
Abstract
Objective:
Prior year medical care was compared among youth dying by suicide to their peers. Effect modification of these associations by age or place of residency (rural versus larger community sizes) was examined in a large, medically insured population.
Method:
This population-based case control study used data from the Office of the Chief Coroner in Ontario, Canada, linked to health care administrative data to examine associations between medical care for mental health or other reasons (versus no medical care) and suicide. Decedents (n = 1203 males and n = 454 females) were youth (aged 10 to 25 years) who died by suicide in Ontario between April 2003 and March 2014, inclusive. Peers of the same ages were frequency matched to decedents on sex and place of residency. Logistic regression was used to calculate odds ratios and 95% confidence intervals and to test effect modification.
Results:
Associations with mental health care were stronger in decedents than peers with a gradation of care (i.e., outpatient only, emergency department [ED], inpatient care) in both sexes. However, these associations were weaker among youth living in rural communities. Furthermore, older males (aged 18 to 25 years) were less likely than younger males (aged 10 to 17 years) to access the ED (ambulatory care only). This decrease was observed in rural and larger communities alongside no increase in medical care for other reasons.
Conclusions:
Geographical and age-related barriers to mental health care exist for youth who die by suicide. Preventive efforts can address these barriers, intervening early and integrating services, including the ED.
Suicide is the second leading cause of death among youth worldwide with profound social and economic costs. 1 However, suicide is too rare to predict in individuals, making developmentally sequenced system-level interventions a priority, particularly in populations at excess risk. 2 –4 Known antecedents of youth suicide vary by age and sex/gender, 5 but less is known about optimal times and places to develop and evaluate promising interventions. Given most youth who die by suicide access medical care in the prior year, 6 we examine how this access differs from their peers to target promising interventions.
There is a dearth of studies comparing prior year health care contact among youth who died by suicide compared to population-based peers, 7 –9 limited by few female decedents, potential biased peer selection, and proxy reporting of mental health care contacts. 7,8 Not examining male and female youth separately is problematic given the ‘gender paradox’ (i.e., higher suicide rates in males alongside higher attempt rates in females) 10 emerging in adolescence, 5,6,11 with suicide rates at least 2 to 3 times higher in male than female youth. 1,12,13 This divergence may be explained, in part, by differences in their interactions with the health care system. 14 Previous research has shown that, arising from greater need, those who died by suicide accessed mental health care more often than peers. 7 –9,15 –17 However, it is unclear whether age modifies these associations in keeping with the age-dependent gender paradox. Furthermore, place of residency may modify these associations. In rural communities, accessing mental health care is compromised by a lower supply of mental health providers 18 despite higher suicide rates. 19,20
We anticipate the association between suicide and prior mental health care will diminish with age, particularly in males, and that this may be accompanied by a compensatory age-related increase in emergency department (ED) contact for other reasons. Evidence from the US general population reveals that between adolescence and adulthood, primary care contact increases in females (but decreases in males), whereas ED contact increases in males. 21 We anticipate the association between suicide and prior mental health care will be weaker among youth living in rural versus larger communities. Furthermore, given the prominent role of EDs in ambulatory medical care in rural communities, 22 we expect that decedents compared to peers in these areas will access mental health care in the ED more often than when compared to either no medical care or to outpatient mental health care alone. Accordingly, we conducted a large, population-based case control study in Ontario, Canada, employing individually linked health care administrative records to assess the strength of the associations between suicide and prior medical care (for mental health or other reasons) in male and female youth and to determine whether these associations are modified by age or place of residency (rural versus larger community sizes).
