
Abstract
Objective:
Traumatic brain injuries (TBIs) are sustained by approximately 17% of males in the general population, many of whom subsequently present mental disorders, cognitive, and physical problems. Little is known about predictors of TBIs and how to prevent them. The present study aimed to determine whether inattention–hyperactivity and/or all externalizing problems presented by boys at age 10 predict subsequent TBIs to age 34 after taking account of previous TBIs and family social status (FSS).
Method:
742 Canadian males were followed, prospectively, from age 6 to 34. Diagnoses of TBIs were extracted from health files, parents-reported sociodemographic and family characteristics at participants’ age 6, and teachers-rated participants’ behaviors at age 10. Separate logistic regression models predicted TBIs sustained from age 11 to 17 and from age 18 to 34. For each age period, two models were computed, one included previous TBIs, inattention–hyperactivity, FSS, and interaction terms, the second included previous TBIs, externalizing problems, FSS, and interaction terms.
Results:
In models that included inattention–hyperactivity, TBIs sustained from age 11 to 17 were predicted by age 10 inattention–hyperactivity (odds ratio [OR] = 1.46, 1.05 to 2.05) and by TBIs prior to age 11 (OR = 3.50, 1.48 to 8.24); TBIs sustained from age 18 to 34 were predicted by age 10 inattention–hyperactivity (OR = 1.31, 1.01 to 170). In models that included all externalizing problems, TBIs from age 11 to 17 were predicted by prior TBIs (OR = 3.66, 1.51 to 8.39); TBIs sustained from age 18 to 34 were predicted by age 10 externalizing problems (OR = 1.45, 1.12 to 1.86). Neither FSS nor interaction terms predicted TBIs in any of the models.
Conclusions:
Among males, using evidence-based treatments to reduce inattention–hyperactivity and externalizing problems among boys could, potentially, decrease the risk of TBIs to age 34. Further, boys who sustain TBIs in childhood require monitoring to prevent recurrence in adolescence.
Introduction
A meta-analysis of studies conducted in developed countries reported that traumatic brain injuries (TBIs) affect approximately 12% of the general population, males (16.7%) more than females (8.5%). 1 TBIs are the leading cause of death and disability in children and young adults 2 and can alter brain development. 3 TBIs are associated with cognitive, physical, and psychological sequelae 4 –9 that can have debilitating, often lifelong consequences. 10 As many as 77% of individuals who sustain a head injury develop depression, 11 and 53% present major depression. 12 Sustaining a TBI increases the risk of death by suicide 2-fold. 13 TBIs are also associated with increased risks of post-traumatic stress disorder, 14 anxiety disorders, schizophrenia, and bipolar disorder. 9 Sequelae depend, in part, on severity 15 and location of injury. Given the consequences of TBIs for those afflicted, their families, and the health system, knowledge of antecedents of TBIs is needed to inform prevention strategies. Studies have shown that male sex, 15 a previous TBI, 7,15,16 low socioeconomic status (SES), 17 –20 adverse life events, 21 aggressive behavior, 22 and substance misuse 22 are associated with an increased risk of TBIs.
We hypothesized that teacher ratings of childhood inattention-hyperactivity and all externalizing problems (inattention-hyperactivity, uncaring, and hurtful behaviors, and conduct problems) would predict subsequent TBIs. Two lines of evidence support our hypothesis. First, motor vehicle accidents are among the leading causes of TBIs, even among children. 17,23,24 Prospectively, collected data show that childhood inattention–hyperactivity predicted motor vehicle accidents in adolescence 25 and that childhood attention deficit hyperactivity disorder (ADHD) comorbid with conduct disorder predicted unsafe driving and injuries to age 38 26 and accidents and head injuries to age 41. 27 Childhood externalizing problems predicted accidents in adolescence 28 and nonintentional injuries to age 32. 29 Second, the prevalence of TBIs is higher among male criminal offenders than among nonoffenders. 30 –33 Robust evidence derived from investigations that prospectively followed birth or population cohorts in several countries showed that most offenders presented externalizing problems in childhood 26,29,34 –39 and that most violent crimes are committed by men with a history of externalizing problems. 34,40 –42 Thus, we reasoned that the elevated prevalence of TBIs among offenders may result from childhood externalizing problems that in turn increase the risk of motor vehicle accidents and TBIs.
