
Abstract
South Africa hosts the highest number of African refugees, who are susceptible to mental health problems because of their trauma exposure and post-migration stressors. We assessed post-migration stressors, correlates, and predictors of post-traumatic stress disorder, depression and anxiety symptoms among refugees in Cape Town, South Africa. A cross-sectional survey of refugees from war and conflict-torn countries settled in Cape Town was conducted between February and May 2023. Participants (N = 147) were selected using a respondent-driven sampling technique. The survey instrument consisted of the Post-traumatic Stress Disorder Checklist, Patient Health Questionnaire, Generalised Anxiety Disorder–7, and the Post-Migration Living Difficulties checklist. We found that the prevalence of post-traumatic stress disorder, anxiety, and depression symptoms was 26.5% for post-traumatic stress disorder, 33.3% for anxiety and 33.3% for depression, respectively. Regression analyses identified discrimination, poor access to health services, and poor access to food as significant predictors of common mental disorders among refugees. The document-seeking process, unemployment stress, language difficulties, not getting help with welfare, fears of being sent to their home countries and isolation were also associated with symptoms of mental disorder. The results suggest that common mental health symptoms are highly elevated among refugees and are associated with post-migration stressors that are perpetuated by bureaucratic inefficiencies. Consequently, mental health interventions for refugees should not only address psychological difficulties but also consider the socio-economic and bureaucratic factors as a protective measure against mental health difficulties.
Post-migration stressors and the associated mental health difficulties, especially in the majority of the world, are burgeoning mental health and human rights concerns (James et al., 2022). The United Nations High Commissioner for Refugees (UNHCR, 2024) states that there are about 122.6 million internally displaced individuals globally, and over 70% of refugees are in low and middle-income countries (LMICs). A systematic review (n = 22 studies) on post-migration stressors and mental health difficulties among refugees and asylum-seekers in Europe found the length of stay in the host country, family difficulties (i.e., separation), and weak social support and integration, among others, as predictors of mental disorders (Gleeson et al., 2020). Considering the ongoing regional conflicts and the continued displacement of persons in Africa and other LMICs (UNHCR, 2024), we assessed post-migration stressors, correlates, and predictors of post-traumatic stress disorder (PTSD), depression and anxiety symptoms among refugees resettled in Cape Town, South Africa.
Refugees, post-migration stressors, and mental health
The 1951 Convention Relating to the Status of Refugees and its 1967 Protocol states that refugee status refers to a person that has a well-founded fear of persecution based on either demographics (i.e., race, religion) or social membership (i.e., political affiliation, or cultural/ethnic group) and is unable or unwilling to return to their country of nationality due to this fear (UNHCR, 2010). Yet the conception of a refugee remains complex and, at times, highly politicised, which perpetuates the adversity experienced by refugees (De Coninck, 2023; Turner, 2023).
Refugees encounter multiple adversities and traumatic experiences, usually termed post-migration stressors or post-migration living difficulties (PMLDs; Bogic et al., 2015; Tinghög et al., 2017). Frequently reported post-migration stressors include the refugee status-determination process, detention, discrimination, social isolation, acculturation, language difficulties, living conditions, and economic difficulties (Borho et al., 2020).
These post-migration stressors can impede recuperation and precipitate symptoms of mental disorders (Tinghög et al., 2017). Several studies report higher rates of mental disorder symptoms among refugees compared with the general population (Bogic et al., 2015; Henkelmann et al., 2020). A systematic review by Hajak et al. (2021) found a high prevalence of depression, anxiety, and PTSD symptoms in refugees, as well as predictors for mental health outcomes, including discrimination, uncertain asylum status, separation from family, unemployment, and language difficulties. Conceptualisations of PTSD, anxiety, and depression in the literature on refugee mental health are aligned with psychiatric nomenclature and taxonomy of mental disorders. Therefore, PTSD, depression, and anxiety are diagnostic constructs that result in distress or dysfunction in a person’s behaviour, cognition, and affect, which has a deleterious impact on one’s social, occupational, and interpersonal functioning (American Psychiatric Association [APA], 2022).
Similarly, a study conducted in Turkey reported on the prevalence of common mental disorders among Syrian refugees in Istanbul found higher rates of mental disorders among this population (Acarturk et al., 2021). Using the Post-traumatic Stress Disorder Checklist (PCL-5; Bovin et al., 2015) and the Hopkins Symptoms Checklist (HSCL-25; Derogatis et al., 1974) to assess PTSD, anxiety, and depression, the proportion who scored in the elevated range was 36.1%, 34.7%, and 19.6%, respectively. Being female, facing economic problems, trauma exposure, and a lack of safety, justice, and social support were found to be significant predictors of PTSD (Acarturk et al., 2021). Research suggests that host country contextual factors are risk factors associated with mental disorders among refugees.
A systematic review and meta-analysis (n = 28,367) by James et al. (2022) examined the literature on the association between post-migration stressors and common mental disorders among persons from various African countries. The study found a high pooled prevalence for anxiety (34.60%), depression (33.20%), and PTSD (37.9%). Importantly, the authors noted significant heterogeneity in the pooled prevalence of these disorders, which was higher among samples displaced within Africa than among participants living outside of Africa. The study highlighted the association between post-migration stressors and mental health difficulties and the need for host countries to develop culturally responsive programmes (James et al., 2022). The study by James et al. (2022) highlights the importance of how the broader sociocultural context is required to understand the full extent to which refugees’ lived experiences and associated mental distress are present across diverse settings.
