
Abstract
Background:
Post-traumatic stress disorder (PTSD) and depression are common mental disorders in individuals experiencing traumatic events. To date, few studies have studied the relationship between genetic basis and phenotypic heterogeneity of traumatized individuals. The present study examined the effects of four FKBP5 SNPs (rs1360780, rs3800373, rs9296158, and rs9470080) in four postdisaster groups (low symptom, predominantly depressive, predominantly PTSD, and combined PTSD-depression symptom groups) as identified by latent profile analysis.
Methods:
A total of 1,140 adults who experienced the 2008 Wenchuan earthquake participated in our study. Earthquake-related trauma, PTSD, and depressive symptoms were measured using standard psychometric instruments. The four FKBP5 SNPs were genotyped using a custom-by-design 2 × 48-Plex SNP scan™ Kit.
Results:
After adjusting for covariates, the main and gene–environment interaction effects of rs9470080 were all significant when the combined PTSD-depression group was compared with the low symptoms, predominantly depression and predominantly PTSD groups. rs9470080 TT genotype carriers had a higher risk of developing high co-occurring PTSD and depression symptoms than the C allele carriers. However, when trauma exposure was severe, the TT genotype carriers and C allele carriers did not differ in the risk of developing high co-occurring PTSD and depressive symptoms. The other three SNPs demonstrated no significant effects. Moreover, the rs3800373-rs9296158-rs1360780-rs9470080 haplotype A-G-C-T was found significantly associated with combined PTSD-depression symptoms.
Conclusion:
Our findings support the genetic basis of phenotypic heterogeneity in people exposed to trauma. Furthermore, the results reveal the possibility that the variants of FKBP5 gene may be associated with depression-PTSD comorbidity.
Introduction
More than 70% of individuals have experienced one or more traumatic events during their lifetime. 1 Most people, after experiencing traumatic events, do not develop mental disorders, but some individuals may develop depressive symptoms, post-traumatic stress disorder (PTSD) symptoms, or both. 2 Exposure to severe traumatic events such as disasters may increase the risk of PTSD and major depressive disorder (MDD). 3 The high prevalence of PTSD (43.9%) and depression (20.9%) was also reported in postdisaster samples in China. 4 Epidemiological studies emphasized the high comorbidity rate between PTSD and MDD, 5 and according to recent review, approximately half of PTSD patients suffered from comorbid MDD. 6 The postdisaster MDD percentage of PTSD patients was reported as high as 55%. Why some individuals suffer from depression, while others develop PTSD, or both requires further clarification after similar trauma exposures clarified. 2 To date, only a few studies have focused on identifying the psychological and biological factors that contribute to the heterogeneity of stress response symptoms in people exposed to trauma.
Family studies and twin studies have shown that both PTSD and depression are moderately inherited. The heritability of PTSD was estimated to be 49%. 7 The most recent molecular studies have shown slightly lower estimates 8 (29% for European American (EA) females and 0 for EA males), and this heritability may be underestimated due to underpowered sample size. 9 According to a meta-analysis, the heritability of depression is within a similar range 10 (37%). Twin studies have also shown shared genetic factors predisposed to the development of PTSD and depression. Koenen et al. 11 reported that shared genetic liability explained 62.5% of MDD-PTSD comorbidities using a bivariate twin model. In another study, complete correlation between genetic factors and PTSD or MDD (r = 1.0) was obtained. 12 As genetic factors were found to be associated with both PTSD and depression, it should be queried whether genetic factors might also be responsible for their comorbidities and contribute to the biological basis of the phenotypic heterogeneity among individuals after trauma exposure.
FK-506 binding protein 5 (FKBP5) is a co-chaperone of a heat shock protein 90 kDa (Hsp90) that regulates glucocorticoid receptor (GR) sensitivity. 13 Overexpression of FKBP5 reduces hormone binding affinity and nuclear translocation of GR, thereby reducing GR sensitivity. 14 Reducing the GR sensitivity will result in impaired negative feedback of the hypothalamic-pituitary-adrenal (HPA) axis, and thus an increase in cortisol levels following trauma exposure, which is associated with many stress-related mental disorders. Therefore, these FKBP5 polymorphisms associated with higher FKBP5 levels would increase the risk of stress-related psychopathologies such as depression. 15 Alleles associated with higher FKBP5 expression were also found to increase GR sensitivity and lead to PTSD symptoms in PTSD patients. 16 Klengel et al. 17 found that an allele-specific FKBP5 DNA demethylation induced by childhood trauma increased the risk of stress-related disorders such as PTSD and depression, which supported the Gene × Environment (G × E) interaction of FKBP5 gene. G × E studies on PTSD and depression showed significant interaction effects between FKBP5 genotype and childhood trauma exposure. 18,19 Given that the G × E effect of FKBP5 gene has previously been reported in PTSD and depression, FKBP5 is a good candidate for examining the G × E contribution to the phenotypic heterogeneity of post-traumatic psychopathology.
