
Abstract
Objective:
In some Australian states clinicians and mental health tribunal members are already required to assess a person’s decision-making capacity before involuntary treatment can be applied. Professionals in other jurisdictions will likely soon be required to do the same as mental health law reform in most Australian jurisdictions makes the assessment of decision-making capacity a central component of the process of providing unconsented psychiatric treatment. We provide a guide to the legal issues around the capacity to refuse psychiatric treatment to assist with this task.
Method:
We review the legislation in the four Australian states most advanced in the mental health law reform process and use examples from clinical practice and the common law to describe how decision-making capacity should be assessed by these statutory standards.
Results:
Clinicians and tribunal members will primarily be required to judge whether a person with mental illness can understand the information relevant to the treatment decision and whether he or she can use or weigh that information to come to a decision. A person with a mental illness is presumed to have capacity, but that presumption can be rebutted. Capacity is specific to the decision at hand and cannot be determined by the nature of the decision made.
Conclusions:
The information provided should assist clinicians and tribunal members to make determinations of decision-making capacity around treatment refusal in the context of mental illness.
Introduction
In four Australian states – Tasmania, Victoria, Western Australia and New South Wales – reformed mental health legislation either currently, or will soon, require clinicians to make an assessment of a patient’s decision-making capacity as a part of ordering involuntary treatment. This paper focuses on the law in these jurisdictions where new mental health legislation was either commenced, or passed through parliament, in 2014 (Mental Health Act 2013 (Tas); Mental Health Act 2014 (Vic); Mental Health Act 2013 (WA); Mental Health Amendment (Statutory Review) Act 2014 (NSW)). 1 Other states and territories have drafted bills that contain similar reforms (Mental Health (Treatment and Care) Amendment Bill 2014 (ACT); Mental Health Bill 2014 (Qld)). Regardless of any jurisdiction’s current legal requirements, the assessment of decision-making capacity is a vital skill for all mental health professionals, with important legal and human rights implications (Callaghan and Ryan, 2014; Ryan et al., 2015).
In the Tasmanian and Western Australian legislation involuntary treatment orders cannot be made if the person retains decision-making capacity (Mental Health Act 2013 (Tas) s 40(e); Mental Health Act 2013 (WA) s 25(1)(c)). In Victoria involuntary treatment of a person with decision-making capacity will only be possible if a number of stringent conditions are met (Mental Health Act 2014 (Vic) ss 70, 71) and should only occur in very unusual circumstances. In Tasmania, Western Australian and Victoria the clinician’s original assessment of the patient’s decision-making capacity must be confirmed by an independent Tribunal or Board. In New South Wales the amended Mental Health Act 2007 has a subsection added to the ‘principles of care and treatment’ providing that ‘every effort that is reasonably practicable should be made to obtain the consent of people with a mental illness or mental disorder when developing treatment plans and recovery plans for their care, to monitor their capacity to consent and to support people who lack that capacity to understand treatment plans and recovery plans’ (Mental Health Act 2007 (NSW) (as amended 2014) sub-s 68(h1)). Arguably this addition should, like the Victorian reforms, mean that involuntary treatment of a person with decision-making capacity will only be possible in unusual circumstances.
While psychiatrists in Victoria and Western Australia have been required to assess decision-making capacity as part of the process of ordering involuntary treatment for some time (Mental Health Act 1986 (Vic) s 8(1)(d); Mental Health Act 1996 (WA) s 26(1)(c)), the ability to give unconsented treatment was not contingent on the result of these assessments. These recent legislative changes make capacity assessment far more important in determining whether or not involuntary treatment can be given at all. It seems increasingly likely that similar reforms will eventually come into place in all Australasian jurisdictions (Callaghan and Ryan, 2012).
In this paper, we aim to provide an analysis of how a patient’s decision-making capacity, or competence (we will use the terms interchangeably), to make decisions about psychiatric admission or treatment is to be understood under these new laws. We hope that this information will be useful, not only to clinicians, but also to legal and lay members of mental health tribunals. To achieve this aim, we review the provisions of the new statutes, attempt to interpret their meaning, and suggest approaches to patient assessment that are likely to assist in meeting their demands.
Determining capacity under the new mental health legislation
Tasmania, Victoria and Western Australia have framed the provisions concerning decision-making capacity around established common law principles governing refusal of medical treatment (see Table 1). The reformed New South Wales legislation contains no specific definition of ‘capacity’ so the courts will interpret the term with reference to the common law. These common law principles are clearly outlined in the lead Australian case in this area – Hunter and New England Area Health Service v A [2009] NSWSC 761 (‘Hunter’). As a consequence of these arrangements, the tests for capacity will vary slightly across the jurisdictions, but in all four, for a person to be regarded as having lost decision-making capacity for a particular decision, he or she must be determined to be unable to do one or more of the following:
understand the information relevant to the decision;
‘use or weigh’, or in Western Australia ‘weigh up’, that information as part of the process of making the decision;
communicate the decision.