To test our hypothesis, we studied a sample of Canadian males. Prospectively collected data were used to determine whether age 10 inattention–hyperactivity alone, or in combination with other externalizing problems, predict subsequent diagnoses of TBIs noted in health files to age 34. We expected that childhood inattention–hyperactivity and externalizing behaviors would be more strongly associated with TBIs in adolescence than in adulthood given the temporal proximity of predictor and outcome and the high prevalence of motor vehicle accidents in adolescence. 43 We therefore computed separate prediction models for the two age periods. As past studies have shown that sustaining one TBI increases the risk of sustaining a second TBI, 15,16,44,45 prior TBIs were entered into prediction models. Previous studies also suggest that family adversity and parent characteristics were associated with an increased risk of TBIs, 17 –21 and therefore, family social status (FSS) was included as a predictor. Interactions of predictors were entered into models. We expected that the risk of sustaining a TBI would be increased by a prior TBI accompanied by high levels of inattention–hyperactivity and/or externalizing problems among boys of families with low FSS, and among boys having experienced a prior TBI and low FSS.
Materials and Methods
Sample
Participants were males from two prospective, longitudinal investigations 46,47 recruited in Quebec when they entered school at age 6 and followed to age 34. One cohort was representative of age 6 children in Quebec, 46 the other was recruited in a deprived urban area. 47 From among these 2,631 males, we drew a sample that included all who had been charged with a criminal offense by age 24 (n = 372) and a random sample of a similar number of those with no criminal record (n = 371; see Figure S1 in Supplementary Material). Studying a sample enriched with offenders ensured sufficient cases with inattention–hyperactivity and externalizing problems to provide the necessary statistical power to robustly test whether these behaviors predicted subsequent TBIs. Of the 743 men, health files were available for 724. Of these 724 participants, 96 were missing ratings of age 10 for inattention–hyperactivity. Those with missing and complete inattention–hyperactivity data included similar proportions who sustained a TBI prior to age 11, from age 11 to 17, and from age 18 to 34. Of the 724 men with health file data, 109 were missing age 10 ratings of externalizing problems. Similar proportions of those with and without missing ratings had sustained TBIs prior to age 11, from age 11 to 17, and from age 18 to 34. Hence, the final sample of participants with complete data was 628 for models that included inattention–hyperactivity and 615 for models that included externalizing behaviors.
Measures
TBIs
The Régie de l’Assurance Maladie du Québec provided data from the health records of 724 participants. TBIs were defined by the International Classification of Disease Ninth Revision (ICD-9) codes: 800.0 to 800.9 fractures of vault of skull; 801.0 to 801.9 fractures of base of skull; 802.0 to 802.9 fracture of face bones; 803.0 to 803.9 other and unqualified skull fractures; 850.0 to 850.9 concussion; 851.0 to 851.9 cerebral laceration and contusion; 852.0 to 852.9 subarachnoid, subdural, and extradural hemorrhage, following injury; 853.0 to 853.9 other and unspecified intracranial hemorrhage following injury; 854.0 to 854.9 intracranial injury of other and unspecified nature; 959.0 head injury unspecified. Previous studies have defined TBIs by using these same ICD-9 codes. 48 –50 Diagnoses repeated within 30 days were counted as one TBI.
Childhood behaviors
When participants were age 10, their classroom teachers rated behaviors (absent = 0, sometimes present = 1, frequently present = 2) using the Social Behavior Questionnaire. 47 Inattention–hyperactivity included the sum of scores from 6 items: restless, doesn’t keep still, runs about or jumps up and down; squirmy, fidgety; poor concentration or short attention span; inattentive; gives up easily; and stares into space. Externalizing problems were indexed by the sum of ratings for inattention–hyperactivity and conduct problems (destroys own or others’ belongings; fights with other children; kicks, bites, or hits other children; doesn’t share material; irritable, quick to fly off the handle; disobedient; truant from school; has stolen things on one or more occasions), hurtful behaviors (tells lies, bullies other children, blames others, inconsiderate of others), and uncaring behaviors (items were reverse coded: takes the opportunity to praise the work of less able children, shows sympathy to someone who has made a mistake; offers to help other children who are having difficulty with a task in the classroom; and comforts a youngster who is crying or upset). Ratings for each behavior were transformed to standardized z-scores.
