
Abstract
Objective:
To estimate the cumulative incidence of self-reported suicide-related thoughts (SRTs) and suicide attempts (SAs) in males and females from 11 to 25 years of age in Canada.
Methods:
A cohort study was conducted by linking cycles 2 to 8 from the National Longitudinal Survey of Children and Youth, a representative survey of Canadians aged 11 to 25 years conducted from 1996 to 2009. The 11- to 25-year cumulative incidence of self-reported SRTs and SAs (with suicidal intent) was estimated in males and females using a novel application of a counting process approach to account for discontinuous risk intervals between survey cycles.
Results:
The risk of SRTs was 29% (95% confidence interval [CI], 26% to 31%) in females and 19% (95% CI, 16% to 23%) in males. The risk of SAs was 16% (95% CI, 14% to 19%) in females and 7% (95% CI, 6% to 8%) in males. Over 70% of SRTs and SAs first occur between 11 and 16 years of age and 30% between 11 and 13 years of age, respectively.
Conclusions:
The risk of SRTs and SAs is high in young Canadians, with most events first occurring in early to mid-adolescence and possibly earlier. Females are at a higher risk compared to males. This research underscores the need for better longitudinal surveillance of SRTs and SAs in the population. A counting process framework could be useful for future research using existing longitudinal surveys suffering from design limitations relating to gaps in respondent follow-up. Furthermore, these findings have implications for younger SRT and SA risk management by clinicians and earlier implementation of suicide prevention programs.
Suicide is the second leading cause of death in 15- to 29-year-olds globally. 1 Suicide-related thoughts (SRTs) and suicide attempts (SAs) 2 manifest in adolescence and are strong predictors of suicide. 3 There is little understanding of the onset and frequency of SRTs or SAs with the intent to die in children and adolescents. This is the result of 1) reliance on health care administrative data to estimate suicide-related behaviour incidence, which excludes SRTs, and individuals who did not access a hospital and where suicide-related behaviour measures are irrespective of intent, 2 and 2) lack of longitudinal and nationally representative surveys including suicide-related measures in young populations and reliance on lifetime prevalence estimates, which are known to be at high risk of recall bias. 4,5 Such knowledge would provide valuable information necessary for developing and implementing age-specific prevention strategies. Thus, the objective of this study was to estimate the cumulative incidence of self-reported SRTs and SAs in males and females from 11 to 25 years of age.
Several studies involving school and community surveys have reported the prevalence of suicidal phenomena in youth, although high heterogeneity between studies and countries exists. 6 A meta-analysis of population-based studies indicated that the lifetime prevalence of SAs, suicide-related behaviours (irrespective of intent), and SRTs in 12- to 20-year-olds is 9.7%, 13.2%, and 29.9%, respectively. 6 Findings from the 2012 Canadian Community Mental Health Survey indicated that the lifetime prevalence of SRTs in 15- to 25-year-olds was 16.2% in females and 12% in males. 7
Few population-based incidence studies of suicidal phenomena have been conducted, and most existing studies stem from health administrative data. In particular, in Ontario youth aged 12 to 17 years, the incidence rate for emergency department based self-harm was 474.5/100,000 for females and 174.6/100,000 for males from 2002 to 2007. 8 In the United States, the annual incidence rate of emergency department visits for self-harm from 2006 to 2013 peaked from 15 to 19 years (459/100,000) in females and between 20 and 24 years (270/100,000) in males. 9 In England, the annual incidence of self-reported suicide-related behaviour in the community in 2015 in 12- to 14-year-olds was 2760/100,000 in males and 8798/100,000 in females, while in 15- to 17-year-olds, it was 2598/100,000 in males and 8968/100,000 in females. 10
While health administrative data estimates of suicide-related behaviour are available internationally, the International Classification of Diseases (ICD) codes referencing self-inflicted injury and self-poisoning do not require the specification of suicidal intent and exclude those who do not go to the hospital. Therefore, these estimates include patients with a mix of suicidal and nonsuicidal behaviours and some cases of accidental self-injury. Nevertheless, most adolescents admitted to the hospital for suicide-related behaviour report prior SAs that did not lead to hospitalization, 11 and two-thirds who present to the emergency department with suicide-related behaviour express suicidal intent. 12,13 These hospital presentations may reflect a progression in behaviours that could have been previously halted. 14 As such, studies reporting on hospital admissions for suicide-related behaviour underestimate SA incidence. Furthermore, reliance on inpatient records (excluding those not admitted) to estimate SAs is problematic. Across all ages, it has been estimated that approximately 75% of SA cases presenting to the emergency department were missed by the use of inpatient ICD-10 codes referencing self-inflicted injuries from hospital discharge records. 14
Accordingly, we have a limited understanding of how many young individuals in the population first think about suicide and attempt suicide with the intent to die. In Canada, the United States, and other countries, this information is not systematically collected longitudinally. In this study, we employed the National Longitudinal Survey of Children and Youth (NLSCY) to estimate the cumulative incidence of self-reported SRTs and SAs in Canada.