Criteria for determination of decision-making capacity.
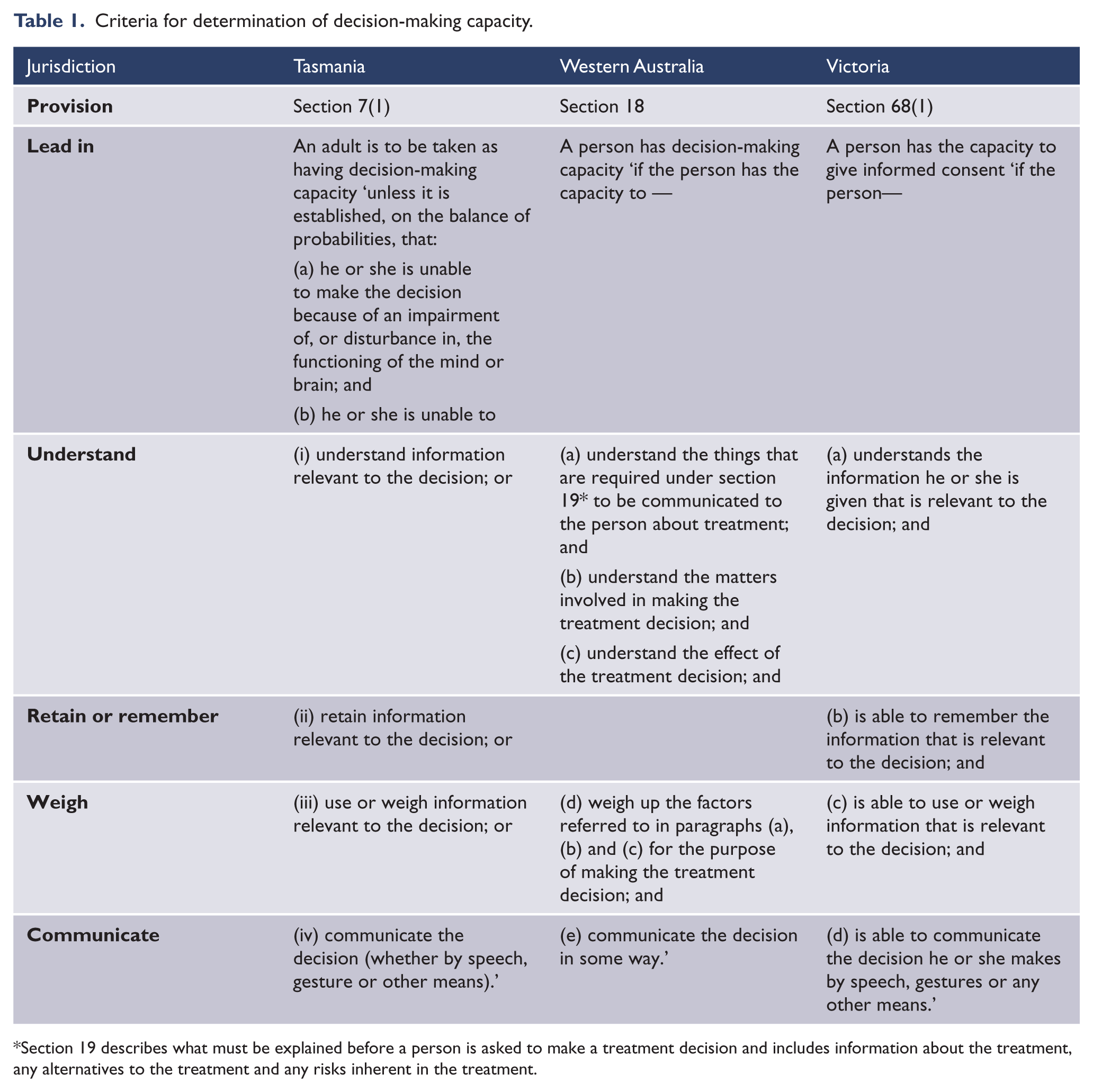
Section 19 describes what must be explained before a person is asked to make a treatment decision and includes information about the treatment, any alternatives to the treatment and any risks inherent in the treatment.