In previous studies, the status of comorbidities was usually defined by the dichotomy diagnosis status. For example, for MDD and PTSD, we can divide into four subgroups based on Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnostic criteria or scale cutoffs: healthy control, PTSD only, MDD only, and comorbid MDD-PTSD groups. But this approach may have problems. The main limitation is the patients’ symptom heterogeneity. There are 636,120 symptom combinations meeting the DSM-5 criteria for PTSD and 227 combinations for MDD, suggesting that there should be high clinical heterogeneity in the subgroups defined by the diagnosis status. 20 As mentioned earlier, potential clinical heterogeneity may be an important factor threatening the replication of PTSD and MDD genetic studies. 21 To address this issue, it is strongly recommended to subdivide the phenotypes into subgroups using novel person-centered statistical methods. 20,22 Recent studies have found that the use of person-centered methods to refine phenotype has greatly improved the effect size and replication rate of genetic studies of MDD. 23
Therefore, to account for the underlying clinical heterogeneity and improve the robustness of our results, we performed person-centered approaches to define the status of MDD-PTSD comorbidities in our sample. Latent profile analysis (LPA) was performed to identify subgroups of individuals with a common PTSD-depression comorbidity pattern after trauma. LPA is a person-centered clustering method used to find meaningful populations who respond similarly to measured variables without using a priori cutoff score. LPA was found to be particularly advantageous over traditional priori categorization methods because it can correctly identify individuals with symptoms close to the preselected defined cutoff score and allows researchers to move beyond examining the presence or absence of pathology by categorization approaches. 24,25 Also, LPA is able to uncover unobserved heterogeneity in the population 26 and has been widely used to investigate co-occurring PTSD and depressive symptoms after trauma. 24,27 –29
The purpose of the current study was to examine whether FKBP5 gene polymorphism contributed to post-trauma symptom profiles (PTSD and depression) in Chinese who were exposed to a deadly earthquake. Considering that rs1360780, rs3800373, rs9296158, and rs9470080 are the majority of reported SNPs of the FKBP5 gene, which are shown to be associated with post-traumatic psychopathologies, 30,31 these SNPs were genotyped as candidate gene loci in this study. We studied 1,140 adult survivors of the 2008 Whenchuan earthquake. The samples were divided into four groups using LPA: low symptoms, predominantly depressive symptoms, predominantly PTSD symptoms, and combined PTSD-depression symptoms. 32
Methods
Participants and Procedures
The sample was recruited from one of the largest reconstruction communities located in Hanwang Town, Mianzhu City. The 2008 Whenchuan earthquake almost completely destroyed the town. The sample is an epidemiological sample of Chinese adult earthquake survivors, and the detailed sampling procedures have been introduced before. 32 We conducted the survey about 5½ years after the earthquake. Participants who personally experienced the earthquake and were at least 16 years old at the time of data collection were included. Exclusion criteria included diagnosis of mental retardation or major psychosis (e.g., schizophrenia and organic mental disorders). All participants understood the purpose of the study and signed an informed consent before completing the self-reported questionnaire. After that, peripheral blood samples were collected and processed for genotyping. Fifty-six participants were not genotyped because of refusal to draw blood (24 participants), DNA extraction failure (26 participants), and DNA genotyping failure (6 participants). Our participants were predominantly adults aged 18 to 65 years (98.5%, mean age = 48.1, SD = 10.0). Detailed demographic information of the participants is shown in Table 1. The study protocol was approved by the Institutional Review Board of the Institute of Psychology, Chinese Academy of Sciences.
Participants’ Demographic Information.