Methods
Data Source
The NLSCY was a longitudinal cohort study conducted by Statistics Canada for which Canadian children, initially zero to 11 years of age, were followed to young adulthood. The sampling frame for the NLSCY was based on the Statistics Canada Labor Force Surveys, 15 a household survey covering approximately 97% of the Canadian population using multistage probability samples stratified by geographic areas. The NLSCY excludes full-time members of the Canadian Armed Forces, inmates of institutions, and those residing in Yukon, Nunavut, Northwest Territories, and Indian reserves.
Study Population
The longitudinal cohort in cycle 1 comprised of 22,831 children aged zero to 11 years between 1994 and 1995. Children were followed up biennially until between 2008 and 2009 with a maximum of 8 cycles of data collection. The outcomes of interest, SRTs and SAs, became available in cycle 2; thus, for this study, cycles 2 to 8 were linked by individual unique identifiers. Respondents who were below the age appropriate to complete the SRT and SA measures (<11 years) and those who did not complete at least 1 cycle were excluded from the study. Due to Statistics Canada budget cuts and to reduce respondent burden, the sample from cycles 1 to 2 was cut by 5928 respondents. The remaining respondents were randomly selected and accurately reflected the survey population. 15 Thus, the study population used in this study comprised 16,903 NLSCY respondents between the ages of 11 and 25 years (Figure 1).
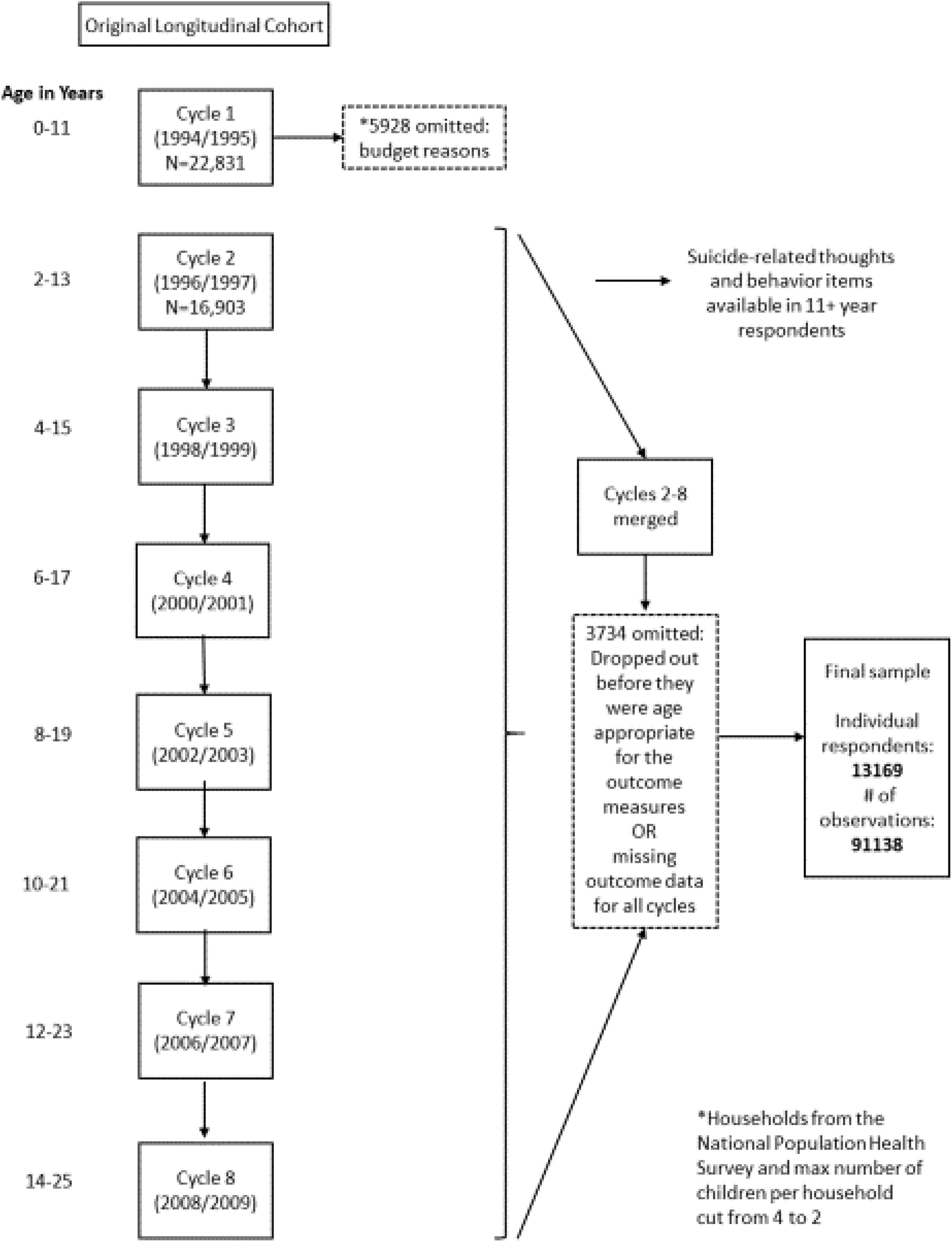
Study sample flow diagram.