FSS
At participant’s age 6, mothers reported sociodemographic information. This information was used to create a composite variable that included family status (whether or not participants lived with both biological parents), biological parents’ ages at participant’s birth, education, and job prestige. 51 This measure was previously validated. 52 The higher the score, the lower FSS.
Statistical Analyses
Table S1 in Supplementary Material presents the variables used in the study. Logistic regression models were computed to determine whether age 10 inattention–hyperactivity predicted TBIs in adolescence (age 11 to 17) and in adulthood (age 18 to 34). Model 1 included two predictors, age 10 inattention–hyperactivity and a previous TBI. Model 2 added a third predictor, FSS. Consistent with much evidence, 26,27,53,54 scores for age 10 inattention–hyperactivity were significantly correlated with scores for age 10 conduct problems (r = .591, P < 0.001), hurtful behaviors (r = 0.553, p<0.001), and uncaring behaviors (r = .236, P < 0.001). A second set of regression models was computed to determine whether the sum of scores for age 10 inattention–hyperactivity, conduct problems, hurtful and uncaring behaviors would predict TBIs when taking account of previous TBIs and FSS. Lastly, regression analyses tested all two-way interactions and one three-way interaction (Inattention–Hyperactivity × Previous TBI × FSS and Externalizing Behaviors × Previous TBI × FSS). Results are reported as odds ratios with 95% confidence intervals.
On the basis of simulation studies, Peduzzi et al. 55 determined that for the estimations of a logistic regression to be accurate, the number of events per variable (EPV), defined by p/k (where p is the number of positive cases in a model, and k is the number of predictors) must be at least 10. The minimum number of positive cases needed to obtain accurate estimations (p min) can be defined as k × 10. For models including inattention–hyperactivity: To predict TBIs from age 11 to 17, the number of positive cases (40) was insufficient for models including interaction terms, and sufficient for models including direct effects (p min = 30); To predict TBIs from age 18 to 34, the number of positive cases (72) was sufficient for models with and without interaction terms. For models including externalizing problems: To predict TBIs from age 11 to 17, the number of positive cases (39) was insufficient for models including interaction terms but sufficient for models including only direct effects; To predict TBIs from age 18 to 34, the number of positive cases (70) was sufficient for models with and without interaction terms.
Ethics Approval
Initially, parents provided consent for participants’ teachers to rate their child’s behavior and also consented to their own participation in the study. Once participants were 18 years old, they provided consent. The Commission d’Accès à l’Information de Québec approved the use of data from health files. The study was approved by ethics committees at the Université de Montréal, Centre Hospitalier Universitaire Sainte-Justine, and the Institut Philippe-Pinel de Montréal.
Results
From the 628 males with complete data for inattention–hyperactivity, 152 (24.2%) had sustained at least one TBI, 47 (7.5%) had sustained a TBI prior to age 11, 42 (6.7%) from age 11 to 17, and 78 (12.4%) from age 18 to 34. The average age at first TBI was 17.00 years (SD = 8.27; range 1.8 to 34.4). The mean number of TBIs was 0.32 (SD = 0.68, range 0 to 6), and the median was 0. The majority (117) of participants who sustained TBIs sustained only one. From the 615 males with complete data for externalizing problems, 149 (24.2%) had sustained at least one TBI, 46 (7.5%) had sustained a TBI prior to age 11, 41 (6.7%) from age 11 to 17, and 76 (12.4%) from age 18 to 34. The average age at first TBI was 17.06 years (SD = 8.33; range 1.78 to 34.43). The mean number of TBIs was 0.32 (SD = 0.67, range 0 to 6) and the median was 0. The majority (115) of participants who sustained TBIs sustained only one.
Does Inattention–Hyperactivity at Age 10 Predict Subsequent TBIs?
Results are presented in Table 1. The first model indicated that sustaining a TBI from age 11 to 17 was predicted by age 10 inattention–hyperactivity and previous TBIs. Model 2, where FSS was added as a predictor, showed that the risk of sustaining a TBI in adolescence was increased 1.46 (1.05 to 2.05) times by each increase of one in the standardized score for inattention–hyperactivity and 3.49 times (1.48 to 8.24) by a previous TBI. None of the interaction terms were significant.
