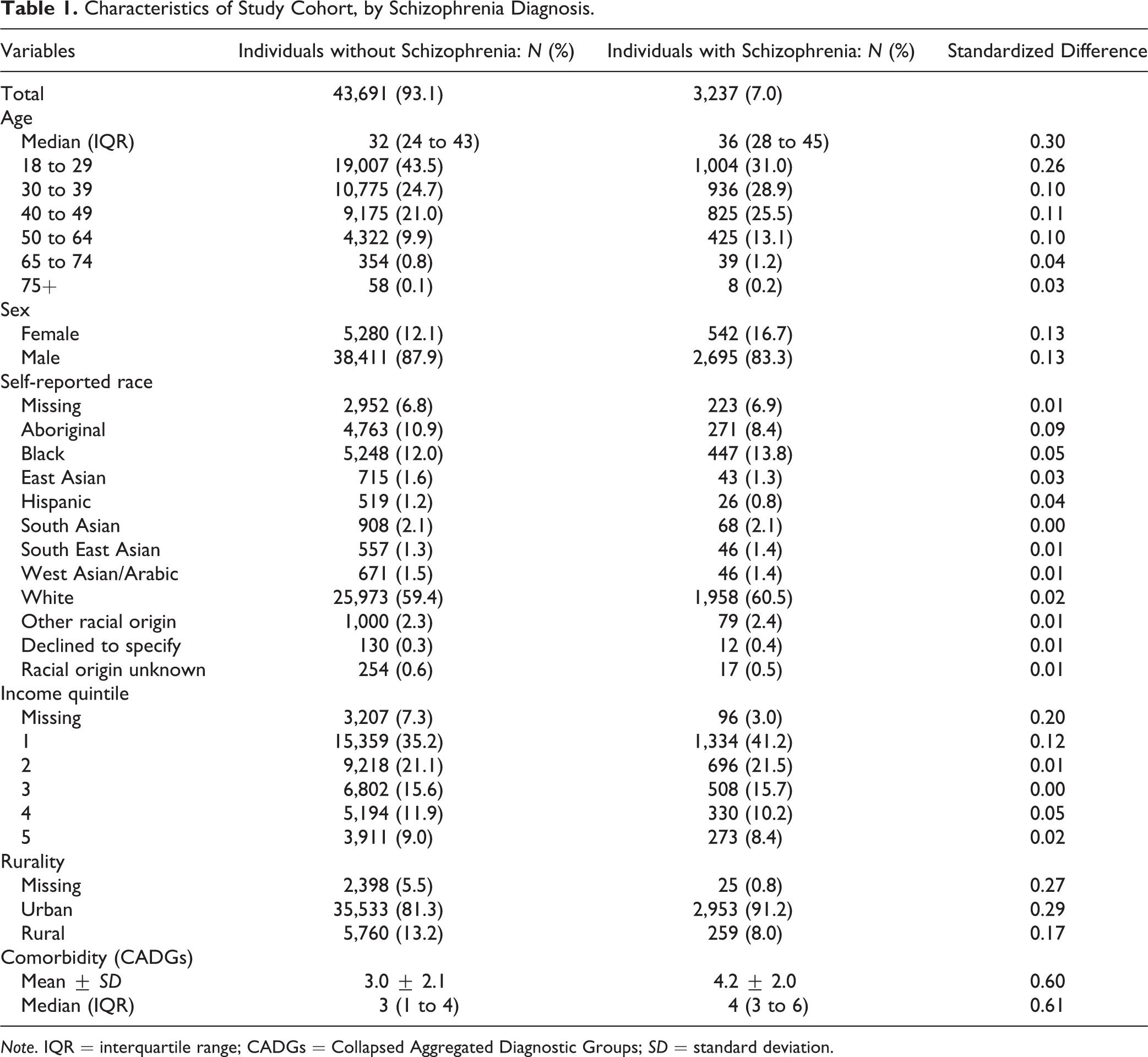
Note. IQR = interquartile range; CADGs = Collapsed Aggregated Diagnostic Groups; SD = standard deviation.
Correctional involvement in the 3 years prior to the index correctional entry date is outlined in Table 2. Individuals with schizophrenia had almost double the median aggregate length of correctional center stay compared to individuals without schizophrenia (66 [IQR: 13 to 176] vs. 38 [IQR: 7 to 123]). The median length of stay of the index event and the number of prior incarcerations were also higher for individuals with schizophrenia. The prior health service utilization is outlined in Supplementary Table 1 and shows higher rates of use of all prior health services measured.
Correctional Involvement 3 Years Prior to the Indexa Incarceration by Schizophrenia Diagnosis.
