
Abstract
Background:
Cost-efficient and non-invasive predictors of antidepressant response to repetitive transcranial magnetic stimulation (rTMS) are required. The personality vulnerabilities—neuroticism and self-criticism—are associated with antidepressant outcomes in other modalities; however, self-criticism has not been examined in response to rTMS, and the literature on neuroticism and rTMS is inconsistent.
Methods:
This naturalistic, 4-week study involved daily dorsolateral prefrontal cortex (DLFPC) rTMS for major depression (15 unipolar, 2 bipolar). Participants completed the Big Five Inventory (neuroticism) and the Depressive Experiences Questionnaire (self-criticism) at baseline and at the end of treatment. Changes in depressive symptoms, as rated by the clinician, were quantified using the 21-item Hamilton Depression Rating Scale. Given the inconsistencies in data regarding the stability of neuroticism in patients receiving rTMS, we performed a systematic review and quantitative meta-analysis of trials examining rTMS and neuroticism.
Results:
rTMS significantly improved depressive symptoms, and this was predicted by higher levels of self-criticism but not neuroticism. Self-criticism was stable over the 4 weeks of rTMS; however, neuroticism decreased, and this was not related to decreases in depressive symptoms. Our quantitative meta-analysis of 4 rTMS trials in major depression (n = 52 patients) revealed decreases in neuroticism, with a moderate effect size.
Limitations:
Our results are limited by a small sample size, and the absence of a sham-rTMS group. Our meta-analysis included only 4 trials.
Conclusion:
Highly self-critical patients appear to benefit more from rTMS than less self-critical patients. Neuroticism, a conceptually similar but distinct personality domain, does not appear to predict antidepressant response, yet this vulnerability factor for depression decreases after rTMS.
Major depression is common and debilitating. Unfortunately, a large proportion of patients do not benefit from existing psychotherapeutic and/or pharmacological interventions, or find available treatments intolerable. 1 For treatment-resistant depression (TRD), 2 non-invasive brain stimulation techniques have emerged as therapeutic alternatives. Among them, repetitive transcranial magnetic stimulation (rTMS) has the largest evidence base to date for TRD, 3 with moderate-to-large antidepressant treatment effects, as compared with sham interventions, and relatively high levels of acceptability to patients. 4 –10
Although this efficacious treatment is approved in many jurisdictions, delivery remains capital intensive, and the time investiture for the patient and the provider are considerable. Although novel stimulation protocols, such as theta-burst stimulation 4 and accelerated delivery, 11,12 aim to minimise the overall costs and disruption to patients’ lives, these factors still remain significant. Moreover, not all patients experience clinically meaningful improvements (clinical response and clinical remission) in their depressive symptoms following rTMS treatment. 4 –10 Accordingly, the identification of readily implementable, low-cost predictors that can guide resource allocation is important. Personality and temperament are attractive in this regard, for they are well-studied in terms of their relation to depression and are relatively stable attributes that can be measured efficiently, economically, and non-invasively. 13
Two of the most widely studied personality vulnerability factors for depression are neuroticism, stemming from the 5-factor model of personality 14 , and self-criticism, stemming from Blatt’s 15 –17 two-polarities model of personality and psychopathology. Individuals with elevated levels of neuroticism are characterised by being prone to anger, sadness, fearfulness, and negative emotions in general, and tend to be highly emotionally reactive to stress. 14 Highly self-critical individuals are permeated with feelings of low self-worth and guilt, and are excessively concerned with maintaining social status and value in the eyes of important others. 16,18,19 Both neuroticism and self-criticism have been cross-sectionally and longitudinally associated with subthreshold and pathological depressive symptoms 13 and they predict the onset of depressive disorders. 20 Accumulating evidence suggests that these factors may serve as clinically useful predictors of antidepressant response to psychotherapeutic and psychopharmacological interventions; 21 –23 albeit, with divergence in findings. 23 Moreover, evidence has linked these traits to activity in the neural circuitry involved in depressive disorders, 23,24 suggesting they may have utility as proxy biomarkers for treatment response.
To our knowledge, no research to date has examined the trait of self-criticism in relation to antidepressant treatment response to rTMS. However, both depression and self-criticism are associated with activation in the dorsolateral prefrontal cortex (DLPFC) during error processing 25 and when monitoring internal emotional states 24,26,27 (for a review, see Kopala-Sibley and Zuroff, 2019 27 ). Doerig et al. (2013) 26 suggest that self-criticism, or perhaps coping with criticism, involves a top-down pathway between prefrontal regions and the limbic system, representing cognitive reappraisal strategies for dealing with evoked negative affect. As such, individuals high in self-criticism may particularly benefit from rTMS targeting the DLPFC as this may upregulate their emotional regulation and cognitive abilities. Alternatively, altering DLPFC connectivity may directly impact self-criticism; however, this has not been tested.
