
Abstract
Objective:
In Canada, 80% of firearm-related deaths are suicides. Access to firearms is associated with increased suicide rates. This study examines the frequency and factors that influence assessment of firearm access in an emergency setting.
Methods:
A total of 15,847 consecutive adults seen for psychiatric consultation in two tertiary emergency departments (EDs) in Winnipeg, Manitoba were interviewed. Data captured whether access to firearms was assessed, and whether respondents endorsed access or not. Comparisons were done to determine group differences among those with and without and with known and unknown firearm access.
Results:
Access to firearms was unknown in 47% (n = 7,363) of psychiatric ED consultations, including 43% (n = 998) of individuals who presented with a suicide attempt. Female sex was associated with decreased odds of firearm access (odds ratio [OR] 0.28; 95% CI, 0.22 to 0.35). Being single was associated with lower odds of known firearm access (OR 0.83; 95% CI, 0.77 to 0.89) yet higher likelihood of firearm access (OR 1.36; 95% CI, 1.11 to 1.68). Presenting with a suicide attempt (OR 2.45; 95% CI, 1.80 to 3.34), preparatory acts (OR 6.40; 95% CI, 4.38 to 9.36) and suicidal ideation (OR 2.45; 95% CI, 1.87 to 3.21) were associated with increased odds of reporting access. When clinicians felt there was a high likelihood of future suicide, firearm access remained unknown in half of cases.
Conclusion:
Firearm ownership and access is an essential component of a suicide risk assessment and remains unknown in half of individuals seen by psychiatry in this tertiary care ED sample. People presenting with suicidal ideation and attempts were more likely to report access to firearms.
Introduction
In Canada, 80% of firearm-related deaths are suicides (compared to 27% globally), and 26% of total suicides are by firearm. 1,2 Suicide attempts, especially by firearms, can be impulsive 3,4 and have a case fatality rate as high as 91%. Access to a firearm is associated with increased suicide rates and an increased probability that a firearm would be the method chosen. 5,6
Means restriction is an evidence-based suicide prevention strategy at a population level. 7 In countries with legislation to reduce firearm ownership, there are lower firearm ownership rates and lower rates of firearm suicide. 8 –13 In the United States, states with the ability to enact Extreme Risk Protection Orders, preventing high-risk individuals from accessing firearms, suggest effectiveness at reducing suicide rates in an initial study. 14 On an individual level, many individuals who die by suicide have health-care contacts in the year preceding death, 15 and many individuals are seen in the emergency department (ED). 16 Those who use firearms in suicide attempts are more likely to die on their first attempt and show fewer suicide attempts in their history 17,18 and therefore unfortunately may not present to medical attention prior to attempt. Firearm access has been associated with male sex (as the primary owner of firearm), Caucasian race, and being married/cohabitating. Despite demonstrated risk factors, health-care providers are not accurate at predicting firearm ownership. 19 Betz et al. 19 sought to assess the occurrence of lethal means assessment in a large ED cohort with suicide ideation and attempts. Only 37% of the cohort had a documented lethal means access assessment on chart review, with the likelihood increasing if a mental health assessment was completed. Somewhat concerning was the finding that if the ED disposition was something other than admission, it was less likely that lethal means were assessed. When participants of this study reported on their firearm access in subsequent interview by study personnel, 50% of those with firearms did not have a documented assessment, including 13% of those who were discharged home. This study, while limited by strict inclusion criteria and excluding those with missing responses about firearms, was able to shed light on the importance of more universal ED screening for lethal means assessment.