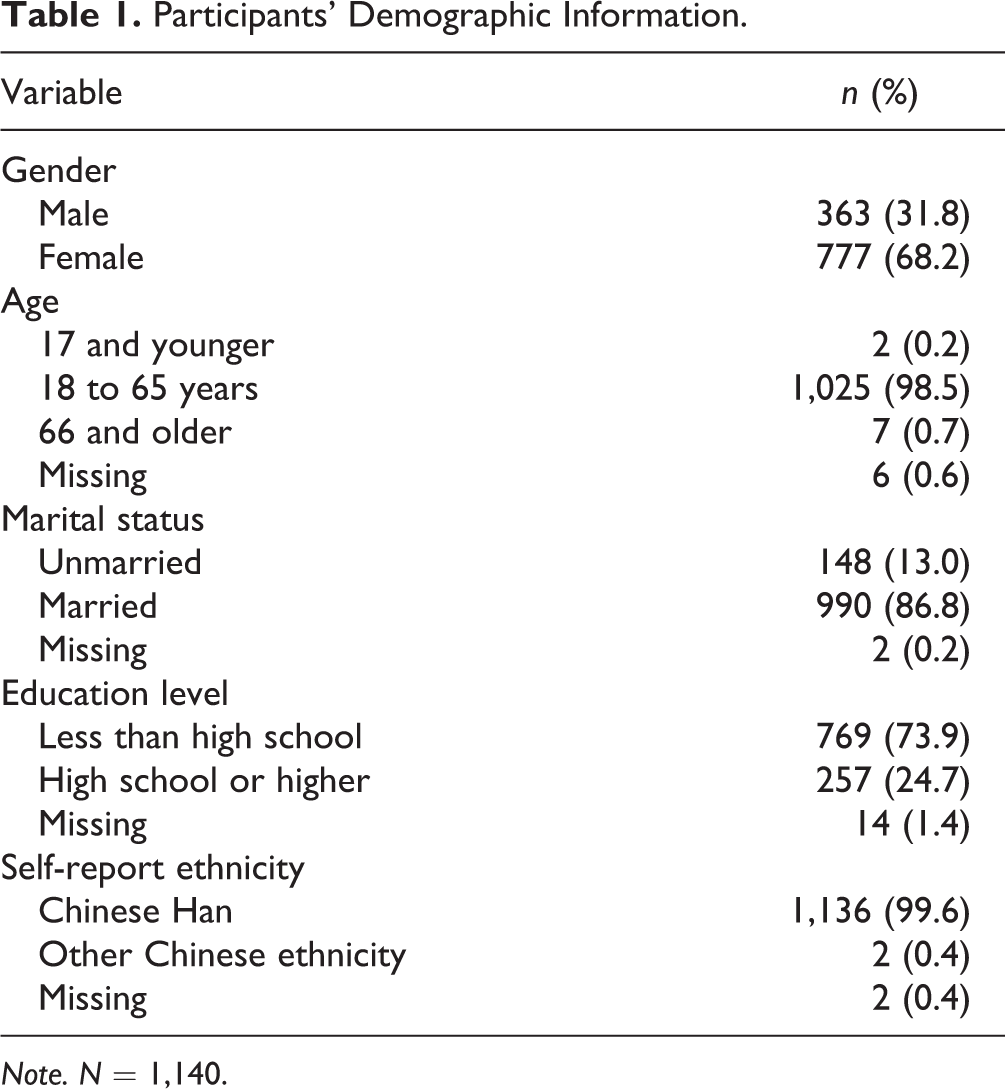
Note. N = 1,140.
Measures
Earthquake-related trauma exposures were assessed by a 10-question questionnaire asking whether people had experienced (1) being trapped under rubble, (2) being injured, (3) being disabled due to injuries, (4) participating in rescue efforts, (5) witnessing a death of someone, (6) exposure to mutilated bodies, (7) traumatic death of a family member, (8) traumatic injury of a family member, (9) traumatic death of a friend or neighbor, and (10) losing livelihood due to the disaster. Each item was rated with either 0 (no) or 1 (yes). The total score of the questionnaire was used to reflect the level of trauma exposure. This Earthquake Trauma Exposure Questionnaire has been used in Chinese samples before. 32 The PTSD symptoms were assessed using a PTSD Checklist for DSM-5 33 (PCL-5). PCL-5 is a self-report checklist of 20 PTSD symptoms defined in DSM-5. Each item is rated on a 5-point Likert-type scale, reflecting the severity of a particular symptom from 0 (not at all) to 4 (extremely) during the past month. PCL-5 is referred as the “Wenchuan Earthquake” in our study. The Cronbach’s α for the PCL-5 was 0.95 in the current sample. Depressive symptoms were assessed using the Center for Epidemiological Studies–Depression Scale 34 (CES-D). CES-D is a 20-item self-reported checklist. Each item is rated on a 4-point Likert-type scale, reflecting the severity of depressive symptoms from 0 (rare or none of the time/less than 1 day) to 3 (most or all of the time/5 to 7 days) during the past month. In this study, Cronbach’s α for CES-D was 0.87.
Genotyping
DNA was extracted from peripheral blood samples using a standard protocol. 35 Genotyping of rs1360780, rs3800373, rs9296158, and rs9470080 was conducted using a custom-by-design 2 × 48-Plex SNP scan™ Kit (Genesky Biotechnologies Inc., Shanghai, China). Sample DNA (10 ng) was amplified by polymerase chain reaction (PCR) using the 3730 DNA Analyzer (Applied Biosystems, Foster City, CA, USA). Genotyping was based on double ligation and multiplex fluorescence PCR. The raw data were analyzed based on the fragment size of the allele-specific ligation-PCR product by GeneMapper 4.1 (Applied Biosystems) software. The genotype call rate was higher than 98%.
