
Abstract
Objective:
The role of mental illness and addiction in acute care use for chronic medical conditions that are sensitive to ambulatory care management requires focussed attention. This study examines how mental illness or addiction affects risk for repeat hospitalization and/or emergency department use for ambulatory care–sensitive conditions (ACSCs) among high-cost users of medical care.
Method:
A retrospective, population-based cohort study using data from Ontario, Canada. Among the top 10% of medical care users ranked by cost, we determined rates of any and repeat care use (hospitalizations and emergency department [ED] visits) between April 1, 2011, and March 31, 2012, for 14 consensus established ACSCs and compared them between those with and without diagnosed mental illness or addiction during the 2 years prior. Risk ratios were adjusted (aRR) for age, sex, residence, and income quintile.
Results:
Among 314,936 high-cost users, 35.9% had a mental illness or addiction. Compared to those without, individuals with mental illness or addiction were more likely to have an ED visit or hospitalization for any ACSC (22.8% vs. 19.6%; aRR, 1.21; 95% confidence interval [CI], 1.20-1.23). They were also more likely to have repeat ED visits or hospitalizations for the same ACSC (6.2% vs. 4.4% of those without; aRR, 1.48; 95% CI, 1.44-1.53). These associations were stronger in stratifications by mental illness diagnostic subgroup, particularly for those with a major mental illness.
Conclusions:
The presence of mental illness and addiction among high-cost users of medical services may represent an unmet need for quality ambulatory and primary care.
There is a need to intervene with high-cost users of health care who account for severely disproportionate health care spending. 1 Many high-cost users are categorized as such in a given year due to an acute illness or traumatic event, 2 but high-cost users exclusively of medical care (after mental health costs are excluded) who have comorbid mental illness have proportionally higher costs. 3 High-cost users with mental illness also have more chronic medical conditions for which they are accessing acute care. 4 Many of these conditions, such as diabetes, chronic obstructive pulmonary disease (COPD), and hypertension, 5,6 may qualify as ambulatory care–sensitive conditions (ACSCs)—illnesses that can often be effectively managed with appropriate outpatient care. 7,8 Thus, emergency department (ED) visits and hospitalizations for ACSCs are a widely used negative indicator for the accessibility and quality of primary and outpatient care. 6,9,10
Studies show that individuals with mental illness and addiction diagnoses have higher rates of acute care use for ACSCs relative to those without mental illness comorbidity, 11 –18 and researchers advocate that the role of mental and physical illness comorbidity in potentially preventable acute care use requires focussed attention. 11 –13 Many studies report these trends to be greatest for people with more severe and chronic mental illnesses, such as schizophrenia, and substance use disorders, 14,17,18 while others have found that mood and anxiety disorders were more highly associated with ACSC acute care use. 12,15 Potential mechanisms for this association include avoided or delayed help seeking for physical illnesses 19 –21 and underrecognized physical issues when complex mental health symptoms dominate the clinical picture paired with a lack of provider skill to assess and manage this comorbidity. 22,23 In theory, an ED visit or hospitalization for an ACSC provides an opportunity to strengthen an individual’s community care plan with a goal of improving health and decreasing risk for repeat visits. Therefore, further knowledge about the extent of ED visits and hospitalizations, particularly repeat visits for ACSCs among high-cost medical care users with mental illness and/or addiction, will be useful for planning of supports and services targeting this complex group. In this study, we examine rates of ED visits and hospitalizations for ACSCs, including repeat visits for the same ACSC, in a cohort of the highest-costing users of medical care in Ontario, Canada, comparing the risk of ED visits and hospitalization between those with and without diagnosed mental health comorbidity.
Methods
Design and Data Sources
This study used a population-based cohort of Ontario residents described previously. 3 In Ontario, all physician and hospital-based health care is covered by the provincial health plan and is recorded in provincial and national health administrative databases. One notable exception is care rendered by outpatient nonphysician health care providers. For all individuals in Ontario, we used health administrative data retrieved from the Institute for Clinical Evaluative Sciences (ICES), where data from various sources are de-identified and linked using an encrypted health care number. Several databases (see Appendix A) were accessed to extract individual-level demographics and medical service use during the observation year, as well as mental illness and addiction service use during the 2 years prior. The data contained in these databases are accurate and reliable with respect to demographic and diagnostic coding. 24 This study was approved by the Research Ethics Board at Sunnybrook Health Sciences Centre (ICES logged study: 20140904318000).
Participants
The study cohort consisted of all Ontarians with a valid health card who were 18 or older as of April 1, 2011 (the index date). For all individuals in the cohort, we calculated medical (i.e., non–mental health) costs for the 2011 to 2012 fiscal year. Medical costs comprised all expenditures associated with the most costly medical services only, which account for 80% of health care spending in Ontario. These costs represent (1) acute inpatient care (excluding obstetrical deliveries), (2) ED visits, (3) continuing care services (inpatient rehabilitation, complex continuing care hospitalizations, and home care), and (4) complex ambulatory care, including same-day surgeries and hospital-based dialysis and oncology care. A validated costing approach was used, 25 which bases cost calculations for all services, excluding home care, on cost per unit for a given service type multiplied by the amount of utilization, weighted for patient complexity using a case-mix methodology for hospital resources and standardized to the fiscal year. Home care costs are calculated using hourly rates for nonphysician care and physician billing claims. We ranked individuals with medical care costs greater than zero into percentiles, 3 and to focus on high-cost users only as others have done previously, 26,27 we selected the top 10% of this sample ranked by cost.