Similar to self-criticism, elevated neuroticism is associated with alterations in both DLPFC structure, 28 –30 resting state function, 31,32 and activation during a working memory task. 33 With data linking neuroticism to depression and to the DLPFC, neuroticism is a putative predictor of rTMS antidepressant response. Yet, we and others have failed to find support for its predictive utility in rTMS for depression. 34,35,36 Instead, neuroticism appears to change as a result of rTMS, and in one sample this was proportional to the improvement in depressive symptoms. 34 Though the utility of neuroticism in predicting clinical response to rTMS is questionable, the literature to date has predominantly underpowered samples. We therefore sought to synthesize the literature through a meta-analysis.
Here, we examine the predictive utility and stability of neuroticism and self-criticism in rTMS for TRD.
Methods
In this 4-week naturalistic study, we prospectively recruited 17 adults with TRD who were referred to the Vancouver General Hospital Neurostimulation Service for consideration for rTMS. All participants had a diagnosis of a major depressive episode, as confirmed by clinical interview and then by a score of ≥9 on the 21-item Hamilton Depression Rating Scale (HDRS-21 37 ). The primary diagnosis was major depressive disorder (MDD) for 15 patients and bipolar disorder type II for 2 patients. Treatment resistance was determined as having failed at least 2 adequate courses of antidepressants, 2 mood stabilizers or antipsychotics, or having failed to tolerate pharmacological trials. All patients consented and completed the initial study package; however, 2 participants did not return the post-treatment study package.
This study was reviewed and approved by the University of British Columbia Clinical Research Ethics Board.
rTMS Treatment
rTMS treatment was delivered using a Magstim Rapid2 magnetic stimulator (Magstim Company Ltd, UK) connected to a figure-of-eight–shaped coil. Over 4 weeks, patients received 20 treatment sessions, composed of 3,000 pulses delivered at 120% of the resting motor threshold (10 Hz, trains of magnetic pulses for 4 sec, followed by 26-sec inter-train intervals) over the left DLPFC. 9 The DLPFC was localised using the 6-cm “rule”. The resting motor threshold was determined weekly.
For 3 patients, high-frequency rTMS (HF-rTMS) of the left DLPFC was discontinued in favour of low-frequency rTMS (LF-rTMS) of the right DLPFC 8 (1,800 pulses at 1 Hz) due to a lack of improvement. Sensitivity analyses were performed without these participants, which did not impact our findings.
Clinical Instruments
A psychiatrist completed medical and psychiatric history and safety screenings. The HDRS-21 was used as a clinician-rated measure of depressive symptoms. Participants also completed the self-report Sheehan Disability Scale, where 3 domains of function (work/school, social life, and family life/home responsibilities) were assessed. Scores of ≥5 on any of these domains reflect impaired function.
Personality Predictors
We used the Big Five Inventory to quantify 5-factor constructs of personality. 38 This is one of the most widely used, well-validated measures of the Big Five Personality traits. This 44-item self-report questionnaire was completed at baseline and then again at the conclusion of 4 weeks of rTMS treatment. Internal consistency for neuroticism was α = 0.86 at baseline and 0.80 at follow-up.
We used the 66-item self-report Depressive Experiences Questionnaire (DEQ 18 ) to quantify self-criticism. Patients completed this instrument at baseline and at the conclusion of 4 weeks of rTMS treatment. Self-criticism is conceptualised as a continuous—not categorical—dimension of individual difference. 39 This scale has shown excellent test-retest reliability and displays high retest stability even following stressful life events. 39 In this sample, internal consistency for self-criticism was 0.87 at baseline and 0.89 at follow-up.
Statistical Analyses
We performed statistical analyses using SPSS Statistics version 24 (IBM, Armonk, NY, USA), and factor weighting of the DEQ was completed using R (R Foundation for Statistical Computing). Internal consistency was measured with Cronbach’s alpha. We performed paired t-tests to examine changes in clinical variables pre- and post-rTMS treatment. We then computed multiple regression models testing the ability of prospectively assessed personality traits to predict antidepressant response, defined as the percentage change in HDRS-21 scores from baseline to the end of treatment. Models controlled for baseline depressive symptom severity, as assessed by the HDRS-21. Given the conceptual and empirical overlap between self-criticism and neuroticism, 40 we performed separate regression analyses for each. For all results, we present both unstandardised (b) and standardised (β) betas. We also report R2 for the full model. Statistical significance was set at α < 0.05.