Statistical Analysis
The first step was to use LPA to identify underlying PTSD-depression comorbidity patterns in the current sample. We found a four-class solution characterized by low symptoms (53.9%), predominantly depression (18.2%), predominantly PTSD (18.9%), and combined PTSD-depression patterns (9.0%), which best described the symptom profiles of our sample. The LPA was performed based on eight sum scores for four PTSD factors (intrusion, avoidance, negative alterations in cognitions and mood, and hyperarousal) and four depressive factors (depressive affect, positive affect, somatic complaints, and interpersonal problems) using Mplus Version 7.0. One-class to five-class solutions of LPA models were compared based on model fitting indices such as Bayesian information criterion, entropy, and Lo–Mendell–Rubin likelihood ratio test. Other detailed information of the LPA was described in our previous work. 32
Based on the results of LPA, we conducted multinomial logistic regression analyses to examine whether the main effect and G × E effect of FKBP5 gene would distinguish the combined PTSD-depression group from the other groups for each SNP using R 3.5.0. The combined PTSD-MDD symptom group was set as reference in the multinomial logistic regression model to compare with other three groups. SNPs and earthquake-related trauma exposure were used as independent variables, and symptom presentation groups were set as dependent variables. The main effects of trauma severity and the genotype, as well as interaction effect, were simultaneously included in the regression model. Demographic characteristics such as age, sex marital status, and educational level were controlled as covariates. α was set to 0.05. For correction of multiple comparisons, permutation tests (number of permutations = 1,000) were performed using R 3.5.0.
After a Gene × Environment interaction was found, we tested the simple effects of the gene. Our sample was divided into two groups: low trauma exposure group (trauma exposure ≤ 3) and high trauma exposure group (trauma exposure > 4) based on the median level of trauma exposure. We examined whether different genotypes distinguished the individuals in combined PTSD-depression group from others in the low and high trauma exposure groups, respectively. Simple effects were examined by logistic regression analyses, and the covariates were the same as those in the Gene × Environment interaction analysis.
Haplotype Analysis
For the four FKBP5 SNPs (rs3800373, rs9296158, rs1360780, and rs9470080), we employed Haploview 4.3 36 to perform linkage disequilibrium (LD) analysis. The results showed that the four SNPs are in high LD with each other (r2 > 0.7) and form an LD block (see Supplemental Figure 1). Then, we used expectation–maximization (EM) algorithm implemented in PLINK 1.07 37 to estimate haplotype frequency of the haplotypes. The results are shown in Supplemental Tables. Next, we estimated individual-level haplotype count by PLINK and used multinomial logistic regression implemented in R to perform haplotype-based association test for the symptom group comparisons. The logistic regression model was set similarly to the single SNP analysis. A permutation analysis was performed for haplotype-based analysis.
Results
Participants in the study experienced severe trauma during the 2008 Wenchuan earthquake, indicated by a mean exposure score of 3.5 (SD = 1.8; range: 0 to 10). The mean score of PCL-5 was 18.8 (SD = 13.5; range: 1 to 77), and the mean score of CES-D was 17.0 (SD = 8.6; range: 0 to 48) in the final sample. No effects of rs1360780, rs3800373, or rs9296158 were found (see Supplemental Tables), and we mainly introduced the results of rs9470080 here. The allele distribution of FKBP5 rs9470080 in the whole sample was in Hardy–Weinberg equilibrium (χ2 = 0.03; P = 0.86). According to previous studies, 38 the CC and CT genotypes were further grouped into C+ group to compare with TT homozygotes. Table 2 shows the allele distribution of rs9470080 in the four groups divided by LPA. We performed ANOVA with trauma exposure as a dependent variable and FKBP5 genotype as a factor to test whether trauma exposure was different across different genotypes in all four groups. No significant differences in trauma exposure were found between participants with different FKBP5 genotypes in the low symptoms group, F(2, 613) = 0.185, P = 0.831, predominantly depression group, F(2, 200) = 0.279, P = 0.757, predominantly PTSD group, F(2, 216) = 0.816, P = 0.443, and combined symptoms group, F(2, 99) = 1.746, P = 0.18. As shown in Table 3, there were significant main effects of rs9470080 genotype on symptom profiles. TT homozygotes tended to enter the combined symptom group compared with the low symptoms group (odds ratio [OR] = 0.120, P = 0.003, P permutation = 0.009), predominantly PTSD group (OR = 0.135, P = 0.011, P permutation = 0.018), and predominantly depression group (OR = 0.212, P = 0.052, P permutation = 0.064).
Frequencies of FKBP5 rs9470080 Alleles in Four Groups Divided by Latent Profile Analysis.

Note. N = 1,140. PTSD = post-traumatic stress disorder.
Logistic Regression Analysis of Trauma Exposure and rs9470080 Genotypes and Their Interaction for Different PTSD and Depression Symptom Presentations.