Exposure: Comorbid Mental Illness and Addiction
We defined comorbid mental illness and addiction using inpatient and outpatient care utilization data during the 2 years prior to the index date (April 1, 2009, to March 31, 2011). Mental illness and addiction diagnoses were based on inpatient psychiatric admissions, psychiatric ED visits, and outpatient visits to either to a psychiatrist or family physician for a mental health reason (determined with a validated algorithm 28 ). We identified individuals in the cohort as belonging to nonmutually exclusive diagnostic groupings: (1) no mental illness or addiction (referent group), (2) any mental illness or addiction, (3) any major mental illness or addiction (any of major mood [including depressive and bipolar disorders], psychotic, or substance use disorders), (4) major mood disorder, (5) psychotic disorder, and (6) substance use disorder. The definition of any mental illness consisted of noncognitive diagnoses inclusive of a range of mental disorders captured in the administrative data. These diagnostic groupings and the associated health administrative codes are listed in Appendix B. The referent group was defined as the absence of any of the mental illness and addiction diagnoses listed in Appendix B. Diagnostic codes in Ontario physician billing data are accurate with respect to these broad categories of illness, with some variability at the level of specific disorders. 29
Outcomes: Health Care Use for Ambulatory Care–Sensitive Conditions
We used a definition of ACSC previously validated with Ontario health administrative data. 5 The ACSCs were angina pectoris, asthma, pneumonia, cellulitis, congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), dehydration, diabetes mellitus, gastroenteritis, grand mal status and epileptic convulsions, hypertension, hypoglycemia, kidney infections and urinary tract infections (UTIs), and severe ear, nose, and throat infections. We categorized all individuals as having any unplanned ED visit not resulting in hospitalization, any hospitalization, and any unplanned ED visit resulting in discharge or hospitalization where the primary diagnosis was any of the defined ACSCs. We also categorized individuals as having any 2 ED visits, hospitalizations, and ED visits or hospitalization for the same ACSC. This categorization was intended to capture repeat visits for the same ACSC that may indicate poor ability to manage conditions in the community and potentially lack of engagement with primary or other outpatient specialty care. We further examined ED visits or hospitalizations as a single outcome for each specific ACSC to identify those conditions with the highest rate of repeat visits.
Covariates
From the individual data, we recorded age, sex, income quintile based on neighbourhood, and region of residence (urban or rural) as of the index date. Using health care data from the 2011 to 2012 year, we also assessed for the presence or absence of 17 Charlson medical comorbidities 30 and coded individuals as having 0, 1, or 2 or more. To assess medical illness severity and chronicity, we used the Johns Hopkins Aggregated Diagnosis Groups (ADG) quintiles (Johns Hopkins ACG system, version 10). 31 ADGs comprise 32 diagnostic clusters assigned based on the etiology, duration and severity of the condition, diagnostic certainty, and need for specialty care involvement. 31 The 3 ADGs that represent psychosocial conditions (ADGs 23-25) were excluded to focus on physical illness chronicity only.
Data Analysis
For each mental illness and addiction diagnostic group, we compared the rate of any ED visit and hospitalization for ACSCs, as well as repeat visits among those with mental illness and addiction to the referent group with no mental illness or addiction. We calculated risk ratios for having any visit for an ACSC and repeat visits for the same ACSC in the presence of mental health and addiction comorbidity versus not, unadjusted and adjusted for age, sex, residence (urban or rural), and income quintile. Each analysis was done for any mental illness and addiction and stratified for each specific mental illness and addiction diagnostic group. All statistical analyses were conducted using SAS Statistical software for UNIX (version 9.4; SAS Institute, Cary, NC).
Results
Our cohort of all Ontarians 18 years and older as of April 1, 2011, who comprised the top 10% of medical care users by cost consisted of 314,936 individuals. This represents 2.9% of the entire adult population of Ontario, which accounts for 72.1% of all costs, totalling $11.3 billion Canadian dollars. In this cohort, 35.9% (n = 113,102) had any mental illness or addiction; 13.2% (n = 41,662) had a diagnosed major mental illness. Table 1 contains baseline characteristics for each mental illness and addiction diagnostic subgroup. Compared to the referent group, individuals with mental illness or addiction were younger, lower in socioeconomic status, and more often living in urban regions. Those with mental illness or addiction were more often female, with the exception of those with substance use disorders who were more often male. There were significant differences in the medical illness profiles of the groups, with the mental illness and addiction groups being less likely to have 2 or more Charlson comorbidities and only slightly higher ADG scores in the index year (Table 1).
Baseline (as of April 1, 2011) Sociodemographic and Illness Variables across Mental Illness and Addiction Diagnostic Groups.
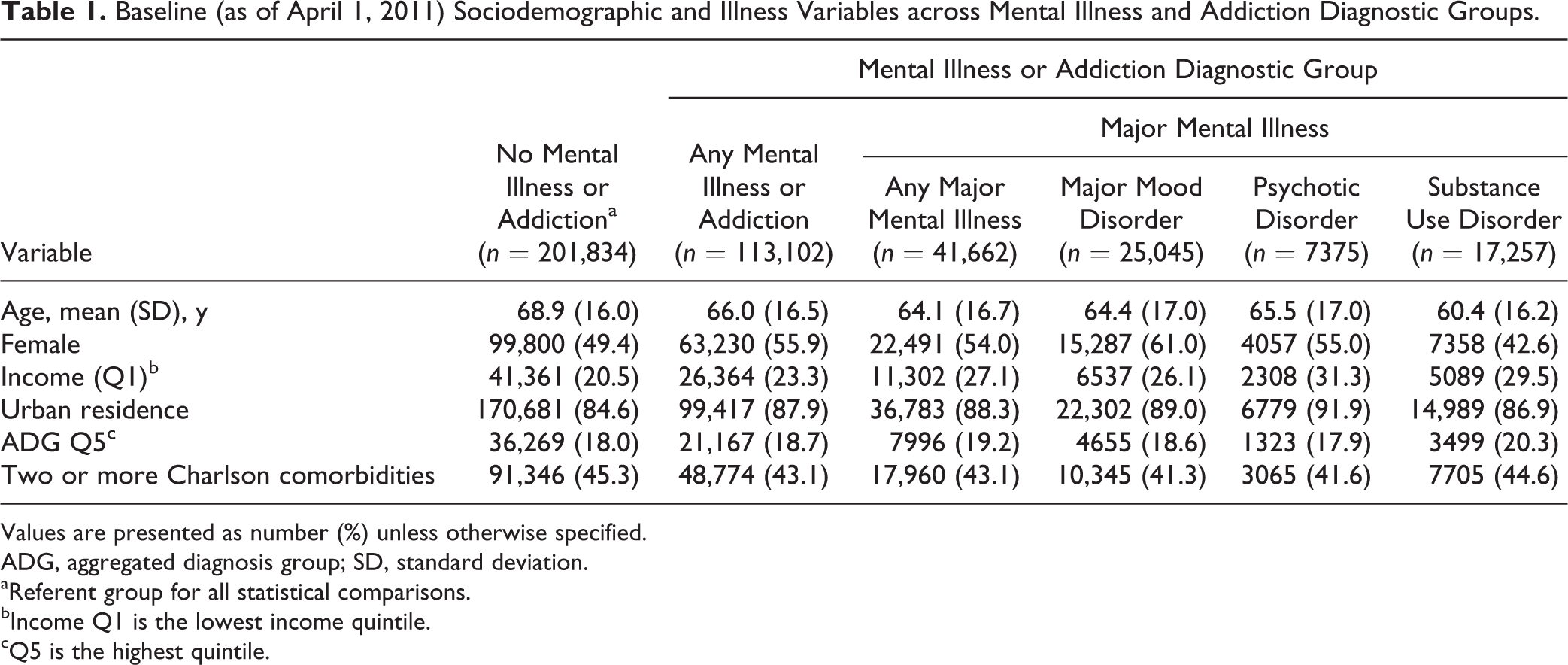
Values are presented as number (%) unless otherwise specified.