Meta-Analytic Procedure
This systematic review was registered with PROSPERO. We searched MEDLINE, EMBASE and PsycINFO from database inception to September 10, 2018. Our search of MEDLINE utilised the following search terms: ((neuroticism) AND ((depression) OR Major Depressive Disorder)) AND ((rTMS) OR Repetitive transcranial magnetic stimulation). Our search of EMBASE utilised the following search terms: (((neuroticism) OR neurosis) AND ((repetitive transcranial magnetic stimulation) OR transcranial magnetic stimulation) AND ((major depression) OR depression))). Our search of PsycINFO used the following search terms: ((depression) AND ((rTMS) OR repetitive transcranial magnetic stimulation) AND (neuroticism)).
Studies were included if they 1) included prospective assessment of neuroticism, 2) assessed neuroticism at the conclusion of treatment, and 3) included participants aged 18-75 years, with a major depressive episode treated with rTMS. Open-label and randomised sham-controlled trials were eligible for inclusion.
The primary outcome was a change in neuroticism from pre- to post-rTMS. Mean scores and standard deviations were extracted in duplicate (AM, SB) and any discrepancies were resolved by consensus together with MTB. To extract graphically depicted data, we utilised freely available digital extraction software (WebPlotDigitizer). As we principally identified non-randomised studies of interventions, we employed the Risk of Bias in Non-randomised Studies – of Interventions (ROBINS-I).
Analyses were performed using Comprehensive Meta-Analyses Version 2.0 (Biostat, Englewood, NJ, USA). Because true treatment effects are likely to vary between studies given different methodological characteristics, such as patient selection, degree of treatment resistance, or concomitant medications, we employed a random effects model. 41 Standardised mean differences (SMD) were utilised for changes in neuroticism pre- and post-treatment. 42 With respect to SMDs, we conservatively assumed a correlation coefficient of 0.7 if we were unable to obtain the correlation between pre- and post-treatment scores. 43 To quantify statistical heterogeneity, we employed Q-statistics, I2 and τ2. Threshold statistical heterogeneity was deemed present if the P value for the Q-statistic was <0.1 or the I2 > 35%. 44 Finally, we used Funnel Plots, Rosenthal’s Fail-Safe N, 45 and Egger’s Regression Intercept 46 to test for the presence of publication bias. 44,47
Results
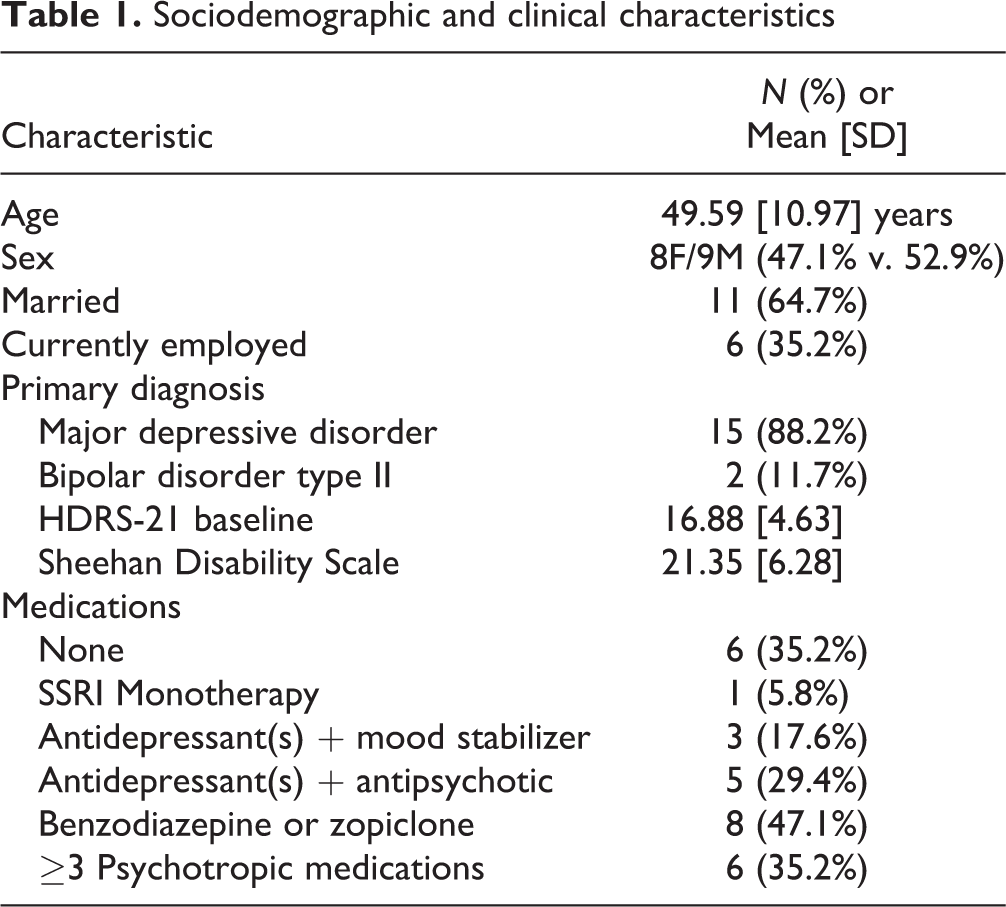
The sociodemographic and clinical characteristics of this sample at baseline are presented in Table 1. This was a moderately depressed sample with a high degree of anxiety and disability. Several patients (n = 6) refused ongoing pharmacological intervention, while polypharmacy was evident in the remainder (n = 6 had 3 or more psychotropics).
