
Abstract
Objective:
We study compulsory community treatment orders (CTOs) for patients with severe and persistent mental illness (SPMI). Focusing on a unique jurisdiction in Canada that allows for long duration CTOs with strict enforcement procedures, our objectives are to determine whether extended duration CTOs are effective and to determine whether associated hospitalization costs are reduced.
Method:
A mirror image, naturalistic design was employed using patients as their own controls to enhance external validity. No inclusive or exclusive criteria were employed for the 367 SPMI clinic patients who were studied over a 5-year period. Detailed documentation of the dates of all CTOs, long-acting antipsychotic injections (LAIs), emergency visits, hospitalizations, duration of hospitalizations, crimes and/or police involvement were collected. To study the relation between CTO and injection adherence, we use a mixed-effect linear regression model. To study the effect of injection adherence and hospitalization, we use survival analysis via Kaplan–Meier and Cox survival models.
Results:
CTO and non-CTO patients did not differ with respect to demographics, but CTO patients were significantly more severely ill. Following a CTO, adherence to LAIs increased over time (P < 0.001). The average time the patients spent in the community, that is, outside the hospital, was significantly longer under a CTO, and the duration of hospitalizations was decreased.
Conclusions:
LAI adherence and outpatient office visits were enhanced by extended duration CTOs, as was time out of the hospital. The shorter duration of hospital stays implies cost savings. These must be weighed against their undesirable coercive nature.
Introduction
Community treatment orders (CTOs) are complex mental health interventions that employ a legal requirement to coerce patients with severe and persistent mental illness (SPMI) who refuse to accept psychiatric treatment to do so. Thus, they remain controversial due to ethical concerns regarding their coercive nature and methodological issues concerning the use of naturalistic designs versus randomized controlled trials (RCTs) in studying their effectiveness.
A substantial number of naturalistic studies have reported decreased recidivism and/or shorter lengths of stay (LOS) in hospital as a result of CTOs. 1 –5 However, due to methodological issues, assessing the outcome of CTOs remains a contentious issue in the literature. Recently, increased attention has been directed toward the weaknesses and/or inadequacies of RCTs as the gold standard in assessing the outcomes of complex interventions—both in medical research at large 6,7 and particularly regarding psychiatric CTOs. 8 These authors detail handicaps in making valid inferences of causal attribution via RCTs, which emphasize efficacy and internal validity at the expense of generalizability and real-world effectiveness. As O’Reilly and Vingilis 8 point out, confounding variables include varying study designs with differing inclusion and exclusion criteria and sample sizes. In addition to the limitations of the RCT design, CTOs represent complex interventions, and this fact creates a second methodological challenge. There are jurisdictional differences in CTO regulatory provisions, differing professional decision-making, differing personal subjective ethical approaches toward restricting autonomy, and differing clinical judgments. Taking these methodological issues into account, various authors suggest alternative methodologies including naturalistic studies. 6,8,9
An early RCT of CTOs concluded that only extended duration orders with enhanced outpatient treatment had a positive impact on reducing recidivism. 10,11 A second study of the duration of CTOs by Rohland et al. 5 showed decreased admissions and LOS with commitment periods of greater than 1 year. Nevertheless, the literature is sparse regarding the outcomes of extended duration CTOs containing strict provisions in the legal order providing that the police can quickly bring nonadherent patients for treatment (see below). We conducted a longitudinal, naturalistic study to fill this gap.
Enhanced interventions are needed for SPMI patients as they suffer significantly short life spans, a multitude of serious symptomatic and functional impairments, and increased involuntary hospitalizations in comparison to the general population. 12,13 A particular subgroup of patients with SPMI suffer deficient or absent insight, 3,14 leading to impaired adherence with treatment 15 and to significantly poor outcomes and quality of life. 16 In addition, these patients incur considerable mental health-care costs. 17,18
To the best of our knowledge, although there is abundant knowledge about the beneficial effects of long-acting antipsychotic injections (LAIs) in SPMI, 15,19,20 the literature is silent on the effect of CTOs on injection adherence by using actual and accurate recorded LAI injection data. In this study, we hypothesize (i) that extended duration CTOs lead to increased adherence to antipsychotic treatment as well as more intensive outpatient clinical management and (ii) that the increased adherence with medications results in enhanced freedom of such individuals by reducing the time they have to spend in hospitals.