ADG, aggregated diagnosis group; SD, standard deviation.
aReferent group for all statistical comparisons.
bIncome Q1 is the lowest income quintile.
cQ5 is the highest quintile.
Out of all hospitalizations and ED visits in this cohort during the observation year, 12.5% were for ACSC (16.3% of hospitalizations and 8.7% of ED visits). The group with diagnosed psychotic disorders had the highest rate of ACSC hospitalizations (24% of all hospitalizations) (Table 2). Within the cohort, 65,491 (20.8%) of individuals had any hospitalization or ED visit for an ACSC. The rate of any ED visit or hospitalization for any of the ACSCs ranged from a low of 19.6% in the no mental illness and addiction group to 29.5% in the diagnostic group with psychotic disorders, which is substantially and significantly higher (Table 2). Mental illness or addiction was associated with a 20% increased risk of having any ACSC visit, relative to individuals without mental illness comorbidity, with this risk increasing among the major mental illness diagnostic groups (Table 2). Specific ACSC visit rates (Figure 1) varied by mental illness diagnostic groups, with higher proportions of individuals in the mental illness groups using the ED or being hospitalized for asthma, cellulitis, COPD, dehydration, diabetes, seizure, UTI, pneumonia, and ear, nose, throat infections. In most cases, rates went up with severity of mental illness and addiction comorbidity (i.e., higher when the diagnosis was narrowed to major mental illness only).
Rates of ED Visits and Hospitalization for Any ACSC.
ACSC, ambulatory care–sensitive condition; CI, confidence interval; ED, emergency department; RR, risk ratio.
aReferent group for all statistical comparisons.
bRRs adjusted for age, sex, residence (urban or rural), and income quintile
***P < 0.001.
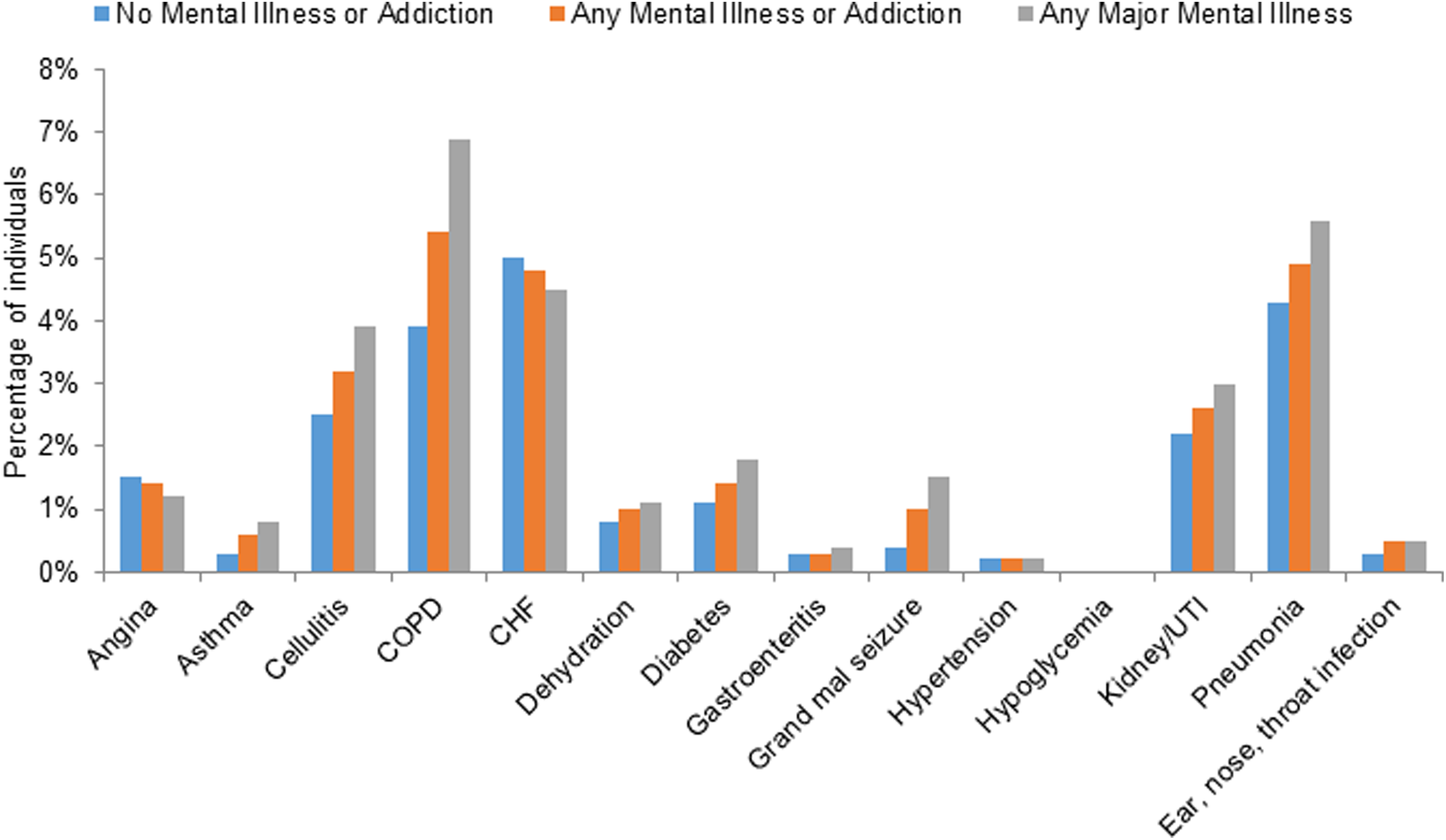
Rate of any emergency department visit or hospitalization for each ambulatory care–sensitive condition category by mental illness or addiction diagnostic subgroup. CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; UTI, urinary tract infection.