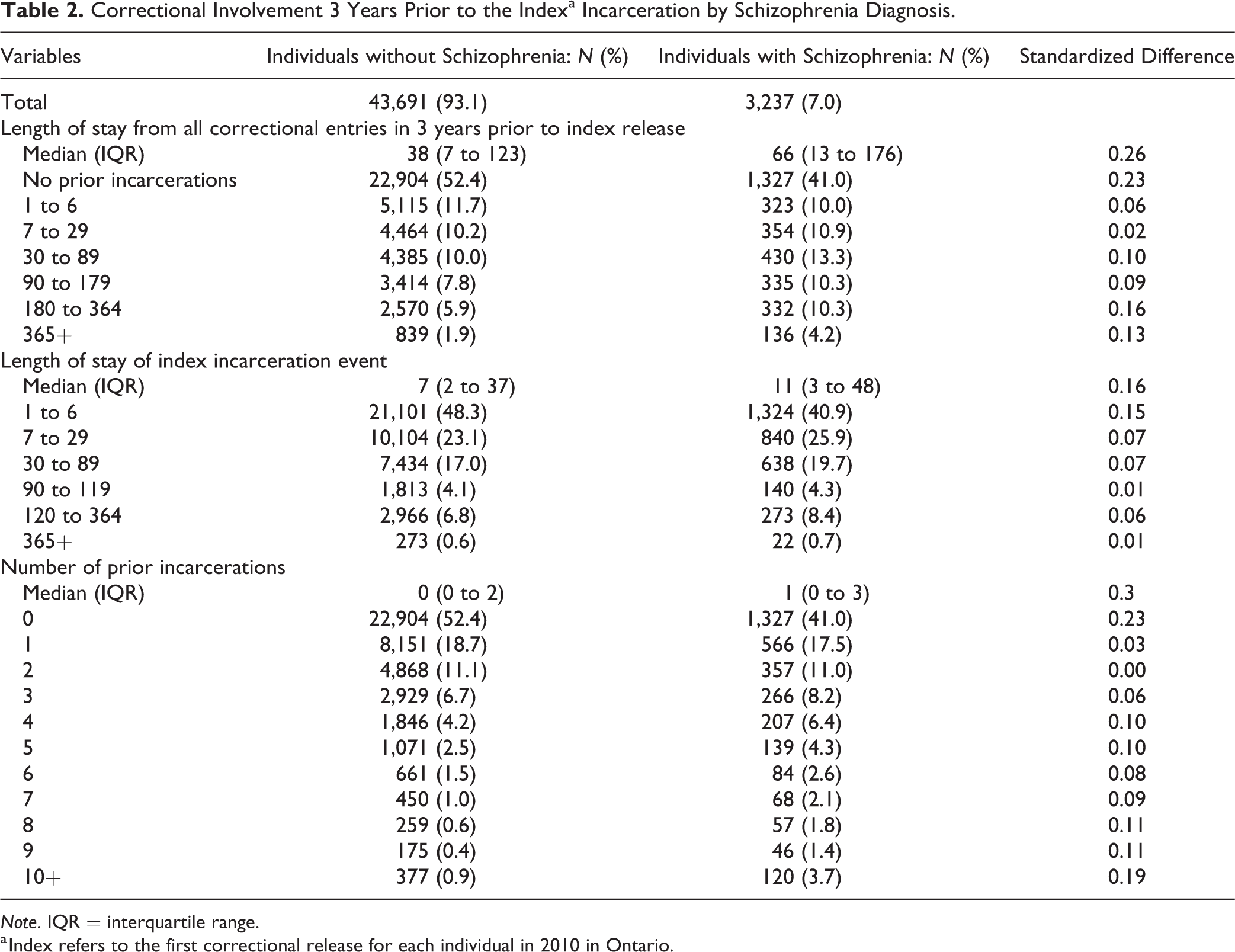
Note. IQR = interquartile range.
a Index refers to the first correctional release for each individual in 2010 in Ontario.
Correctional involvement following index correctional event release date is outlined in Table 3. Slightly more individuals with schizophrenia had at least 1 incarceration event in the 5 years following release than individuals without schizophrenia (67.5% vs. 58.8%). The median time to reincarceration was shorter for individuals with versus without schizophrenia (156 days [IQR 52 to 410] vs. 219 days [IQR 81 to 531]) although total length of time in custody did not differ between the groups.
Correctional Involvement 5 Years after Indexa Release, by Schizophrenia Diagnosis.
