
Abstract
Background:
Assessing an individual’s capacity to consent to treatment is a complex and challenging task for psychiatrists and health-care professionals. Diminished capacity to consent to pharmacological treatment is a common concern in individuals with schizophrenia. The MacArthur Competence Assessment Tool for Treatment (MacCAT-T) is the most common tool used in individuals with schizophrenia to evaluate the decision-making abilities for judgments about competence to consent to treatment. This instrument assesses patients’ competence to make treatment decisions by examining their capacities in 4 areas: understanding information relevant to their condition and the recommended treatment, reasoning about the potential risks and benefits of their choices, appreciating the nature of their situation and the consequences of their choices, and expressing a choice. Despite its importance, there is no French version of this scale. Furthermore, its factor structure has never been explored, although validated measures are strongly needed to further detect deficits in patients’ decision-making abilities. The goal of this study was thus to empirically validate a French version of the MacCAT-T in a French sample of individuals with schizophrenia.
Method:
In this cross-sectional study, we included 125 inpatients with a diagnosis of schizophrenia from the University Department of Adult Psychiatry in Montpellier. The MacCAT-T was administered to patients by a trained psychologist. Patients were also assessed for severity of symptoms, insight into illness, and depressive and anxiety symptoms. Inter-rater reliability and psychometric properties including internal consistency, construct validity, and discriminant and divergent validity were also investigated.
Results:
The MacCAT-T’s internal consistency was high (Cronbach α of 0.91). A high degree of inter-rater reliability was found for all the areas of the MacCAT-T (intraclass correlation coefficient range, 0.92 to 0.98). Exploratory factor analysis revealed a 2-factor model. The factor analysis explained 50.03% of the total score variation. Component 1 included all subparts of “understanding.” Component 2 included all subparts of “appreciation” and “reasoning” and was therefore labeled “reflexivity.” After Bonferroni corrections, decision-making capacity was positively associated with insight and the severity of psychotic symptoms but not with sociodemographic variables except for education.
Conclusions:
The MacCAT-T demonstrated a high degree of inter-rater reliability and strong psychometric properties. The French version of the MacCAT-T is a valid instrument to assess the decision-making capacity to consent to treatment in a French sample of individuals with schizophrenia.
Introduction
In the past 40 years, there has been a growing interest in research on capacity to consent to treatment in individuals with mental disorders. This interest is related to the development of laws increasing patients’ protection in health domains and shared decision-making models of treatment planning, putting individuals at the center of decisions regarding their health-care choices. 1 –4 For example, the Canadian Psychiatric Association first published a position paper on “Consent in Psychiatry” in 1980. 5 In England, the Mental Capacity Act, which came into effect in 2007, was designed to enable people with mental illness or learning disabilities to be adequately protected if they cannot make decisions for themselves but also allow them to make their own decisions as much as possible. 3
From a legal point of view, determining one’s competence regarding treatment decisions (i.e., forced treatments against one’s will) is of major importance in a psychiatric context. Many medical professionals and particularly psychiatrists are asked to decide whether a patient who refuses a recommended treatment (e.g., antipsychotic) is competent enough to make decisions regarding their treatment. At the same time, most of the developed countries require that a patient’s wish regarding treatment be respected unless the patient can be shown legally incompetent. Thus, the assessment of patients’ competence to consent to treatment must be established by an appropriate balance between respecting the patient’s autonomy and protecting them from the consequences of a deleterious decision. This ethical and legal position is supported by a large number of studies showing that even if decision-making incapacity is common in mental disorders (median 29%), the majority of psychiatric inpatients are capable of making treatment-related decisions. 6 These points are particularly important for the protection of vulnerable populations where decisional capacities are impaired. Regarding mental disorders, many studies have focused on the ability to consent to treatment in patients with schizophrenia. 7 –13 Indeed, the negative assumption that individuals with schizophrenia do not possess the capacity to make decisions is an opinion largely shared by mental health professionals. 14,15 However, even if, as a group, patients with a diagnosis of schizophrenia perform significantly worse on many measures of decision-making than patients with depression, other mental disorders, or healthy subjects, 7,8 a significant proportion of individuals with schizophrenia have preserved decisional capacity. 9,10,16 As a consequence, diagnosis does not allow clinicians to conclude on the competence or not to consent to treatment. In line with this view, a recent meta-analysis indicated that 48% of inpatients had preserved decision-making capacity for treatment (DMC-T). 11 Rather than psychotic symptoms severity, DMC-T deficits appear largely due to cognitive deficits 12,13 and poor insight, 17,18 and apart from years of education, a recent meta-analysis suggested no evidence for an association with other sociodemographic factors such as age or sex. 11
For the past 20 years, a consensus has emerged concerning the conceptualization of the capacities relevant to competence to consent, including 4 primary elements: the ability to understand relevant information, to assess risk and benefits of potential options, to appreciate the nature or impact of one’s choices, and to express a choice. 19 –21 Based on these criteria, and in order to further standardize and increase the reliability and validity of competence evaluations, Appelbaum and Grisso developed the MacCAT-T. 9,22 The MacCAT-T is a semistructured interview tailored to the patient’s specific disorder and treatment and has been widely used in competence studies in neurological disorders, 23,24 in mental disorders such as depression, 25 anorexia nervosa, 26 and more particularly in individuals with schizophrenia. 10 –13,17,18 The MacCAT-T has been translated in Greek, 27 Spanish, 28 and Chinese, 29 but no validated French version exists to this day. In addition, to our knowledge, and contrary to the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR), 29 the construct validity of the MacCAT-T has not been yet conducted.
Consequently, the aim of the present study was to (1) translate and to test the psychometric properties of the French version of the MacCAT-T in a French sample of individuals with schizophrenia and (2) determine its factorial structure in this clinical population. We expected the MacCAT-T to show good psychometric properties. More precisely, we were interested in inter-rater reliability, internal consistency, construct validity, and discriminant and divergent validity. We also investigated correlations between the MacCAT-T and clinical features (severity of the disease and insight into illness) in a population of patients with schizophrenia.