As such, suicide prevention guidelines call for universal lethal means assessment 20 and many national organizations recommend lethal means counseling by ED care providers. 19 Unfortunately, this is not common practice, 21 –24 and little is known about assessment of firearm access in the Canadian context. The current study aims to assess the frequency of asking about firearms in a high-risk ED population and specifically to characterize the groups of people who report access to firearms as compared to those who do not and those with known vs. unknown access after ED psychiatric assessment. Health-care providers may be less likely to ask about firearm access, given that suicide by hanging is more common in Canada 25 ; however, firearm ownership in Canada, estimated at 26% of households, is still common. 26 With the high case fatality rate for suicide by firearm, it is prudent to use best practice recommendations as outlined by other national organizations. This study will inform areas where we may overlook risk in the ED setting and provide support for universal lethal means assessment and guidance on next steps.
Methods
Ethical Approval
Ethics approval was obtained from the University of Manitoba’s Health Research Ethics Board.
Setting and Study Population
The study population came from the Suicide Assessment Form in Emergency Psychiatry (SAFE) database which collects data on all psychiatric consultations seen in the two tertiary care hospitals in Winnipeg (population > 700,000), Canada. Emergency rooms are staffed 24 hr daily by psychiatrists and psychiatric residents. The sample was comprised of all psychiatric consultations between January 1, 2009, and December 31, 2016 (n =15,847). All consecutive consults were recorded without exclusion criteria.
Measures
After a comprehensive psychiatric assessment, the SAFE database is completed. The SAFE data set is a research database that includes existing suicide risk tools and a list of potential risk factors for suicide, each encoded as a separate field. The assessor is instructed to record an entry for each variable, one of either “present,” “absent,” or “unknown.” The SAFE form includes the SAD PERSONS Scale, a suicide screening instrument based on collated risk factors that includes sex, age, depression or hopelessness, previous attempts or psychiatric care, ethanol or substance abuse, rational thinking loss, lacking of social support, an organized plan or serious attempt, and having no spouse. Other risk factors for suicide are recorded in the database and include a history of childhood abuse, the presence of an anxiety disorder, acute stressor, aggression or impulsivity, and access to firearms. For the purpose of this study, the access to firearms variable was used to ascertain the assessment about firearms. The Columbia Classification Algorithm of Suicide Assessment (C-CASA) is used to categorize the type of suicidal presentation into mutually exclusive categories, those included in the analysis were suicide attempt (with intention to die), preparatory acts toward imminent suicidal behavior, suicidal ideation (SI), self-injurious behavior without SI, self-injurious behavior with unknown intent, and no suicidal or self-injurious behavior. 27 The Clinician Prediction Scale is a 10-point Likert-type scale completed by the clinician after the psychiatric assessment that measures their overall impression of future risk of self-injurious behavior, suicide attempt, and death by suicide within the next 6 months and has been used in other studies. 28,29 Its predictive validity shows acceptable area under the curve statistics for suicide attempts but not for suicide deaths, 28,30 and while negative predictive values are high, positive predictive values for both attempts and suicide are very low. The scale was then categorized to create “no risk,” “low,” “moderate,” and high-risk categories (0 = no risk, 1 to 3 = low risk, 4 to 6 = moderate risk, 7 to 10 = high risk).
Statistical Analysis
Study participants were categorized into three groups at their baseline assessment: “Access to firearms” if the firearm access for the individual was known, “No access to firearms” if the individual was asked and had no access to a firearm, and “Unknown access” where the question was not asked or the answer was unknown. Descriptive prevalence rates for each of the study measures among each of the three groups at the baseline assessment were generated using SPSS Version 21.0. Binary logistic regression was used to investigate the association between measures and firearm access, comparing (1) those with access to firearms to those with no access and (2) those with a known status (combining those with and without access) to those with an unknown status of firearm access.
Results
A total of 15,603 ED psychiatric consultations were included in analysis (98% of all ED psychiatric consultations during the study period). There were 381 ED presentations to psychiatry where access to firearms was endorsed, and 7,859 cases where access to firearms was denied, leaving 7,363 (47%) visits where the access to firearms was unknown.