Method
Study Sample and Data Collection
This study extends on a prior one 6 by adding more years and, therefore, decedents and by including population-based controls, all identified within the Registered Persons Data Base (RPDB). The RPDB contains unique encrypted identifiers issued to individuals insured through Ontario’s public health care system. 23 Decedents were youth (ages 10 to 25 years) who died by suicide in Ontario, Canada, between April 2003 and March 2014, inclusive. These data were accessed from the Office of the Chief Coroner (OCC) through a data-sharing agreement between the OCC and the Institute for Clinical Evaluative Sciences (ICES) with strict privacy procedures. Death records were securely abstracted from OCC electronic and decedent files and transmitted to ICES for probabilistic linkage to the RPDB. Through the unique identifiers, decedents were individually linked to their administrative health care records in the year prior to their death. 6
Decedents and peers were stratified according to their sex (male or female) and study year. Within each of these strata, potential peers were randomly assigned decedent death dates in that year and all those alive and aged 10 to 25 were retained, capturing the full population base. Place of residency was then determined in the year prior with peers’ frequency matched to decedents on community size: rural (population < 10,000) or larger (population ≥ 10,000). Frequency matching was chosen to optimize the number of decedents and peers per stratum and to permit the assessment of effect modification with matching variables (not possible with 1:1 matching).
As with the decedents, unique encrypted identifiers in the RPDB were used to link peers to their corresponding administrative health care records at ICES. Project-specific data files were then created and stripped of identifying information for analyses at ICES.
This study was approved by the Hamilton Integrated Research Ethics Board and the Health Canada and Public Health Agency of Canada’s Research Ethics Board.
Study Measures
Age and sex were identified in the RPDB. Prior year medical care contact was defined as any mental health care 18 (including any outpatient medical, ED, and inpatient), other medical care (i.e., all other outpatient medical, ED, or inpatient care), or no medical care. Outpatient mental health care was categorized by physician specialty: psychiatrist or another specialty. Mutually exclusive levels of medical care (vs. no medical care) were defined hierarchically first, according to setting: outpatient medical only, ED (but no inpatient contact) or inpatient, and then, at the highest level, the reason: mental health 18 or other. Thus, youth accessing inpatient mental health care may have also accessed inpatient or ambulatory care for other reasons. Youth accessing inpatient care for other reasons did not access mental health care at this level but may have at lower levels. Community size (rural vs. larger) was defined using postal code information contained in the RPDB and according to Statistics Canada recommended definitions. 24
Statistical Analyses
To examine the strength of associations, we compared the number and proportion of decedents and peers according to their medical care (by reason, outpatient psychiatric care, and level by reason) classified by residency and separately in male and female youth. Multiple logistic regression was used to calculate odds ratios (ORs) by decedent (vs. peer) status and corresponding 95% confidence intervals (CIs), adjusted for age (14 to 15,16 to 17, 18 to 19, 20 to 25 vs. 10 to 13) within these strata. Changes in the magnitude of the associations after age adjustments were assessed along with a possible gradation in associations by comparing successive levels of care (i.e., outpatient only, ED but no inpatient, and then inpatient care) to no medical care by reason. Post hoc sex differences were described.
To assess effect modification, we tested whether age and community size modified the associations between decedent status and level of care by reason separately in male and female youth. Age was dichotomized as 18 to 25 versus 10 to 17, in keeping with transitions between youth and adult care systems in Ontario. Deviance statistics from multiple logistic regression models incorporating 2- and 3-way interactions between decedent status, age, and community size were compared to successive baseline models. ORs and corresponding 95% CIs were then reported, according to best model fit.
Results
A total of 1657 youth (n = 1203 males and n = 454 females) who died by suicide were successfully linked (94%) to their health care records (Table 1). As per the frequency matching, the proportion of peers was the same as the decedents within each year for male and female youth living in rural and larger communities. About one-quarter of the decedents lived in rural communities, with males outnumbering females by 2.6 times in both rural and larger communities.