Results of Logistic Regression Models Predicting Traumatic Brain Injuries (TBIs) from Age 11 to 17 and 18 to 34 Years by Age 10 inattention–Hyperactivity and Family Social Status.
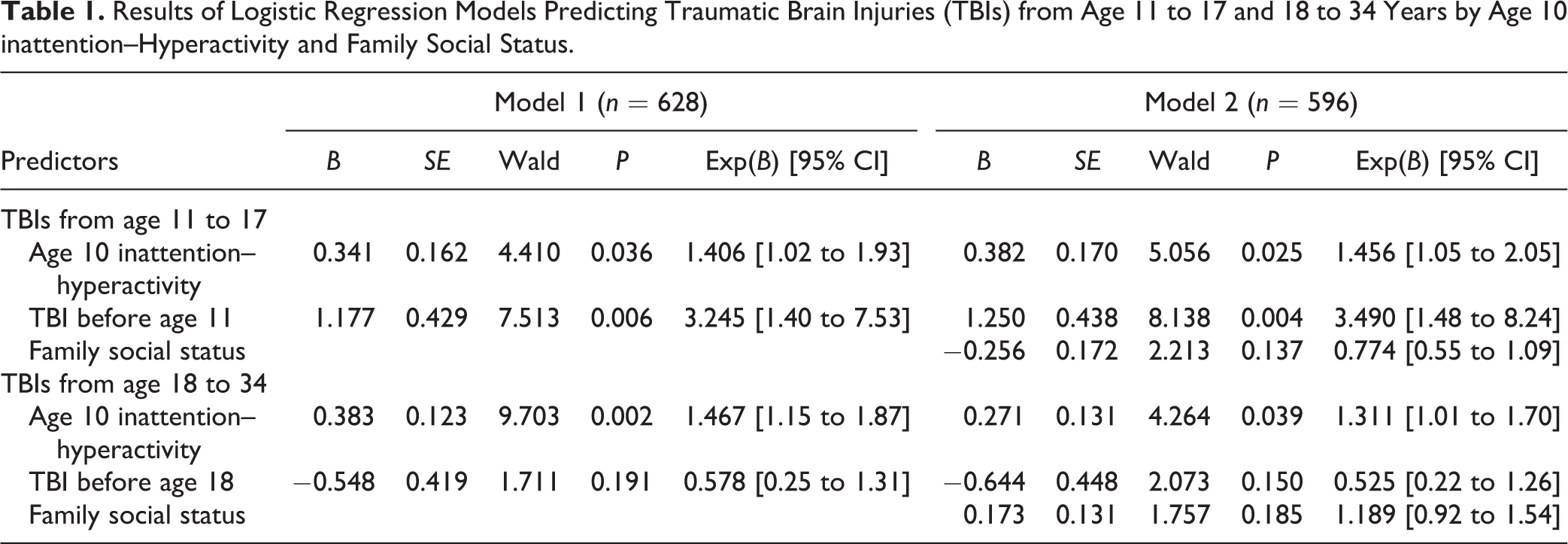
As also shown in Table 1, TBIs sustained from age 18 to 34 were predicted by age 10 inattention–hyperactivity and previous TBIs. In Model 2, sustaining a TBI in adulthood was not predicted by TBIs prior to age 18 nor by FSS. Rather, each increase of one in the standardized score for age 10 inattention–hyperactivity was associated with a 1.31 (1.01 to 1.70) increase in the risk of TBIs in adulthood. None of the interaction terms were significant. Figure 1 illustrates the percentages of participants who sustained TBIs from age 11 to 17 and from age 18 to 34 as a function of prior TBIs and inattention–hyperactivity.