Table 1 describes the characteristics of the sample across the three groups. Several variables were correlated with an unknown status of firearm access. Notably, an acute stressor contributing to ED presentation (odds ratio [OR] = 0.73; 95% CI, 0.68 to 0.78; P < 0.0001), a diagnosis of psychosis (OR = 0.56; 95% CI, 0.53 to 0.60; P < 0.0001), and a history of aggression and impulsivity (OR = 0.58; 95% CI, 0.54 to 0.62; P < 0.0001) were associated with a lesser likelihood of knowing whether they had access to a firearm. Conversely, every category of suicidal presentation was correlated with the assessor knowing the status of firearm access.
Sample Characteristics.
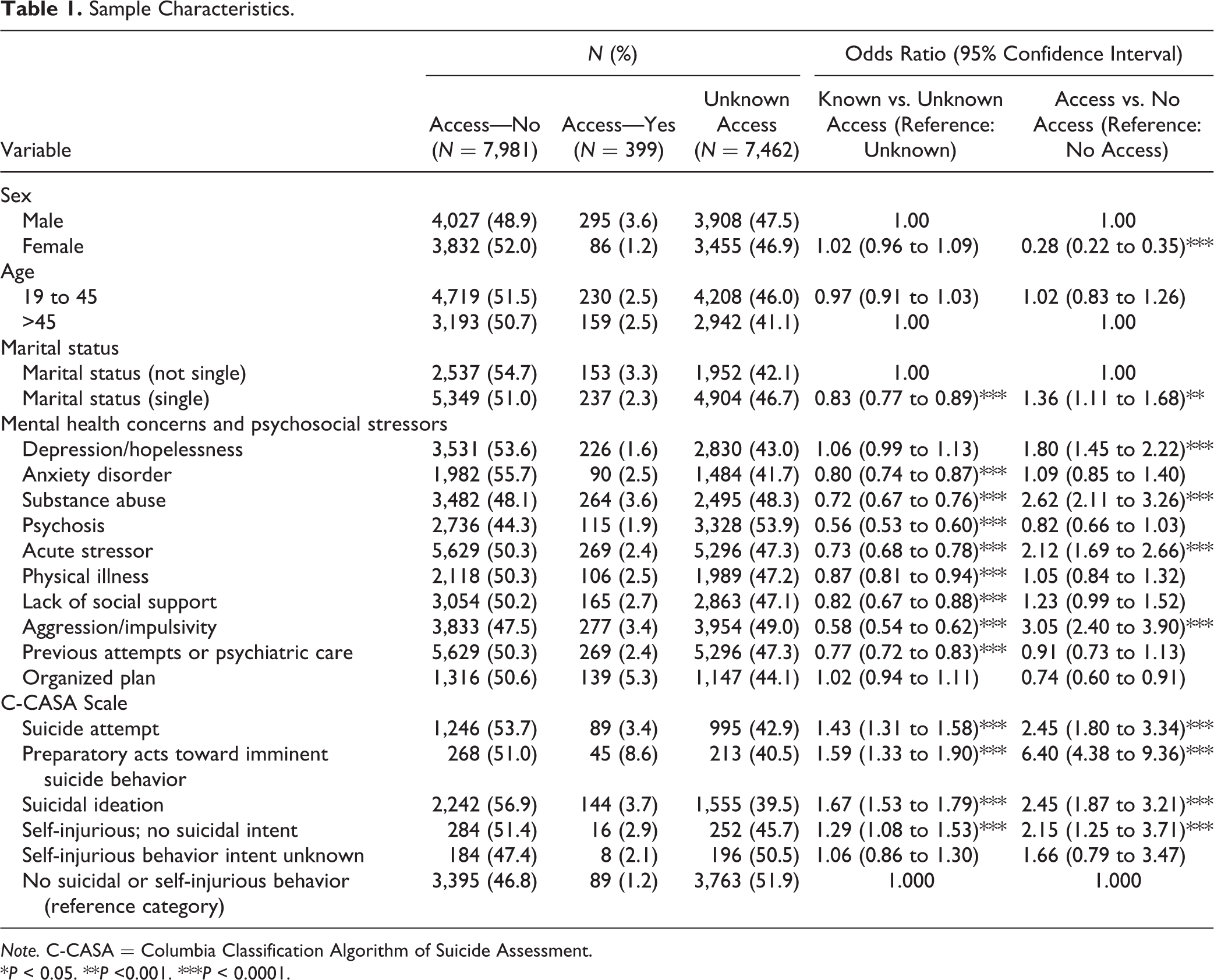
Note. C-CASA = Columbia Classification Algorithm of Suicide Assessment.