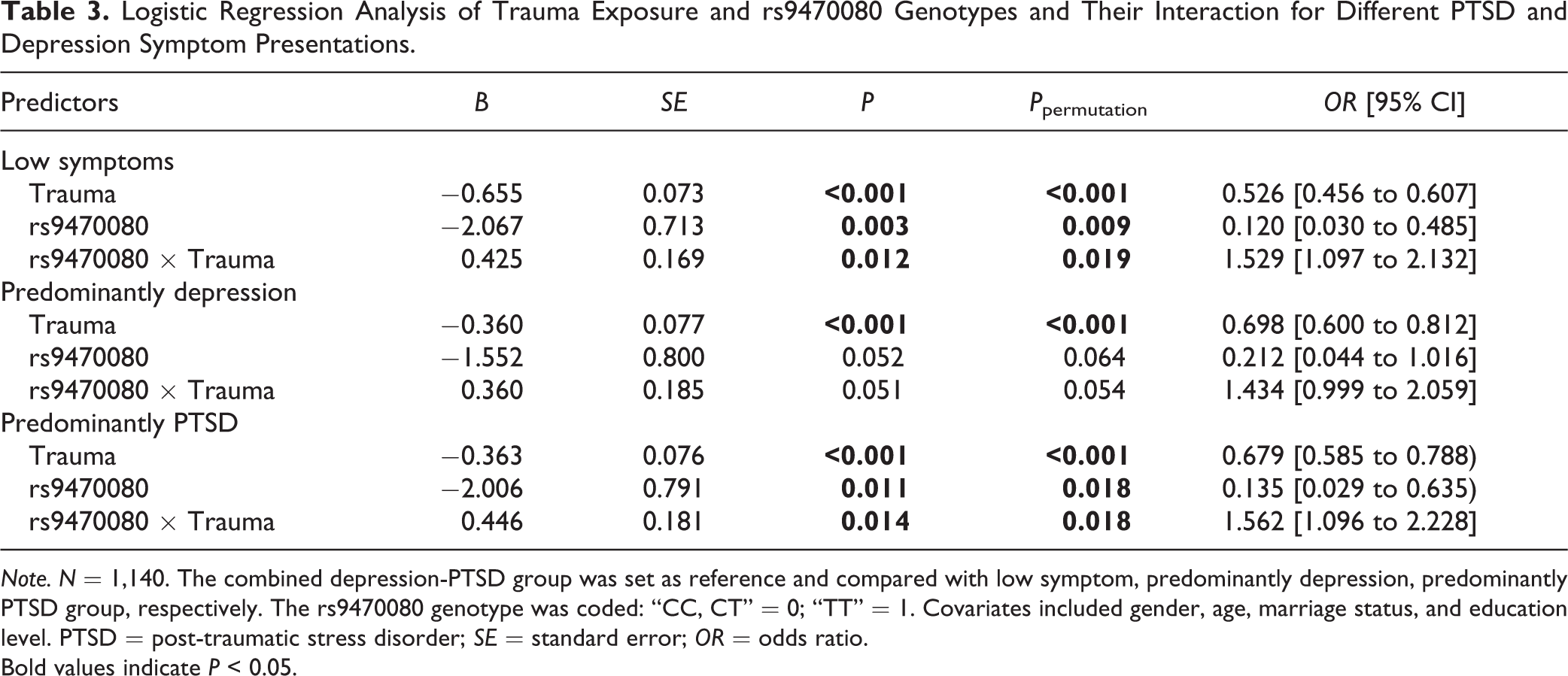
Note. N = 1,140. The combined depression-PTSD group was set as reference and compared with low symptom, predominantly depression, predominantly PTSD group, respectively. The rs9470080 genotype was coded: “CC, CT” = 0; “TT” = 1. Covariates included gender, age, marriage status, and education level. PTSD = post-traumatic stress disorder; SE = standard error; OR = odds ratio.
Bold values indicate P < 0.05.
The effect of Trauma Exposure × Genotype interaction was also revealed. Specifically, the interaction effect was significant when the combined symptom group was compared with the low symptoms group (OR = 1.529, P = 0.012, P permutation = 0.019), predominantly PTSD group (OR = 1.562, P = 0.014, P permutation = 0.018), and strong but nonsignificant trend when compared with the predominantly depression group (OR = 1.434, P = 0.051, P permutation = 0.054). That is to say, TT genotype of rs9470080 was no longer a risk factor for developing combined PTSD and depression when people experienced more severe trauma (see Figure 1). The gene–environment interaction effect was not present when comparing the other three—depression, PTSD, and low symptoms groups (all P > 0.6). According to the simple effect analysis (see Table 4), for individuals in the low trauma exposure group, rs9470080 genotype TT was a risk factor for developing combined PTSD-MDD symptoms (OR = 2.881, P = 0.036). While in the high trauma exposure group, it was no longer a risk factor any more (P = 0.471).