Mental illness comorbidity was also associated with increased risk of having a repeat visit for the same ACSC inclusive of ED visits and hospitalizations (Table 3). This pattern persisted across all diagnostic categories and was most pronounced for psychotic and substance use disorders. The specific ACSCs for which the proportion of visits that were repeat visits (ED visits or hospitalizations) was at least 10% higher in the any mental illness and addiction group compared to the referent group included asthma (44% vs. 32%), diabetes (33% vs. 18%), and grand mal seizure (41% vs. 29%) (Figure 2). The same patterns held in diagnostic subgroups with a 10% difference also present for rates of COPD in the major mental illness group (53% vs. 40%) (Figure 2) and ear, nose, and throat infection visits in psychotic disorders only (31% vs. 8%) (not shown).
Rates of Repeat ED Visits and Hospitalizations for the Same ACSC.
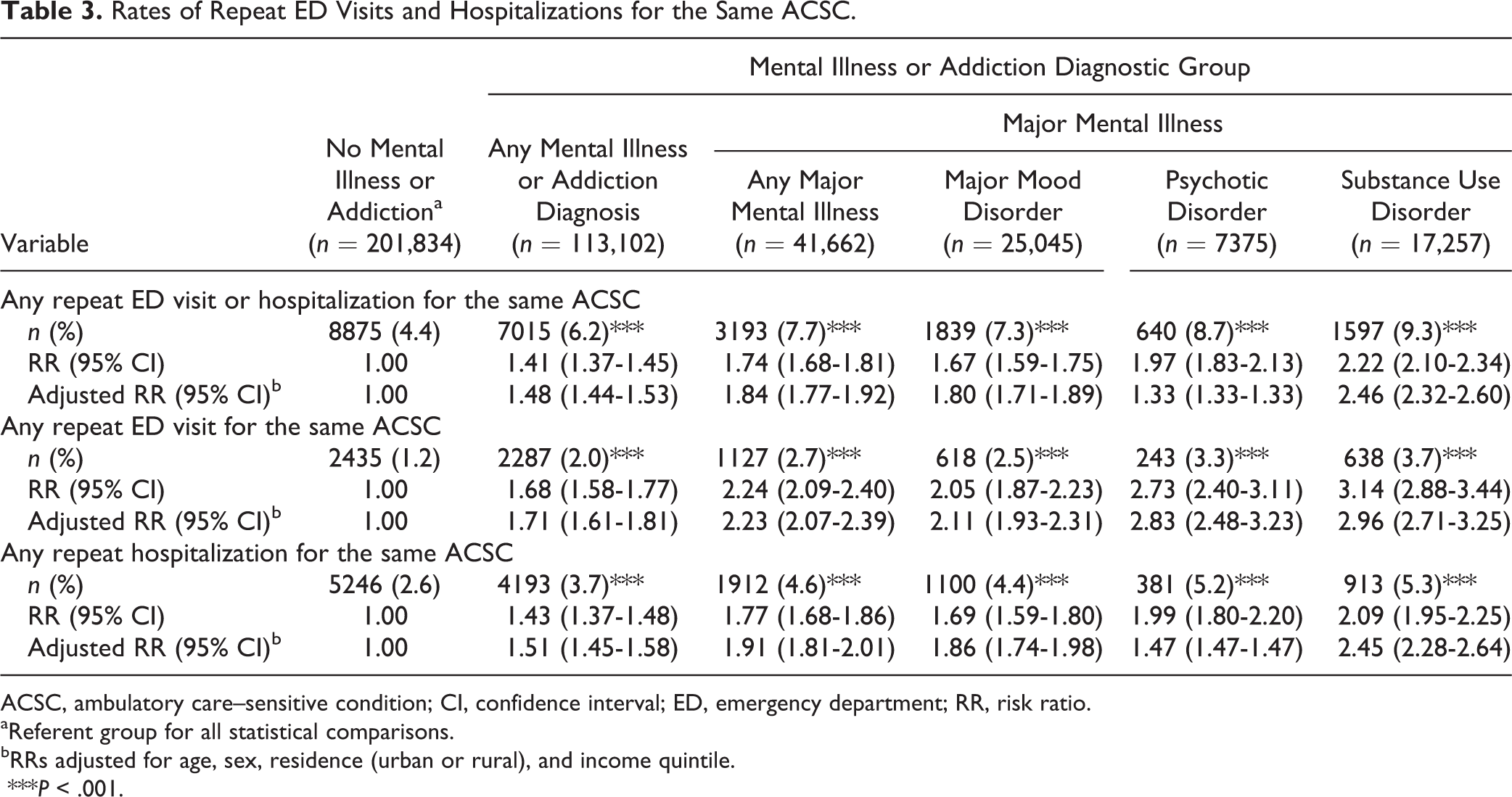
ACSC, ambulatory care–sensitive condition; CI, confidence interval; ED, emergency department; RR, risk ratio.
aReferent group for all statistical comparisons.
bRRs adjusted for age, sex, residence (urban or rural), and income quintile.