Patients and Methods
The study was carried out in Quebec, a distinctive jurisdiction where CTO duration is usually 3 years and can be as long as 5 years. In contrast, outside Quebec, CTOs tend to be of 6 to 12 months duration, and if further treatment is considered necessary, further legal procedures must be undertaken (from Personal Communication with Dr. Rohland BM.). 5,21
According to the Quebec civil code, the criteria for awarding a CTO are that the impaired person is unable to understand and appreciate that he or she requires psychiatric and/or social intervention, refuses it, and is unable to understand the risks and benefits involved. Dangerousness, per se, is not a legal criterion for a CTO in Quebec, although it is often elsewhere where a deterioration criterion, approximating dangerousness, is sometimes utilized. In Quebec, if the patient fails to show up for their visits and medications, the court order can be faxed to the local police who promptly bring the patient to the doctor’s hospital for evaluation and an injection of the required LAI. This is another uncommon feature of the Quebec system—the CTO itself directly allows for involuntary administration of medication. This feature is often explicitly prohibited elsewhere where obtaining permission for an involuntary injection or other coercive treatment requires additional legal authority and procedures. 22,23 The above organizational factors render Quebec a distinctive laboratory in which to test the outcome of CTOs.
We conducted a follow-back prospective study over a 5-year period between 2010 and 2015, based on our clinic’s entire SPMI population. Criteria for acceptance to the Continuing Care Clinic (CCC) i are cases where a patient suffers from SPMI and has suffered from repeated hospitalizations and significant morbidity. The most frequent diagnoses in the clinic are schizophrenia and schizoaffective disorder. The dates of (i) all clinic visits, (ii) injections of LAIs, (iii) CTOs, (iv) hospitalizations, (v) ER emergency room visits, and (v) crimes were recorded and the interrelationships were studied. Among the 367 patients studied, 77 were obliged via a CTO during the study period to have regular injections and clinical follow-up. Note that many of these 77 patients were also prescribed oral medications including clozapine, but injections were utilized because these particular patients are not reliable in taking oral meds. The remaining 290 patients did not have a CTO during the study period. Consent to participate in this retrospective study was not required, and no patient was identified by name. Ethics approval was received from the hospital’s research and ethics committee.
In Montreal, mental health care is provided by the designated hospital in its geographical catchment area, that is, the patients who present at the emergency room of another hospital are immediately transported to their assigned hospital. There are virtually no private or alternative mental health services available to this population. As a result, the psychiatric care utilization data for our patient population can be considered to be quite complete and accurate. These facts are not usually applicable to other jurisdictions. No meaningful changes in the legal tenets, organizational functioning, bed capacity, or clinic staffing occurred during the 5 years of the study.
Demographic and care utilization data were obtained from the hospital’s medical and administrative records and from the patient charts in an electronic database record. Each injection was recorded in the electronic medical records by nurses in the outpatient clinic. Data regarding costs of psychiatric hospitalizations were obtained from the hospital information technology department. CTO and criminal records were obtained at the Montreal Courthouse by the hospital’s legal consultants. We obtained the rates and types of crimes committed as described by the CCC.
The study was designed to enhance its external validity—no exclusion criteria for entry to the clinic were employed. As emphasized in detail by O’Reilly, 24 these features convey a significant advantage of a naturalistic method compared to RCT methodology, aside from the fact that regression to the mean is not controlled.
We categorized patients into two groups: CTO patients, who were under active CTOs at some point during the study period and non-CTO patients, for whom a CTO was never requested. Two-sample t test was conducted to report the significances of the differences between these two patient groups. We recorded age, gender, ethnicity, substance abuse history, injection, hospitalization, ER visit history, and criminal records. Specifically, age is defined as the age of the patient at the year of the study start; substance abuse history is defined as the existence of any substance abuse records during the study period; injection is defined as the existence of injection records from the clinic, that is, at least one injection is recorded as admitted to the patient in the clinic; hospitalization is further divided into three subcategories, that is, the existence of one hospitalization during the study period, the existence of two hospitalizations, and more than three hospitalizations; ER visit is defined as the existence of any ER visit records during the study period; and, criminal record is defined as the existence of any criminal history for the patient.