Refugees in South Africa: post-migration stressors and mental health
South Africa is one of the most developed countries in Africa, with a relatively stable economy, and this has led to a heavy influx of refugees from the African continent (Vuningoma et al., 2021). Yet, unlike other refugee host nations, South Africa does not have refugee camps; therefore, refugees settled in South Africa mainly survive without state or humanitarian aid and have to navigate social adversities such as trauma exposure and social isolation (Idemudia et al., 2013; Schockaert et al., 2020).
Thela et al. (2017) examined the resettlement adaptation and mental health of refugees in Durban, South Africa. Using the 25-item Hopkins Symptom Checklist and the Harvard Trauma Questionnaire, they found 49.4% anxiety symptoms, 54.6% depression symptoms, and 24.9% post-traumatic stress symptoms. Symptoms of mental disorders were associated with discrimination, separation from family, low income, older age and being divorced or widowed. Furthermore, a qualitative study by Walker and Vearey (2023) found that refugees and asylum-seekers based in the Johannesburg area experienced post-migration stress, such as unemployment, food insecurity, and shelter, experiencing exacerbating mental disorders among the participants.
On a policy level, Manji et al. (2023) conducted a document analysis of 227 related policy documentation from 2002 to 2019, germane to migration and health care in South Africa. The study found a lack of progress and responsiveness from a policy regarding the association between migration/refugees and health, among other factors. Concerningly, the authors highlight the potential risks of insufficient policy guidance in that blame can be shifted onto refugees and migrant populations in the host country, which increases the adversity and post-migration stressors experienced by refugees.
The empirical literature on post-migration stressors and mental disorders among refugees in South Africa is dearth (Thela et al., 2017). Considering the growing concerns of crises of displacement due to regional conflicts in sub-Saharan Africa and elsewhere, we aimed to investigate (a) the prevalence of post-migration stressors, (b) the correlation between post-migration stressors and mental disorders, and (c) which post-migration stressors are predictors of elevated symptoms of mental disorders among refugees in Cape Town, South Africa. The study was guided by the following requestions:
What are the post-migration stressors among refugees resettled in the Cape Town area?
Are post-migration stressors correlated with elevated scores of PTSD, major depressive disorder, and generalised anxiety disorder among refugees resettled in the Cape Town area?
Which post-migration stressors predict elevated scores of PTSD, major depressive disorder and generalised anxiety among refugees resettled in the Cape Town area?
Methods
Participants and procedure
A cross-sectional research design with a respondent-driven sampling method was used due to the broader contextual challenges of working with a hard-to-find population, also known as a hidden population (Heckathorn, 2002; Taris et al., 2021). Therefore, respondent-driven sampling was a valuable and necessary sampling strategy for recruiting refugee participants, which also meant that refugees who participated also assisted in recruiting other refugees to participate (Lattof, 2018; Setia, 2016).
We recruited participants older than 18 years (n = 147) who consisted of refugees from conflict and war-torn countries, namely, Rwanda, Democratic Republic of Congo (DRC), Somalia, Cameroon, and Burundi, residing in the Cape Town area for over 12 months. Our study specifically focused on refugees resettled in the Cape Town area, not asylum-seekers and/or general migrants. Refugees settled in South Africa do not receive or participate in formal government or humanitarian programmes but depend on miscellaneous groups and organisations to provide support and shelter. Therefore, the recruited refugees resided in various areas and communities across Cape Town, usually clustered within groups of similar residential status to access support.
Data were collected from February to May 2023 using face-to-face completion of questionnaires at the Baptist Refugee Ministry in Woodstock, Bellevue Baptist Church, Elsies River Burundian Refugee Church, and Kensington refugee tent. The sample frame of the population under study was unknown as there is currently no exact number of refugees residing in South Africa. We followed Roscoe’s (1975) guidelines for determining sample size instead of formulas. Roscoe (1975) suggested that while sample sizes less than 500 and more significant than 30 are appropriate for quantitative research, where samples are to be divided into categories, each category must have a minimum of 30 respondents in studies with more than one dependent variable the sample size should be preferably ten times or more as large as the number of variables in the study. Thus, the sample size was 147 respondents, calculated based on the dependent variables of the study using G power software (Faul et al., 2007).
Instruments
Measurement theory and quantities focus on systematically applying discrete or continuous numerical values to psychological constructs such as sadness, worry, or fear (Michell, 2014). The assessment instruments are conceptually informed by the principles of measurement theory and were selected based on their psychometric properties, deeming them reliable and valid. Their use in previous studies across different settings makes our results comparable with the extant literature (Bastos et al., 2014). Participants completed a demographic survey, which consisted of items related to sex, marital status, nationality, reason for leaving their home country, mental health history, employment status, education, and age.
PTSD Checklist for DSM-5
The PTSD Checklist for DSM-5 (PCL-5) assessed post-traumatic stress outcomes (Bovin et al., 2015). The PCL-5 is a 20-item, self-report measure which assesses symptoms of PTSD based on the DSM-V diagnostic criteria and has been found to have good convergent and discriminant validity, test–retest reliability (r = .84), and high internal consistency (α = .96) (Bovin et al., 2015). The PCL-5 has also been found to be an effective measure in assessing PTSD symptoms in a South African setting (Kagee et al., 2022). All the endorsed items were summed up to yield a total score, and then a cut-off of 32 was applied to screen PTSD. A cut-off score of 31 to 33 is indicative of probable PTSD across studies (National Centre for PTSD, 2015).
Patient Health Questionnaire–9
The Patient Health Questionnaire–9 (PHQ-9) assessed major depressive disorder symptoms (Kroenke et al., 2001). The PHQ is a 9-item scale used to detect depression severity – total scores on the scale range from 0 to 27. The PHQ-9 has been found to have good psychometric properties, with internal reliability ranging from .86 to .89 and a test–retest reliability of r = .84 (Kroenke et al., 2010). In its first validation in Africa, the PHQ-9 showed reasonable accuracy in classifying cases of depression among HIV patients in South Africa (Cholera et al., 2014). To screen for major depressive disorder symptoms, research has suggested a cut-off between 8 and 11 for reasonable sensitivity and specificity (Manea et al., 2012). Thus, a cut-off of 9 was applied in this study.