***P < .001.
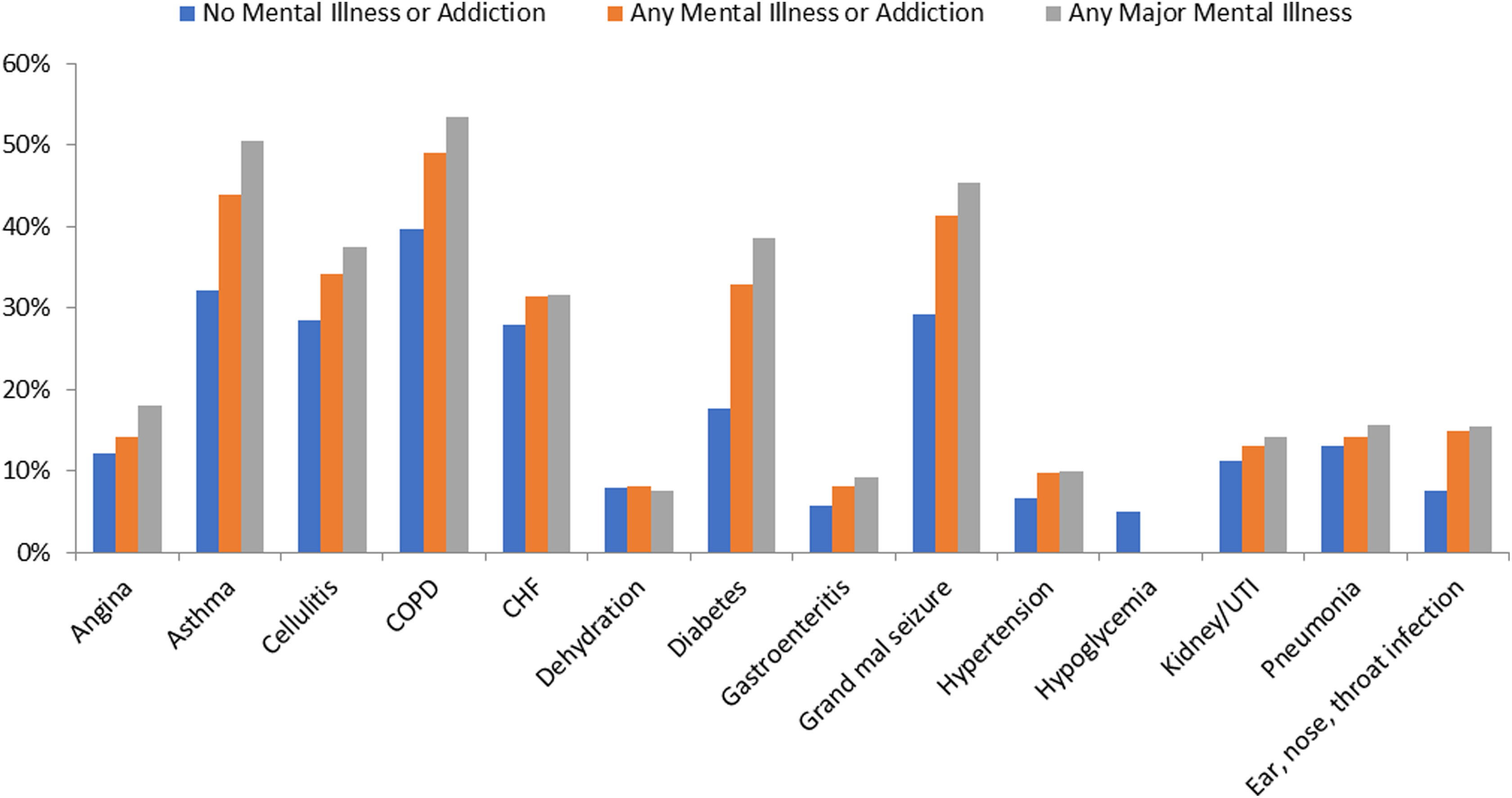
Proportion of all emergency department visits and hospitalizations that were repeat visits for the same ambulatory care–sensitive condition, by mental illness or addiction diagnostic subgroup. CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; UTI, urinary tract infection.
Discussion
This study examined acute care use for ACSCs among the top 10% of users of medical care in Ontario ranked by cost, comparing those with and without comorbid mental illness and/or addiction. The rate of mental illness and addiction in this group (35.9%) is notable, relative to the rate among nonusers of medical care during the same time period that we have reported previously (21.3%). 3 In this study, we found that individuals with mental illness and addiction, particularly those with psychotic and substance use disorders, had a higher risk for acute care use for ACSCs compared to the no mental illness group. Mental illness and addiction was also associated with up to a 3-fold increase in the rate of repeat ED visits and hospitalization for the same ACSC within the index year. Although more severe medical illness profiles might explain this, Charlson comorbidities and ADG scores were not highly different between groups. This finding of increased repeat care use may represent a particularly important target for improved community care to reduce potentially avoidable acute care use.
The findings of this study are consistent with other work demonstrating an association between mental illness and addiction and acute care use for ACSCs. 13 –18 Using New York State data, Li et al. 14 reported that those with comorbid mental illness were 2.3 times more likely than those without to have an ACSC hospitalization relative to non-ACSC admissions. Mai et al. 15 reported similar findings in a population-level study with case matching from Australia. Similar to our findings, both studies reported this association to be even stronger for major mental illness. 14,15 In a study of hospitalizations in the United States, schizophrenia was associated with an increased rate of hospitalization for ACSCs noted to be driven specifically by hospitalizations for asthma, COPD, and diabetes. 18 We also found these conditions to be more frequently associated with hospitalization, specifically repeat care use, among individuals with mental illness comorbidity. We found higher overall acute care use for ACSCs relative to studies in primary care patients 11 or population studies, 15 likely reflecting the more medically unwell cohort we used. Our risk ratios for any ACSC care use were higher than a Veterans Affairs study of primary care patients 11 but lower than those reported in samples from Australia 15 and the United States. 14 However, in contrast to the latter studies where rates of hospitalization for any reason were similarly increased in the mental illness group, we focussed on a cohort where nearly all participants had at least 1 hospital admission. To our knowledge, no studies have examined repeat care use for the same ACSCs. Our focus on the highest medical care users likely represents the individuals with the most serious medical issues and mental illness, which would amplify the impact of this comorbidity on disease management and care utilization.
What is novel in our study is that we observed this association between mental illness and ACSC care utilization in a subset of the population who are the highest-costing users of medical care, after mental health costs were excluded. This pattern is similar to what has been found in other health systems, including the United States and Australia, suggesting these disparities occur irrespective of health system organization and funding. We also showed that this finding persists for repeat visits for the same ACSC. Since ACSCs are often amenable to high-quality community care that should prevent unnecessary acute care use, 6,9,10 repeated acute care use for the same condition may represent a lack of access to such care, failure of the patient to engage well with available services, or ineffective services. Lack of access to consistent primary care has been noted to be more prevalent among those with mental illness. 32 Some literature suggests that integrated models with mental health teams can lead to improved medical outcomes. 33 Opportunities for improved care after an ED visit or hospitalization for an ACSC may be present, particularly if patients are accessing care from or can be connected to mental health professionals who might be able to support the medical issues through improved care coordination, supervision of medications and other treatments, or accompaniment to appointments.