Sociodemographic and clinical characteristics
rTMS significantly improved clinician-rated depressive symptoms (Figure 1A) and self-reported disability (Figure 1B). rTMS was associated with a decrease in neuroticism over the treatment period (Figure 1C) but did not change self-criticism (Figure 1D). Contrary to previous findings, 34 the decrease in neuroticism in this sample was not in proportion to the decrease in depressive symptoms (b = −0.01, β(standardised) = −0.21, t = 1.15; not significant).
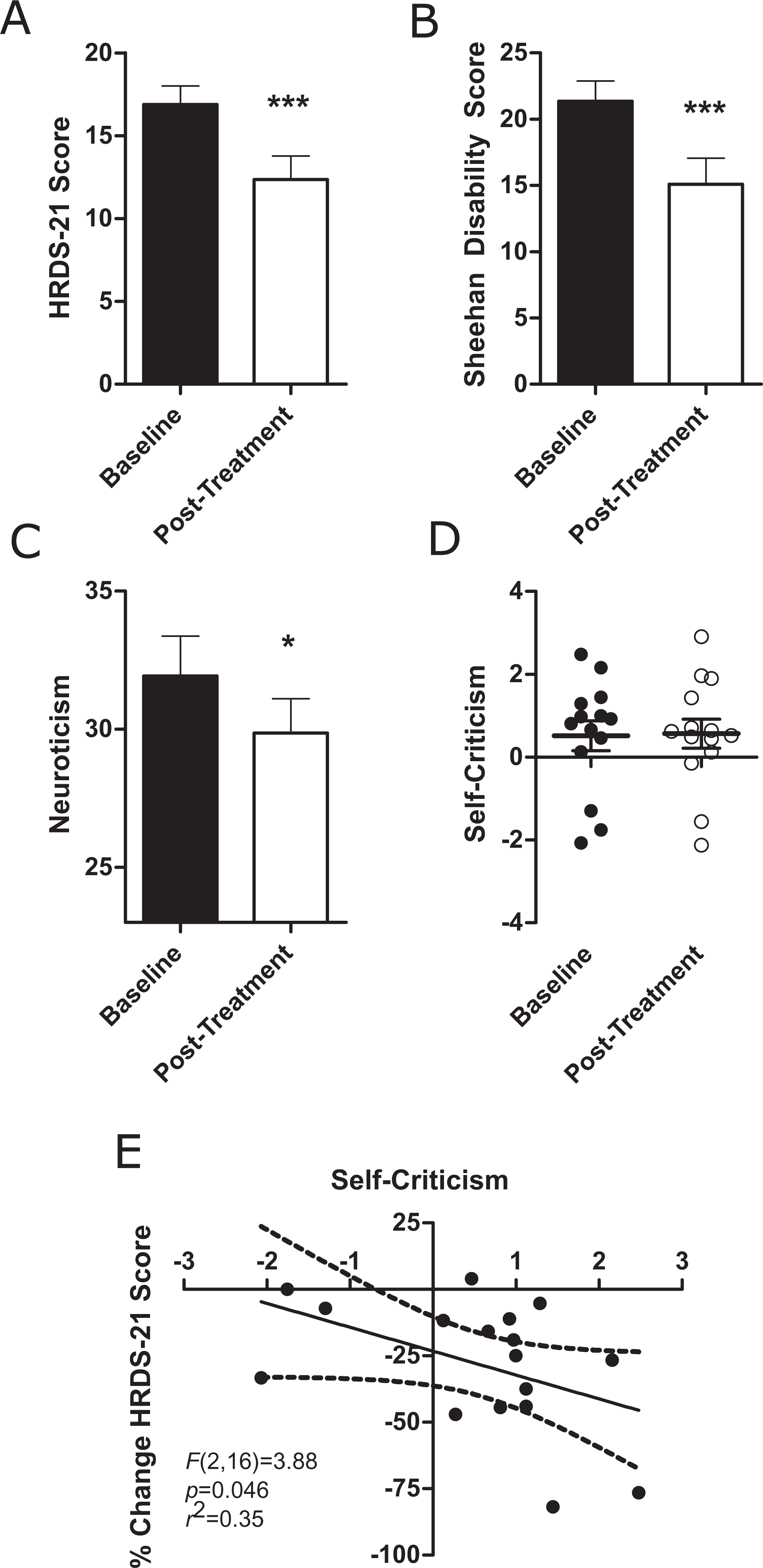
Change in clinical and personality factors after 4 weeks of DLPFC rTMS treatment. (A) Change in depressive symptoms as measured by the 21-item Hamilton Depression Rating Scale (HDRS-21) (16.88 [4.63] v. 12.35 [5.86], t(16) = 4.82, P < 0.001). (B) Change in function as measured by the Sheehan Disability Scale (21.35 [6.28] v. 15.08 [8.07], t(16) = 3.91, P = 0.001). (C) Change in the personality domain Neuroticism (31.92 [5.39] v. 29.85 [4.68], t(13) = 2.32, P = 0.037). (D) Self-Criticism remained stable after 4 weeks of rTMS (0.51 [1.35] v. 0.56 [1.31], t(13) = −0.19, P = 0.85). (E) Change in depressive symptoms as a percentage of baseline was predicted by baseline self-criticism (F(2,16) = 3.88, P = 0.046).