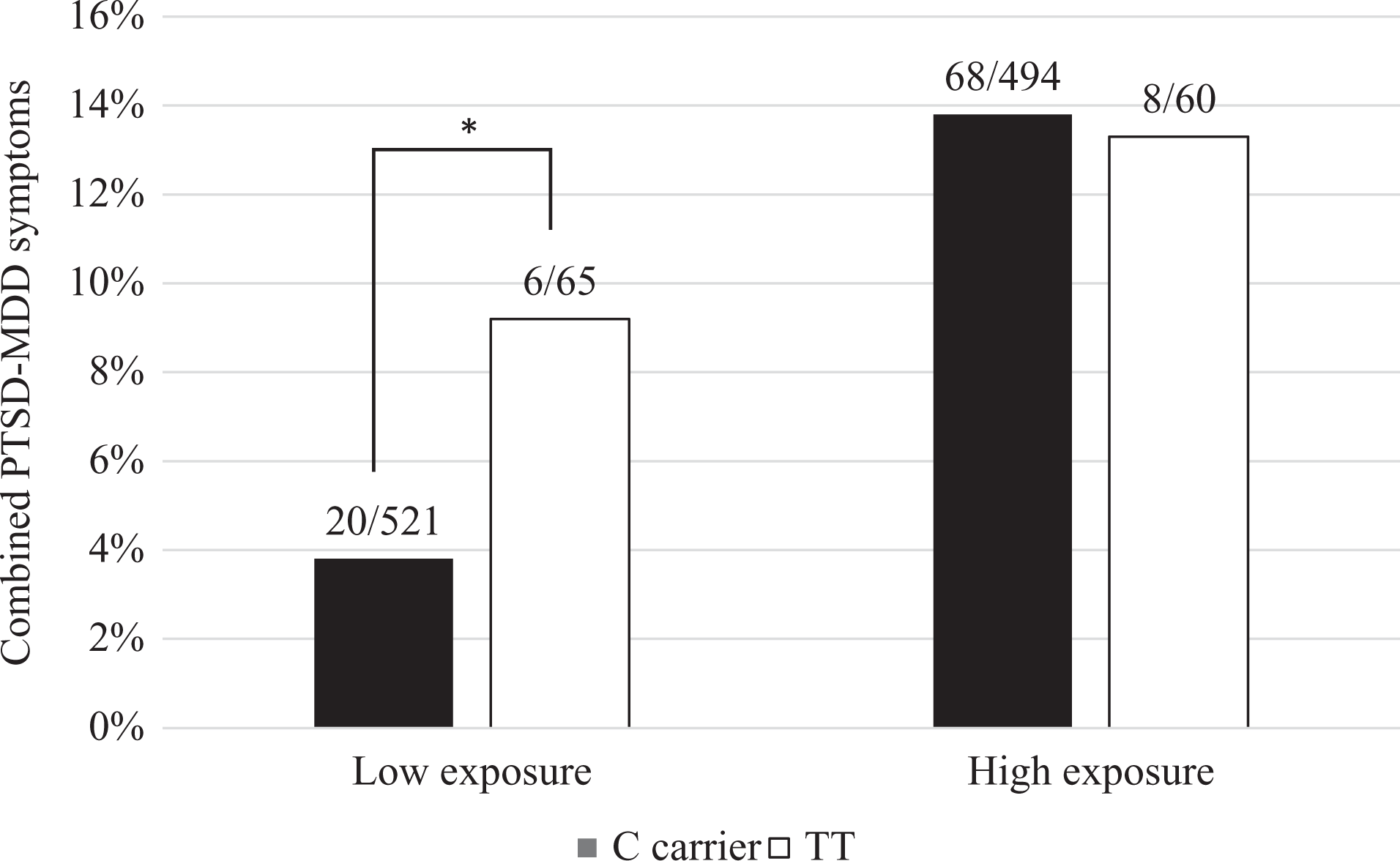
The genotype of rs9470080 interacted with trauma exposure to modify risk of developing combined post-traumatic stress disorder–major depressive disorder symptoms.
Simple Effect Analysis for Gene–Environment Interaction Effect on Combined Post-Traumatic Stress Disorder–Major Depressive Disorder Symptoms.