Procedure
Interviews for the NLSCY were completed in person or by telephone using computer-assisted interviewing by Statistics Canada trained personnel or by self-report in schools for the child and youth questionnaires in age-appropriate respondents (11 to 17 years). 15 In cycles 6 to 8, to accommodate the aging cohort, in 18- to 25-year-olds, the youth survey was completed by computer-assisted phone interview, to capture those respondents who were no longer in school. The parent respondent completed informed consent for his or her child.
Outcome Measures
SRTs were measured by the following item: “During the past 12 months, did you seriously consider attempting suicide?” Respondents were asked to indicate yes or no. SAs were measured by the following item: “During the past 12 months, how many times did you attempt suicide?” Respondents from the youth school surveys were asked to indicate never/none, once, or more than once, while respondents from the youth self-report measure (in 18- to 25-year-olds) were asked to indicate yes or no. 15 For the purposes of this analysis and owing to small numbers of individuals indicating the “more than once” response category, the SA measure was coded as a binary variable indicating yes or no for all respondents. The wording of the SRT and SA items was different in cycle 2 compared to later cycles. In cycle 2, the phrase “try to kill yourself” was used instead of “attempt suicide.”
Statistical Analysis
To calculate the cumulative incidence of first reported SRTs and SAs over follow-up in males and females, a counting process framework 16 was used, with age in years at interview as the time scale. Because of the NLSCY response structure, discontinuous risk intervals (gaps in a respondent’s follow-up) were present. Two forms of discontinuous risk intervals were present: 1) by design and 2) by participant dropout and reentry into the survey. The assessments were spaced every 2 years, while the response format for the outcomes was during a 1-year look-back window producing 1-year gaps in time following each assessment where the outcome status is unknown. There were also scenarios where respondents dropped out of the survey at one cycle and reentered at a later cycle, and the time elapsed between assessments reflects another form of discontinuous risk interval. To account for these discontinuous risk intervals, a counting process approach was used. 16 Incidence was estimated in 2 ways: not accounting for the discontinuous risk intervals by design (which possibly underestimates incidence if events occur during these 1-year gaps) and accounting for discontinuous risk intervals by design (which possibly overestimates incidence by cutting the time at risk approximately in half through removing the 1-year gaps after each cycle from the risk set). Both approaches accounted for discontinuous risk intervals by respondent dropout. To avoid overestimating incidence, primary results are presented while not accounting for discontinuous risk intervals by design. Implications of both approaches are discussed.
Using a counting process approach, all respondents contribute a row of data with a start and stop time reflecting each time interval they were observed as at risk, until they report the outcome, and among those not reporting the outcome, until their last assessment. Cumulative incidence was estimated as the inverse of the survival probability. This approach accounts for different ages and follow-up periods, present in the NLSCY.
Sensitivity analyses were conducted to determine if individuals with 1 or 2 cycles of nonresponse compared to those with complete response across all cycles differed significantly in main outcomes.
The NLSCY involved a complex survey design. To produce unbiased estimates of the population, all reported estimates are weighted using the longitudinal weights provided by Statistics Canada. 15 The design weights reflect the inverse probability of selection and account for poststratification and nonresponse. To estimate the frequencies of first captured SRTs and attempts, SAS procedures for complex surveys were used to estimate weighted frequencies. Variances were estimated using the bootstrap weights provided by Statistics Canada using the balanced repeated replication method. All analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC).
Results
The original longitudinal cohort at cycle 2 comprised 16,903 individual respondents (Figure 1). There were 828 respondents classified as out of scope, indicating that they died, moved out of province or to an Indian Reserve, or their age was out of range. As such, less than 3.6% of the original longitudinal sample died during the study follow-up. From the cohort sampled at cycle 2 (16,903), there were 3734 (22%) cases where respondents did not contribute to cycles 2 to 8 and were excluded either due to nonresponse or not being age appropriate for the outcome measures (Figure 1). The final sample analyzed includes 13,169 respondents (6601 females and 6568 males) with a weighted total of 3,745,388 respondents.
Among Canadians aged 11 to 25 years reporting SRTs, the highest proportion first occurred between 14 and 16 years of age in both males and females. The proportion reporting these thoughts from 11 to 13 years of age was 32% in both females and males. When attempts occurred, the peak times were at a later age in females compared to males, where the highest proportion of attempts occurred between 14 and 16 years in females (52%) and between 11 and 13 years in males (38%) (Table 1).