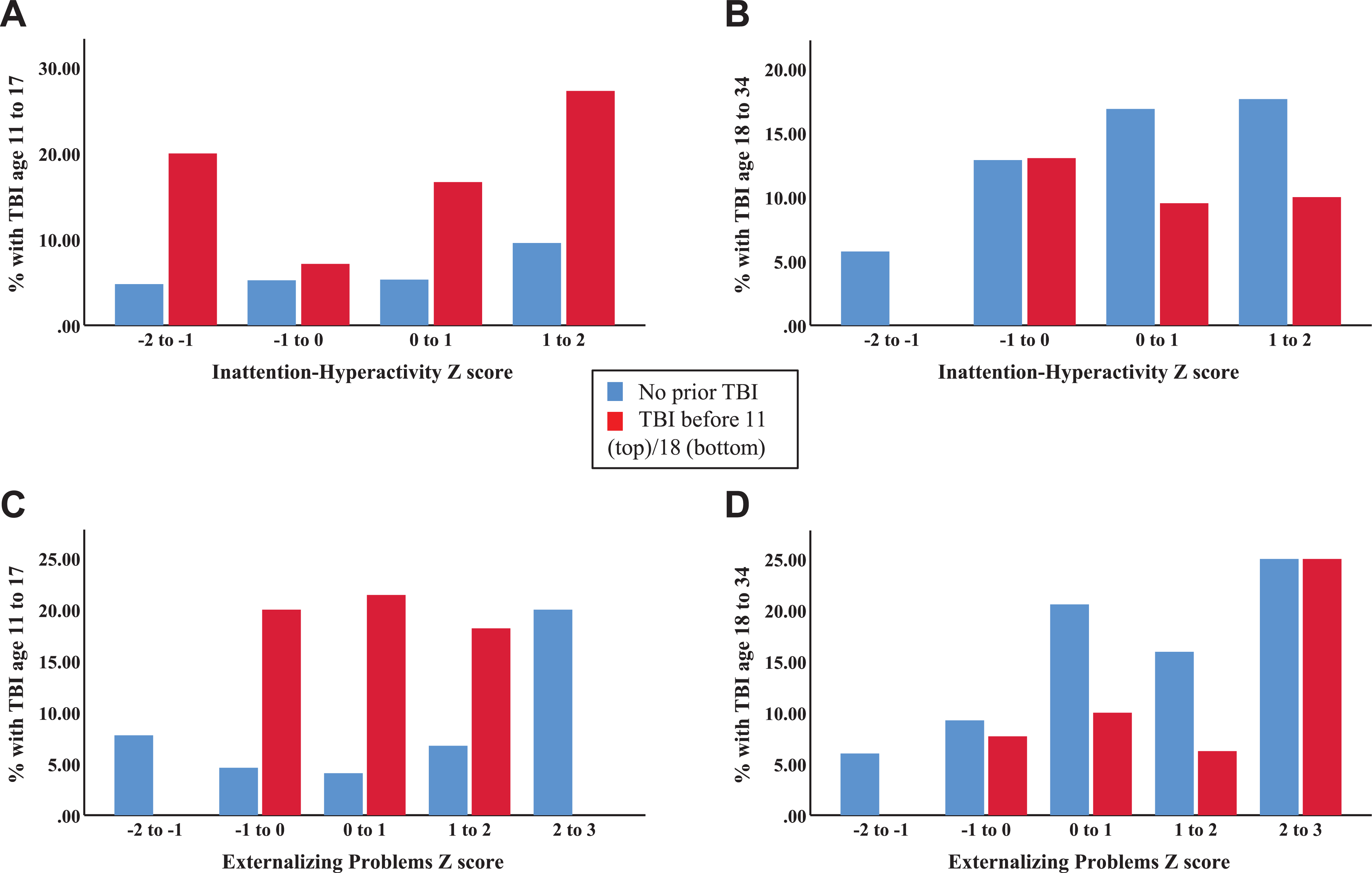
Percentages of participants who experienced a traumatic brain injury as a function of previous traumatic brain injuries and age 10 inattention–hyperactivity or externalizing problems. (A) TBI from age 11 to 17, age 10 inattention-hyperactivity. (B) TBI from age 18 to 34, age 10 inattention-hyperactivity. (C) TBI from age 11 to 17, age 10 externalizing problems. (D). TBI from age 18 to 34, age 10 externalizing problems.
Post Hoc Analyses
Most boys presenting ADHD also present other externalizing problems. 56,57 Therefore, we conducted exploratory analyses to determine whether inattention–hyperactivity accompanied by low ratings for other externalizing problems was associated with an increased risk of sustaining a TBI. For both inattention–hyperactivity and externalizing (without inattention–hyperactivity), we defined low scores as a z-score of −1.5 to 0, and high scores as 0 to 1.5. Participants were classified by low and high scores for inattention–hyperactivity and other externalizing problems. Proportionately more of the boys with high inattention–hyperactivity and low other externalizing (15.5%) as compared to boys with low scores for both measures (7.1%) sustained TBIs from age 18 to 34, χ2(N = 336) = 5.22, P = 0.022. The proportions who sustained TBIs from age 11 to 17 were similar.