In addition to these, in Tasmania it is explicitly stated that any incapacity must be as a result of ‘impairment of, or disturbance in, the functioning of the mind or brain’; and in Tasmania and Victoria, though not Western Australia, it is explicitly required that the person must be able to retain or remember the relevant information. In Victoria the new legislation explicitly notes that a determination that a person does not have the capacity to make a decision should not be made only because the person makes a decision that could be considered to be unwise (Mental Health Act 2014 (Vic) s 68(2)(d)). In all the new legislation, a person’s capacity to make a decision is specific to the decision to be made, and in Victoria, the legislation expressly notes that decision-making capacity may change over time (Mental Health Act 2014 (Vic) s 68(2)(a), (b)). In all four jurisdictions adults are presumed to have decision-making capacity (Mental Health Act 2013 (Tas) s 7; Mental Health Act 2013 (WA) s 13; Mental Health Act 2014 (Vic) s 70), but this presumption may be rebutted.
We will examine each of these elements separately, exploring how each might be tested in clinical practice or examined in a hearing.
A determination on decision-making capacity cannot be made solely from the nature of the decision made
Our society places a very high value on individual autonomy and on allowing people the freedom to chart their own course in life. Generally speaking, we believe, that if people want to follow a particular path, they should be able to, as long as they are not harming others in doing so (Mill, 1859). We do not usually restrict people’s choices merely because we feel that the decisions made are foolish or unwise.
When it comes to the refusal of medical treatment, the common law has reflected society’s view and strongly protected the right to autonomy. Numerous decisions have held that the right of a competent individual to refuse treatment is protected even if the decision is ‘not sensible, rational or well considered’ (Hunter [2009] NSWSC 761, [10]; Re T (Adult: Refusal of Treatment) [1992] EWCA Civ 18 (‘Re T’)) and even if the refusal will likely lead to death or serious injury (Hunter [2009] NSWSC 761, [11]; Re T [1992] EWCA Civ 18).
Therefore, while a seemingly unwise decision may form part of a rationale to begin to question whether a person has decision-making capacity, the nature of the decision, on its own, cannot be determinative of the issue of competence. The assessment of decision-making capacity involves an assessment of the person’s ability to undertake the process of coming to the decision, not the quality or worth of the decision itself.
Consider, for example, a person who has frequently attempted suicide in the context of severe recurrent major depression. It could easily be argued that it would be wisest for that person to continue antidepressants in the long term so as to make further relapse less likely. Nonetheless, if, when well, that person decides to cease his medication, the apparent foolishness of this decision is not determinative of whether or not he has the capacity to make this decision, even if the treating team feel that such a cessation might ultimately place his life in danger.
Decision-making capacity is decision- and time-specific
The common law and the capacity tests in the new legislation are clear that decision-making capacity is only relevant to the person’s ability to make a particular decision (or closely related set of decisions). That means that a person should not be assessed as lacking capacity in a global sense, or in relation to all decisions. For example, a patient with acute mania may not have capacity to refuse a mood stabiliser because her euphoria may seriously impair her ability to consider the benefits of that class of drugs. Nonetheless, she may still have capacity to choose between mood stabilisers based on an understanding of their varying side effect profiles.
Similarly, an examination of decision-making capacity is only relevant to the person’s ability to make a decision at the time the assessment is made (Kerridge et al., 2013). As a consequence the assessment may only be valid for a limited period, depending on the reason for the incapacity.
It is likely that many people who are, or were, treated under the more traditional mental acts had community treatment orders (CTOs) made after they had regained decision-making capacity following the resolution of an acute episode of illness (Skipworth et al., 2013). Since tribunals will now be concerned with a person’s capacity at the time an order is made, it is likely that considerably fewer people will be able to be compelled to undergo community treatment under the new legislative schemes.
A presumption of capacity
Like the common law, the new mental health acts all contain a presumption that an adult patient has decision-making capacity. This gives rise to two questions: when should capacity be tested? and what should be done if a person refuses to cooperate with a capacity assessment?
The Tasmanian, Victorian and Western Australian statutes all set out a procedure for detaining persons for the purposes of assessment for involuntary admission, including capacity testing. In some Acts the threshold for provisional detention is different for assessors with different levels of expertise, such as doctors, mental health professionals and police officers, and the thresholds vary considerably between jurisdictions. For example, Table 2 sets out the criteria for apprehension as they apply to police officers across those three jurisdictions. The threshold for police in Victoria is significantly higher than in Tasmanian or Western Australia.
Criteria for detention by police.

In any case, capacity assessment should only occur where it seems necessary to do so for some particular reason. While, a treatment refusal might at least raise some consideration of the person’s capacity in the doctor’s mind (Re T [1992] EWCA Civ 18, [28]), neither the mere presence of a mental illness nor a simple refusal of treatment, would normally be sufficient grounds to initiate a formal test. That said, there remains some controversy about when exactly a capacity assessment should be undertaken for the purposes of authorising involuntary treatment (Victorian Law Reform Commission, 2012: [7.105]). We suggest that a capacity assessment should be made where a person appears to have a form of mental illness that is likely to impair his or her decision-making capacity, and where that person appears to be making a decision that may entail serious adverse effects, such as significant suffering, loss of property, failure to provide for the necessitates of life, serious illness or injury, violent or self-harming behaviour, or choices that seem inconsistent with the person’s usual values, wishes and preferences (Callaghan and Ryan, 2014).