Timing of First Captured Suicide-Related Thoughts and Attempts in Males and Females among Those Reporting Thoughts and Attempts by Age from 1996 to 2009, Weighteda to Reflect the Canadian General Population.
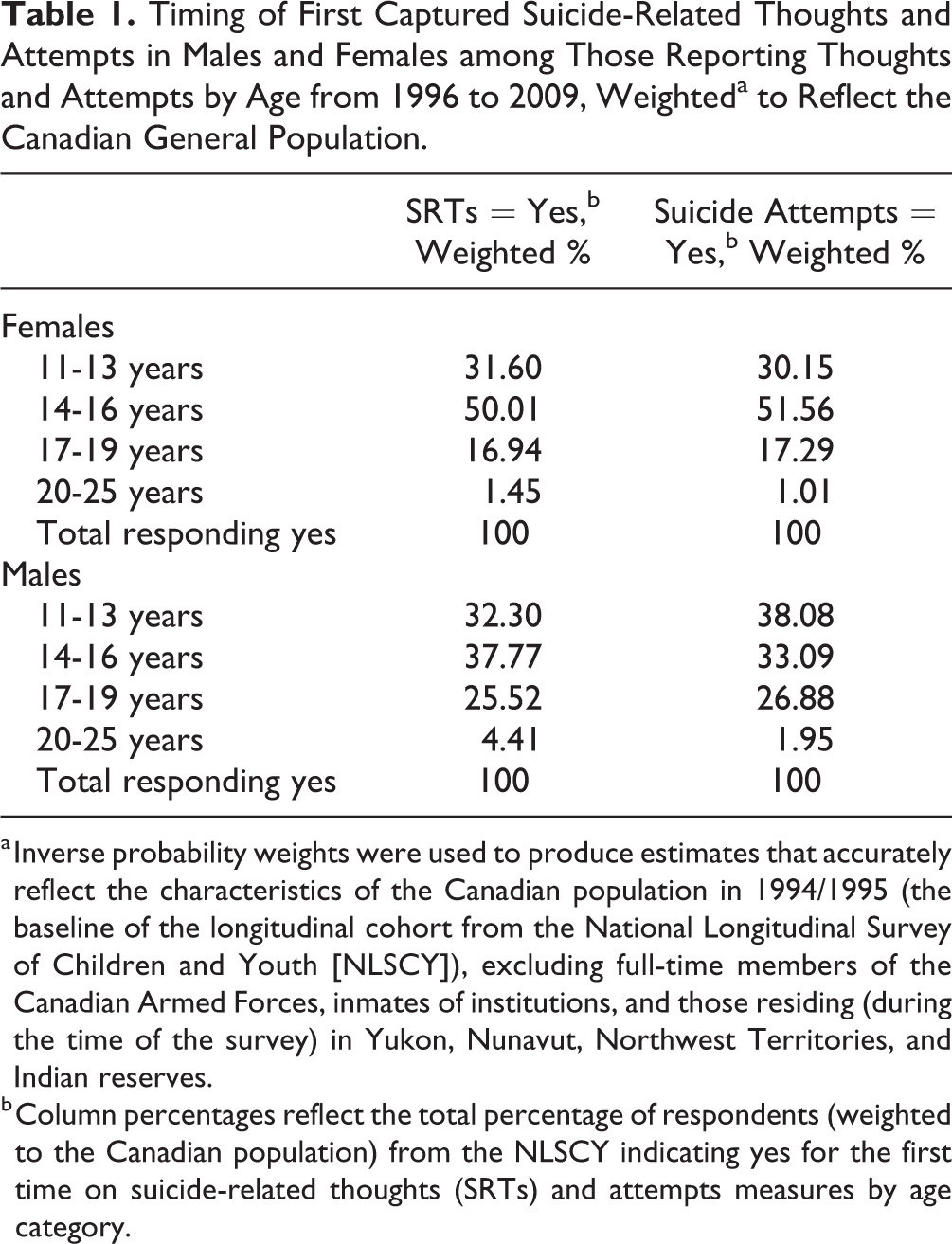
a Inverse probability weights were used to produce estimates that accurately reflect the characteristics of the Canadian population in 1994/1995 (the baseline of the longitudinal cohort from the National Longitudinal Survey of Children and Youth [NLSCY]), excluding full-time members of the Canadian Armed Forces, inmates of institutions, and those residing (during the time of the survey) in Yukon, Nunavut, Northwest Territories, and Indian reserves.
b Column percentages reflect the total percentage of respondents (weighted to the Canadian population) from the NLSCY indicating yes for the first time on suicide-related thoughts (SRTs) and attempts measures by age category.