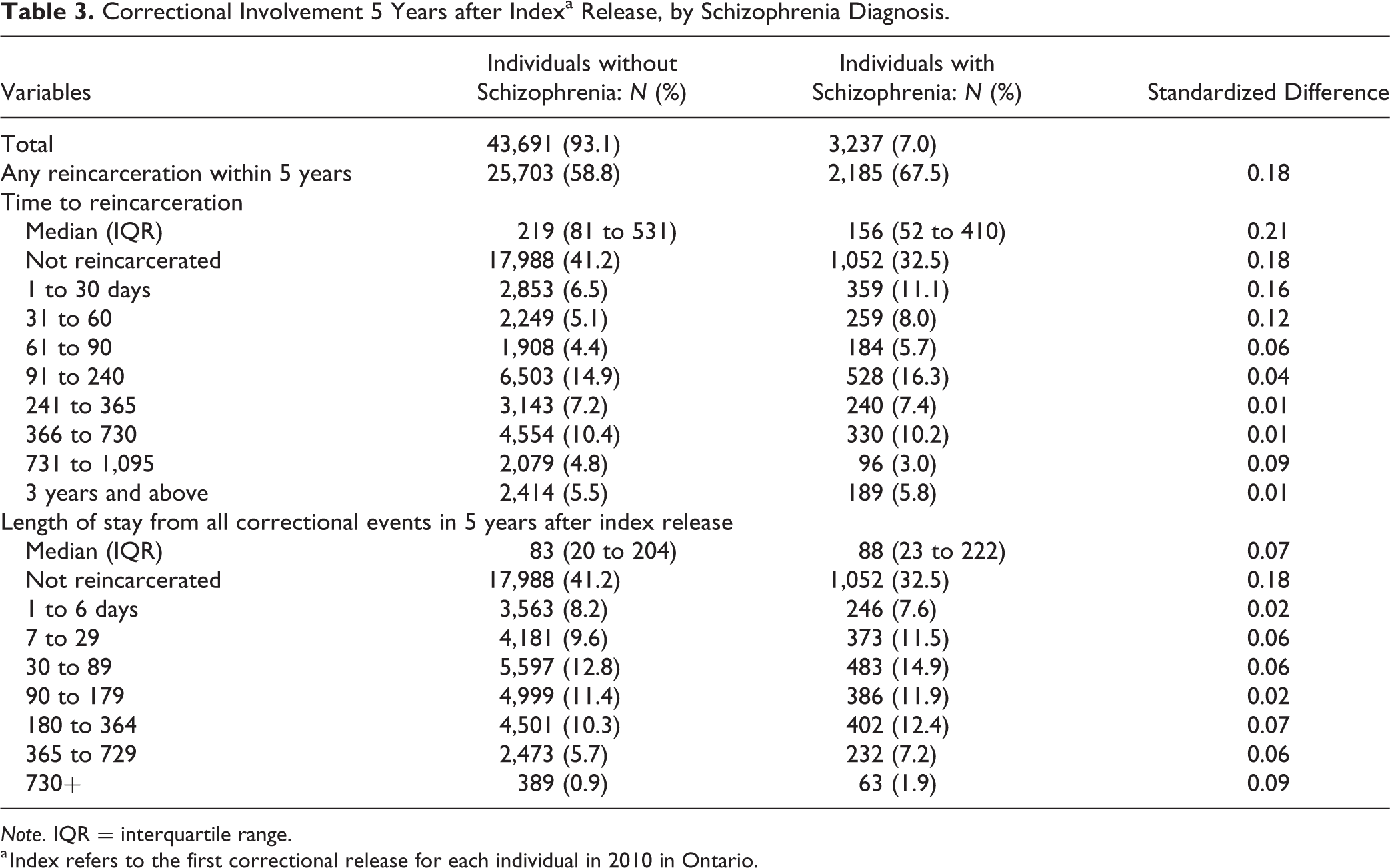
Note. IQR = interquartile range.
a Index refers to the first correctional release for each individual in 2010 in Ontario.
Supplementary Table 2 shows health service utilization in the 5 years following release from correctional centers. As with health service utilization prior to correctional center entry, individuals with schizophrenia had higher rates of all health service utilization in comparison to individuals without schizophrenia; 24% of people with schizophrenia (N = 776) did not see a psychiatrist within 5 years following correctional center release, and the median time postrelease for a person with schizophrenia to see a psychiatrist was 114 days (IQR = 30 to 374).
In a multivariable Cox regression model adjusting for age, sex, neighborhood income quintile, and rurality, individuals with schizophrenia had a 40% increased risk of reincarceration (adjusted HR = 1.39; 95% CI, 1.33 to 1.45; Figure 1A) compared to those without schizophrenia. Further adjusting for prior correctional involvement, comorbidity, and prior health service utilization, individuals with schizophrenia were only at 8% increased risk of reincarceration compared to individuals without schizophrenia (adjusted HR = 1.08; 95% CI, 1.03 to 1.14; Figure 1B).