Incapacity must be due to ‘an impairment of, or disturbance in, the functioning of the mind or brain’
In the common law, loss of decision-making capacity must be due to ‘some impairment or disturbance of mental functioning’ (Hunter [2009] NSWSC 761, [25]). Only the Tasmanian legislation has incorporated similar wording into its criteria for incapacity. Section 7(1) of the Act states that any incapacity must be as a result of ‘impairment of, or disturbance in, the functioning of the mind or brain’.
The additional criterion in the Tasmanian Act raises a question as to whether the threshold for incapacity in mental illness is significantly higher in Tasmania than it is in Victoria or Western Australia. One might ask, for example, whether an ‘impairment of, or disturbance in, the functioning of the mind or brain’ would encompass an adjustment disorder. If it did not, then even if a person with an adjustment disorder were regarded as suffering a mental illness as defined in the Tasmanian Act and as a result was unable to understand, retain or weigh the information relevant to a decision, this additional criterion would prohibit his or her involuntary treatment. However, the phrasing of the Tasmanian provision is cast in broad terms and courts have previously found that the similarly worded common law requirement for incapacity has covered reasons that have included ‘needle phobia’ (Re MB (Medical Treatment) [1997] EWCA 1361 (‘Re MB’)) and the effects of shock, severe fatigue or pain (Re T [1992] EWCA Civ 18, [28]). It is likely therefore that the emotional turmoil usually evident in, at least, a severe adjustment disorder would be regarded as ‘impairment of, or disturbance in, the functioning of the mind or brain’ for the purposes of the Act.
An inability to understand information relevant to the decision
In all four states, to have capacity, a person must be able to ‘understand’ information relevant to a treatment decision. Even so, a person is not to be regarded as lacking capacity if the assessor has failed to communicate with the patient in way that he or she is likely to understand (Mental Health Act 2013 (Tas) s 8(4); Mental Health Act 2013 (WA) s 9; Mental Health Act 2014 (Vic) s 8).
The first aspect of this requirement is that the assessor must be certain that the person has sufficient English language comprehension to understand the relevant information, and an interpreter must be arranged if there is any doubt.
In addition, the assessor must communicate in an accessible way. For most patients, medical jargon should be avoided, and in some circumstances additional adjustments should be made to assist a patient’s comprehension, especially if the patient is distressed or intellectually impaired. Assessors should use clear, plain language wherever possible, and should repeat information if asked to, or if it seems to help the patient’s understanding. There is empirical evidence that for patients with schizophrenia, repeating consent-relevant information improves understanding of that information (Palmer and Jeste, 2006).
Environmental factors can also contribute to incapacity, so care should be taken to ensure the people are not overwhelmed by noise or other distractions and that they have sufficient time to process the information they have been presented with. It is important that, as much as possible, the patient feels safe and supported. If the patient wishes, it may help to have a friend or family member available to talk through a decision and provide further support. Overall, efforts can, and should, be made to support the person to demonstrate their decision-making capacity to the fullest extent possible (Peisah et al, 2013; Mental Health Act 2007 (NSW) (as amended 2014) sub-s 68(h1)).
However, even where a person is well supported, and information has been given appropriately, there may still be doubt as to a person’s ability to understand information. In those circumstances, the clinician can usually test understanding by asking the patient to paraphrase the information given (Appelbaum, 2007; Appelbaum and Grisso, 1988).
It is worth noting briefly that under the common law test for capacity, there has been some debate as to whether a person is merely required to have the ability to understand the relevant information or whether it is necessary for the person to actually understand the information (Stewart and Biegler, 2004). In Tasmania and Western Australian, the new legislation requires that a person be able to understand, while in Victoria the person must actually understand (see Table 1). However, for the purposes of clinical capacity assessment, the issue is somewhat moot, since it will normally only be possible to test the ability to understand information by reference to what the person actually understands.
Note too that a person need only understand information that is relevant to the decision. His or her understanding of other information outside the decision at hand is irrelevant. Each of the Tasmanian, Victorian and Western Australian statutes contains a list of information that must be communicated to patients for a valid treatment decision (Mental Health Act 2013 (Tas) s 8(2)(c); Mental Health Act 2013 (WA) s 19; Mental Health Act 2014 (Vic) s 69(2)). The required information includes the risks of the treatment and alternatives, as well as any information that the clinician knows would influence the person’s choice.