Methods
Participants
This cross-sectional study consisted of 125 inpatients with a diagnosis of schizophrenia from the University Department of Adult Psychiatry in Montpellier over a 2-year period (September 2015 to September 2017). Inclusion criteria were as follows: (a) age between 18 and 60 years; (b) a diagnosis of schizophrenia according to Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria; (c) to be in a phase of the illness allowing the evaluation according to the current treating psychiatrist, as defined by having no hospitalization or change in housing in the month prior to entering the study; and (d) speak French. Exclusion criteria were as follows: (a) known neurological disease and (b) developmental disability. The institution’s ethics committee approved this study, and after full explanation of the study, signed informed consent was obtained from all participants. The procedures used in these studies were in line with the Declaration of Helsinki in 1975 (revised in 2008) as well as national and institutional ethical committee standards of human experimentation.
Measures
Clinical assessment
For each participant, information was collected related to sociodemographic status, duration of the disease, age at the beginning of the disease, number of hospitalizations, and treatments. Severity of symptoms was evaluated using the Positive and Negative Syndrome Scale (PANSS). 30 The scores derived from this measure and used in the analysis were positive and negative syndrome subscales, general psychopathology, and total scores. A higher score on either scale indicates greater symptom severity. In this study, the scale had good internal consistency (total score, α = 0.77).
Insight into illness was assessed using the first 3 items of the “Scale to Assess Unawareness of Mental Disorder” (SUMD 31 ; French validation, Raffard et al. 32 ), evaluating consciousness of having a mental disorder, of the need of treatment, and of the social consequences of the disease, respectively. Each SUMD item is rated on a 5-point Likert-type scale (1 = conscious; 3 = relatively conscious; 5 = unconscious). In this study, the scale had good internal consistency (total score, α = 0.72).
Level of depressive symptoms was evaluated by the Beck Depression Inventory-II (BDI-II). 33 The BDI-II is a 21-item self-administered questionnaire measuring depressive symptomatology for a total score ranging from 0 (no depressive symptoms) to 63 (major depressive symptomatology). In this study, the scale had good internal consistency (total score, α = 0.92).
Current self-reported anxiety was assessed using the Spielberger State-Trait Anxiety Inventory (STAI). 34 The STAI is a self-administered questionnaire with 2 distinct scales. The “state” scale, correspond to the intensity of anxiety felt at the time of the handover. This subscale contains 20 sentences to which the patient must respond to on a Likert-type scale ranging from 1 to 4 (not at all to very much). For the “trait” scale, the patient is asked to respond by rating the frequency of general anxiety on a Likert-type scale from 1 to 4 (almost never to almost always). In this study, the scale had good internal consistency (α = 0.81)
Capacity to consent to treatment
Capacity to consent to treatment was evaluated using the MacCAT-T 22 : a semistructured interview that includes relevant information from each patient’s chart to evaluate the decision-making abilities for judgments about competence to consent to treatment. The interview always starts with a disclosure of relevant information concerning the disorder (diagnosis, features of the disorder, and course of the disorder), the treatment (name and features of the treatment), and benefits and risks of the treatment. Questions assess understanding, appreciation, and reasoning, and finally, the patient who is interviewed is supposed to offer a clear expression of a treatment choice. “Understanding” is measured by means of 13 items and includes the subscales understanding the “disorder” (5 items), “treatment” (4 items), and “risks” and “benefits” (4 items). To assess this section, the patient is asked to repeat in his or her own words what he or she has comprehended. If there is any sign of poor understanding, the interviewer must redisclose the information and reassess the patient. Two items assess “appreciation” which refers to whether the patient acknowledges that the disclosed information applies to him or her (appreciation of the disorder subscale) and whether he or she recognizes the possible treatment benefits (appreciation of the treatment). Then, 4 items assess “reasoning” that explores whether the person mentions any consequence of the treatment alternatives (consequential thinking), any comparison among alternatives (comparative thinking), and any consequences that were not mentioned in the disclosure (generating consequences). Finally, 1 item assesses “expressing a choice” that occurs when the individual establishes a preference for a treatment option. The MacCAT-T takes approximately 15 to 20 minutes to administer and 2 to 3 minutes to score. Ratings for each item are 2 (adequate), 1 (partially adequate), and 0 (inadequate). There is a quantitative score for each of the 4 abilities: 0 to 6 for understanding, 0 to 4 for appreciation, 0 to 8 for reasoning, and 0 to 2 for expressing a choice. There is no total score for competence, but the evaluators must integrate the results with other relevant clinical information to reach a judgment. The feasibility, reliability, and validity of this instrument have been tested, with excellent inter-rater reliability (κ > 0.80). 22 Intraclass correlations calculated among 3 raters were .99 for understanding, 0.87 for appreciation, 0.91 for reasoning, and 0.97 for expressing a choice. 22
Procedure
The MacCAT-T was adapted into French from the original English version following a precise translation protocol based on international standards. 35 Initially, we contacted the original authors of MacCAT-T and obtained their formal authorization to conduct the adaptation of the instrument to French. Second, the MacCAT-T was translated into French by 2 professional translators, and then, a reconciled version was elaborated by an independent translator, who identified and resolved any possible inadequate expressions or discrepancies between the 2 forward translations. A bilingual expert then translated the French version of the questionnaire into English. To ensure the conceptual equivalence of the translation, a review of the back translation against the original version was practiced. This new back translation was compared to the original version by a panel of experts to verify the equivalence of the 2 English versions in terms of meaning and conceptual content. At this step, we aimed to harmonize across different translations to ensure intertranslation validity. Following the suggestions of the experts, a new version in French was proposed. As a pretest, the new version was applied to 15 participants with schizophrenia disorder according to the DSM-5 criteria to verify its comprehension by our target population. No difficulties were observed in the administration and comprehension of the instrument. The finalized translation was proofread to correct any remaining spelling, diacritical, grammatical, or other errors. Finally, the final version was written.