Generalised Anxiety Disorder-7
Generalised anxiety disorder symptoms were measured by the Generalised Anxiety Disorder–7 (GAD-7). The GAD-7 is a seven-item measure designed to diagnose generalised anxiety disorder. The GAD-7 has good internal consistency (Cronbach’s α = .92, test–retest reliability of r = .83) and good convergent validity, as indicated by its correlations to the Beck Anxiety Inventory, r = .72 (Kroenke et al., 2010.) The measure has been validated for use in primary health care settings in Africa (Chibanda et al., 2016). Recent research suggests that if the GAD-7 is to be employed in assessing any anxiety disorder, a cut-off score of 8 provides more reasonable sensitivity and specificity than the cut-off of 10 recommended at its initial validation (Plummer et al., 2016). Hence, a cut-off of 8 was used to screen generalised anxiety disorder symptoms.
Post-Migration Living Difficulties
Post-migration stressors were assessed by the PMLD checklist (Silove et al., 1997). The PMLD is a 24-item scale which assesses resettlement stressors or difficulties experienced within the past 12 months. The PMLD has been found to have high validity and an internal consistency of .90. The Cronbach’s alpha for PMLD subscales are as follows: Health and Welfare Problems .84, Refugee Determination Process .76, General Adaptational Stressors .77, Family Concerns .79, and Social and Cultural Isolation .82 (Bentley et al., 2019).
Ethical considerations
Ethical approval was obtained from Rhodes University Human Research Ethics Committee (Reference: 2022-5863-7258). Gatekeeper permission was also obtained from a non-profit organisation (NPO) helping refugees living in South Africa. After receiving permission from the NPO, prospective participants were informed of the opportunity to participate in the study, and the second author (A.M.) connected with those interested. Once the participants were identified and consent forms were signed, the data collection process began, and the surveys were completed at various organisations where refugees were receiving assistance. Before consenting to participate, participants were given information sheets in every meeting to read and become familiar with the study’s aim, purpose, duration, and rights. They participated only after fully understanding the details of the research and had given both written and verbal consent.
Data analysis
Descriptive and inferential analyses were conducted by the Statistical Package for Social Sciences (SPSS) version 22 (2013). The proportion of the sample who scored within the elevated range of PTSD, major depressive disorder, and anxiety symptoms was calculated as frequencies and percentages. To compare the prevalence of PTSD, major depressive disorder and generalised anxiety disorder symptoms across demographics, the Chi-square test for independence was employed. The Chi test of independence determines whether there is a significant relationship between mental disorders and males and females. The Pearson correlation coefficient was also performed to test correlations between dependent and independent variables. The statistical procedures were chosen because they allowed us to account for all factors in one model, and this assisted in providing an accurate and precise understanding of the association between each post-migration stressor and mental disorder symptom. Multiple regression models were performed, with dependent variables being PTSD, depression, and anxiety symptoms and the independent variables being post-migration stressors.
Results
As seen in Table 1, 51.7% of the sample were males and 48.3% were females. Most respondents were between 30 and 44 (44.2%), while 28.6% were in the 18 to 29 age group, 25.2% were in the 45 to 59 age group, and 2.0% were 60 or above. Most participants who understood English were between 30 and 44 years old. Regarding marital status, 49% of the respondents were married, 32.7% were single, 5.4% divorced, and 12.9% were widowed. More than half of the participants were refugees from the Democratic Republic of the Congo (54.4%), whereas 15% came from Burundi, 10.2% from Somalia, 8.4% from Cameroon, 6.1% from South Sudan and 5.4% from Rwanda.
Characteristics of the sample (N = 147).