Do Externalizing Problems at Age 10 Predict Subsequent TBIs?
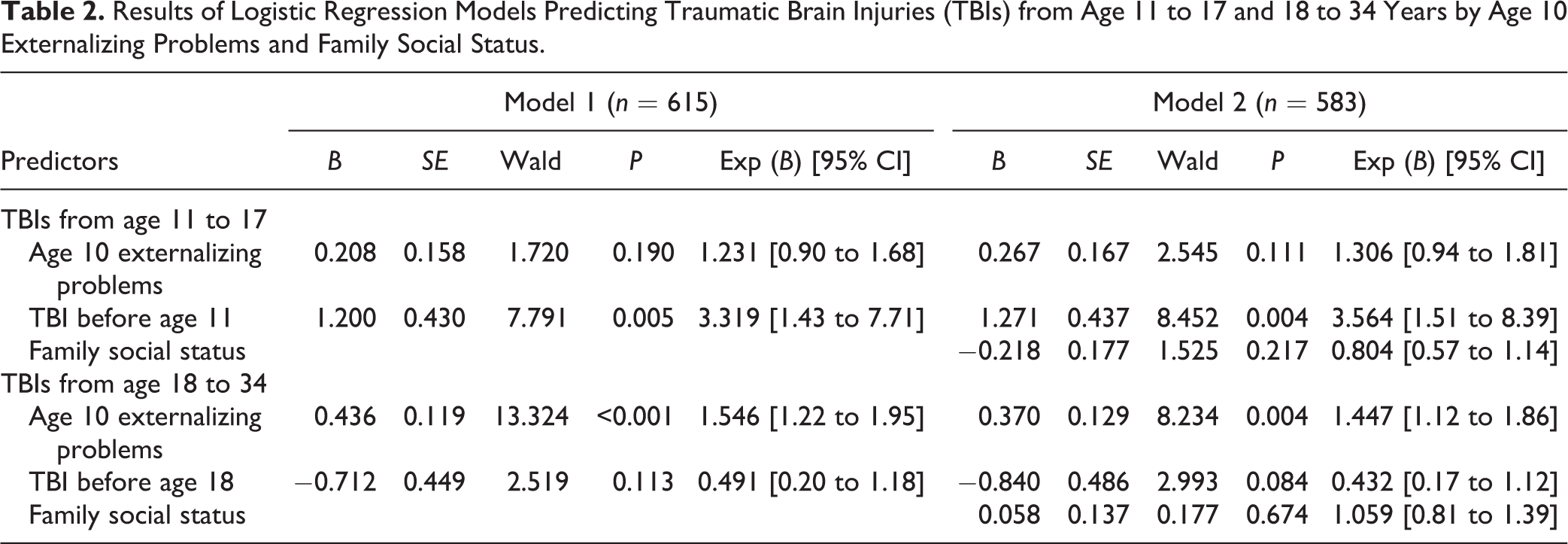
A total score for inattention–hyperactivity, conduct problems, hurtful and uncaring behaviors was calculated for each participant. As presented in Table 2, the risk of sustaining a TBI in adolescence was increased approximately 3.5 times in each model by a previous TBI, but not by the age 10 externalizing score or FSS. By contrast, sustaining a TBI from age 18 to 34 was predicted by age 10 scores for externalizing problems, and not by previous TBIs or FSS. In Model 2, each increase of one in the age 10 standardized externalizing problems score was associated with a 1.45 (1.12 to 1.86) increase in the risk of TBIs in adulthood. No interaction terms were significant. In the bottom panel of Figure 1, the percentages of participants who sustained TBIs from age 11 to 17 and from age 18 to 34 are presented as a function of prior TBIs and externalizing scores.
Results of Logistic Regression Models Predicting Traumatic Brain Injuries (TBIs) from Age 11 to 17 and 18 to 34 Years by Age 10 Externalizing Problems and Family Social Status.