After patients gave written informed consent, clinical and sociodemographic data were collected during a standard psychiatric interview on an individual basis. The MacCAT-T assessment took place after the regular appointment of the patient with the psychiatrist. The MacCAT-T interview was administered by a trained psychologist who was previously provided with relevant information on the patient by the attending psychiatrist. Inter-rater reliability was assessed with the help of a second trained rater, who was also present during the MacCAT-T assessment, and who simultaneously completed the interviews for 20 patients. Like Owen et al. (2009), 3 we decided not to offer an alternative treatment in order to reduce demands on the patient’s cognitive abilities. Patients were therefore asked to decide for or against antipsychotic treatment (first- or second-generation antipsychotics). The raters of the PANSS and the MacCAT-T received beforehand specialized training (i.e., videotaped interviews with individuals with schizophrenia) in performing the ratings.
Statistical Analyses
All variables were inspected for normality before analysis. The parametric variables were described by their mean, standard deviations, and range. Demographics and clinical variables for the 125 patients with schizophrenia are presented in Table 1.
Demographic and Clinical Characteristics of the Total Sample.
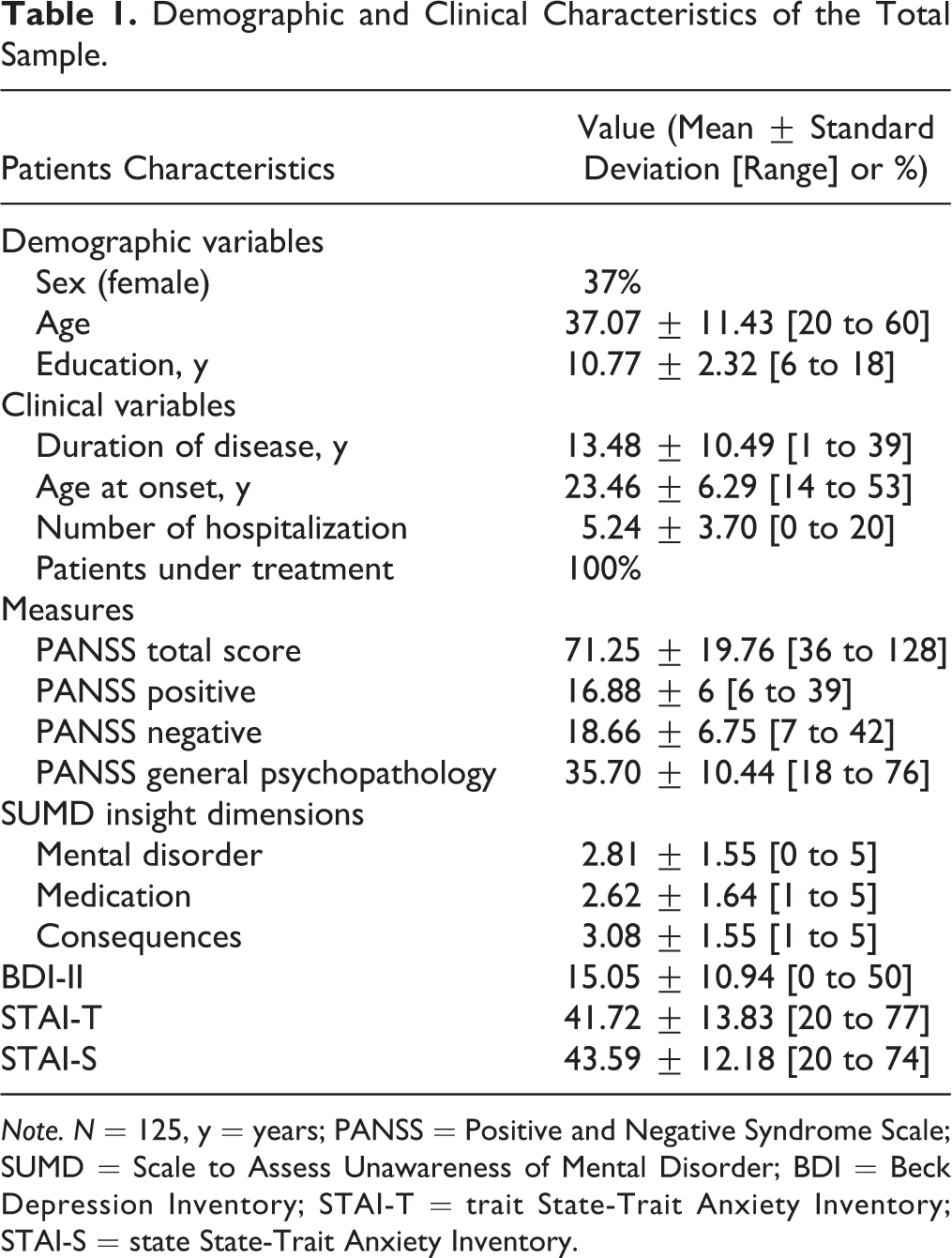
Note. N = 125, y = years; PANSS = Positive and Negative Syndrome Scale; SUMD = Scale to Assess Unawareness of Mental Disorder; BDI = Beck Depression Inventory; STAI-T = trait State-Trait Anxiety Inventory; STAI-S = state State-Trait Anxiety Inventory.
Inter-rater reliability
Inter-rater reliability of the MacCAT-T item scores for the sets of 2 raters was evaluated using weighted κ coefficients. Inter-rater reliability of the MacCAT-T subscale scores was evaluated using intraclass correlations with a 95% confidence interval (CI; 2-way mixed and single measure).
Item Characteristics and Internal Consistency
Item characteristics (means and standard deviations) were calculated, along with corrected item-total correlations for the subscales understanding, reasoning, and the MacCAT-T as a whole. Scale consistency was determined by Cronbach α 36 (good internal consistency was considered 0.7 > α < 0.9, according to Cronbach 36 ).