A lack of insight may impact a person’s ability to understand relevant information, but the presence or absence of insight is not a proxy for the presence or absence of decision-making capacity. Insight is an extremely complicated phenomenon that is rarely either simply present or absent. Various aspects of insight – such as insight into diagnosis, insight into the presence or veracity of phenomenology and insight into the need for treatment – may all vary independently (Diesfeld, 2003; Melamed et al., 1997; Smith et al., 2004). This, in combination with the requirement that a person only needs to understand information that is relevant to the decision being made, means that while a lack of insight may suggest a lack of decision-making capacity, this deficit alone will rarely be determinative.
The relevance of a lack of insight really depends on the degree to which it impacts each element of the capacity test. For example, a person with chronic schizophrenia may disagree with his doctors about his diagnosis, and may not believe that the voices he experiences are a result of mental illness. However, he may acknowledge that the voices are less troublesome when he takes antipsychotic medication. This understanding of the reason for treatment and its effect may be sufficient to fulfil this part of the capacity test.
An inability to retain information relevant to the decision
Under the Tasmanian and Victorian Acts, a person who is unable to retain or remember the information relevant to the decision will not have decision-making capacity. Though this is not a formal criterion under the Western Australian legislation nor, of course, under the New South Wales legislation, retention of the relevant information is probably still required insofar as it is necessary for the person to be able to ‘weigh up’ information.
The statues do not specify how long exactly the information should be able to be retained, though in the Tasmanian legislation a provision explains that a person may be taken to be able to retain information relevant to a decision if they can do so at least briefly (Mental Health Act 2013 (Tas) s 7(3)(b)). In any case, it would seem that a person must be able to retain information long enough to make a decision.
An inability to use or weigh the information as part of the process of making the decision
An inability to ‘use and weigh’ information has provided the basis for most of the determinations of incapacity encountered in case law (Donnelly, 2010). Of the criteria in the common law tests of decision-making capacity, this has inspired most controversy. Part of the reason for the controversy is that there is no clear consensus as to what an inability to use and weigh information actually means.
Similar disagreement is likely to arise in the legislative tests which also require (using various forms of words – see Table 1) that a person is able to ‘use or weigh’ information to reach a decision.
Ultimately the courts interpret the meaning of legislation using a complicated process involving numerous approaches, which are informed by theories that often run counter to one another (Pearce and Geddes, 2011). As a result, any attempt to interpret the meaning of legislation – which is really the whole point of this paper – runs the risk of eventually being wrecked on the shores of a later confounding judicial decision. As a general rule, courts interpret legislation by giving the language its ‘ordinary and natural’ meaning, taking into account the purpose of the legislation to help resolve any ambiguity. The purpose of legislation is usually described in the Act’s objects and principles sections (Mental Health Act 2013 (Tas) ss 12,15; Mental Health Act 2014 (Vic) ss 10,11; Mental Health Act 2013 (WA) ss 10,11); Mental Health Act 2007 (NSW) ss 3,68). The court may also consider any meaning ascribed to similar phrases in the common law from which the provisions were derived.
The first case to carefully formulate the test for capacity to refuse medical treatment concerned a 68-year-old inpatient, dubbed ‘C’ (Re C [1994] 1 All ER 819). C suffered chronic paranoid schizophrenia and in Re C he sought an injunction to prevent the hospital from amputating his leg without his express written consent. C had peripheral vascular disease and a month earlier he had been noted to have a large necrotic ulcer on the dorsum of his right foot. At that time a surgeon had considered that C would ‘die imminently’ without an amputation and had stated that conservative treatment gave him no better than a 15% chance of survival. C had refused amputation saying ‘he would rather die with two feet than live with one’ (291F). C did agree, though, to debridement and a skin graft. This was performed and appeared to have been successful at the time of the hearing, but the hospital had refused to give an undertaking not to force C to have an amputation at some time in the future.
As a part of his illness, C experienced ‘grandiose delusions of an international career in medicine’ (293D). He also had some persecutory delusions, though these did not include any concerns about his treating team. Appearing in court, he ‘expressed complete confidence in his ability to survive his present trial aided by God, the good doctors and the good nurses’. Although he believed he would not die as a result of his ulcer, he made clear that ‘he could not say that would not happen’ (293D) and he accepted that dying as a consequence of retaining his limb was a possibility. A surgeon testified that he felt that ‘all C’s responses were normal’, and that they did not ‘deviat[e] much from the mean’ (292H).
The judge, Thorpe J, found that there was no direct link between C’s refusal and his persecutory delusions. He noted that, in court, C was ‘ordinarily engaged and concerned’, his answers ‘measured and generally sensible’ and that his ‘rejection of amputation seemed to result from sincerely held conviction’ (294C). As a result, His Honour stated that he was completely satisfied that C ‘had understood and retained the relevant treatment information, that in his own way he believes it, and that in the same fashion he has arrived at a clear choice’ (294E). Accordingly he granted the injunction.