We studied the effectiveness of CTOs on hospitalization rates and injection adherence using the uncontrolled before and after comparison method. To ensure a representative group of patients with enough observation periods, we selected 53 CTO patients for whom we have at least 6-month worth observations both before and after the initiation of CTOs. Each patient acts as their own control, and paired sample t test was used to examine the change after the initiation of CTOs. The hospitalization rate is defined as the number of hospitalizations divided by the duration of the time interval of interest, and injection adherence is defined as the number of injections received at the outpatient clinic during the time interval of interest divided by the number of injections prescribed during the same interval. To examine the impact of CTOs on LOS, we focus on the subgroup of 26 CTO patients, from whom we observe hospitalizations both before and after the initiation of their CTOs.
We also examined the effect of CTOs on injection adherence and the effect of injection adherence under CTOs on hospitalization rate
We aimed to establish the link between the increased injection adherence and the reduced hospitalization rate under CTOs. Defining survival as living in the community without any hospital admissions, we applied the Kaplan–Meier method 25 and the Cox survival regression models. 26 –29 The Kaplan–Meier method accounts only for adherence rate and does not take into account other factors that can potentially affect hospitalization rate and hence we resorted to the Cox survival regression model to analyze the effect of adherence on hospitalization with other covariates as controls. Again, the 53 CTO patients with sufficient observation periods were used in both of the above survival analyses. Since injection adherences tended to fluctuate over time for all patients and Cox survival regression can readily incorporate time-varying covariates, we calculated the monthly injection adherences to better capture the fluctuation of injection adherences and to have a better estimate on their effects on hospitalizations. In total, the 53 CTO patients produced 2,497 monthly observations for the Cox regression model.
Results
Demographic and Clinical Characteristics
Table 1 displays the basic characteristics for these two patient groups, CTO patients group and non-CTO patients group, and reports substance abuse history, LAI injections, hospitalizations, ER visits, and criminal history within each group.
Demographics Characteristics: CTO and Non-CTO Patients.
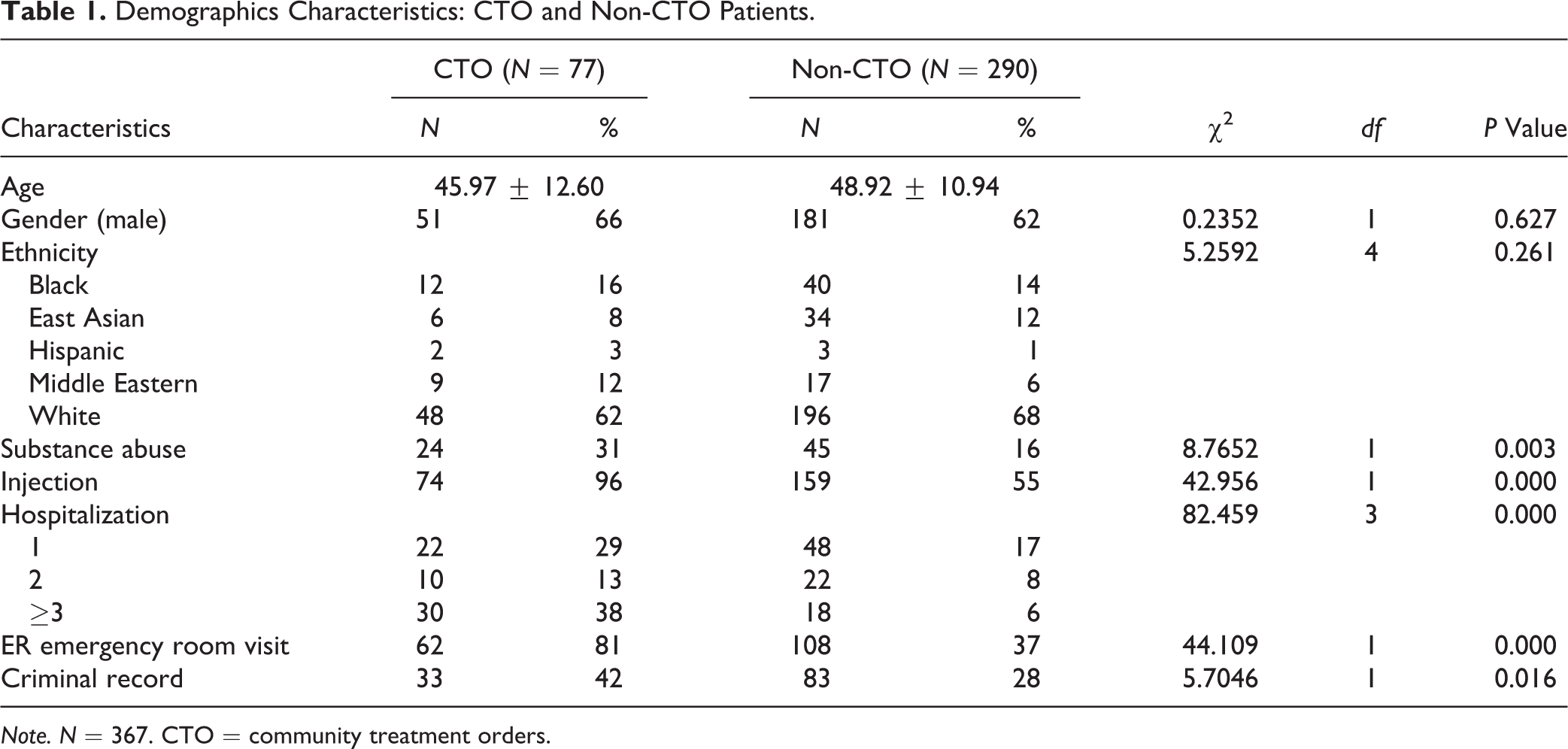
Note. N = 367. CTO = community treatment orders.