The 11- to 25-year cumulative incidence of SRTs in males and females was 19% (95% confidence interval [CI], 16% to 23%) and 29% (95% CI, 26% to 31%), respectively (Figure 2). The cumulative incidence of SAs was 7% (95% CI, 6% to 8%) in males and 16% (95% CI, 14% to 19%) in females (Figure 3). In both females and males, the cumulative incidence of SRTs more than doubled from 11 to 13 years of age (females: 8% [95% CI, 7% to 9%]; males: 4% [95% CI, 3% to 5%]) to 11 to 16 years of age (females: 21% [95% CI, 19% to 23%]; males: 10% [95% CI, 9% to 11%]) (Figure 2). In females, the cumulative incidence of having a SA was approximately 4% (95% CI, 3% to 5%) from 11 to 13 years, and by age 16, this risk tripled to 12% (95% CI, 11% to 13%). In males, the cumulative incidence of SAs from 11 to 13 years and from 11 to 16 years was 2% (95% CI, 2% to 3%) and 4% (95% CI, 3% to 5%), respectively (Figure 3).
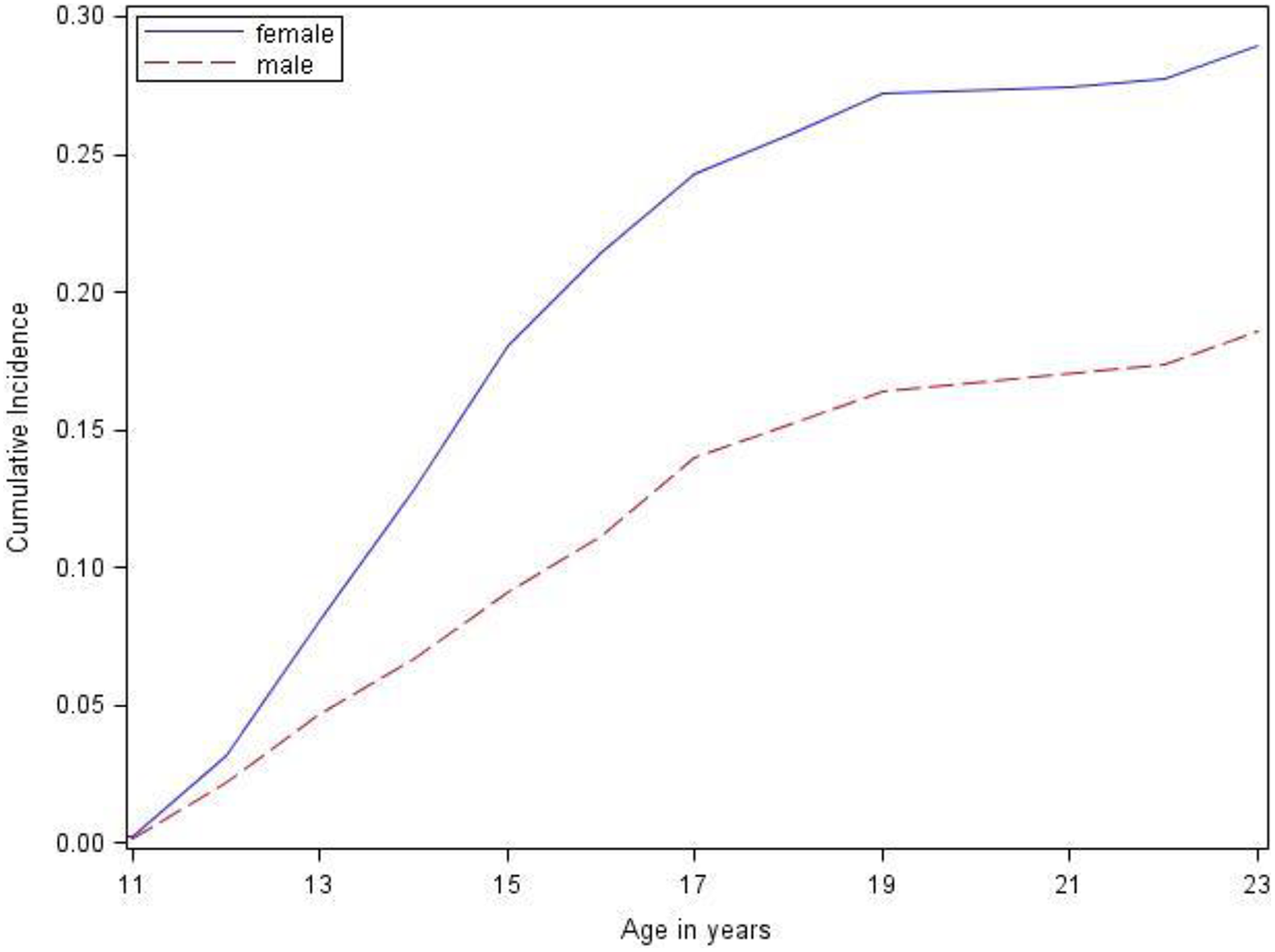
Cumulative incidence of suicide-related thoughts in males and females from 1996 to 2009, weighted to reflect the Canadian general population. Cumulative incidence was estimated as 1-survival, calculated from a counting process model. The upper tail end was collapsed in keeping with Statistics Canada release guidelines. Inverse probability weights were used to produce estimates that accurately reflect the characteristics of the Canadian population in 1994/1995 (the baseline of the longitudinal cohort from the National Longitudinal Survey of Children and Youth [NLSCY]), excluding full-time members of the Canadian Armed Forces, inmates of institutions, and those residing (during the time of the survey) in Yukon, Nunavut, Northwest Territories, and Indian reserves.