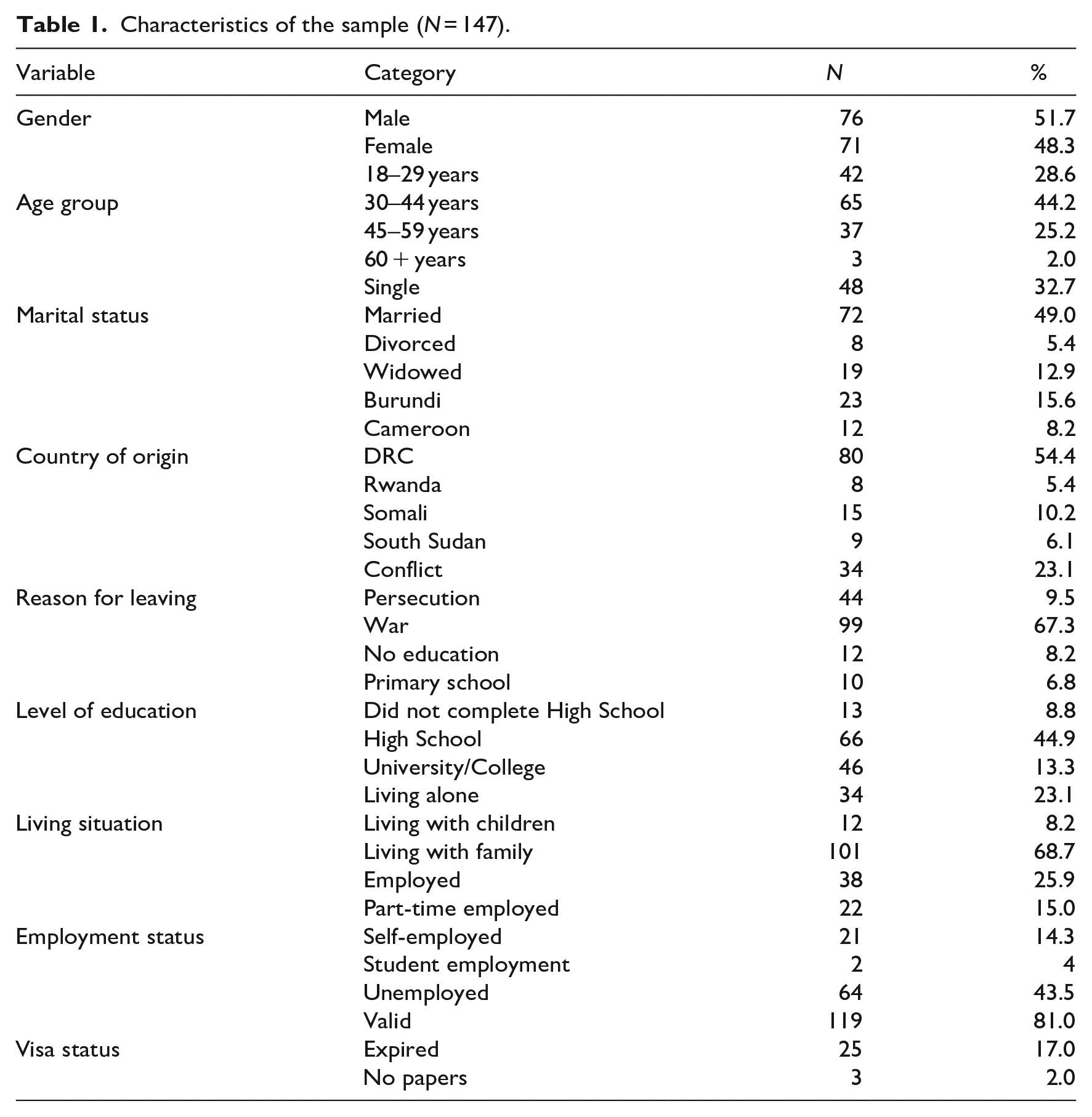
Refugees from the Democratic Republic of the Congo (DRC) participated in the study more than other nationalities because they are one of the largest refugee groups in South Africa; most war refugees come from the DRC. Most respondents had left their country of origin because of war (67.3%), whereas 23.1% fled from conflict and 9.5% from persecution. Another critical factor is that most refugees who participated in the survey had valid refugee status (81%), only 17% had expired refugee status, and 2% had no papers.
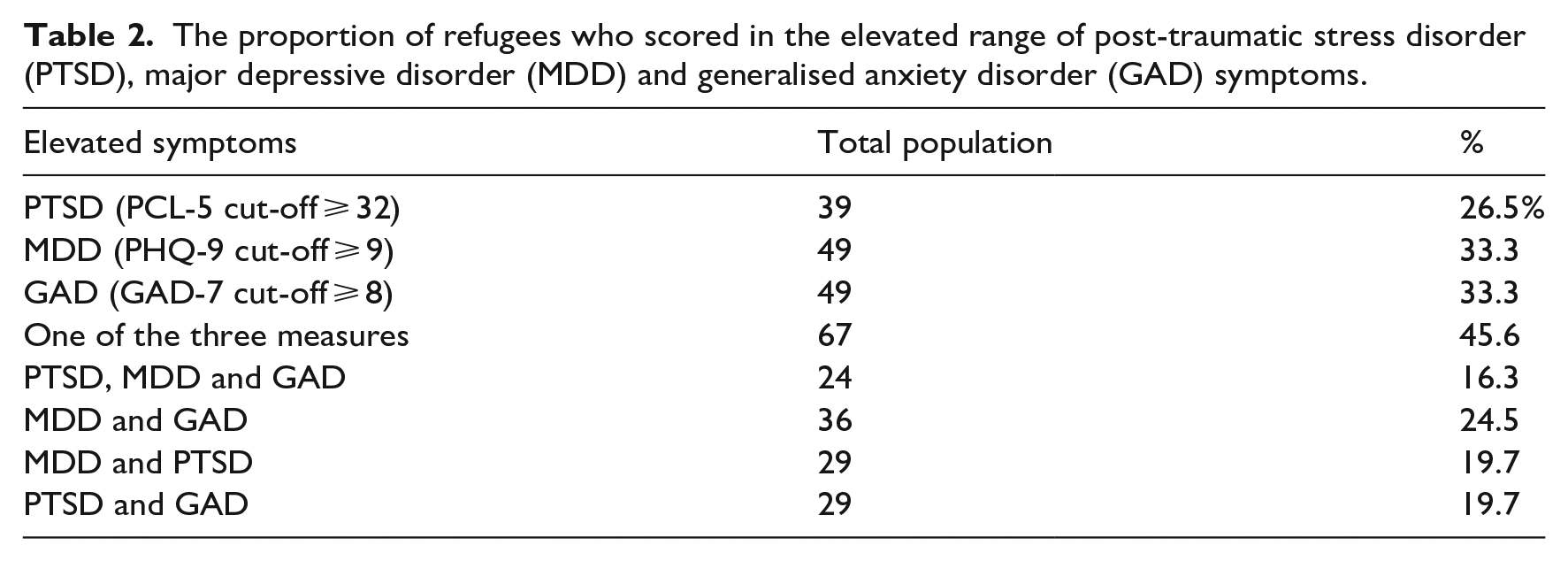
Table 2 presents refugee mental health outcomes based on the proportion of participants who scored above or equal to the cut-off values for each measure. The elevated range for each measure was scores above or equal to the commonly used cut-offs (PCL-5 cut-off ⩾ 32, PHQ-9 cut-off ⩾ 9, GAD-7 cut-off ⩾ 8). Refugees who scored in the elevated range on the PCL-5, GAD-7, and PHQ-9 were 26.5%, 33.3%, and 33.3%, respectively. Almost half of the study participants (45.6%) scored in the elevated range on at least one measure, and 16.3 % scored in the elevated range on all three measures. Nearly a quarter of the sample (24.5%) scored in the elevated range of both depression and anxiety symptoms, while 19. 7% scored in the elevated range of depression and PTSD symptoms. Notably, chi-square analysis found no significant association between gender and the occurrence of mental disorder symptoms.