Note that although C was clearly delusional, and although some of those delusions had a medical theme, the judge did not feel these pathological mental state features impacted on C’s decision-making with respect to the decision about the amputation. Note too that in describing the mental processes C engaged to come to a decision, Thorpe J used terms that underlined the normality of C’s mental processes in broad terms.
The same sort of language and analysis was used in a subsequent case involving a 23-year-old woman with severe needle phobia who required an emergency Caesarean section (Re MB [1997] EWCA 1361). Before the emergency hearing, MB had several times consented to the operation, only to withdraw that consent at the last minute when confronted with a cannula or oxygen mask. A psychiatrist reported that just prior to the operation, with the thought of the needle penetrating her skin, MB ‘got into a panic’ and that ‘her fear dominated all’. At that point he felt, ‘she was not capable of making a decision at all, in the sense of being able to hold information in the balance and make a choice’.
In her decision in Re MB, Butler-Sloss J first set the ground by stating that a ‘woman who has the capacity to decide may, for religious reasons, other reasons, for rational or irrational reasons or for no reason at all, choose not to have medical intervention, even though the consequence may be … her own death’. This statement echoed similar judicial statements in similar circumstances (Sidaway v Board of Governors of the Bethlem Royal Hospital [1985] AC 871, 904F; Re T [1993] Fam 95, 102E) implying a clear distinction between capacity and rationality and in support of autonomy against the imposition of the values of others (Parker and Cartwright, 2005). Her Honour went on to say that ‘panic, indecisiveness and irrationality in themselves do not as such amount to incompetence, but they may be symptoms or evidence of incompetence’ and clarified that in using the term ‘irrationality’ she meant ‘a decision which is so outrageous in its defiance of logic or of accepted moral standards that no sensible person who had applied his mind to the question to be decided could have arrived at it’. She accepted that, because of her phobia, at the crucial moments, fear dominated MB’s thinking and as a result ‘she was incapable of making a decision at all’.
In both cases the judges appeared to regard the conceptual ground encompassed by the ability to use and weigh the relevant information as wide enough to accommodate the range of mental processes that fall within the extensive range of ordinary human experience. The mental processes did not need to be logical or rational to demonstrate the ability to use and weigh (Parker and Cartwright, 2005), although significant irrationality in the process (or in the actual decision) may constitute evidence of incapacity (Somerville, 1981).
The Courts have again and again decided the matter of decision-making capacity by determining whether or not a patient’s ability to use and weigh information fell within this broad territory. In Trust A v H the Court decided that the decision-making ability of woman with schizophrenia considering a hysterectomy and bilateral salpingo-oophorectomy as treatment for ovarian cancer was being impeded by her delusional belief that she had not yet had children and that this influence took her outside the bounds of a normal ability to use and weigh (Trust A and Trust B v H (an Adult Patient) [2006] EWHC 1230 (Fam)). In another case a young woman with anorexia nervosa was found to lack capacity due to ‘obsessive fear of weight gain mak[ing] her incapable of weighing the advantages and disadvantages of eating in any meaningful way’ (Re E [2012] EWHC 1639 (COP), [49]).
Courts have also found an inability to use and weigh in the context of personality disorder. In NHS Trust v T, a 37-year-old woman with borderline personality disorder, who frequently cut and bled herself down to life-threatening anaemia, was found to have lacked capacity when she completed an advance directive refusing blood transfusions (NHS Trust v T (Adult Patient: Refusal of Medical Treatment) [2004] EWHC 1279 (Fam)). The basis for the Court’s decision was Ms T’s insistence, recorded in the advance directive, that her blood was evil. Charles J found that this belief rendered her unable to use and weigh the relevant information. Notably some of the psychiatrists who gave evidence did not regard T’s insistence as delusional and Charles J characterised it as ‘a misconception of reality’.
In another case a health service applied for authority to perform an instrumental delivery and, if that were to fail, a Caesarean section upon a 32-year-old woman, ‘W’, who had presented to the emergency department in arrested labour (Norfolk and Norwich Healthcare NHS Trust v W [1996] 2 FLR 613). W had had no prior antenatal treatment and ‘despite the obvious indications to the contrary, she continued to deny that she was even pregnant’. She was seen by a psychiatrist, who did not believe she was mentally ill (in the sense implied by the Mental Health Act 1983 (UK)). He felt that she understood that she was in an obstetric ward and that Caesarean was proposed but, given that she persisted in denying her pregnancy, he did not believe she could balance the information given her. Johnson J agreed and found her ‘incapable of weighing up the considerations that were involved’, commenting that she ‘was called upon to make that decision at a time of acute emotional stress and physical pain in the ordinary course of labour’.