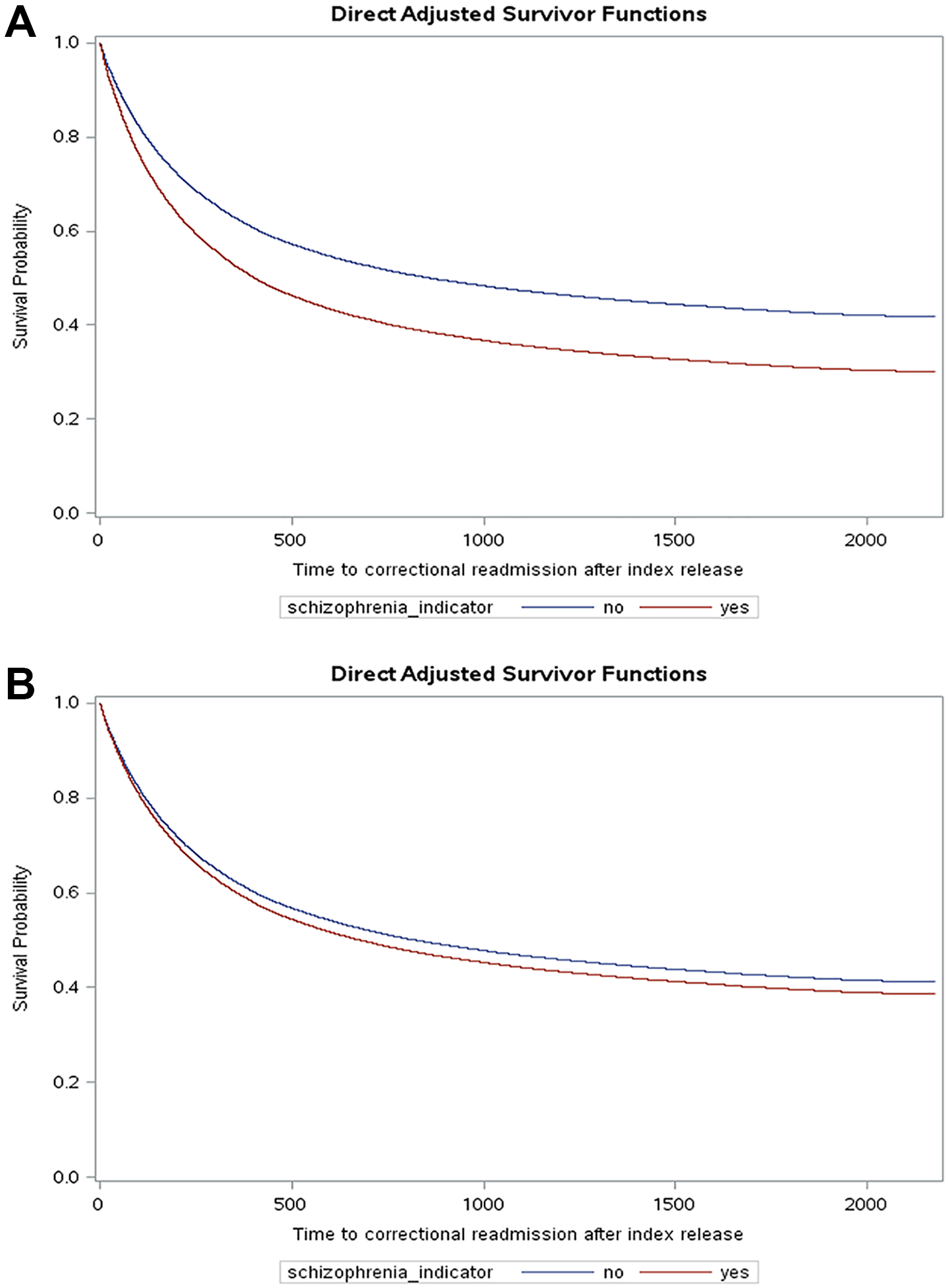
(A) Time to reincarceration for individuals with and without schizophrenia from multivariable cox regression.a aAdjusted for age, sex, neighborhood income quintile and rurality. (B) Recidivism survival curves between individuals with and without schizophrenia.a aAdjusted for age, sex, neighborhood income quintile, rurality, comorbidity, prior correctional involvement, and prior health service utilization.