We next examined baseline neuroticism and self-criticism as predictors of antidepressant response. In these analyses, we controlled for baseline HDRS-21 scores. High levels of self-criticism strongly predicted percent improvement in depressive symptoms in this sample (b = −0.11, β(standardised) = −0.57, t = −2.54, P = 0.023; Figure 1E). Self-criticism and baseline HDRS-21 scores explained 43.7% of the variance in percentage change in HDRS-21 scores. Neuroticism did not predict antidepressant response in this sample (b = 0.01, β(standardised) = 0.23, t = 0.81; not significant).
Meta-Analysis
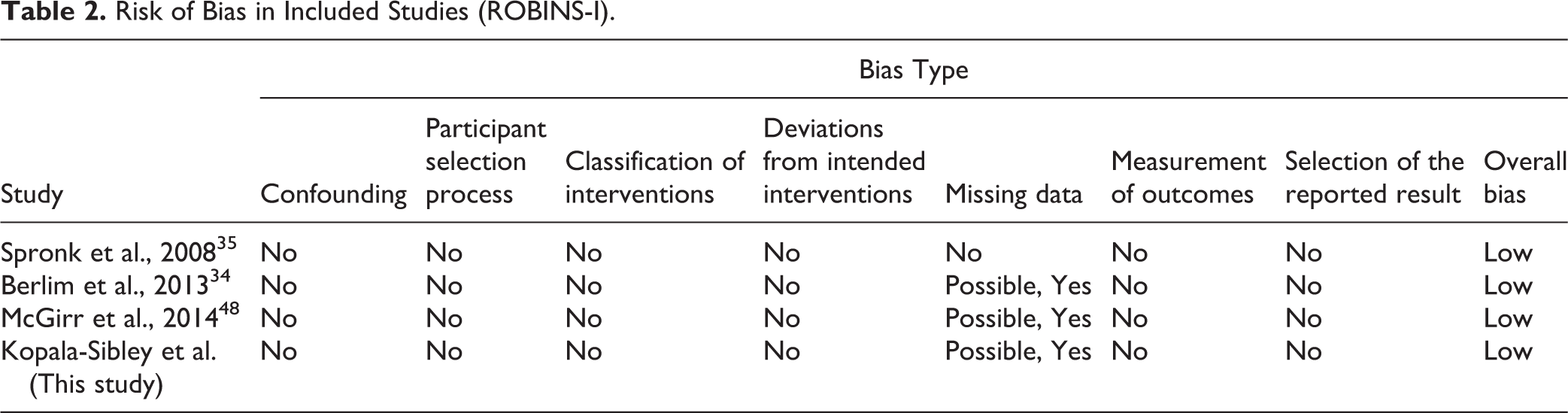
Our literature search is detailed in Figure 2. Our systematic literature review identified 3 eligible studies, 34,35,36 all of which were open-label, to which we added the data from the current study. The first study involved 8 patients (3F/5M) with MDD who received 15 to 25 daily treatments of 10 Hz stimulation of the left DLPFC at 100% RMT until they achieved clinical response. 35 The second involved 14 patients (8F/6M) with MDD who received 20 daily treatments of 10 Hz stimulation of the left DLPFC at 120% RMT. 34 The third involved 15 patients (12F/3M) who received 20 daily treatments of deep rTMS of the left DLPFC at 120% RMT. 36 The second risk of bias according to ROBINS-I overall was low (Table 2). Thus, we included a total of 4 studies and 52 depressed participants who completed prospective characterisation of neuroticism before receiving DLPFC rTMS and then again at the conclusion of treatment.