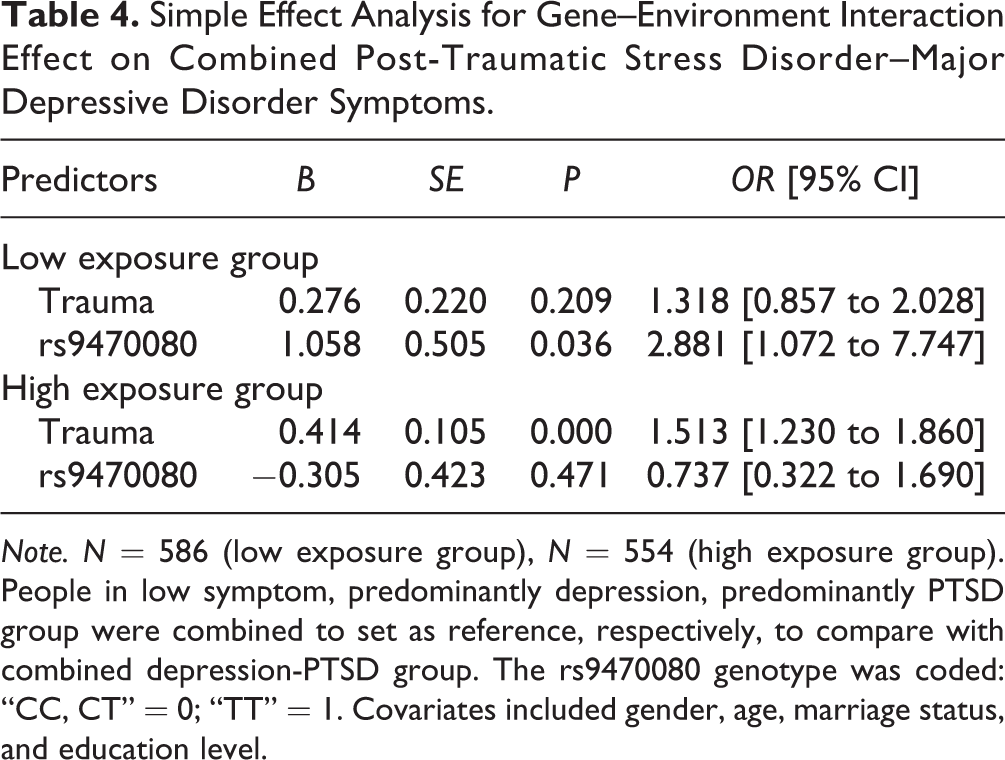
Note. N = 586 (low exposure group), N = 554 (high exposure group). People in low symptom, predominantly depression, predominantly PTSD group were combined to set as reference, respectively, to compare with combined depression-PTSD group. The rs9470080 genotype was coded: “CC, CT” = 0; “TT” = 1. Covariates included gender, age, marriage status, and education level.
Haplotype analysis identified significant main effect of rs3800373-rs9296158-rs1360780-rs9470080 haplotype A-G-C-T on different PTSD-MDD symptom patterns. Those with the A-G-C-T haplotype tended to enter the combined PTSD-MDD symptom group compared with the low symptoms group (OR = 0.338, P = 0.024, P permutation = 0.016), predominantly PTSD group (OR = 0.129, P = 0.006, P permutation = 0.001), and predominantly depression group (OR = 0.299, P = 0.052, P permutation = 0.032). See Supplemental Table 5 for details. The gene–environment interaction effect of the haplotype was not significant.
Discussion
In the current study, we tested whether the gene–environment interaction effects of FKBP5 polymorphisms can partially explain the phenotypic heterogeneity after disaster in an epidemiological earthquake-exposed sample in China. We found the G × E effect of rs9470080 of the FKBP5 gene in individuals who developed comorbid PTSD and depression symptoms after the disaster. Participants with the C allele at the rs9470080 loci were less likely to develop co-occurring PTSD and depressive symptoms when exposed to low levels of trauma exposure. However, the C alleles were no longer a protective factor when people experienced more severe trauma. We also found that the rs3800373-rs9296158-rs1360780-rs9470080 haplotype A-G-C-T was significantly related to co-occurring PTSD and depressive symptoms.
We identified that the interaction between FKBP5 rs9470080 polymorphism and trauma exposure distinguished the combined depression-PTSD group from the other three groups. Thus, our findings are consistent with studies supporting the genetic components of depression-PTSD comorbidity. 11,39 We found that rs9470080 TT homozygotes had a higher risking of developing both PTSD and depressive symptoms after low-level trauma exposure in our sample. As reported before, those with the rs9470080 TT genotype have lower FKBP5 mRNA expression, which is linked to lower plasma cortisol levels. 40 Therefore, our results suggest that low cortisol level may constitute a vulnerability factor that might partially explain the high comorbidity of PTSD and depression. Previous studies on FKBP5 18,38,41,42 found that the rs9470080 C allele can be a protective factor for developing psychopathologies such as PTSD when exposed to more severe trauma. However, this conclusion is restricted to low level of trauma exposure according to our results. We noticed that when the trauma exposure was severe, C allele of rs9470080 no longer had protective effects. We believe that the inconsistent results may result from different types of trauma in the studies. Previous findings were mainly based on childhood abuse. Nevertheless, in our current study, we investigated the interaction between rs9470080 and natural disaster. Abuse and natural disasters have different properties and therefore may interact with genetic backgrounds in different patterns. It has been pointed out that alleles that increase the risk of a certain disorder in one environment may confer protection to the same disorder in another environment. 43 For example, for a polymorphism in a gene that interacts with early life stress (such as rs9470080), one allele confers protection to future psychopathology while another allele confers risk; however, in the context of a less stressful life event (like natural disasters), those relationships are reversed, 9 just as observed in current study. Different gene–environment patterns for a same gene polymorphism could be an interesting topic that deserves future researches.