The proportion of refugees who scored in the elevated range of post-traumatic stress disorder (PTSD), major depressive disorder (MDD) and generalised anxiety disorder (GAD) symptoms.
Post-migration stressors among refugees
In Figure 1, post-migration stressors were presented to participants, who were asked to indicate post-migration stressors that stressed them during their stay in South Africa. The sample endorsed several post-migration stressors. Namely, stress related to delays in refugee application status and the document-seeking process was endorsed as some of the most distressing. In addition, due to administrative delays and service delivery issues in South Africa, participants were also concerned about being unable to return home for emergencies.
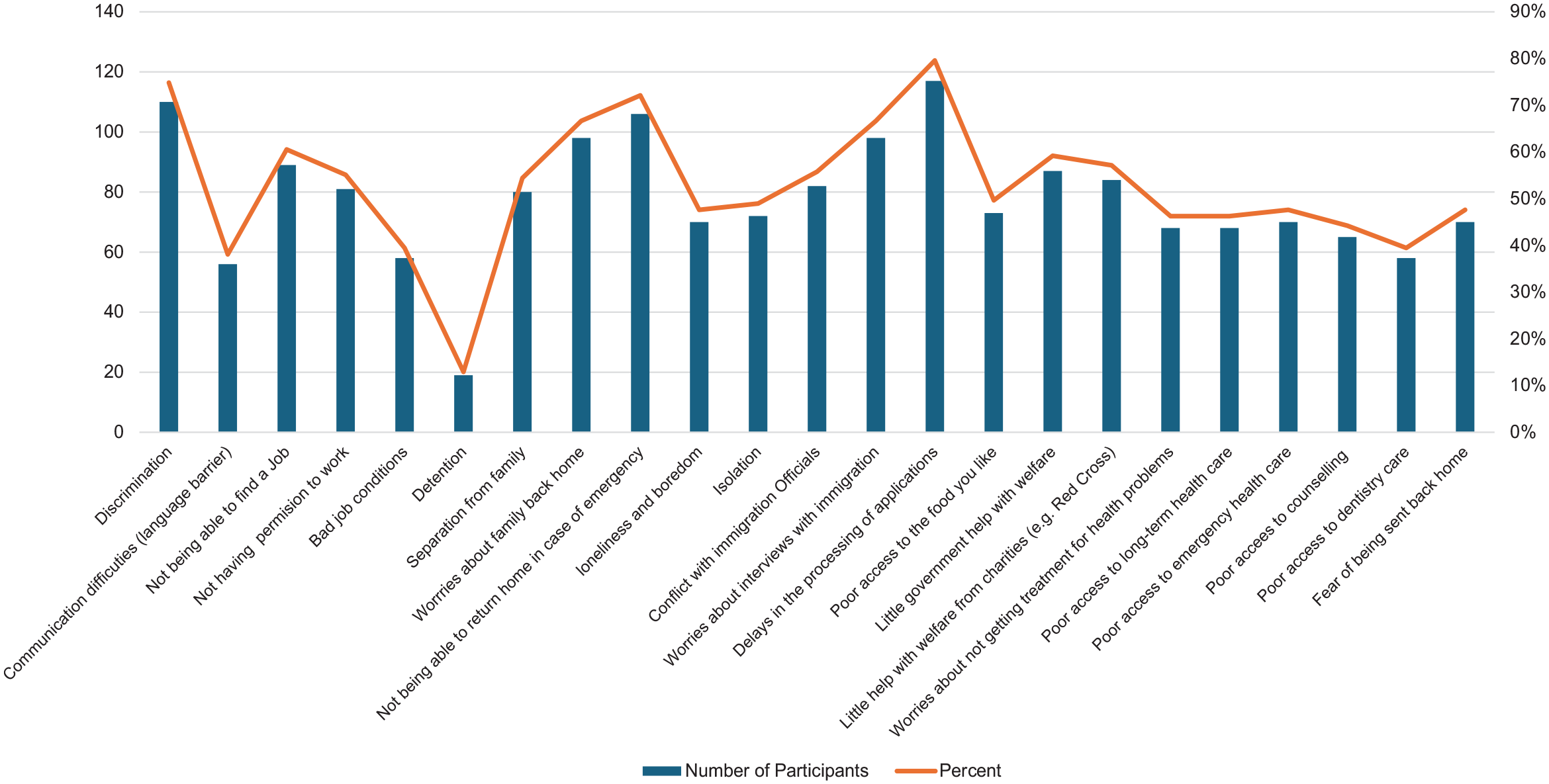
Prevalence of post-migration stressors among refugees in Cape Town.