We observe that there are no significant differences between CTO patients and non-CTO patients in terms of demographics, that is, age, gender, and ethnicity; while CTO patients are more severely ill in the sense that they are significantly more likely to have substance abuse history, to have LAI injection history, to have ER visits and hospitalization histories, and to have criminal history records.
It is evident from our data set that the crime rate of our SPMI patient cohort is higher than the general population in Montreal. During the 5-year study period, there were 570 charges reported for the 367 patients. This amounts to 21 times the rate of adults charged in Montreal in 2012. ii Note that we include all indicted and acquitted charges from both the criminal court and municipal court in our calculation. The CTO patients had a higher frequency of charges, that is, 220 charges for the 77 CTO patients.
Uncontrolled Before and After Comparison of Hospitalization Rates
On average, patients were admitted 0.96 times per year before the start of their CTOs, whereas the frequency decreased to 0.56 times per year during the CTOs. The decrease is statistically significant (P = 0.013, degree of freedom = 52, t statistic = 2.554) using paired-sample t-test method.
To assess CTO’s impact on the hospital LOS, we focused on a subgroup of 26 CTO patients, from whom we observe hospitalizations both before and after the initiation of their CTOs. Comparing the last hospitalization prior to the initiation of CTOs to the first hospitalization posterior to the initiation of CTOs, there was an average decrease of 31.5 days on LOS from 84.53 days prior to 53.03 days posterior. Using the cost information provided by the hospital, that is, $472.11 per day in the psychiatry ward, we estimate that the CTOs are associated with savings of up to CAD$14,871 per hospitalization.
Effect of a CTO on LAI Adherence
LAI injection adherence rate increased from 10.7% to 42.2% on average—statistically significant (P < 0.001, degree of freedom = 52, t statistic = 7.438) using paired-sample t-test statistic method. Correspondingly, we also observe that the number of outpatient visits also increased under a CTO—statistically significantly from 5.22 visits per year to 21.8 visits per year (P < 0.001, degree of freedom = 52, t statistic = 9.7640) using paired-sample t-test statistic method.
Through mixed-effect linear regression, we used injection adherence before the initiation of CTOs as benchmark, then calculated injection adherence for the 1st year after the initiation of CTOs, the 2nd year, the 3rd year, and so on. Table 2 depicts that number of years after CTO is the only statistically significant factor corresponding to LAI injection adherence. The benchmark injection adherence, that is, injection adherence before the initiation of CTOs, is 10.6%; the 1st, 2nd, and 3rd year during CTOs result in a significant increase in the injection adherence rate, and the level of increases are 0.28 (standard error [SE] = 0.05, P < 0.001), 0.32 (SE = 0.05, P < 0.001), and 0.38 (SE = 0.06, P < 0.001) respectively, comparing to the benchmark.
Injection Adherence over Time (Relative to Community Treatment Orders).