Ensuring Generalizability
The present sample was enriched with criminal offenders as these men are very likely to have presented externalizing problems in childhood. 26,29,34 –39 In order to increase confidence in the generalizability of results, analyses were rerun among only the nonoffenders. Despite the smaller sample size, results were similar to those reported for the whole sample (see Supplementary Material).
Discussion
Prospectively collected data indicated that among males, teacher ratings of inattention–hyperactivity at age 10 predicted TBIs from age 11 to 17 and from age 18 to 34. Teacher ratings of age 10 externalizing behaviors did not predict TBIs sustained from age 11 to 17 but did predict TBIs sustained from age 18 to 34. Additionally, TBIs sustained prior to age 11 predicted TBIs from age 11 to 17, but TBIs sustained prior to age 18 did not predict TBIs from 18 to 34. FSS did not predict TBIs at any age. Thus, as illustrated in Figure 1, TBIs sustained in adolescence were associated with previous TBIs and high levels of inattention–hyperactivity, while TBIs sustained from age 18 to 34 were associated with inattention–hyperactivity and with a total score for age 10 externalizing problems. These findings are consistent with previous studies showing that childhood inattention–hyperactivity and externalizing problems were associated with increased risks of motor vehicle accidents, 25 –29 a primary cause of TBIs, 17,23,24 from adolescence through the third decade of life. The findings from the present study are also consistent with reports that male offenders, most of whom have a history of childhood externalizing problems, are at elevated risk to sustain TBIs. 30 –33
Our finding that childhood TBIs were associated with an increased risk of TBIs in adolescence, although TBIs prior to age 18 did not increase risk of TBIs in adulthood, is consistent with results from a Swedish study 45 showing that recurrence was more likely after a childhood TBI than after an adolescent TBI. While previous studies have shown that sustaining a TBI increases the risk of future TBIs, 44,58 –63 the risk of recurrence varies not only by age at first TBI and length of follow-up 45,62 –64 but also by sample characteristics (community, 22,45,63,65,66 prisoners, 67 sex, ethnicity 64 ), self-report or medical diagnosis, 62,68 cause of injury, 15 severity of first TBI, 45,69 engagement in sports, 16,22 alcohol intoxication, 63 and seizure disorder. 64,69
In our study, FSS of the family of origin was not associated with TBIs, consistent with results from a New Zealand birth cohort showing that neither SES nor family living standard was associated with child/adolescent TBIs, 21 and those from the British Columbia Trauma Registry showing that, of several measures of SES, only the percentage of people aged 15 and older in the neighborhood without a high school diploma was related to TBIs. 17 In a large UK cohort, low SES of the family was associated with the child/adolescent not experiencing a TBI. 66
Results of the present study extend previous findings 25 –27 by showing that childhood inattention–hyperactivity and externalizing problems were associated specifically with an increased risk of TBIs to age 34. inattention–hyperactivity at age 10 predicted TBIs up to age 34, but as would be expected inattention–hyperactivity was strongly correlated with other externalizing problems. Recent studies show that externalizing problems precede Inattention problems and that the correlation between inattention and externalizing problems continues to increase to age 20. 70 In the present study, it was the total score for these childhood problems that predicted TBIs in adulthood, but not in adolescence. Robust evidence shows that the earlier the onset of externalizing problems, the greater the likelihood of antisocial and aggressive behaviors through adolescence and adulthood. 71 Thus, it is reasonable to speculate that the boys with the highest ratings of externalizing problems at age 10 would have displayed similar problems in adolescence and adulthood. In addition, most would have begun misusing substances early in adolescence and developed substance use disorders in adulthood. 72 Such boys engage in risky behaviors at all ages, but as they age, risky behaviors become more dangerous. By age 18, they drive motor vehicles, often when intoxicated, and they fight with peers who use weapons, thereby increasing the risk of incidents that may lead to TBIs. This scenario may explain why age 10 externalizing problems did not predict TBIs sustained in adolescence but did predict TBIs sustained from age 18 to 34. TBIs sustained in adolescence are reported to result, principally, from accidents occurring when playing organized sports. 22,73 Boys with externalizing problems are less likely than healthy boys to participate in organized sports as they have difficulty following rules. 74,75 This may be an additional reason why childhood externalizing problems are not associated with an increased risk of TBIs in adolescence, but only from age 18 through 34 when the likelihood of accidents resulting from risky behaviors dramatically escalates. While statistically significant, childhood inattention–hyperactivity and externalizing problems are associated with a moderate increase in the risk of TBIs, indicating a need for future investigations that prospectively measure the multiple factors that increase and that decrease the risk of TBIs.