Importantly, and considering the political climate of bouts of discrimination, three-quarters of the sample (75%) reported having experienced discrimination in the form of xenophobic violence, insults, and limited access to housing, employment, and education. The high number of refugees facing discrimination indicates elevated experiences of discrimination in Cape Town, with it being experienced in many spheres of their lives. Poor access to health services was also reported as a major source of stress among refugees. Nearly half of the participants (47%) expressed significant distress about not getting emergency health care, whereas 46% of refugees were stressed about poor access to long-term health care and not getting treatment for health problems. Participants also reported stress about not having access to counselling (44%) and poor access to dentistry care (39%). These results reflect the high magnitude of unmet important needs in a post-migration environment that are likely to have negative implications on the physical and psychological health of refugees.
As seen in Table 3, there was a positive association between the total score of the 23 post-migration stressors and mental disorder symptoms (PTSD, depression, and anxiety). Post-migration stressors were moderately correlated with depression symptoms (.47) and anxiety (.50) symptoms. This means that an increase in post-migration stressors coincides with increased depression and anxiety symptoms among refugees. Participants who had higher post-migration living difficulty scores had higher depression and anxiety symptoms. For PTSD, the association with post-migration stressors was weak (.38).
Post-migration stressors correlation with mental disorder symptoms.
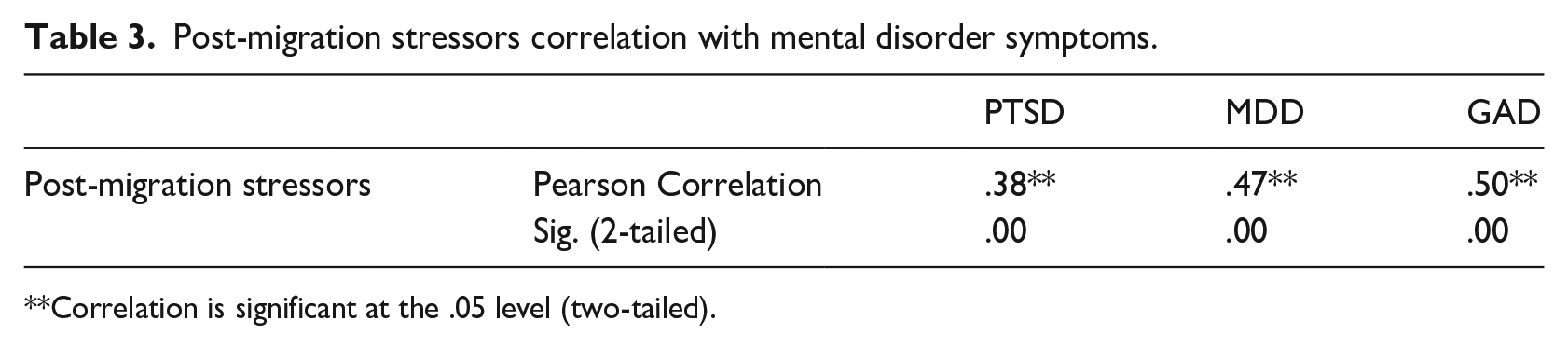
Correlation is significant at the .05 level (two-tailed).
The variable, PTSD, was regressed onto the predictor variables of post-migration stress. The linear combination of the independent variables explained 17% of the variance in PTSD symptoms, F(2,144) = 14.51, p < .001. Poor access to emergency health care (β1 = .28, p < .05) and discrimination (β2 = .21, p < .05) were the only variables that uniquely predicted PTSD symptoms. The other post-migration factors did not have a statistically significant impact on PTSD symptoms. Anxiety was regressed on the predictor variables of post-migration stress. The independent variables significantly predicted elevated symptoms of anxiety. Poor access to food one likes and poor access to counselling services were the only post-migration predictors that uniquely predicted elevated symptoms of anxiety symptoms. The two variables explained 33% of the variance in anxiety symptoms. Elevated symptoms of depression regressed onto the predictor variables of post-migration stress, and it was found that Discrimination and Poor access to food explained 21.8% of the variance. Discrimination significantly predicted elevated symptoms of PTSD (β1 = .30, p < .05), as did poor access to food (β2 = .26, p < .05).
Discussion
Human displacement due to regional and global conflicts, war, and now climate change is a burgeoning public health and human rights concern. To date, the empirical literature is limited on post-migration stressors and symptoms of mental disorders among refugees in LMICs such as South Africa. We found elevated levels of PTSD, depression, and anxiety symptoms among refugees settled in the Cape Town area of South Africa. The study found that more than one-quarter (26.5%) of the sample had elevated symptoms of PTSD, which, on average, indicates a clinically significant range. This finding is similar to Kazour et al. (2017), who reported 27.2% PTSD in a sample of Syrian refugees resettled in Lebanon. However, it is much lower than the prevalence rates reported in other refugee populations, which range between 60% and 80% (Bapolisi et al., 2020; Mahmood et al., 2019; Womersley & Kloetzer, 2018).
As PTSD develops because of exposure to traumatic events, variability in results can be attributed to the type and frequency of the traumatic event/s experienced in both the pre-and post-migration phases. The type and dose of trauma influence each outcome, with participants exposed to multiple life-threatening events or interpersonal trauma, such as rape and torture, being more likely to exhibit severe PTSD symptoms (Sengoelge et al., 2019).
We found elevated levels of depression and anxiety symptoms in the sample. One-third of the study participants scored in the elevated range on the GAD-7, which coincides with the 31.8% prevalence reported in Germany (Tinghög et al., 2017) and the 36.1% symptom prevalence reported in Turkey (Acarturk et al., 2021). We also found that one-third of the participants scored in the elevated range on the PHQ-9, similar to other studies conducted in refugee populations (Acarturk et al., 2021; Borho et al., 2020). These findings indicate the clinical significance of these symptoms and the likely need for interventions aimed at reducing the burden of mental disorders as anxiety and depression symptoms can interfere with the ability to function daily. Furthermore, a systematic review by James et al. (2022) found that refugees resettled in other African countries had higher levels of mental health distress compared with those outside of Africa. This finding may relate to the impact of migrating to similar or less resourced settings characterised by ailing bureaucratic systems and how such issues impact refugee mental health.