*P < 0.05. **P <0.001. ***P < 0.0001.
Also reported in Table 1 are the variables associated with a higher likelihood of access to firearms (compared to no access). Single marital status and male sex were correlated with access. Depression (OR = 1.80; 95% CI, 1.45 to 2.22; P < 0.0001), substance abuse (OR = 2.62; 95% CI, 2.11 to 3.26; P < 0.0001), and an acute stressor (OR = 2.12; 95% CI, 1.69 to 2.66; P < 0.0001) were correlated with higher odds of firearm access. People with aggression and impulsivity had a 3-fold greater likelihood of firearm access. People presenting to the ED with SI and suicide attempts had increased risk of firearm access. Those with preparatory acts toward imminent suicidal behavior had a more than 6-fold increased likelihood of firearm access (OR = 6.40; 95% CI 4.38 to 9.36; P < 0.0001).
Figure 1 depicts the proportion of those with known versus unknown firearm access based on their C-CASA presentation. Among those who presented with a suicide attempt, preparatory acts toward suicidal behavior, and SI, 43% (n = 998), 41% (n = 213), and 39% (n = 1,555), respectively, had unknown firearm access.
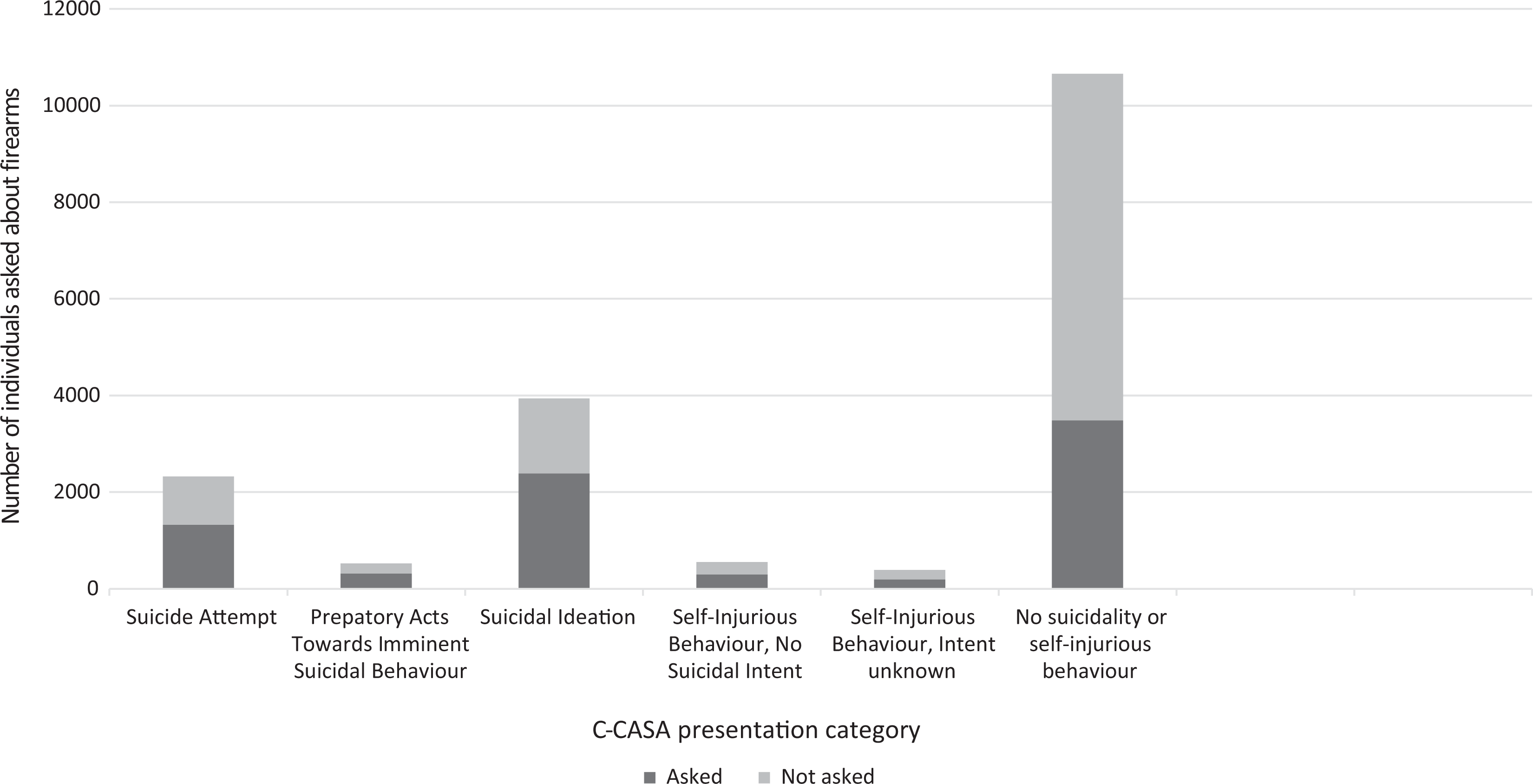
Proportion of individuals asked about firearms by Columbia Classification Algorithm of Suicide Assessment presentation.
Table 2 shows the rates and associations of clinician prediction of future suicidal behavior with firearm access. Regarding clinician knowledge of firearm access, most notable is that increasing clinician concern of future suicide and suicide attempt risk does not correspond to increasing knowledge of whether the person has access to a firearm. Among people rated as high likelihood of attempt and suicide in the next 6 months, 50% and 47%, respectively, had unknown status of firearm access. This finding is contrasted by clinician impression of risk when a person was known to have access to a firearm. People judged to be at high risk of suicide were more than 5 times more likely to have access to a gun, when compared to those deemed not at risk (OR = 5.66; 95% 2.21 to 11.34; P < 0.0001).