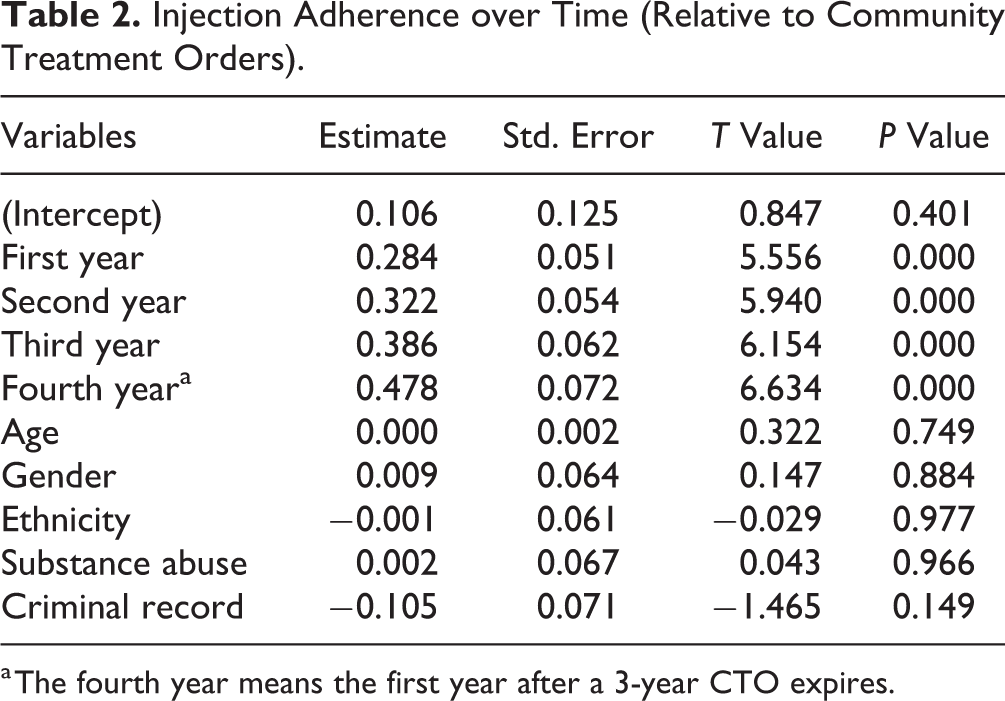
a The fourth year means the first year after a 3-year CTO expires.
Note that the injection adherence rate during CTOs is still relatively low and that late injections appear periodically. Figure 1 depicts that the majority of late injections are administered at the next scheduled appointment. An interesting and unanticipated finding was that in terms of the first injection received after the initiation of CTO, one subgroup received their LAIs in a timely manner considering the date at which the judge signed the order (36.4%), a second group’s injections were moderately delayed (21.2%), and a third group did not receive any injections (42.4%) till the next hospitalization.
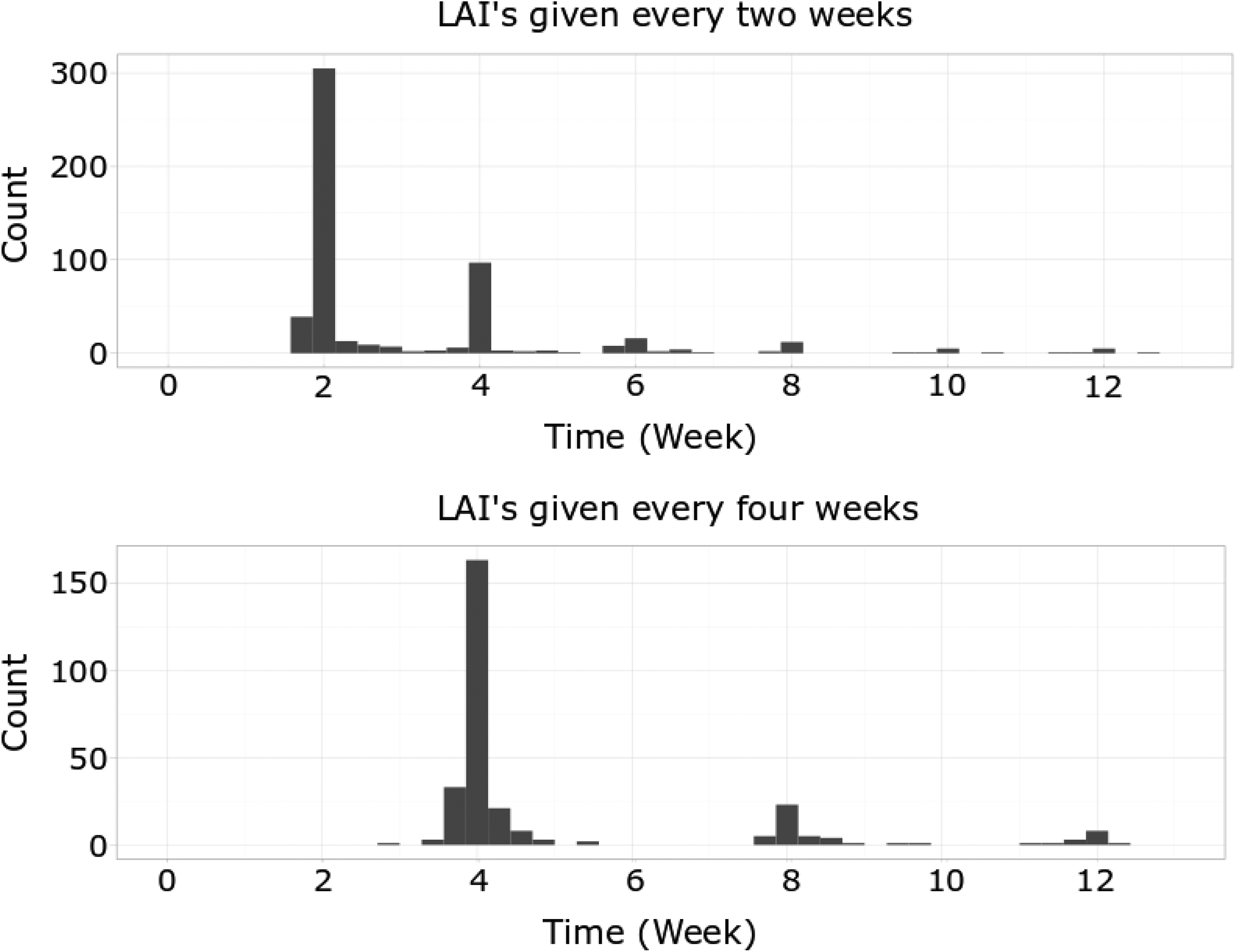
Injection received intervals during community treatment order periods. This figure shows the time intervals between sequential injections received by patients. The x-axis is time (per week), and the y-axis is the number of injections.