Construct Validity
An exploratory factor analysis, which excluded the subscale “expressing of a choice,” was conducted to test the construct validity using a principal component analysis with a varimax rotation to investigate the structure of the MacCAT-T. The Kaiser–Meyer–Olkin measure and Bartlett test of sphericity tested the sampling adequacy. As the Kaiser criterion 37 (eigenvalues > 1.0) may result in an overestimation of the number of extracted factors, 38 we used the scree test (i.e., scree plot) and the parallel analysis with a set at 0.01 to determine the number of factors to retain.
Correlations between the MacCAT-T and Clinical Variables
Relationships between the MacCAT-T subscales and clinical variables (severity of the disease, PANSS, insight into illness, and SUMD) were tested using Pearson correlation coefficients.
According to Cohen (1988), 39 a correlation between 0.10 and 0.30 represents a small effect, a correlation between 0.30 and 0.50 a medium effect, and above 0.50 a large effect.
Discriminant Validity
For discriminant validity, patients with schizophrenia were divided into 2 groups according to their scores on the medication dimension of the SUMD, namely a group of patients with high levels of insight into treatment (medication SUMD range: 1 to 2; N = 62) versus a group with poor levels of insight into treatment (medication SUMD range: 3 to 5; N = 63), according to Amador and Strauss (1993). 31 Comparisons of age, gender, and education level as well as the subscale scores of the MacCAT-T were made between the high- and the poor insight groups. An independent t test was applied for continuous variables, whereas a χ2 test was applied for categorical variables. In addition, we calculated Cohen d′ as a measure of the effect size for the difference between patients with high levels of insight into treatment compared with those with poor levels of insight. The effect size was considered small (d′ = 0.2), medium (d′ = 0.5) or large (d′ = 0.8) according to Cohen. 39
Divergent Validity
Divergent validity was investigated examining correlations between the MacCAT-T subscale scores and the measures of depression and anxiety, and the selected demographical variables (i.e., age, gender, and level of education). We also calculated the Cohen d′ as the measure of the effect size. 39 According to Cohen (1988), 39 a correlation between 0.1 and 0.3 represents a small effect, a correlation between 0.3 and 0.5 a medium effect, and above 0.5 a large effect. The data were analyzed using the Statistical Package for the Social Sciences (Version 24.0), with a 2-tailed α level of 5%. We expected the MacCAT-T to show a high degree of inter-rater reliability and good psychometric properties.
Results
MacCAT-T Inter-rater Reliability
To determine the inter-rater reliability of the MacCAT-T, 2 independent raters simultaneously assessed 20 patients (Table 2). The intraclass correlation coefficient for the MacCAT-T total score was 0.98 (95% CI, 0.96 to 0.99); for the understanding subscale, 0.96 (95% CI, 0.92 to 0.98); for the appreciation subscale, 0.92 (95% CI, 0.83 to 0.97); for the reasoning subscale, 0.96 (95% CI, 0.93 to 0.98); and for the expressing a choice subscale, 1 (95% CI, 1 to 1). Weighted κ values for individual items ranged from 0.40 (Item 10) to 1 (Items 1, 13, and 20).
Inter-rater Reliability and Internal Consistency of MacCAT-T Item and Subscale Scores.
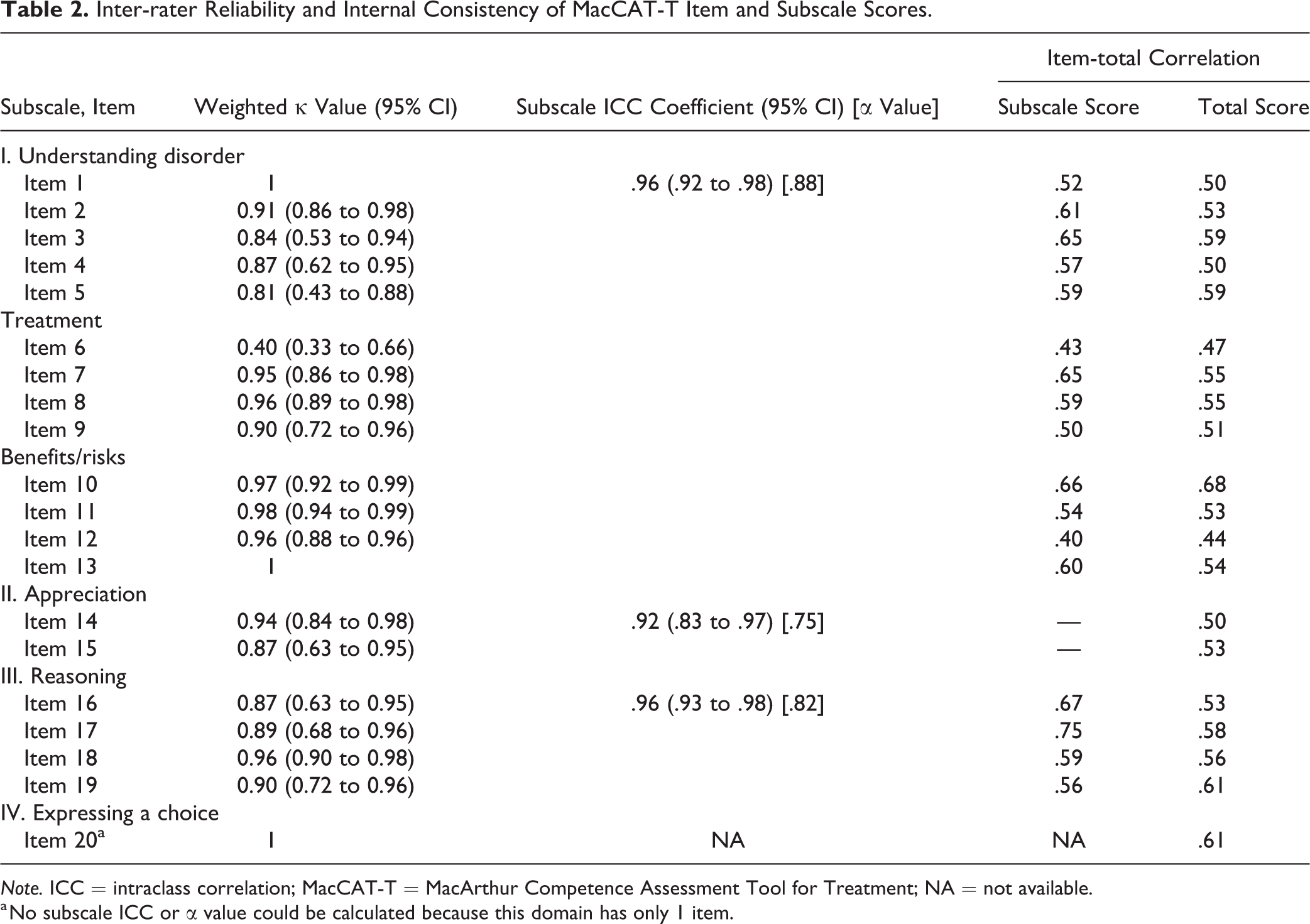
Note. ICC = intraclass correlation; MacCAT-T = MacArthur Competence Assessment Tool for Treatment; NA = not available.