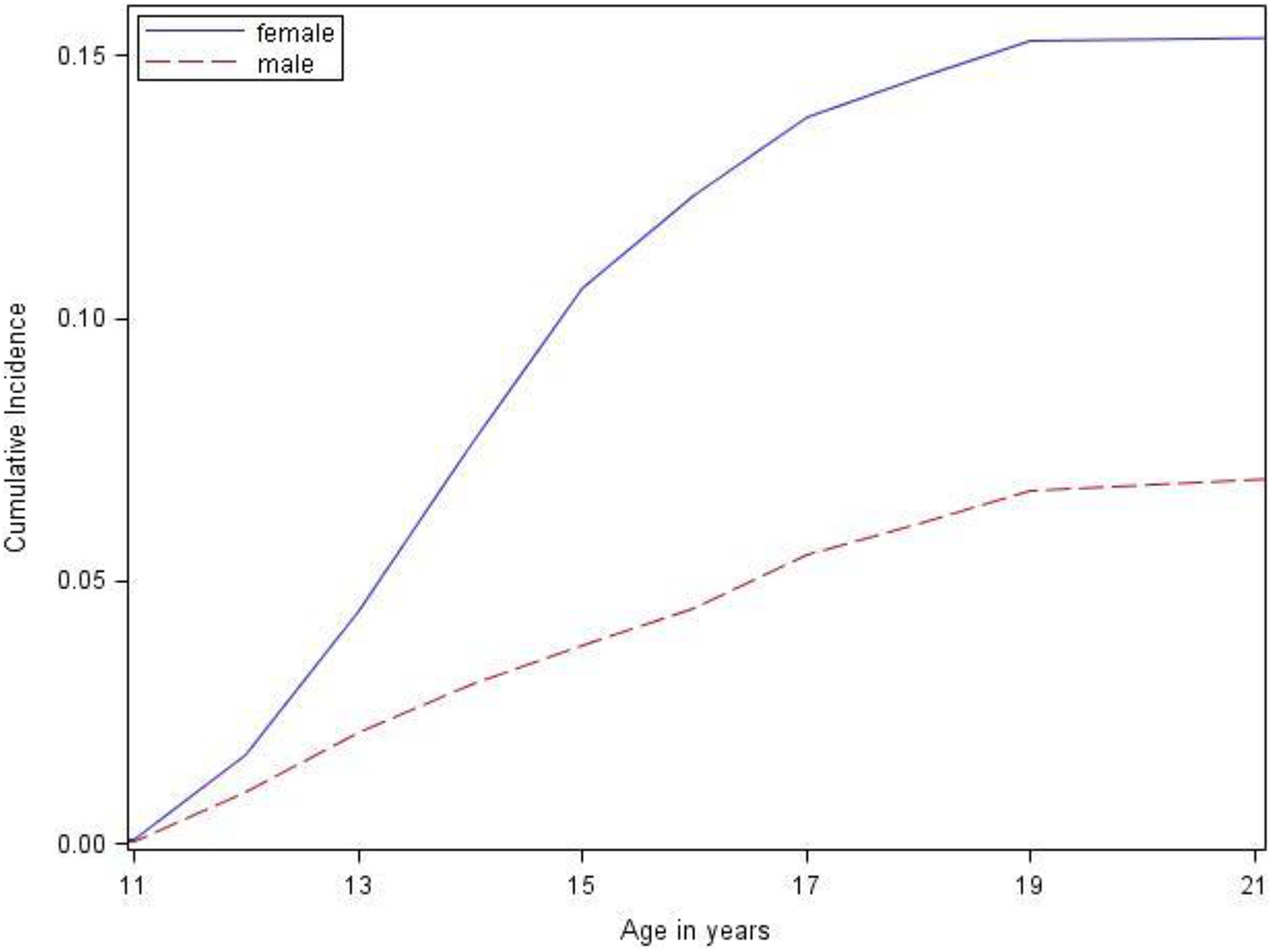
Cumulative incidence of suicide attempts in males and females from 1996 to 2009, weighted to reflect the Canadian general population. Cumulative incidence was estimated as 1 <@150> survival, calculated from a counting process model. The upper tail end was collapsed in keeping with Statistics Canada release guidelines. Inverse probability weights were used to produce estimates that accurately reflect the characteristics of the Canadian population in 1994/1995 (the baseline of the longitudinal cohort from the National Longitudinal Survey of Children and Youth [NLSCY]), excluding full-time members of the Canadian Armed Forces, inmates of institutions, and those residing (during the time of the survey) in Yukon, Nunavut, Northwest Territories, and Indian reserves.