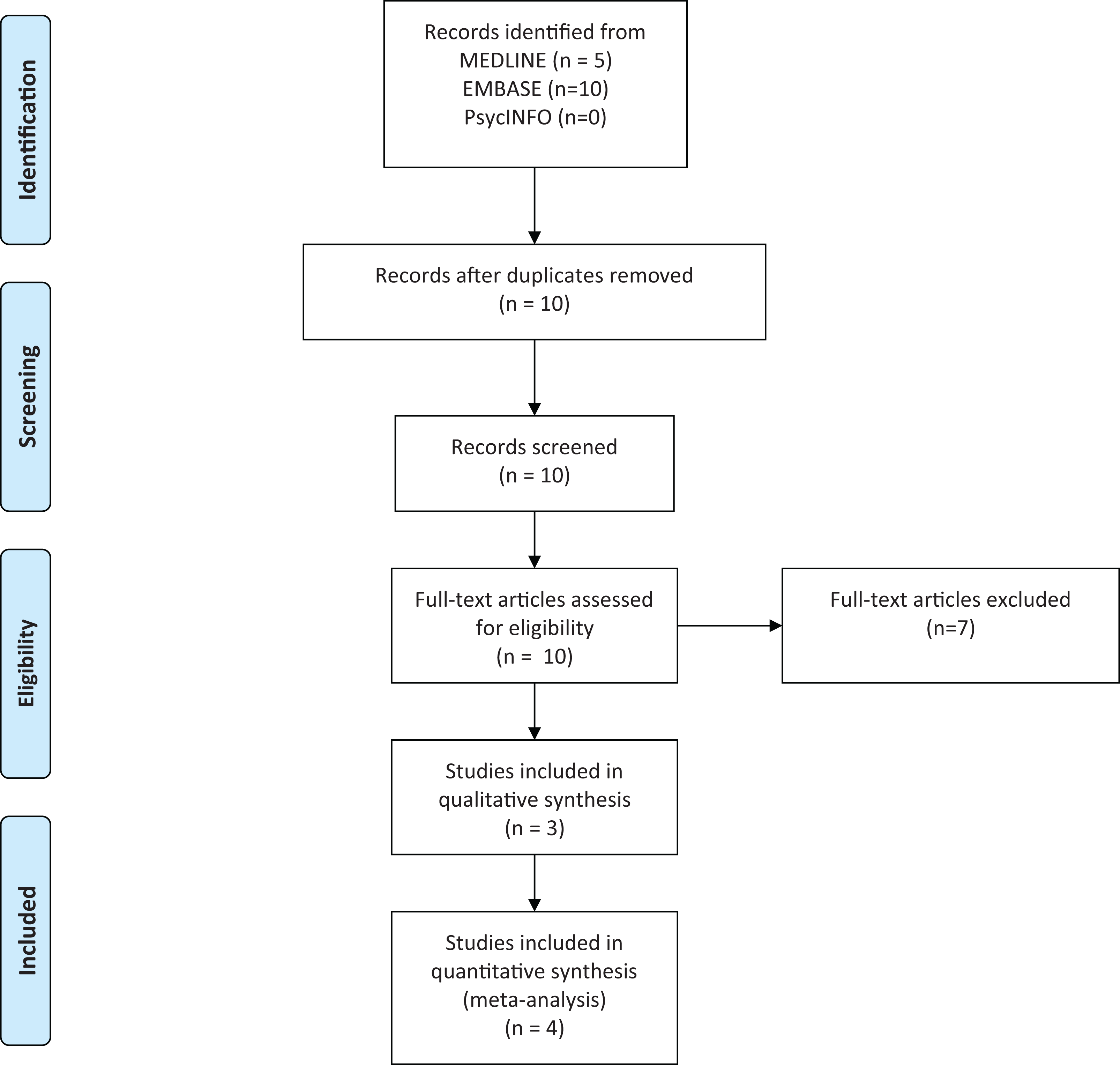
PRISMA systematic review and meta-analysis flow-chart
Risk of Bias in Included Studies (ROBINS-I).