a No subscale ICC or α value could be calculated because this domain has only 1 item.
Item characteristics and internal consistency
Item characteristics (means and standard deviations) are presented in Table 3. The Cronbach α for the total MacCAT-T scale was 0.91. Corrected item-total correlations score ranged from 0.44 to 0.68 (median, 0.54; Table 2). The Cronbach α values for the subscales (understanding, 0.88; appreciation, 0.75; and reasoning, 0.82) indicated good internal consistency (Table 2).
Factor Analysis and Item Statistics of the MacCAT-T of Patients with Schizophrenia.
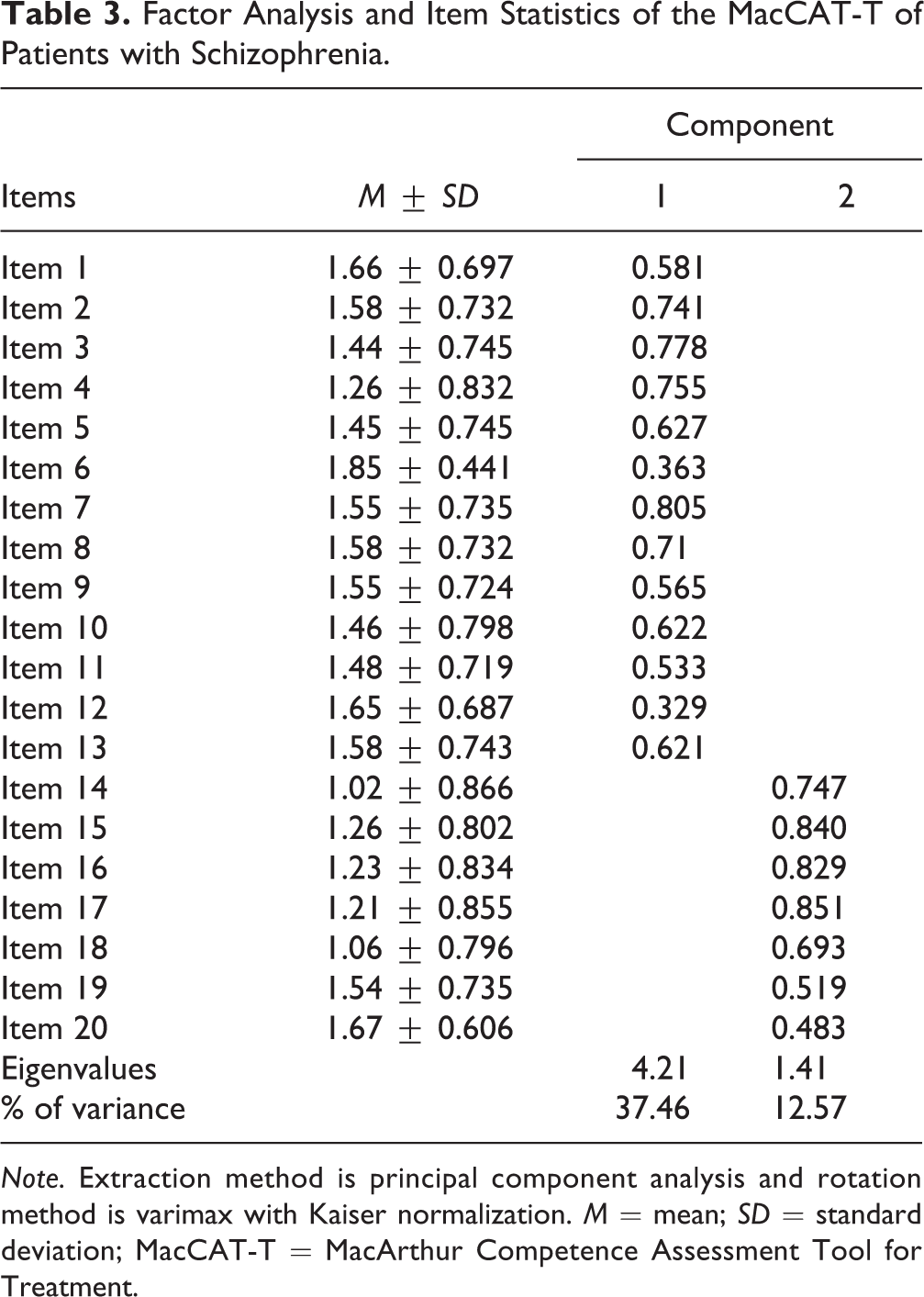
Note. Extraction method is principal component analysis and rotation method is varimax with Kaiser normalization. M = mean; SD = standard deviation; MacCAT-T = MacArthur Competence Assessment Tool for Treatment.