Discussion
Approximately 1 in 14 individuals (7%) released from provincial correctional facilities in 2010 had a diagnosis of schizophrenia. People with schizophrenia had a higher number of correctional encounters prior to and following release than individuals without schizophrenia and were 40% more likely to be reincarcerated within 5 years following correctional release than individuals without schizophrenia. That this relative increase in reincarceration was substantially attenuated by prior health service utilization, correctional involvement, and comorbidity suggests that these factors may play an important role in reincarceration. That prior correctional involvement is an important contributor is not surprising; however, prior health service utilization may point to opportunities to intervene if individuals with better preincarceration access to care have reduced rates of reincarceration.
We found that individuals with schizophrenia are highly overrepresented in Ontario’s provincial correctional facilities compared to the general population, which is consistent with prior research. 3,19 –23 The schizophrenia prevalence within this cohort was notably high (7%), compared with estimates of schizophrenia prevalence observed in prior studies 3 and in the general population (approximately 1%). 24,25 Our findings that a diagnosis of schizophrenia is associated with a higher rate of reincarceration are also consistent with existing literature. 13,14,26,27
The findings also highlight service fragmentation following the index release in 2010. In the 5 years following release, approximately 1 in 4 individuals with schizophrenia did not see a psychiatrist. Given the complexities associated with support for individuals who have a diagnosis of schizophrenia such as the continuation of antipsychotic medication, the need for other psychosocial interventions such as cognitive behavioral therapy, the need for regular physical health assessments, stable housing, among other socioeconomic supports, 28 timely access to specialty mental health care services, including psychiatrists, quickly following release should be an expected standard of care for individuals with schizophrenia who have had correctional involvement. Indeed, 44% of individuals with schizophrenia had at least 1 psychiatric hospitalization following index correctional event release. Lack of psychiatric care and treatment may contribute to both reincarceration and psychiatric hospitalizations. Indeed, the same factors that create challenges adhering to conditions of release (parole, etc.) likely contribute to challenges attending psychiatric follow-up.
There are several limitations that merit discussion. Given the limited availability of sociodemographic data, we were unable to include largely cited sociodemographic factors including marital status, education level, and housing status. 8,29 –33 Our diagnosis of schizophrenia relies on clinical codes in administrative health data rather than a comprehensive clinical assessment, and there may be misclassification of schizophrenia status. However, the algorithm used to identify individuals with a primary diagnosis of schizophrenia was validated using population-based health administrative databases in Ontario. 11 Finally, the correctional data did not include information on the criminal charges or convictions. Distinguishing whether individuals with schizophrenia within this cohort were incarcerated for violent or nonviolent crimes or for administrative offences such as failing to comply with probation/parole or to attend court appearances could have contributed to the analysis in understanding the length of correctional episodes and whether individuals were receiving the type of care necessary. In addition, this study focused on Ontario’s provincial correctional facilities and did not include data on federal correctional involvement.
Conclusion
Individuals with schizophrenia are overrepresented in correctional facilities in comparison to the general population. Additionally, individuals with schizophrenia experience higher rates of reincarceration. Further work is needed to understand the needs of individuals with schizophrenia and risk factors contributing to reincarceration. However, these individuals would likely benefit from more coordinated and integrated health service delivery following correctional release.
Supplemental Material
Supplemental Material, Scz_Corrections_Supplement_File - Prevalence and Predictors of Reincarceration after Correctional Center Release: A Population-based Comparison of Individuals with and without Schizophrenia in Ontario, Canada: Prévalence et prédicteurs de la réincarcération après la libération d’un centre correctionnel : une comparaison dans la population-de personnes souffrant ou non de schizophrénie en Ontario, Canada
Supplemental Material, Scz_Corrections_Supplement_File for Prevalence and Predictors of Reincarceration after Correctional Center Release: A Population-based Comparison of Individuals with and without Schizophrenia in Ontario, Canada: Prévalence et prédicteurs de la réincarcération après la libération d’un centre correctionnel : une comparaison dans la population-de personnes souffrant ou non de schizophrénie en Ontario, Canada by Mayuri Mahentharan, Fiona G. Kouyoumdjian, Claire de Oliveira, Tomisin Iwajomo, Alexander I. F. Simpson, Roland Jones and Paul Kurdyak in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() . The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification. Parts of this material are based on data and information compiled and provided by: the Ontario Ministry of Health and Long-term Care and the Canadian Institute for Health Information (CIHI). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification. Parts of this material are based on data and information compiled and provided by: the Ontario Ministry of Health and Long-term Care and the Canadian Institute for Health Information (CIHI). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-term Care. This study was funded by a grant from the Canadian Institutes for Health Research.
ORCID iD
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.