A limitation of this study is that a diagnosis of mental illness or addiction relied on a health care visit captured in the administrative database in the 2 years prior to the observation year for medical care utilization. This likely represents an underestimation of prevalence as care may be accessed exclusively from nonphysician providers, particularly for less serious mental health issues. In addition, mental health diagnoses can change over time, which would translate to some individuals being misclassified as both having and not having a mental illness as of the index date. The major mental illness categories we looked at (with the exception of substance use disorders) are more often persistent illnesses and more likely to be associated with some physician contact. These limitations result in some uncertainty about the true effect size of the results. We looked at ED visits and hospitalizations both separately and combined to get a more robust analysis of repeat care use for the same conditions. Hospitalizations likely represent more serious presentations but also offer a longer period of time for stabilization and postdischarge care planning. Finally, our study looked at a single year of care utilization in the highest-costing users of medical care, which does not provide more longitudinal analysis of health care use patterns in these groups or comparison to lower-costing users.
This study adds to the literature characterizing high-cost users with mental illness and addiction comorbidity. The presence of this comorbidity increases medical costs through a range of mechanisms, some modifiable, such as access to care, and others that may not be as readily predictable or preventable, such as illness interactions, socioeconomic determinants of health, and behavioural factors. As policy makers focus on high-cost users, coordinating strong primary and community-based specialty care for individuals with comorbid mental and medical issues is needed, including effective mental health screening and treatment initiatives, particularly where there are ACSCs that might be unmanaged or undermanaged. More study is needed in this area as the literature is variable with respect to how effective community- and primary care–based interventions are for preventing acute care use for ACSCs, 17,34 with no data specifically among those with mental illness comorbidity. This is an area needing focussed attention, 11 –13 as well as carefully planned and evaluated interventions to improve patient outcomes and experience and possibly lead to cost savings.
Footnotes
Appendix A. Detailed Description of Data Sources
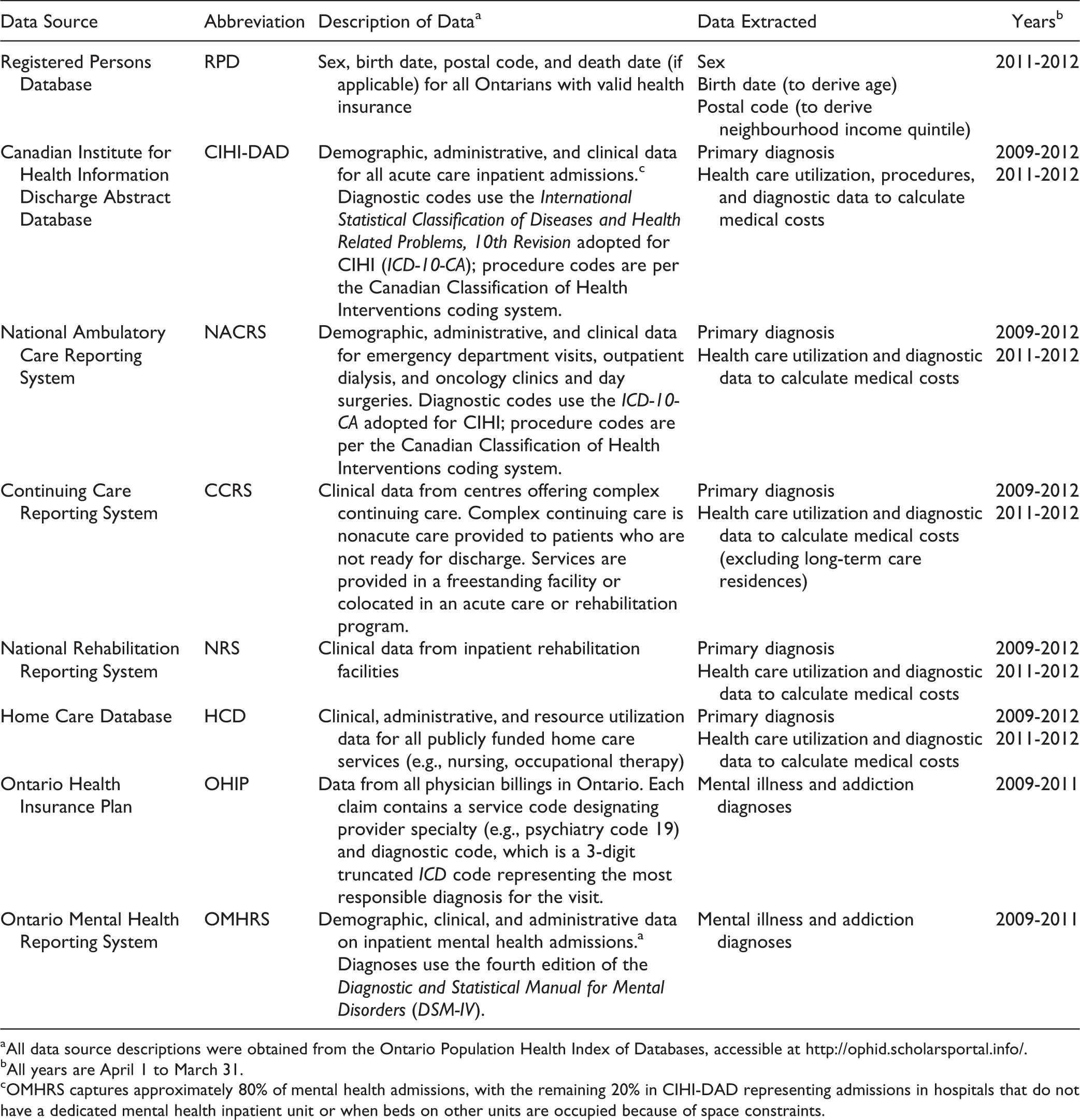
| Data Source | Abbreviation | Description of Dataa | Data Extracted | Yearsb |
|---|---|---|---|---|
| Registered Persons Database | RPD | Sex, birth date, postal code, and death date (if applicable) for all Ontarians with valid health insurance | Sex Birth date (to derive age) Postal code (to derive neighbourhood income quintile) | 2011-2012 |