Post-migration stressors affecting refugees
The refugee status-determination process was reported as the major post-migration stressor, affecting more than 80% of the refugees reached. As described in previous studies (Freedman et al., 2020; Khan et al., 2021; Landau, 2006, Schockaert et al., 2020), refugees settling in South Africa are frustrated and stressed by the never-ending interviews with immigration officials, which often result in conflict with immigration officials, exposure to traumatic events, loss of finance and time, and employment opportunities. Reforms in the implementation of legislation and policies towards refugees are necessary for promoting the meaningful integration of refugees and mitigating mental disorders. Manji et al. (2023, p. 14) assert that there is an urgent need to address the ‘bureaucratic injustices’ experienced by migrants in South Africa and to acknowledge that such poor systems and procedures can perpetuate post-migration stressors among refugees.
We found that a high number of refugees (75%) faced systemic and community discrimination in the Cape Town area despite the open policy of integration. This form of discrimination in a population with a previous history of trauma could potentially threaten refugees’ safety, compound existing mental health difficulties, impair the quality of life, and erode successful integration. A similar study conducted in Durban found that almost half of the study participants experienced discrimination in South Africa, affecting their health (Thela et al., 2017). There is a need for systematic efforts to reduce discrimination in host countries to promote refugees’ quality of life, safety, and integration.
We also found that more than 50% of refugees were distressed by poor access to health care. Previous studies have shown that refugees have poor access to health services because of a lack of documentation, xenophobic attitudes of health care workers and language issues (Freedman et al., 2020; Khan et al., 2021; Zihindula et al., 2017). A document analysis by Manji et al. (2023) highlights the implications of inadequate policy regarding migration and health care in South Africa. Our findings support the need for socially inclusive policies that eliminate ‘bureaucratic injustice’ and educate health care workers about the rights and needs of refugees, which may improve refugees’ access to health services and consequently promote refugees’ physical and mental well-being.
Half of the sample (54%) was significantly distressed about separation from family and the safety of family members who were still back home, similar to a recent study conducted in Hong Kong (Ng et al., 2023). Separating from family during migration and consequently resettling in an alien land without familiar support systems can cause significant distress to many refugees. Refugees can worry excessively about the safety and financial needs of family members they have left behind and feel helpless while perambulating foreign lands without a familial support system (Ali-Naqvi et al., 2023).
Family absence and uncertainty about family reunification can precipitate emotional loneliness and isolation in host countries, which present elevated post-migration stressors. Unsurprisingly, almost 50% of the sample was stressed by isolation and loneliness in the post-migration environment. Moreover, more than half of the sample (56%) were stressed by communication difficulties, which can be seen as further experiences of isolation in a foreign country. Establishing structures that facilitate social inclusion, communication, and support of refugees in host countries may be useful in buffering social isolation and loneliness.
Post-migration stressors correlated with symptoms of mental disorders
South Africa is one of the most developed and economically stable countries in Africa, and the Cape Town area serves as a unique economic appeal for refugees to seek refuge and opportunities (Vuningoma et al., 2021). Yet, unlike other countries, South Africa does not provide state or humanitarian aid to refugees, which arguably may precipitate and or perpetuate post-migration stressors and mental disorders among persons settled in South Africa (Idemudia et al., 2013; Schockaert et al., 2020). To this end, South Africa is a unique context compared with the international context, which offers humanitarian support to refugees, in evaluating post-migration stressors, correlates, and common mental disorders among refugees.
The study found that discrimination in the host country predicted mental disorder symptoms among refugees. Consistent with Solberg et al. (2020) and Brooks et al. (2022), discrimination was significantly associated with PTSD, depression, and anxiety symptoms. Regression analysis also found discrimination as the major predictor for PTSD and depression. The constant fear of xenophobic attacks and exposure to xenophobic violence is undoubtedly the source of mental distress among refugees in South Africa. Studies conducted in Durban, South Africa, also indicate that discrimination is a risk factor for depression and post-traumatic stress symptoms (Thela et al., 2017; Womersley & Kloetzer, 2018). Taken together, all these findings indicate that discrimination is detrimental to the mental health of refugees. If the ongoing xenophobic attacks on refugees are not addressed, refugee mental health is at elevated risk and may continue to deteriorate.
The study also found that separation from family was associated with the three mental disorder symptoms. This finding affirms that family networks are protective factors for mental health (Ali-Naqvi et al., 2023). Being separated from family increases refugee vulnerability in the host country, and the stress of starting a new life without familiar support systems, coupled with increased worries about the whereabouts and safety of family members, can cause significant psychological distress. In line with this finding, Solberg et al. (2020) and Tinghög et al. (2017) found associations between sadness due to family absence and mental disorder symptoms (PTSD, anxiety, and depression). These findings indicate that family separation does not only break social ties and bonds but also causes emotional and psychological suffering, which heightens the risk of mental disorders. Interventions that facilitate family reunification, such as Khumbula Ekhaya (a programme that unifies South African separated families), can be useful in promoting refugees’ psychological well-being.
Sociocultural considerations are important in resettling refugees in host countries, which is essential to integration and the mitigation of post-migration mental health difficulties (McAllum, 2020). Our sample consisted of mostly men between the ages of 30 and 44 years from the DRC who left their home countries due to war. Thela et al. (2017) found that more refugees from other African countries had cultural adjustment challenges in South Africa. Negating such factors during resettlement increases the risk of post-migration stress experienced in a host country.