Overall, a standardised mean difference of 0.59 (95% CI = 0.14 to 1.05, z = 2.57, P = 0.010; Figure 3A) was observed, indicating a moderate treatment effect size of rTMS on neuroticism. The classic fail-safe N indicated that 21 null or missing studies would be required to render this finding statistically non-significant. Although Egger’s regression intercept failed to reveal statistical evidence of publication bias (t(2) = 2.98, P = 0.096), the funnel plot revealed an outlying study. 35 There was evidence of statistical heterogeneity, as quantified using the Q statistic (Q-value = 11.03, df = 3, P = 0.012), by I2 (72.80), and by τ2 = 0.14, and this appeared to be driven by the same outlying study. 35 We therefore repeated our analyses excluding data from Spronk et al., 35 and found a similar statistically significant effect (SMD = 0.37; 95% CI, 0.14 to 0.59, z = 3.19, P = 0.001; Figure 3B), with minimal evidence of statistical heterogeneity (Q-value = 0.10, df = 2, P = 0.94) by I2 (0.00) and by τ2 (0.00).
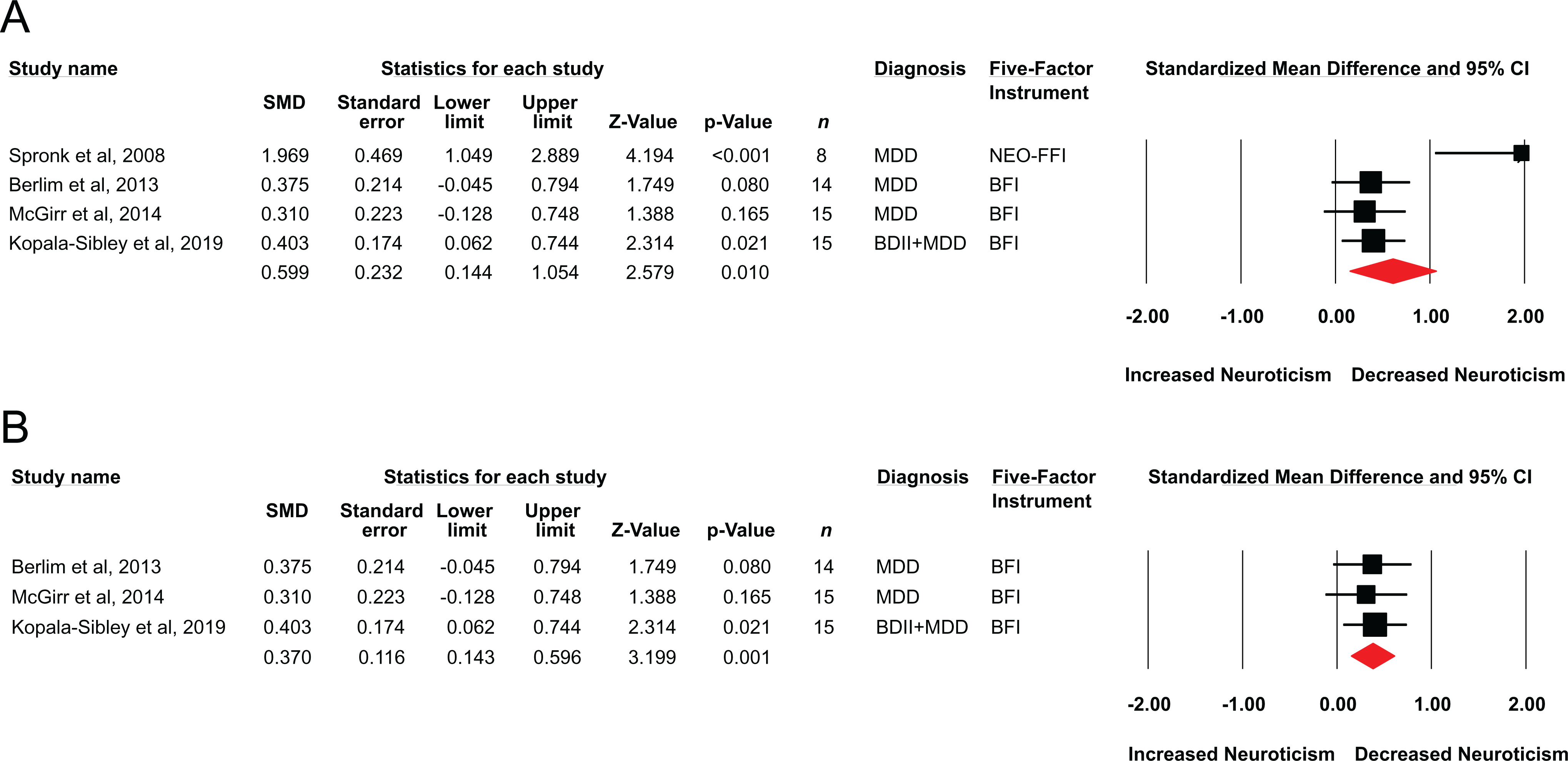
(A) Standardised mean differences for change in neuroticism scores in prospective studies of DLPFC rTMS in major depression. (B) Sensitivity analysis showing illustrating standardised mean differences after excluding the data by Spronk et al., 2008. 35
Discussion
This study investigated whether rTMS treatment for TRD can be predicted by personality vulnerabilities—neuroticism and self-criticism—and whether rTMS treatment results in changes in depression. To our knowledge, this is the first study to examine whether the trait of self-criticism predicts response to rTMS. Our analyses revealed that improvement in depressive symptoms is related to participants’ degree of self-criticism at baseline, and that self-criticism remains stable with rTMS. Meanwhile, rTMS results in decreases in neuroticism, which we then sought to confirm using a quantitative synthesis of the available literature. This meta-analysis revealed a moderate effect of rTMS on this personality trait in 4 open-label trials of rTMS in the treatment of TRD (n = 52). These results may have clinical utility, and further inform our understanding of the antidepressant mechanism of rTMS.