Clinician Prediction Scale and Access to Firearms.
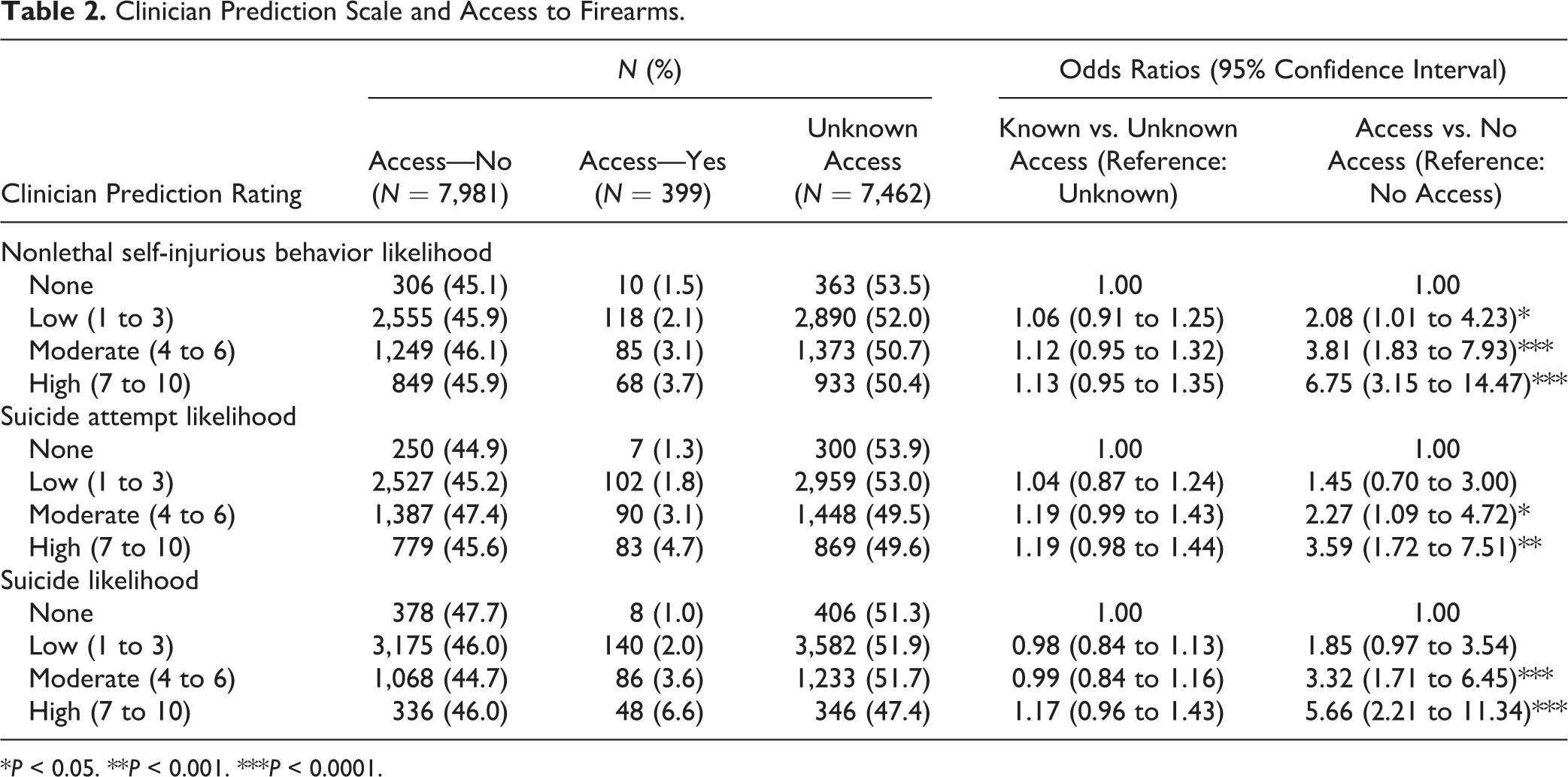
*P < 0.05. **P < 0.001. ***P < 0.0001.
Discussion
The current study adds to the literature of ED assessment of lethal means with specific attention to assessment of access to firearms in the psychiatric ED population. A previous chart review study (n = 800) found only 18% of the charts had documentation regarding lethal means, and among all suicidal patients who were discharged from the ED, 85% did not have any documentation of lethal means access. 24 In this current large, tertiary ED sample of over 15,000 psychiatric visits, where approximately 50% of patients seen are discharged, 31 we found a large proportion (47%) of this high-risk population with unknown access to firearms. Moreover, there appears to be a discrepancy for risk factors that might influence one asking about access to firearms and those that are associated with firearm access, leaving individuals with access and increased risk factors for suicide unassessed.