Effect of LAI Adherence on Hospitalization
We applied the Kaplan–Meier method for CTO patients by categorizing the adherences into two groups: (i) 0% to 30% adherence and (ii) 30% to 100% adherence, based on a visual inspection of the clustering of the data points. Figure 2 (left) visualizes the survival curves and shows that the patient group with low adherence has a significantly lower survival probability than the second group of patients. We use the log-rank test to determine whether the survival curves for the two groups are significantly different. This gives a P value < 0.001 using log-rank test, indicating that the two groups are in fact significantly different.
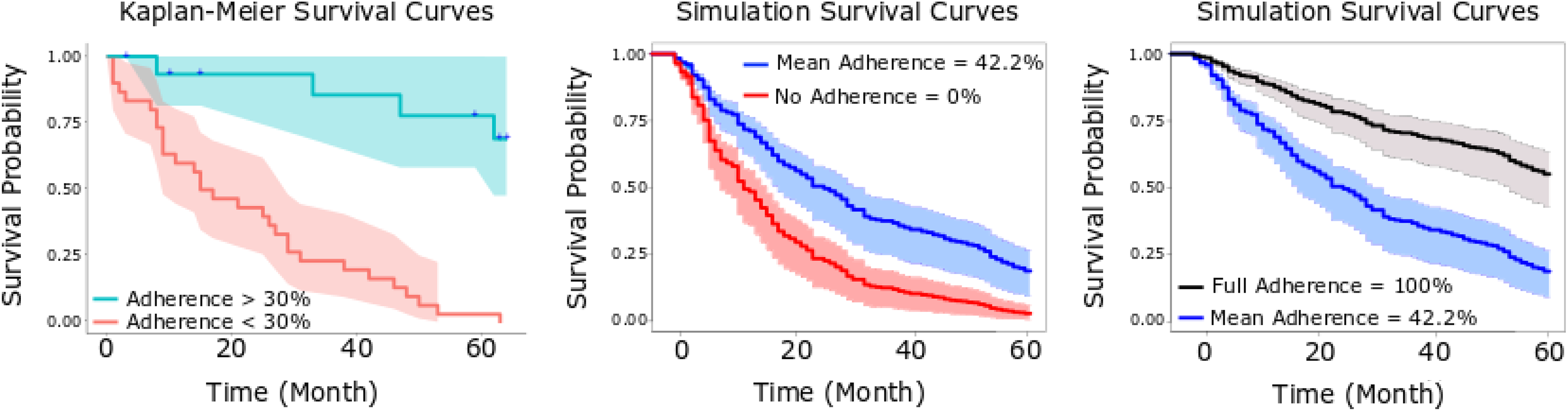
Time to hospital admissions among community treatment order patients with high-, medium-, and low-injection adherence: Kaplan–Meier survival curves (left) and simulation survival curves based on Cox model (middle and right).