Sensitivity analyses to determine the impact of cycle nonresponse on cumulative incidence estimates did not reveal major differences. For example, the 11- to 25-year cumulative incidence of SAs changed from 7% to 6% for males and 16% to 14% in females, while the cumulative incidence of SRTs changed from 19% to 18% in males and 29% to 27% in females (online supplemental table).
The cumulative incidence of both outcomes was estimated while additionally accounting for the discontinuous risk intervals by design. Using this approach, the cumulative incidence of SRTs between 11 and 25 years of age in females and males was 50% (95% CI, 44% to 55%) and 34% (95% CI, 29% to 37%), while the cumulative incidence of SAs between 11 and 25 years of age was 28% (95% CI, 26% to 31%) and 13% (95% CI, 11% to 16%), respectively.
Discussion
This study is unique, providing cumulative incidence estimates of self-reported SRTs and SAs (measuring the intent to die) from the age range of 11 to 25 years. The incidence of thinking about suicide in males and females by 11 to 25 years of age was high, 29% in females and 19% in males, with estimates possibly as high as 50% and 34%, respectively. Furthermore, the incidence of attempting suicide by age 25 was 16% in females and 7% in males, with estimates possibly as high as 28% and 13%, respectively. It is challenging to compare these estimates to other published reports because existing incidence studies are largely of ICD-coded hospital presentations, where as expected, the incidence over adolescence and young adulthood is much smaller, typically under 1%. Moreover, among the few conducted incidence studies of self-reported SRTs or SAs, the age range was narrower, typically not reported below 12 years, and incidence estimates were annual rates, 17 rather than cumulative, or studies used long recall periods. 18,19 As such, the cumulative incidence reported here is higher than prior published incidence reports. In terms of prevalence, the 11- to 25-year cumulative incidence of SRTs in this study is consistent with the average lifetime prevalence estimate from a meta-analysis of population-based studies of 12- to 20-year-olds synthesizing studies up until the year 2000. 6 Our cumulative incidence estimates of both SRTs and SAs are higher than more recent lifetime prevalence studies 7,20 –22 and annual prevalence studies 23 –25 in youth and young adults between 12 and 25 years of age. Lifetime prevalence studies are limited by recall biases that have been shown to underestimate incidence. 26 Furthermore, some of these studies measured SRTs and SAs in the context of major depression, 21 and cases of SRTs and SAs can be missed among respondents not meeting criteria for depression-related gate questions. 27
Considering the methodological limitations of existing incidence and prevalence studies of SRTs and SAs, the true incidence of these thoughts and behaviours in the population, irrespective of a hospital setting, is likely higher than previously reported. Furthermore, no study has employed the method used in this study to more accurately estimate the time at risk. We estimated incidence in 2 ways: 1) not accounting for the discontinuous risk intervals by design (which assumes events did not occur in the year after each cycle), leading to a possibility of underestimating incidence, and 2) accounting for the discontinuous risk intervals by design (which cuts the time at risk by almost half), leading to a possibility of overestimating incidence. On one hand, there is the possibility that respondents in the NLSCY recalled events since last assessment (rather than the past year look-back window), which would reflect a 2-year window. If this were true, it would be acceptable to assume that the outcome did not occur during these 1-year gaps, making it appropriate to make this assumption. On the other hand, there may be missed events during these gap years. Ultimately, the risk of SRTs and SAs is likely somewhere in between the 2 reported scenarios, both of which indicate that these outcomes are common in the population, much more so than previously reported.
Sex Differences
The risks of SRTs and SAs from individuals 11 to 25 years of age were 1.5 times and 2.3 times higher in females compared to males, respectively. These findings are consistent with the extant literature showing higher rates of these phenomena in females compared to males in adolescence and early adulthood. 6,28 The pattern of first captured events from age 11 years on was similar between males and females for SRTs, where the majority of first occurring thoughts were observed between 11 and 16 years, with the peak time for these events to start between 14 and 16 years. This is inconsistent with other population-based incidence studies of hospital presentations for suicide-related behaviour reporting peaks at later ages, from 15 to 19 years of age in females and even later in males, between 20 and 24 years of age. 9,29,30 Suicide-related behaviour may be less lethal in adolescents compared to adults, 31 which could in part explain this discrepancy. However, this hypothesis assumes that hospital presentations are in fact more serious than self-reported SAs, which, to our knowledge, have not been examined. Some portion of the latter group may be quite suicidal and/or engage in more lethal behaviours, yet never seek formal care. The concern is that without broader and early prevention strategies that reach these youth, they may progress to more lethal behaviours. Nevertheless, there were dramatic jumps in risk of SRTs and SAs from 13 to 16 years of age in both males and females. SRTs and SAs begin to onset in parallel with pubertal changes, which may in part explain more pronounced differences in incidence between females and males at younger ages as well as dramatic increases in risk during this time. 32
Strengths and Limitations
This study used a novel application of a counting process approach to estimate cumulative incidence. The design of the NLSCY, like many other panel surveys, poses analytical challenges, including loss to follow-up, nonexact event times, and discontinuous risk intervals. The approach applied in this study was able to use all available data from the NLSCY and appropriately estimate time at risk among participants dropping out and reentering the survey.