Based on this retrospective analysis, well-established risk factors for suicide, including aggression and impulsivity, substance use, and an acute stressor were associated with a lower chance of the provider knowing whether they had access to a gun. This was either the result of the assessor not asking about firearm access or else it being information unattainable for some other reason. Either way, this represents a substantial concern, given that these same risk factors correlated with a higher likelihood of firearms access. This may speak to this often-overlooked part of a psychiatric assessment or to the difficulty of these assessments while individuals are presenting acutely in the ED. Having a previous suicide attempt was associated with decreased odds of knowing about access to firearms. Past firearm suicide attempts however are associated with a 93% rate of using a firearm in a subsequent, and most often fatal, attempt 32 ; therefore, it is important to inquire into methods of past suicide attempts and continue to ask about firearm access. Current presentation with a suicide attempt, preparatory acts toward imminent suicide behavior, and SI were associated with increased odds of firearm access, without corresponding increased clinician knowledge of this access, highlighting the need for routine inquiry into firearm access in order to be able to mitigate this risk. It is also important to highlight the gap in firearms assessment among those with depression, an important risk factor in the suicide pathway, as this group was associated with an increased rate of access to a firearm.
The Clinician Prediction Scale is a subjective score of the impression of risk of future suicidal behavior and incorporates all the information gathered from the clinical assessment. The clinician prediction scores may have been influenced by whether the person had access to firearms, where access would likely increase the clinician’s impression of risk. Alternatively, several factors that could have elevated the clinician’s perception of risk, such as a current suicide attempt presentation or depression, were correlated with firearm access. Interestingly, the clinicians’ perception of suicide risk did not appear to prompt the clinician to more assertively determine the status of gun access, which highlights a gap in assessment that should likely be factoring into to the clinical risk conceptualization.
Firearm ownership and access is an essential component of a standard suicide risk assessment; 9 however, there are still significant gaps in this practice, even in individuals who have substantial risk factors. Assessment of access allows the opportunity for lethal means counseling to patients. Safer practices around firearm storage, one component of counseling, has been associated with a lower likelihood of dying by firearm. 33 It may be that clinicians are reluctant to ask about firearm access as they are unsure of the related interventions. Counselling on Access to Lethal Means, a free, online course, has demonstrated improved confidence and counseling intentions in trained mental health professionals at 3-month follow-up. 34 At the individual level, counseling about safe storage, having firearms removed from the home, and involving family members have all been proposed.
These findings must be interpreted in the context of several limitations. First, the variable that assessed firearm access assessment is based on the clinician answering “unknown” on the SAFE database or where an answer for the question was left blank altogether. We cannot say for certain if the assessor neglected to inquire about firearms or whether the information was unattainable. Our assessment of reasons for unknown firearm access is limited to data available on the SAFE form. It is possible that the question about access was asked, but that the answer was unreliable and the clinician felt it was more appropriate to mark unknown. A future qualitative study could explore assessment practices, including why clinicians did or did not ask about firearm access. Despite this, the variable is broad in its definition of access rather than ownership, which is a strength to be able to capture those that have the risk despite not having personal ownership. Second, these data do not capture mental health presentations that were not referred to psychiatry for assessment. Therefore, we cannot report data on the ED providers’ assessments of firearm access. Given previous literature on psychiatric consultation increasing the rates of lethal means assessment, 19 it is likely that we would find a decrease in firearm access assessment rates without psychiatric consultation. Third, these data represent only the practice of one psychiatric program at two hospitals in a Canadian city; assessment practices are likely to be different in other jurisdictions. Finally, we are unable to comment on how the knowledge of firearm access influenced management and if lethal means counseling took place. This would be fruitful for further study.
This study was able to use a large, consecutive clinical sample that captures close to 100% of psychiatric consultations seen at the two largest tertiary hospitals in the city. We have replicated findings of suboptimal inquiry about firearms access in a large data set and expanded the concern to the Canadian context, where firearm suicides remain an important and underrecognized problem, thereby highlighting the need for further knowledge translation about the importance of this assessment and increased standards for ensuring this is part of daily clinical assessment.
Footnotes
Authors’ Note
The funding sources had no role in the design and conduct of the study; no role in the collection, management, analysis, and interpretation of data; and no role in the preparation, review, and approval of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article was supported by research grants from the Manitoba Health Research Council (Dr. Bolton) and Canadian Institutes of Health Research New Investigator Awards (Dr. Bolton #113589).