Contrary to the conclusions of some academic commentators, Commonwealth courts appear to have interpreted the boundaries of an ability to use and weigh the relevant information more widely than the boundaries of either a logical process (Appelbaum and Grisso, 1988), a rational process (Freedman, 1981), a not irrational process (Stauch, 1995) or even a reasoned process (Donnelly, 2010; O’Neill and Peisah, 2011). Instead they appear to regard a person as having failed the test if he or she is unable to use or weigh the relevant information in one of the many ways that people ordinarily process information when not affected by an impairment of, or disturbance in, the functioning of the mind or brain. Using this broad understanding of the test it is possible to imagine how it is likely to be applied in various clinical situations.
Consider a patient with a delusional belief that he is the victim of a worldwide Internet conspiracy to do him harm, who is constantly in fear for his life as a result (Ryan et al., 2012). Because of this he is generally distrusting of others and is constantly anxious. His doctors recommend antipsychotic medication to improve his circumstances, but because to him, his fears are well-founded, and he does not believe that his fears are based on a delusion, he is very unlikely to be able to use and weigh the information about the benefits of treatment against information about the treatment’s potential adverse effects and disbenefits.
The ability to use and weigh information will also be disrupted by certain other features of severe psychiatric illness. People in the midst of severe depressive illnesses may understand all the information relevant to their decision, but may, as a result of their pathological hopeless and despair, weigh the information quite differently to the way they would have had they been well. In particular they may seriously underestimate their chances of recovery, or even their ‘worthiness’ to receive treatment. This may be so severe that they may be thought to be ‘unable’ to use or weigh information in the way we might expect (Grisso and Appelbaum, 1995). As a result of an inability to use or weigh the relevant information they would likely be judged to lack capacity (Donnelly, 2010). A similar analysis might be applied in the case of a patient with mania who might be considered optimistic to a pathologically extraordinary extent.
Even without a psychosis or a severe mood disorder, extreme psychological distress, as is frequently evident in occasions of sudden and expected loss, might make a person temporarily unable to use or weigh information. This not uncommonly arises when a person impulsively takes an overdose in the context of a traumatic life event and then refuses medical treatment. Aside from the potential intoxication caused by the overdose, capacity may also be compromised by distress itself. People who have recently experienced the death of loved one, or a relationship break-up or any other acutely distressing life event, might be so emotional that they are unable to provide any real rationale for their self-destructive actions, often saying simply that they cannot go on. At other times they may be so blinded by emotion that they can neither consider, nor even see, any alternative actions. In such circumstances the person may be so severely distressed that they are unable to use or weigh information relevant to a decision.
There is an obvious danger in using this sort of analysis that the assessor may confuse the importance of an abnormality in the process of coming to a decision with the relative unimportance of a decision that is itself abnormal or unusual. This is especially likely if the decision taken is not one that the assessor would agree with on rational or moral grounds. If this confusion were allowed to render the decision invalid it would undermine respect for the individual’s autonomy and would be contrary to the rationale of the reformed legislative schemes that seek to support personal choices. Assessors need to be wary of the potential for such errors in administering the test and be at pains to guard against them.
Consider a woman with severe recurrent bipolar disorder, who, when previously unwell, has gone on extravagant spending sprees, which have placed herself and her loved ones at considerable financial risk. If, when she was well, this woman were to decide that she no longer wanted to take the mood stabiliser prescribed by her doctor and wished to use diet and exercise to control her symptoms under the supervision of her alternative health practitioner, then, despite the fact that most doctors would regard this choice as wrong, irrational or even irresponsible, such judgments are not, by themselves, evidence of incapacity. It is obviously well within the range of ordinary human choices to put faith in alternative therapies and to bring this to bear in the process of using and weighing options. Unless the woman’s convictions about the efficacy of diet and exercise were new and could be convincingly traced to a phenomenological feature of her bipolar illness, it seems quite unlikely that the processes of her decision making could be seen as pathologically influenced and she could not, therefore, be seen as unable to ‘use or weigh’.
An inability to communicate the decision
Being unable to communicate a decision is a criterion for incapacity in all of the new mental health acts.
In practice an inability to communicate is very unlikely to apply without the person also being unable to understand information and use and weigh it (obvious examples are unconsciousness, or severe intellectual disability), however it is possible to imagine circumstances where the communication test will be relevant on its own. Catatonia (including excited catatonia) might result in a scenario where a person might reasonably be believed able to understand, retain, and use and weigh information, and yet he or she may be unable to communicate a treatment decision (Roth et al., 1977). Elective mutism (including a refusal to engage in any sort of communication) might be another example.
A person should not be regarded as being unable to communicate information in circumstances where they require special means to communicate, and these means have not been provided. For example, a person who is unable to speak or who is dysphasic may well be able to communicate via sign language or another assisted communication alternative, sometimes facilitated by a speech pathologist (Aldous et al., 2014). A person should be provided with a means of communication they are able to use.