We applied Cox survival model for the 53 CTO patients who have sufficient observation periods. From Table 3, there is a strong relationship between injection adherence and decreased risk of hospital admissions. Holding the other covariates constant, having one unit increase of injection adherence reduces the hazard ratio by a factor of 0.248 or 75.2% (CI, 0.126 to 0.489, P < 0.001).
Cox Model: Effect of LAI Adherence on Hospitalization.
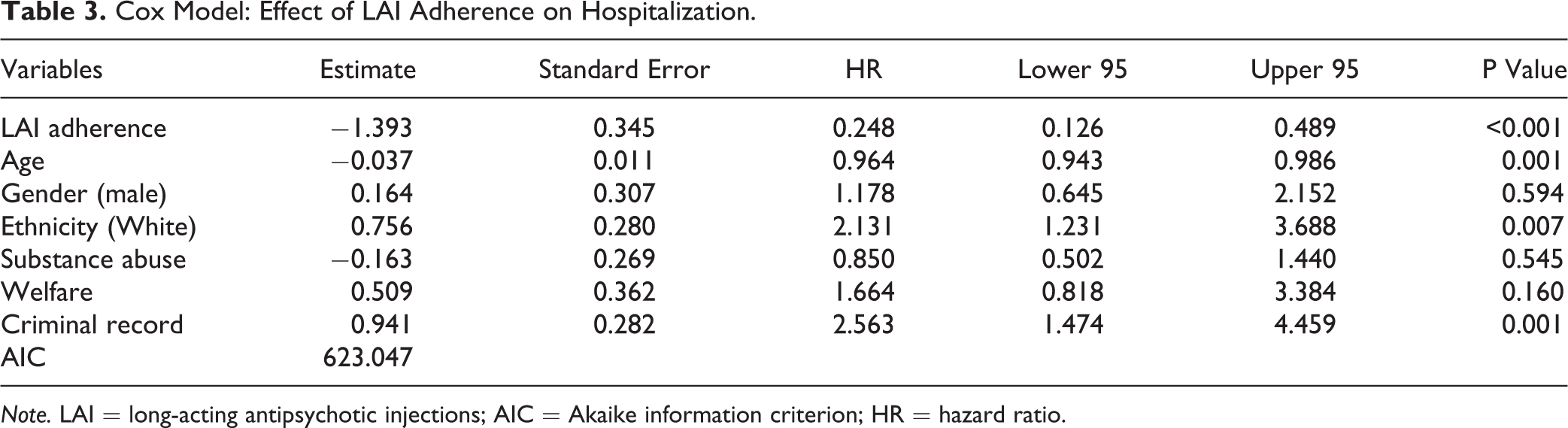
Note. LAI = long-acting antipsychotic injections; AIC = Akaike information criterion; HR = hazard ratio.
Discussion
Despite the numerous studies pointing to reduced recidivism with CTOs, only two prior studies investigated the relationship between the length of CTOs and outcome. 5,11 In the RCT study, extended outpatient commitment for 180 days or more had 57% fewer admissions and 20 fewer hospital days than shorter CTOs and were effective when combined with frequent outpatient services. The patients became more adherent with treatment, were less likely to be victimized, had reduced family strain, and had an improved quality of life. Shorter duration of CTOs in this study did not produce statistically significant results. 11 In the second study, CTO durations of longer than 1 year increased the number of outpatient visits, decreased the number of hospital admissions and total hospital days compared to the levels of use in the same patients over the 1-year period preceding the CTO. The positive effects persisted for CTO patients for up to 5 years. 5 A proviso in comparing these two studies with the present one is that as complex interventions the CTOs were conducted in each of the three settings under a different set of legal provisions and different service delivery characteristics.