The results of the present study, if replicated, suggest that the interventions that effectively reduce childhood inattention–hyperactivity 76 and externalizing problems 77 could, potentially, reduce the risk of subsequent TBIs and their physical and psychological sequelae. This hypothesis requires testing. The present results add to previous evidence showing that children who sustain TBIs are at elevated risk to sustain similar injuries in adolescence and thus require monitoring. Further, knowledge of behavioral, environmental, and family factors promoting TBIs and factors promoting recurrence of TBIs is also needed.
Limitations and Strengths
The sample was relatively small. According to the Peduzzi et al.’s 55 criteria, the number of participants who sustained TBIs in adolescence was insufficient for prediction models that included interaction terms, but the number who sustained TBIs from age 18 to 34 was sufficient for prediction models that included interaction terms. The number of TBIs may have been underestimated by using ICD codes to identify TBIs, as a Canadian study reported that one in six patients with concussion signs and symptoms were misdiagnosed in emergency departments. 78 Additionally, TBIs may have been underestimated by counting diagnoses given within a 30-day period as one TBI. This was done because physicians were required to record a diagnosis each time they saw a patient. Another limitation may be that diagnosing TBIs has changed over the decades during which data were collected, mid-1980s to 2013. Further, previous studies suggested that TBIs may lead to externalizing problems. One study found that TBIs requiring hospitalization sustained before age 5 predicted inattention–hyperactivity and externalizing behaviors in adolescence. 79 Two other studies reported an increase in aggressive behavior following child/adolescent TBIs, 80,81 others did not. 82 However, we found no significant difference in inattention–hyperactivity and externalizing scores between boys who had, and who had not, sustained TBIs before age 10. Finally, only males were studied. While inattention–hyperactivity 83 and externalizing problems 84,85 are at least twice as prevalent among boys than girls, stability into adulthood is similar. 29 Studies are needed to determine whether these childhood problems are linked to TBIs in females. Strengths of the study include the use of health records to identify TBIs, information on sociodemographic characteristics of participants’ parents, composition and SES of the family of origin at age 6, and teacher ratings of inattention–hyperactivity and externalizing problems at age 10.
Conclusion
Boys who sustain TBIs constitute a population-at-risk for further TBIs in adolescence. High levels of inattention and hyperactivity observed by teachers at age 10 were a precursor of TBIs to age 34. Boys who sustained a TBI in childhood and who displayed inattention and hyperactivity have an especially high risk for subsequent TBIs. Additionally, boys who presented high levels of externalizing problems at age 10 were at risk to sustain a TBI from age 18 to 34, probably as a result of increasingly reckless behavior. Future studies are needed to determine whether evidence-based treatments to reduce childhood inattention–hyperactivity and externalizing problems lower the risk of future TBIs.
Supplemental Material
Supplemental Material, 882171_Supplementary_material - A Prospective Study of Childhood Predictors of Traumatic Brain Injuries Sustained in Adolescence and Adulthood
Supplemental Material, 882171_Supplementary_material for A Prospective Study of Childhood Predictors of Traumatic Brain Injuries Sustained in Adolescence and Adulthood by Guido I. Guberman, Marie-Pier Robitaille, Peter Larm, Alain Ptito, Frank Vitaro, Richard E. Tremblay and Sheilagh Hodgins in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors thank the participants, their families, and their teachers for their long-term contributions to this study, and the staff of the Research Unit on Children’s Psychosocial Maladjustment for their assistance with administration and data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the longitudinal study has been provided by the Fonds Québécois de la Recherche sur la Societé et la Culture, Fonds de Recherché du Québec—Santé (FRQS), Social Sciences and Humanities Research Council of Canada, and Canadian Institutes of Health Research. Support for this study also comes from a Doctoral Training for Medical Students Award (to G. Guberman) from the FRQS, a Tomlinson Doctoral Fellowship (to G. Guberman) from McGill University, and a Vanier Canada Graduate Scholarship (to G. Guberman) from the Canadian Institutes of Health Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.