Construct Validity
The sample size for the factor analysis was 125 participants and 20 items. A ratio of 6.25 respondents for each item was obtained, which, according to several recommendations, 40 –45 is suitable for the factor analysis. The Kaiser–Meyer–Olkin measure of sampling adequation was 0.85, suggesting that the sample size is suitable and Bartlett test of sphericity was significant (P < 0.001), indicating adequation of the data for conducting exploratory factor analysis. Factor analysis showed that 2 components had an eigenvalue greater than 1, namely 4.21 and 1.41, explaining 50.03% of the total score variation. Factor loadings ranged from 0.32 to 0.85. The remaining 17 factors each explained 0.6% to 7% of the total variation. Examination of the scree plot and parallel analysis confirmed the 2 extracted factors (see Figure 1). Each extracted component from the factor analysis exceeded the corresponding mean random data set eigenvalue at the 99th percentile (Component 1, 7.40 vs. 1.95; Component 2, 2.23 vs. 1.74). The next factors were not supported. Component loadings and item statistics are presented in Table 3. Component 1 included all subparts of understanding. Component 2 included all subparts of appreciation and reasoning and was therefore labeled “reflexivity” because it contains items related to the fact of being able to apply the information abstractly understood to his or her own situation and to engage in logical processes in arriving to a decision.
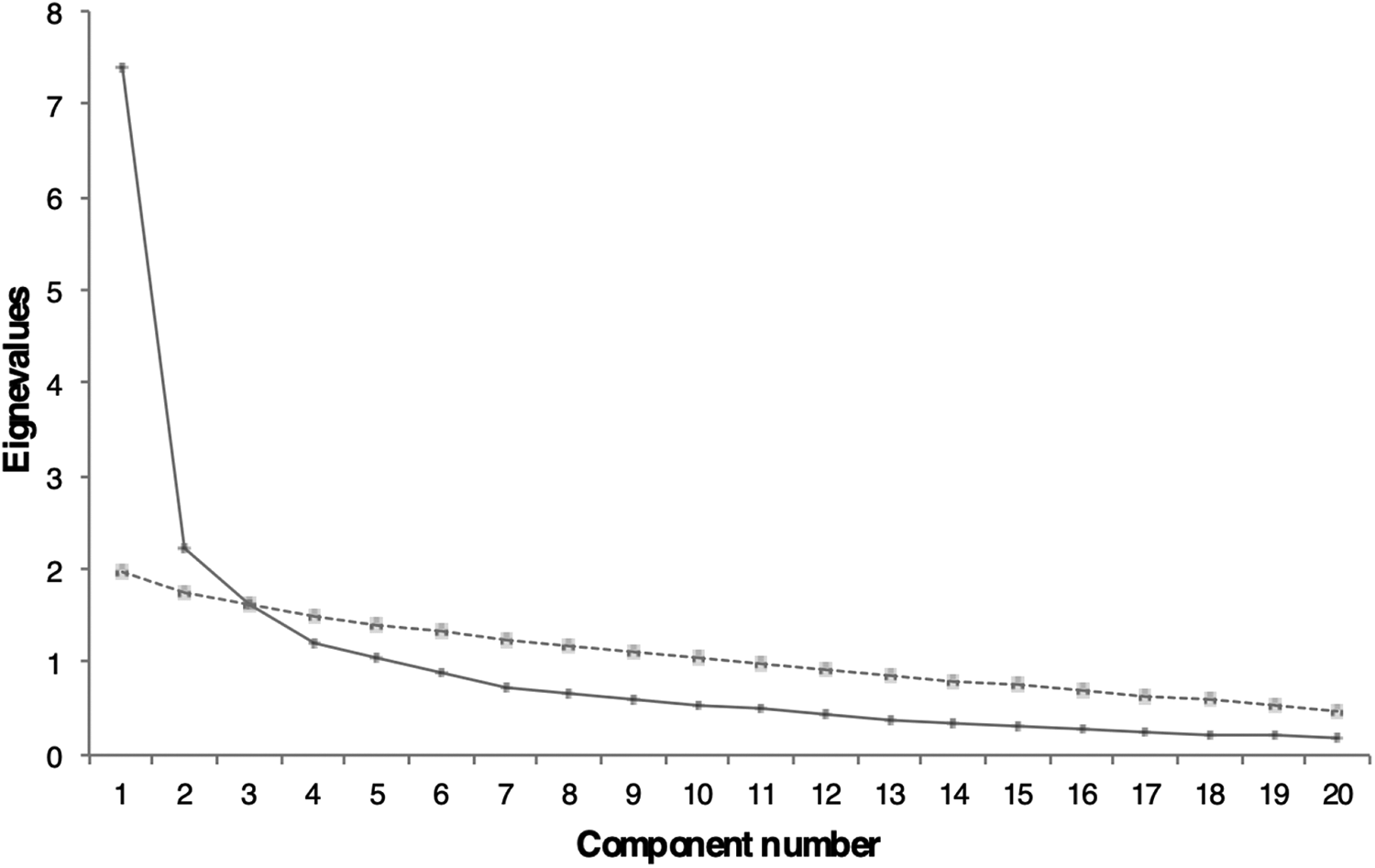
Scree plot and parallel analysis of eigenvalues for the MacArthur Competence Assessment Tool for Treatment components.
Correlation between the MacCAT-T and Clinical Variables
Table 4 shows that the scores of the MacCAT-T subscale understanding were negatively correlated with PANSS positive (r = −0.45), general psychopathology (r = −0.40), and total scores (r = −0.44). The size of these effects was medium. SUMD subscales scores were all positively correlated with scores of appreciation (SUMD mental disorder: r = −0.72; SUMD medication: r = −0.62; SUMD consequences: r = −0.54) and reasoning (SUMD mental disorder: r = −0.57; SUMD medication: r = −0.48; SUMD consequences: r = −0.56). The size of these effects was medium to large. Low and negative correlation was noted between the understanding subscale and the mental disorder subscale scores of the SUMD (r = −0.29). Finally, scores on the expressing a choice subscale was moderately and negatively associated with mental disorder (r = −0.30) and consequences SUMD subscales (r = −0.34).
Correlation Coefficients among the MacCAT-T Scores and Other Outcomes.