The present study offers extended outcome data validating the benefit of longer duration CTOs with respect to recidivism, length of confinement in hospital, and cost savings of approximately $14,871 per hospitalization. Further, it contributes data about the mediating effect of LAIs and the intensity of outpatient visits on producing the effects. Considering the ethical concerns regarding the perceived coercion associated with CTOs, 30,31 authors skeptical about the outcome literature caution against the infringement on autonomy that CTOs involve and promote less restrictive alternatives. 32 –35 These authors tend to highlight the 2013 The Oxford Community Treatment Order Evaluation Trial (OCTET) study from England that utilized a RCT in showing no advantage of CTOs compared to a less restrictive control group. 34,36 The persistence of this controversy is apparent in various articles and in an exchange of letters to the editor in a 2016 issue of this journal between Dawson 37 and Hastings. 38
With these methodological considerations in mind, we employed a naturalistic technique for our CTO study. In choosing a naturalistic design, we were influenced by our clinical experience with very disturbed SPMI patients who, in our clinic population, and in correspondence with Quebec law, demonstrate a striking absence of insight, strong and continued no-adherence with treatment and clinical contact with associated severe psychiatric and social dysfunction and liabilities. With this type of patient, we considered it to be questionably ethical to randomize the given patient to a control group. The results remain consistent with our underlying hypothesis: The enforcement of a CTO is associated with increased LAI adherence, which in turn is associated with reduced hospitalization rates and LOS and a reduction in costs.
A possible explanation for the positive results under extended CTOs is that a longer period of time than a 6- to 12-month duration, which is standard elsewhere may be necessary for all the different individuals and stakeholders involved in a CTO to enact the intervention in a meaningful fashion. As an example, the clinical management techniques of our team, in addition to the provision of LAI’s, include intervening in the patient’s psychosocial milieu including group home or family issues, recovery/rehabilitation activities, building a treatment alliance, and interacting with the legal system. Over a 3-year to 5-year period, the various individuals and community systems become increasingly familiar and fluent with the intervention—patients, family members, psychiatric staff, police, lawyers, and the courts.
We have mentioned an interesting and unanticipated finding in terms of the delay in the first injection received after the initiation of CTO. There are a number of possible reasons for these delays or nonadherences: To avoid being forced to receive an injection, the patient may have fled or abandoned their apartment and not been able to be found, become imprisoned, may have presented some understandable life event or reason for a delay, the absence may not have been detected by the clinic staff considering its procedures for monitoring missed appointments, delays with particular patients may have been tolerated due to protecting and promoting doctor–patient alliance issues, and so on. Should adherence have been enforced more strictly in a timely fashion according to the legal order than this clinic has done, the resultant impacts on patient outcome, care utilization and costs would need further investigation.
Limitations of this work include the fact that regression to the mean is an alternative explanation to the improvements registered. This is a cogent criticism in that the patients may have been at low point in the intensity of their illness and improved over time. Another limitation of the study is that although we measured the crimes committed by our cohort, the numbers were too low to demonstrate any statistically significant link to CTOs. Replication of naturalistic methodologies with enhanced measurement of quality of life outcomes in the area is required.
Conclusion
Being mindful of the ethical and methodological conundrums surrounding CTOs, we have shown that, for a particular subgroup of patients with SPMI, a longer duration of CTOs with stricter enforcement procedures than has previously been utilized elsewhere enhances their freedom in the community due to lower hospitalization rates and shorter LOS. This favorable result increases with time over the time course of the order. Further, the data suggest that outcomes seem to be mediated by increased outpatient visits including improved adherence to long-acting injections of antipsychotic medications and the time required to implement interdisciplinary team psychosocial and community interventions with enhanced treatment techniques for treatment resistant patients The lower frequency and duration of hospitalizations is associated with significant cost savings. Finally, although the patient numbers and length of time of the study are too limited to show statistically meaningful results on the commission of criminal acts, for some patients, the CTO has diminished the frequency of criminal charges.
Footnotes
Authors’ Note
Data were collected through patient chart reviews, which was made possible by an ethic clearance that prohibits the authors from sharing the original data set.
Acknowledgments
The authors thank Yang Lan, Sabine Cohen, Sia Argyropoulos, Isabelle Aumont, Michael Buonvino, Yves Gabbay, Lavery de Billy, Avocats, S.E.N.C.R.L., Legal Affairs office of the Jewish General Hospital, Anne Lemay, Karl Looper, J. Christopher Perry, and Arthur Propst.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported partially by a Collaborative Research and Training Experience (CREATE) grant from the Natural Sciences and Engineering Research Council (NSERC) of Canada.