| Canadian Institute for Health Information Discharge Abstract Database | CIHI-DAD | Demographic, administrative, and clinical data for all acute care inpatient admissions.c Diagnostic codes use the International Statistical Classification of Diseases and Health Related Problems, 10th Revision adopted for CIHI (ICD-10-CA); procedure codes are per the Canadian Classification of Health Interventions coding system. | Primary diagnosis Health care utilization, procedures, and diagnostic data to calculate medical costs | 2009-2012 2011-2012 |
| National Ambulatory Care Reporting System | NACRS | Demographic, administrative, and clinical data for emergency department visits, outpatient dialysis, and oncology clinics and day surgeries. Diagnostic codes use the ICD-10-CA adopted for CIHI; procedure codes are per the Canadian Classification of Health Interventions coding system. | Primary diagnosis Health care utilization and diagnostic data to calculate medical costs | 2009-2012 2011-2012 |
| Continuing Care Reporting System | CCRS | Clinical data from centres offering complex continuing care. Complex continuing care is nonacute care provided to patients who are not ready for discharge. Services are provided in a freestanding facility or colocated in an acute care or rehabilitation program. | Primary diagnosis Health care utilization and diagnostic data to calculate medical costs (excluding long-term care residences) | 2009-2012 2011-2012 |
| National Rehabilitation Reporting System | NRS | Clinical data from inpatient rehabilitation facilities | Primary diagnosis Health care utilization and diagnostic data to calculate medical costs | 2009-2012 2011-2012 |
| Home Care Database | HCD | Clinical, administrative, and resource utilization data for all publicly funded home care services (e.g., nursing, occupational therapy) | Primary diagnosis Health care utilization and diagnostic data to calculate medical costs | 2009-2012 2011-2012 |
| Ontario Health Insurance Plan | OHIP | Data from all physician billings in Ontario. Each claim contains a service code designating provider specialty (e.g., psychiatry code 19) and diagnostic code, which is a 3-digit truncated ICD code representing the most responsible diagnosis for the visit. | Mental illness and addiction diagnoses | 2009-2011 |
| Ontario Mental Health Reporting System | OMHRS | Demographic, clinical, and administrative data on inpatient mental health admissions.a Diagnoses use the fourth edition of the Diagnostic and Statistical Manual for Mental Disorders (DSM-IV). | Mental illness and addiction diagnoses | 2009-2011 |
aAll data source descriptions were obtained from the Ontario Population Health Index of Databases, accessible at http://ophid.scholarsportal.info/.
bAll years are April 1 to March 31.