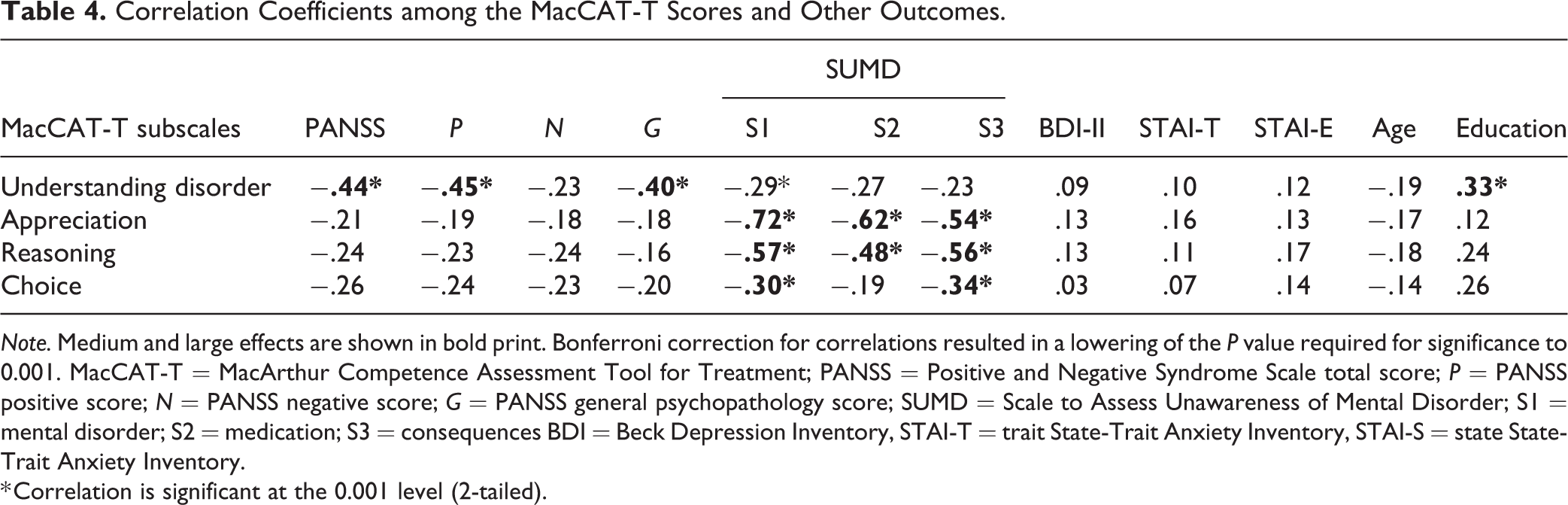
Note. Medium and large effects are shown in bold print. Bonferroni correction for correlations resulted in a lowering of the P value required for significance to 0.001. MacCAT-T = MacArthur Competence Assessment Tool for Treatment; PANSS = Positive and Negative Syndrome Scale total score; P = PANSS positive score; N = PANSS negative score; G = PANSS general psychopathology score; SUMD = Scale to Assess Unawareness of Mental Disorder; S1 = mental disorder; S2 = medication; S3 = consequences BDI = Beck Depression Inventory, STAI-T = trait State-Trait Anxiety Inventory, STAI-S = state State-Trait Anxiety Inventory.
* Correlation is significant at the 0.001 level (2-tailed).
Discriminant Validity
On MacCAT-T, patients with high levels of insight into treatment reported higher scores on the understanding, 5.04 ± 1.11 versus 4.26 ± 1.54, t(123) = −3.20, P = 0.002, d′ = 0.58; appreciation, 3.19 ± 1.05 versus 1.38 ± 1.31, t(123) = −8.50, P < 0.001, d′ = 1.52; reasoning, 6.18 ± 1.90 versus 3.92 ± 2.67, t(123) = −5.35, P < 0.001, d′ = 0.97; and expressing a choice subscales, 1.81 ± 0.47 versus 1.54 ± 0.69, t(123) = −2.51, P = 0.013, d′ = 0.45, than those with poor levels of insight into treatment. The size of these effects was medium to large. Note that patients with high levels of insight did not significantly differ from patients with low levels of insight regarding age, 36.58 ± 10.67 versus 37.54 ± 12.12, t(123) = 0.46, P = 0.64; gender, 28.5% versus 32.2% females, χ2(1, N = 125) = 0.20, P = 0.65, and level of education, 11.16 ± 2.48 versus 10.51 ± 2.29, t(123) = −1.52, P = 0.12).
Divergent Validity
To investigate the divergent validity, the MacCAT-T subscale scores were associated with measures of depression and anxiety and selected demographical variables (Table 4). No association was found between the MacCAT-T subscale scores and measures of depression and anxiety. Likewise, no association was reported between age and scores on all the MacCAT-T subscales. Only level of education was associated with the understanding subscale (r = 0.33). The size of this effect was medium. There were no differences between women and men on all the MacCAT-T subscale scores, understanding, 4.70 ± 1.34 versus 4.53 ± 1.52, t(123) = 0.59, P = 0.55; appreciation, 2.31 ± 1.55 versus 2.21 ± 1.35, t(123) = 0.34, P = 0.73; reasoning, 5.15 ± 2.52 versus 4.79 ± 2.80, t(123) = 0.70, P = 0.47; and expressing a choice, 1.69 ± 0.57 versus 1.63 ± 0.67, t(123) = 0.49, P = 0.62.
Discussion
The main purpose of this study was to assess the psychometric properties of a French version of the MacCAT-T for use with individuals with schizophrenia. In addition, and to the best of our knowledge, this is the first article reporting on the MacCAT-T factor structure in individuals with schizophrenia.