In this study, all the studied mental disorder symptoms were significantly associated with poor access to health services. Poor access to emergency health care was a major predictor of PTSD, while poor access to counselling services emerged as the main predictor for anxiety symptoms in the regression analysis. Considering the physical and psychological harm experienced by refugees in all the migration phases, poor access to medical and psychological services can compound existing difficulties or precipitate the onset of mental disorders. The lack of treatment, which is urgently needed for health problems in a population, can cause significant distress that may culminate in mental disorder symptoms. These results are similar to Brooks et al. (2022), who found that anxiety about not receiving medical treatment was associated with PTSD, while poor access to psychological services was associated with depression among Syrian refugee women in Jordan. If host countries are to be safe sanctuaries for refugees, health services should be accessible. Without adequate medical and psychological facilities, refugees’ physical and mental health is at risk. Promoting refugee access to health services is essential in improving refugees’ psychological functioning.
We also found that the prolonged refugee status-determination process was associated with PTSD, depression, and anxiety symptoms. Though this finding does not imply causality, Uncertainty about the legal process outcome and barriers encountered because of insecure residence status while waiting for permit renewal are undoubtedly the source of psychological distress and explain the link between the refugee status-determination process and mental disorder symptoms. In line with our findings, Hvidtfeldt et al. (2020) observed that the increased risk of psychotic, affective and nervous disorders was 59% higher for refugees who have been waiting for 24 months compared with refugees who have been waiting for 6 months. Considering that South Africa’s Department of Home Affairs has the highest number of pending asylum cases and the longest asylum adjudication period in the world (Crush et al., 2017), refugees in South Africa are at high risk of mental disorders. Reforms in the implementation of policies and the utilisation of psychological services among refugees with insecure residence status are also essential in reducing psychological distress.
Post-migration stressor predictors of mental disorders
Poor access to food is a major predictor of depression and anxiety symptoms. Although these findings cannot imply causality, several studies have found that food insecurity is associated with mental disorder symptoms, mainly because of the constant worry about the source of one’s next meal (Dlamini et al., 2023; Trudell et al., 2021). Considering that refugees resettled in South Africa are self-reliant, refugees without a source of income can struggle to access food daily. Refugees may constantly worry about accessing food, which heightens the development of anxiety and depression symptoms. Thus, promoting food security should be part of the intervention strategy if mental health is to be effectively addressed. Arguably, until daily stressors are addressed, refugees cannot focus on psychotherapy and recover from war-related trauma. To reduce psychological distress and foster recovery, current stressors should be eliminated, and basic needs should be met.
Limitations
The study employed self-reporting measures instead of clinician-administered diagnostic interviews. Self-reporting instruments are more prevalent than diagnostic interviews (Patanè et al., 2022). The sample included refugees who could read and understand English; it is possible that refugees who cannot read and understand English may experience more post-migration stressors and severe mental health problems. Finally, the study was cross-sectional, and due to its nature, it was impossible to examine causality between post-migration predictors and mental health symptoms. Our study only focused on the pre- and during-migration stressors, which limits our understanding of the complexity of migration stressors and mental health distress. Finally, we know that selection and information bias can impact our results (Maier et al., 2023).
Recommendations
Several recommendations flow from the findings of this study. It is apparent, given the high proportion of participants who scored in the elevated range on the PCL-5, GAD-7, and PHQ-9, that there is considerable psychological distress in this population. For this reason, psychological support, including counselling and psychotherapeutic services, should be available to this population. The Trauma Centre for Survivors of Violence and Torture and the Scalabrini Centre of Cape Town are examples of such organisations that are available to assist in this regard. Despite the work of such organisations, a considerable mental health gap persists. Where appropriate, task sharing of psychological support to lay and peer counsellors should be considered.
Food security is another matter that is closely associated with mental distress. For this reason, relief organisations such as Gift of the Givers and other charities play an important role in providing sustenance for persons who experience food insecurity. Yet, as short-term interventions are necessary, there is also a medium and long-term need to ensure longer-term financial and food security for the refugee community. The ability to work legally in South Africa is a matter for the Department of Home Affairs to consider, although this is usually done on a case-by-case basis.
The streamlining of the documentation process appears to be about to improve following the election of the Government of National Unity and the appointment of a new minister in the Home Affairs portfolio. In the context of scarce public resources for social services, such as assistance with documentation, employment, and translation services may not be easily available from the state. To this extent, refugee communities themselves may engage in self-help and social support, especially to newcomers. This is likely already occurring, and the refugee community may benefit from greater publicising such community support structures.
Xenophobia and anti-immigrant sentiments are global concerns and are a much harder problem to solve, especially in the context of populist politics and scarce resources, even for South Africans. The xenophobic attacks on foreign nationals in 2008 were especially severe and have occurred episodically since then. While solutions to this problem lie outside of the scope of this study, it should be stated that, as with any host country that accepts those fleeing war and political turbulence, South African communities have a responsibility to provide places of safety for persons with a refugee background.
Conclusion
Refugees settled in Cape Town, South Africa, present with elevated symptoms of common mental disorders that are associated with several post-migration stressors in the context of resettlement. Significantly, refugees experience a double burden of adversity, which is to become a refugee and then the ongoing adversities of discrimination, food insecurity, and bureaucratic injustices in host countries, which perpetuate symptoms of mental health distress. The presence of elevated symptoms of mental health distress among refugees requires not only psychological intervention but also a systemic and multi-stakeholder approach to ameliorate post-migration stressors and the associated mental health distress.
Footnotes
Acknowledgements
We want to thank all of our participants for completing this survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D.D.B. acknowledges support from the University Capacity Development Grant and the National Research Foundation.