It is also noteworthy that our study has examined the effect of four possible functional SNPs of FKBP5 but only found one significant SNP, rs9470080. This result was consistent with another study investigating G × E effect of the same four SNPs on PTSD. 36 Of all the four FKBP5 SNPs (rs1360780, rs3800373, rs9296158, and rs9470080) tested, only the G × E effect of rs9470080 remained significant after correction in an African American sample but not in EA sample. Our study is the first one conducted in an Eastern Asian population and found a similar Gene × Environment interaction pattern of the SNPs. The results suggest that ethnicity might be an important factor to affect the functions of the FKBP5 SNPs. More studies using non-Caucasian samples are further needed to examine that.
Additionally, our current study identified a haplotype of FKBP5 conferring high risk of developing co-occurring PTSD and depression symptoms. It was found that the rs3800373-rs9296158-rs1360780-rs9470080 haplotype A-G-C-T could be a risk factor for developing combined PTSD-MDD symptoms. This result provides further support for our finding. Further research on the functional role of this risk haplotype would be helpful for understanding the biological underpinning of PTSD-MDD comorbidity.
The interaction of FKBP5 gene with environment determines the GR sensitivity and subsequent HPA axis function. 44 Therefore, our findings suggest that there is an abnormality in HPA axis activities in individuals with combined PTSD and depressive symptoms. However, it could be difficult to infer the direction of the change in HPA axis activity solely based on the results of this study. The opposite changes in the sensitivity and function of GR receptors have been reported in individuals with depression and PTSD, with depression being associated with hyposensitive GR receptors, while PTSD with GR receptors hypersensitivity. 13 The exact profile of GR receptor sensitivity in comorbid PTSD-depression is yet to be determined, and future studies investigating HPA axis activity in these individuals directly are clearly needed.
Several limitations of this study have to be considered. The main limitation of this study is the limited sample size. The sample size of our study was moderate to detect small effect size of SNPs, especially when we combined genetic studies with person-centered methods like LPA, resulting a small subsample of TT genotype carriers in combined PTSD-depression symptom group. Although we have performed permutation tests to minimize the effect of sample size on our results, the best approach is to replicate our result in a larger sample. Also, with a larger sample, it would be interesting to test our results in males and females independently. Second, PTSD and depressive symptoms were assessed by self-report instruments. Thus, these results need to be replicated by using clinician-administered instruments. Third, the sample we used was comprised of Chinese adults who had experienced a specific traumatic event. The potential influences of other lifetime trauma exposure and mental disorder diagnosis to the results were not evaluated in the current studies. Studies on populations from different cultures and exposed to various traumatic events, with more detailed information of lifetime trauma exposure and mental disorder diagnosis, are needed to understand the relationship between genes and heterogeneity in post-traumatic phenotype. Last but not least, only one specific gene has been studied as a candidate gene in this study without genome-wide significance tests. Therefore, in the absence of large replication cohort, the current results have to be considered as preliminary, and further replications are warranted.
Despite the aforementioned limitations, our work provides the first evidence of a genetic association with the combined PTSD and depression in individuals who experienced a deadly natural disaster. Importantly, this is a unique genetic risk study as it involves people who are not European and non-North American. The current findings yield new empirical evidence supporting the link between FKBP5 gene polymorphisms and combined depression-PTSD symptomatology and suggest that variants in FKBP5 gene could predict differential development of comorbid post-traumatic psychopathology. Finally, these findings may have some immediate practical implications. Given that individuals with specific genotypes are more susceptible to developing both PTSD and depression even after low levels of trauma exposure, they might benefit more from closer follow-up and early secondary prevention. But for those with higher trauma exposure, all of them should be taken good care of regardless of their genotypes because the protective genotype may no longer work in that situation.
Supplemental Material
Supplemental Material, 870505_Supplemental_materials - FKBP5 Genotype Linked to Combined PTSD-Depression Symptom in Chinese Earthquake Survivors
Supplemental Material, 870505_Supplemental_materials for FKBP5 Genotype Linked to Combined PTSD-Depression Symptom in Chinese Earthquake Survivors by Gen Li, Li Wang, Kunlin Zhang, Chengqi Cao, Xing Cao, Ruojiao Fang, Ping Liu, Shu Luo and Xiangyang Zhang in The Canadian Journal of Psychiatry
Footnotes
Data Access
We cannot make the survey data public because it is not covered by our ethics approval. Interested investigators could contact the corresponding author to get access to the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the External Cooperation Program of Chinese Academy of Sciences (No. 153111KYSB20160036), the National Natural Science Foundation of China (Nos. 31271099 and 31471004), the Key Project of Research Base of Humanities and Social Sciences of Ministry of Education (No. 16JJD190006), and the Beijing Municipal Science and Technology Commission (No. Z171100000117014).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.