In their classic paper on assessing capacity, Appelbaum and Grisso suggest that concept of communicating a choice also requires ‘the ability to maintain and communicate stable choices long enough for them to be implemented’ (Appelbaum and Grisso, 1988). The authors did not provide a citation for this pronouncement and there is little to support this notion in the common law context at least. It is probably better to regard rapid changes of mind as evidence that the patient may be having difficulty using and weighing the relevant information (Re MB [1997] EWCA 1361), which is how Appelbaum has regarded this sign in later publications (Appelbaum, 2007).
A sliding scale of capacity and proceeding in the face of doubt
The notion of a sliding scale of capacity refers to the notion that ‘[t]he more serious the decision, the greater the capacity required’ (Re T [1992] EWCA Civ 18, [28]). It is the idea that the threshold amount of capacity required to make a competent decision rises as the gravity of a decision increases.
Originating in English cases and frequently supported in academic commentary (Backlar, 1996; Howe et al., 1991; Wilks, 1997), the sliding scale of capacity has also been referred to in the lead Australian case on treatment refusal (Hunter [2009] NSWSC 761, [24]), though it did not form part of the basis for that decision.
Whether or not this sliding scale should be adopted, however, is a point of considerable debate in the academic literature. It may well be that, in general, more weighty decisions are more complicated, and that that added complexity may require that an individual have more cognitive power to meet the (same) thresholds of understanding and using and weighing (Kerridge et al, 2013; Wicclair, 1999), but it is hard to see how the thresholds themselves could change.
Perhaps the better approach is, not that a person need have ‘more’ or ‘better’ capacity to make a more important decision, but that we should be more careful in our assessment of capacity when the stakes are high (Cale, 1999; Parker, 2004; Parker and Cartwright, 2005; Stewart and Biegler, 2004; Wicclair, 1999). Certainly the common law seems clear that we should be reluctant to endorse a harmful decisions unless we are sure that that decision is truly made with capacity.
The law also provides guidance for proceeding in the face of genuine doubt when considering decisions that may result in harm. In such circumstances the courts have held that ‘if there were doubt as to the individual’s expression of preference, “that doubt falls to be resolved in favour of the preservation of life”’ (Hunter [2009] NSWSC 761, [9]; Re T [1992] EWCA Civ 18, [26]).
It is easy to imagine a circumstance where, even after extensive assessments of an individual’s decision-making capacity, clinicians and tribunal members will be left unable to definitely displace the presumption of competence, but still earnestly believe that the person may lack capacity. In those circumstances, and bearing in mind that coercive treatment itself may have powerful negative effects on an individual’s health (Large et al., 2013), it seems both wise and consistent with the law that clinicians provide whatever support is necessary to preserve life and then refer the decision to the tribunal (Re MB [1997] EWCA 1361); and that tribunal members, if still genuinely uncertain, authorise treatment aimed at sustaining life and clearly restoring capacity.
Conclusion
We have presented an analysis of the law around decision-making capacity as it applies to the refusal of psychiatric treatment in order to assist clinicians and tribunal members as they try to determine whether a person has decision-making capacity as referred to in the new or reformed mental health legislation of Tasmania, Victoria, Western Australia and New South Wales. It is increasingly likely that other Australasian jurisdictions will make similar reforms in coming years and we anticipate that the principles outlined above are likely to be useful in these contexts as well.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
From time to time CR and CP provide expert testimony in civil cases where the assessment of capacity may be at issue.
Legislation cited
Mental Health Act 1986 (Vic).
Mental Health Act 1996 (WA).
Mental Health Act 2013 (Tas).
Mental Health Act 2013 (WA).
Mental Health Act 2014 (Vic).
Mental Health Amendment (Statutory Review) Act 2014 (NSW).
Mental Health Bill 2014 (Qld).
Mental Health (Treatment and Care) Amendment Bill 2014 (ACT).
Cases cited
Hunter and New England Area Health Service v A [2009] NSWSC 761 (‘Hunter’).
NHS Trust v T (Adult Patient: Refusal of Medical Treatment) [2004] EWHC 1279 (Fam).
Re C (Adult: Refusal of Medical Treatment) [1994] 1 All ER 819 (‘Re C’).
Re E (Medical treatment: Anorexia) [2012] EWHC 1639 (COP) (‘Re E’).
Re MB (Medical Treatment) [1997] EWCA 1361 (‘Re MB’).
Re T (Adult: Refusal of Treatment) [1992] EWCA Civ 18 (‘Re T’).
Sidaway v Board of Governors of the Bethlem Royal Hospital [1985] AC 871.
Trust A and Trust B v H (an Adult Patient) [2006] EWHC 1230 (Fam) (‘Trust A v H’).