Our findings may also have implications both for our understanding of factors that predict rTMS treatment efficacy and for our understanding of the role of personality factors in TRD. Our findings are consistent with previous evidence that self-criticism predicts response to pharmacotherapy or psychotherapy. 22,23 Moreover, whereas neuroticism and self-criticism have some conceptual overlap, these preliminary results suggest that self-criticism is more stable than neuroticism during rTMS treatment for depression and better able to predict antidepressant response. This is consistent with neuroimaging research, which has found that engaging in self-critical thoughts or receiving critical feedback to task performance is associated with activation in the lateral prefrontal brain regions, potentially indicating involvement of brain regions linked to error processing and the monitoring of internal emotional states. 24,26 As such, these results may have clinical utility: pre-treatment screening for self-criticism may be useful in determining who is most likely to respond well to rTMS for depression; albeit, our findings require replication with a larger cohort before clinical implementation.
Where neuroticism is concerned, there is some evidence to suggest the stability of this personality dimension during pharmacological and psychotherapeutic intervention. 48 Meanwhile, others have reported that this personality trait may change during antidepressant treatment, 49 raising the possibility of state influences during acute depression or a modifiable vulnerability to TRD. To date, neuroticism has not demonstrated predictive utility of the antidepressant effects of rTMS; the conceptually similar character trait of harm avoidance has also failed to show predictive utility. 50 Our analyses demonstrating that neuroticism is modifiable by rTMS are consistent with previous DLPFC rTMS studies, where neuroticism decreased as a function of treatment. 34,35 Although we have not consistently found this effect, 36 our meta-analysis reveals that rTMS has a robust effect on neuroticism, and that insufficient statistical power, together with natural variability, may account for previous inconsistencies. Neuroticism has been linked to the DLPFC both anatomically 28 –30 and functionally, 31 –33 and therefore it will be important for future studies to examine neuroticism as a proxy biomarker for pathology that responds to DLPFC rTMS.
Limitations
This study is limited by a small convenience sample. Although the results are also limited by the absence of a sham or another appropriate control group, the clinical utility of these findings is unaffected by this limitation. Our assessment of personality traits was during a major depressive episode and, while it is reflective of information that may be used for clinical decision making and prognostication, it is complicated by both trait- and state-dependent influences. In addition, although the study is prospective, the duration of follow-up is limited, and therefore the stability of clinical improvement is unclear. This is an important question for future research, given the literature linking high self-criticism with a vulnerability to depression and the stability of this trait at the conclusion of rTMS treatment. Conversely, it will be important to determine if changes in neuroticism, a factor that also affects vulnerability to depression, can confer protection against future depressive episodes.
Our systematic review and meta-analysis also have limitations; notably, a small number of trials and the absence of a sham-comparison group to determine specificity to DLPFC rTMS. Moreover, our group has contributed 3 of the 4 studies in this field and have done so each time with the same instrument, the Big Five Inventory. Replication by other groups and using other instruments is needed.
Conclusion
Understanding efficient, non-invasive, and economically viable factors that predict who will respond to rTMS in the treatment of refractory depression is vital for treatment selection and resource allocation. The personality trait of self-criticism may provide a useful, efficient, and cost-effective predictor of response to rTMS for TRD. Neuroticism does not appear to provide prognostic value, yet rTMS has a moderate-to-large treatment effect on vulnerability to depression. Further research is required to determine whether this confers protection against future episodes of depression.
Footnotes
Acknowledgements
We are very appreciative of Sharon Willan’s assistance with providing treatments and to participants for dedicating their time.
Data Access
Data is available on communication with the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GBC was supported through Vancouver Coastal Health and the UBC Psychiatry Research Track Program.