Our study including 125 individuals with schizophrenia showed that the French version of the MacCAT-T has adequate inter-rater reliability (from 0.92 to 0.98) and high internal consistency (Cronbach α total score was 0.91). These findings are in accordance with the original English- 9 and other language versions of the scale (i.e. Greek, Spanish, and Chinese). 27 –29 In addition, significant group differences in the subscales understanding, appreciation, reasoning, and expressing a choice of the MacCAT-T between participants with high levels of insight into treatment versus low levels of insight into treatment suggested good discriminant-related validity. Specifically, schizophrenia patients with high levels of insight into treatment showed greater performances in all aspects of capacity to consent than patients with low levels of insight into treatment. At a subscale level, the greatest differences between groups were found in items that measured appreciation and reasoning. These results are in accordance with the meta-analysis of Spencer et al., 11 reporting that impaired decision-making has been linked with lack of insight in other studies.
Results from the exploratory factor analysis provided empirical support for a conceptual distinction between lower and higher cognitive processes underlying decision-making capacity processes in schizophrenia patients. First, 1 component emerged and included all subparts of understanding, referring to the ability to repeat/describe the treatment and the main symptoms of the disease to the clinician. Indeed, during the evaluation of the understanding dimension in the MacCAT-T, the patient is simply asked to repeat in his own words what he or she has comprehended about the information given to him or her by the clinician (e.g., “now explain with your own words what I told you about your disease…or your treatment”). Understanding therefore refers to the lower cognitive element of decision-making capacity. Second, a component that we named reflexivity, including all subparts of appreciation and reasoning, was extracted, suggesting that patients who rate high on this component are aware of having a mental disorder and capable to deduce the consequences of the recommended treatment. Indeed, the dimension appreciation is considered positive if the patient recognizes the disorder and its symptoms or the benefits he or she can have which are expected to result from treatment. Moreover, to evaluate different aspects of reasoning, the ability of the patient to name consequences of the treatment choice, to compare alternatives, and to anticipate consequences on his or her everyday life is evaluated. As suggested by Appelbaum & Grisso, 19 capacity to consent to a treatment requires to understand, reason, and act on the key elements of informed consent presented to an individual. This more complex mental processing is likely to become more difficult as cognitive and self-reflexivity deficits emerge. In agreement with this statement, Raffard et al. 18 found a strong positive relationship between the dimension “Self-reflectiveness” of the Beck Cognitive Insight Scale 46 and the subscore reasoning of the MacCAT-T. By consequences, it can be suggested from the results of our factor analysis that both understanding and reflexivity are the 2 major dimensions of DMC-T in individuals with schizophrenia. Interestingly, the factor structure of the MacCAT-T is closely related to the 2-dimensional structure of the MacCAT-CR found by Lan et al. 29 Their factor analysis found 2 components explaining 42.8% and 13.6% of the variance, respectively. The first component (labeled by the authors “Component 1”) included all subparts of understanding and appreciation, whereas Component 2 included all subparts of reasoning. In our factor analysis, appreciation, contrary to Lan et al. 29 belongs to the dimension reflexivity. The MacCAT-CR is directly derived from the MacCAT-T and was similarly structured according to the 4 components of decision-making capacity described in the MacCAT-T, that is, understanding, appreciation, reasoning, and the ability to express a choice. Whereas MacCAT-T administration involves disclosure about treatment, Mac-CAT-CR administration involves disclosure of information about the study that subjects are being asked to consider (i.e., nature of project, possibility of withdrawal, effects of individual care, comparative reasoning). However, the dimension appreciation of the MacCAT-T is closely linked to the concept of awareness of having a mental disorder (insight), which is not the case in the Mac-CAT-CR, the latter corresponding to an appreciation of the effects of participation to a given research (e.g., possibility of withdrawal, personal benefit from study).
With regard to symptoms of psychosis and decision-making capacity, correlations, with medium effect sizes, were found between positive, general psychopathology, and severity of overall psychotic symptoms and the subscale understanding. These associations are partly in accordance with the meta-analysis of Spencer et al., 11 who found some evidence for a negative association of PANSS total symptoms and PANSS negative symptoms with understanding but little evidence for a possible negative association of PANSS positive symptoms with dimension scores. Potential confounding factors such as cognition, an important factor associated with capacity to consent 11 but which was not assessed in our study, could explain such discrepancies. From a clinical perspective, these findings suggest that the severity of symptoms may however affect the ability of the patient to participate in shared decision-making and consequently must be taken into account when choosing the moment to assess the decision-making capacities in an individual with schizophrenia.
Regarding the relationships between patients’ treatment decision-making capacity and sociodemographic and affective characteristics, we initially detected several small associations between age, duration of illness, years of education, and the different subscales of the MacCAT-T. However, these significant results all disappeared after Bonferroni corrections apart for a positive association with moderate effect size between education and the subscale understanding. These results are in accordance with the 2 meta-analyses existing on this subject, 11,47 giving additional evidence for a lack of association between decision-making capacities and sociodemographic factors.
Conclusion
To our knowledge, our study is the first to explore the factorial structure of the MacCAT-T in a sample of schizophrenia patients from France. Statistical analyses indicated that the French version of the MacCAT-T is a valid instrument that can provide a standardized measure for assessing treatment decision capacity in French-speaking patients from France.
Our exploratory factorial analysis revealed a 2-factor structure including a dimension understanding and a dimension labeled reflexivity. Regarding the clinical determinants of competence to consent to an antipsychotic treatment, insight and severity of psychotic symptoms, rather than sociodemographic variables, were most closely associated with decision-making capacity in our sample.
The results of this study must be interpreted within the context of its limitations. First, the sample size of the included participants in the study was relatively small particularly in the sample used to establish inter-rater reliability. Second, no measures of cognition were included in our study whereas cognitive performance is central to the MacCAT-T assessment of mental capacity. Third, we compared antipsychotic treatment to no pharmacological treatment and did not ask patients to decide about an alternative treatment. Future research could conduct a study comparing antipsychotic treatment to a psychological treatment such as cognitive behavioral therapy for reducing positive symptoms. 48 Finally, even if our study is the first to explore the structure of the MacCAT-T in individuals with schizophrenia, confirmatory factor analysis is needed to confirm its 2-factor structure.
Footnotes
Acknowledgment
We sincerely acknowledge all the participants of this study and Dr. Florian Garcia for his support and help in executing this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.