cOMHRS captures approximately 80% of mental health admissions, with the remaining 20% in CIHI-DAD representing admissions in hospitals that do not have a dedicated mental health inpatient unit or when beds on other units are occupied because of space constraints.
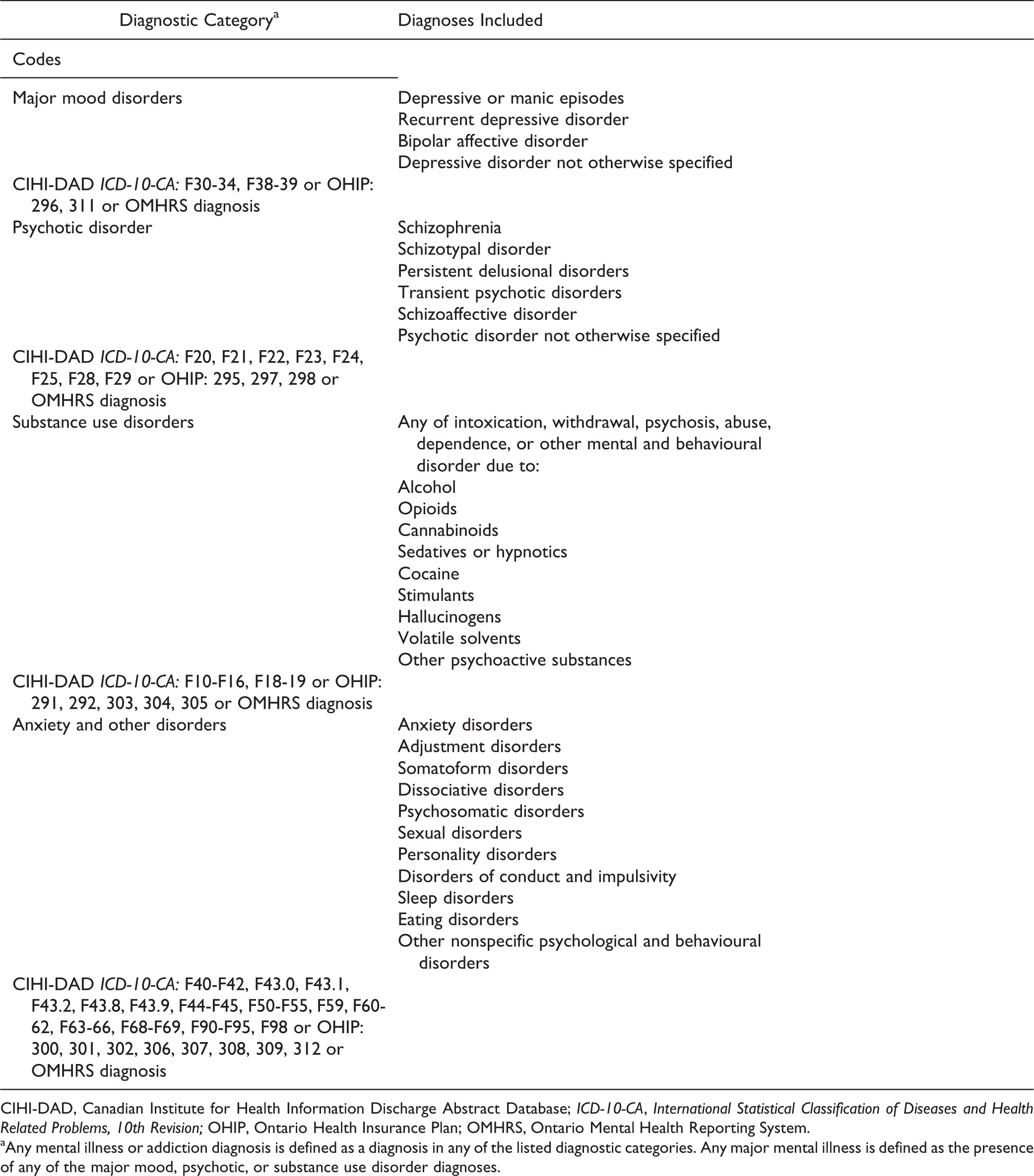
Appendix B. Detailed List of Diagnoses and Data Codes Used to Define Mental Illness and Addiction Comorbidity
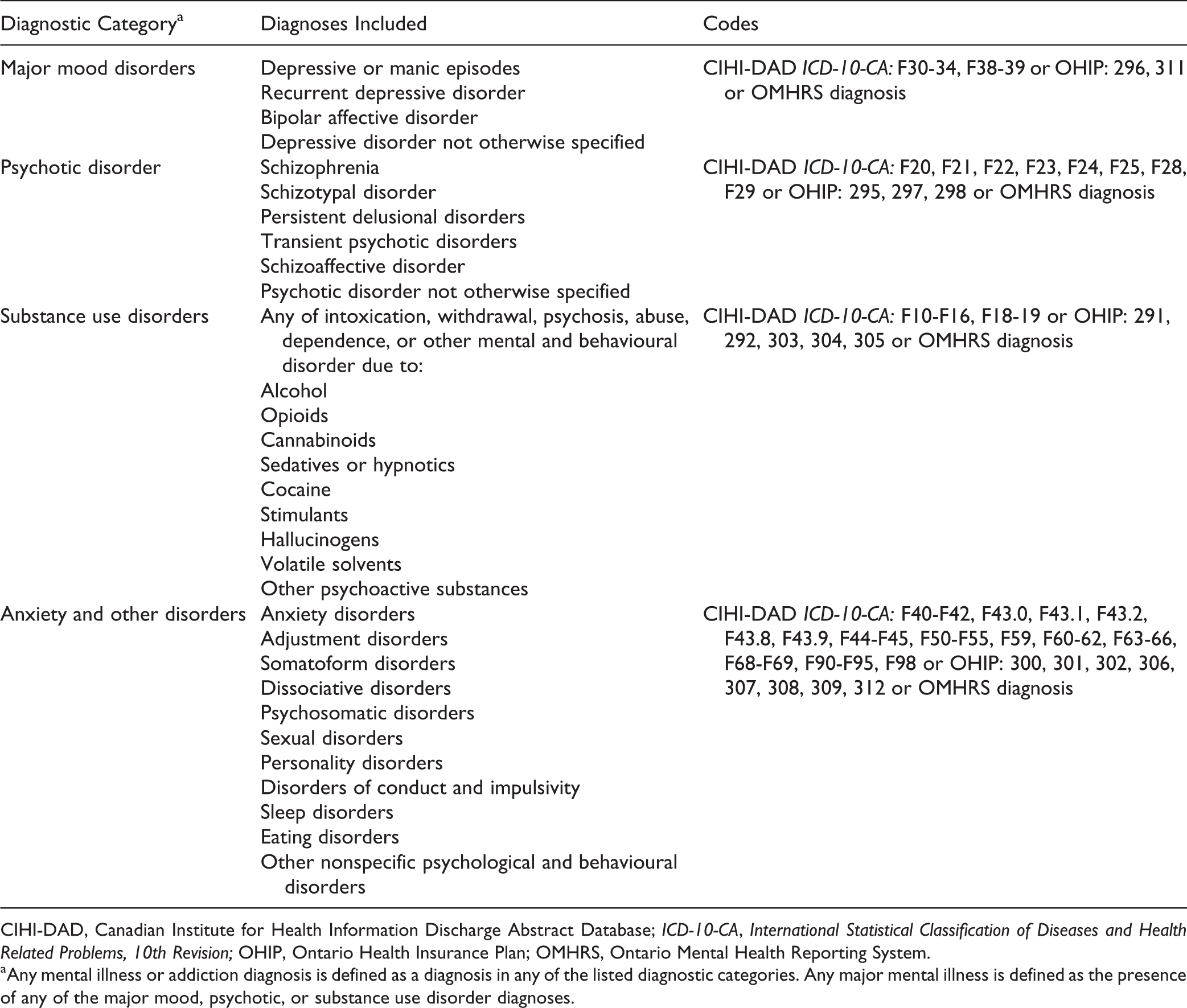
| Diagnostic Categorya | Diagnoses Included | Codes |
|---|---|---|
| Major mood disorders | Depressive or manic episodes Recurrent depressive disorder Bipolar affective disorder Depressive disorder not otherwise specified | CIHI-DAD ICD-10-CA: F30-34, F38-39 or OHIP: 296, 311 or OMHRS diagnosis |
| Psychotic disorder | Schizophrenia Schizotypal disorder Persistent delusional disorders Transient psychotic disorders Schizoaffective disorder Psychotic disorder not otherwise specified | CIHI-DAD ICD-10-CA: F20, F21, F22, F23, F24, F25, F28, F29 or OHIP: 295, 297, 298 or OMHRS diagnosis |
| Substance use disorders | Any of intoxication, withdrawal, psychosis, abuse, dependence, or other mental and behavioural disorder due to: Alcohol Opioids Cannabinoids Sedatives or hypnotics Cocaine Stimulants Hallucinogens Volatile solvents Other psychoactive substances | CIHI-DAD ICD-10-CA: F10-F16, F18-19 or OHIP: 291, 292, 303, 304, 305 or OMHRS diagnosis |
| Anxiety and other disorders | Anxiety disorders Adjustment disorders Somatoform disorders Dissociative disorders Psychosomatic disorders Sexual disorders Personality disorders Disorders of conduct and impulsivity Sleep disorders Eating disorders Other nonspecific psychological and behavioural disorders | CIHI-DAD ICD-10-CA: F40-F42, F43.0, F43.1, F43.2, F43.8, F43.9, F44-F45, F50-F55, F59, F60-62, F63-66, F68-F69, F90-F95, F98 or OHIP: 300, 301, 302, 306, 307, 308, 309, 312 or OMHRS diagnosis |
CIHI-DAD, Canadian Institute for Health Information Discharge Abstract Database; ICD-10-CA, International Statistical Classification of Diseases and Health Related Problems, 10th Revision; OHIP, Ontario Health Insurance Plan; OMHRS, Ontario Mental Health Reporting System.
aAny mental illness or addiction diagnosis is defined as a diagnosis in any of the listed diagnostic categories. Any major mental illness is defined as the presence of any of the major mood, psychotic, or substance use disorder diagnoses.
Access to Data Statement
The data used in this study were obtained from data sets that were linked using unique encoded identifiers and analyzed at the Institute for Clinical Evaluative Sciences (ICES). Kinwah Fung is affiliated with the Institute of Clinical Evaluative Sciences and had full access to all the data in the study. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the author, and not necessarily those of CIHI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No external funding was received for this study. It was supported in-kind by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.