Another concern relating to these longitudinal data surrounds attrition and whether cycle nonresponse was associated with the outcome. However, our sensitivity analyses confirmed that the incidence did not significantly change after excluding those with incomplete follow-up.
The outcomes reported are based on self-report, thereby increasing the risk of misreporting. Factors that significantly contribute to inaccurate estimates of self-reported suicidal phenomena in adolescents include lack of anonymity 6 or perceived privacy and confidentiality, 26 misunderstanding of the definition used, 33 and social desirability. 34 The questions used in the NLSCY explicitly refer to suicide, thereby reducing potential confusion over nonsuicidal behaviours. 35 Moreover, the youth survey was paper and pencil, and youth respondents were ensured confidentiality from their parents and teachers when completing the measure.
The incidence estimates reported may by outdated, deriving from data collected between 1996 and 2009. However, there are no newer Canadian, nationally representative longitudinal studies measuring these outcomes.
The NLSCY did not include a measure of suicide or other causes of death. Therefore, we were unable to account for the competing risk of death. While the proportion of respondents dying over follow-up was low (<3.6%), this competing risk could have altered our primary results toward an underestimation.
The NLSCY also does not provide information on lifetime SRTs or SAs. Therefore, we were unable to determine if there were events occurring prior to baseline, below the age of 10 years. However, suicidal phenomena are very rare under the age of 10 years, 3 and we expect that most events reported here were the first occurring.
The NLSCY does not include a measure of nonsuicidal behaviour, a predictor of SAs and possibly suicide, which fluctuates over time along with SRTs and SAs. 36 Further understanding of the epidemiology of these behaviours is needed to fully understand their collective burden.
Finally, the NLSCY excludes Canadians residing on Indian reserves and as a result omits an important population at high risk for suicide. Further research is necessary to also understand when SRTs and SAs start to occur in aboriginal populations.
Conclusions
The risk of thinking about suicide and attempting suicide with the intent to die is common in young Canadians, particularly in females. These thoughts and behaviours start to occur in early to mid-adolescence, earlier than reported rates of hospital presentations for suicide-related behaviour. This underscores the need for better surveillance of SRTs and SAs in the population, as hospital presentations for suicide-related behaviours exclude a substantial proportion of youth reporting attempts and do not routinely collect information on SRTs. This study used a novel application of a counting process approach to estimate cumulative incidence using a methodologically complex survey. This approach could be applied to other longitudinal surveys that have the same methodological limitations involving discontinuous risk intervals, contributing to improved surveillance of SRTs and SAs. These findings suggest that clinicians be aware of the young ages of SRT and SA onset when conducting mental health assessments and managing risk. These findings also suggest that primary suicide prevention programs targeting youth could be implemented earlier. School-based prevention programs aimed at strengthening protective factors in students have been effective in reducing the risk of SAs. 37 Yet, such preventions 38 –40 target the mid- to late-adolescent population. Future and ongoing programs may consider targeting younger ages, ideally before the onset of suicide-related behaviour. Prior SAs are strong risk factors for suicide reattempts and suicide, 3 making it increasingly challenging to intervene after the initial attempt. Accordingly, it should be a priority for suicide prevention efforts to start at younger ages, before youth enter the trajectory toward suicide.
Supplemental Material
Supplemental Material, 787794_Supp_table - The Cumulative Incidence of Self-Reported Suicide-Related Thoughts and Attempts in Young Canadians
Supplemental Material, 787794_Supp_table for The Cumulative Incidence of Self-Reported Suicide-Related Thoughts and Attempts in Young Canadians by Sarah M. Goodday, Susan Bondy, Rinku Sutradhar, Hilary K. Brown, and Anne Rhodes in The Canadian Journal of Psychiatry
Footnotes
Data Access
This study was a secondary analysis of data collected by Statistics Canada. As per Statistics Canada privacy and confidentiality guidelines, data cannot be released or shared with outside parties that have not applied for access through Canadian Research Data Centers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by an Ontario Graduate Scholarship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.