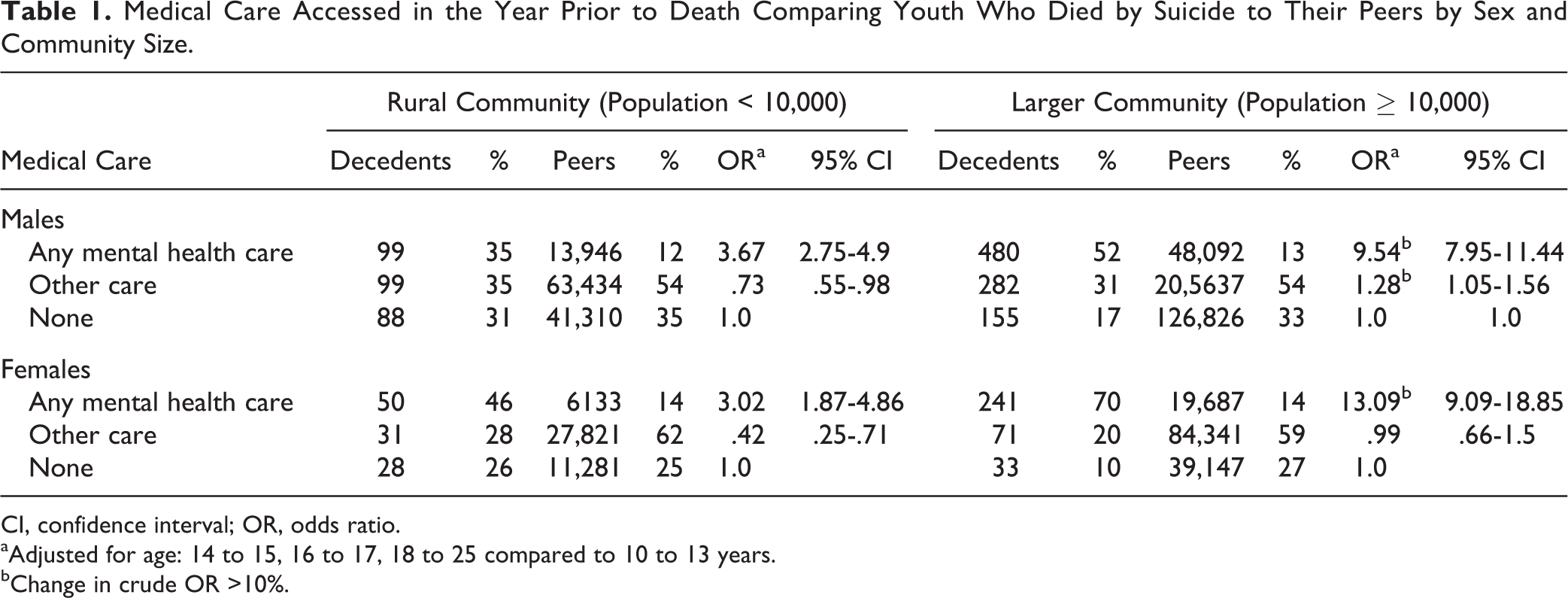
Medical Care Accessed in the Year Prior to Death Comparing Youth Who Died by Suicide to Their Peers by Sex and Community Size.
CI, confidence interval; OR, odds ratio.
aAdjusted for age: 14 to 15, 16 to 17, 18 to 25 compared to 10 to 13 years.
bChange in crude OR >10%.
Any Mental Health Care
The distribution of decedents and peers who accessed any mental health care by residency and sex is shown in Table 1. The proportion of decedents who accessed this care ranged from 35% in rural males to 70% in females living in larger communities.
The age-adjusted associations between decedent status and mental health care show decedents were significantly more likely than peers to access any mental health care compared to no medical care in the prior year (Table 1). However, these associations were significantly weaker among rural youth than those living in larger communities, in both sexes. Furthermore, the difference between rural males and females living in larger communities was also statistically significant (OR, 3.67 vs. 13.09), respectively.
Outpatient Mental Health Care
Among decedents who accessed any mental health care, most accessed outpatient care: 75 of 99 (76%) rural males, 39 of 50 (78%) rural females, and 409 of 480 (85%) males and 207 of 241 (86%) females living in larger communities (numerators shown in Table 2; denominators, Table 1).
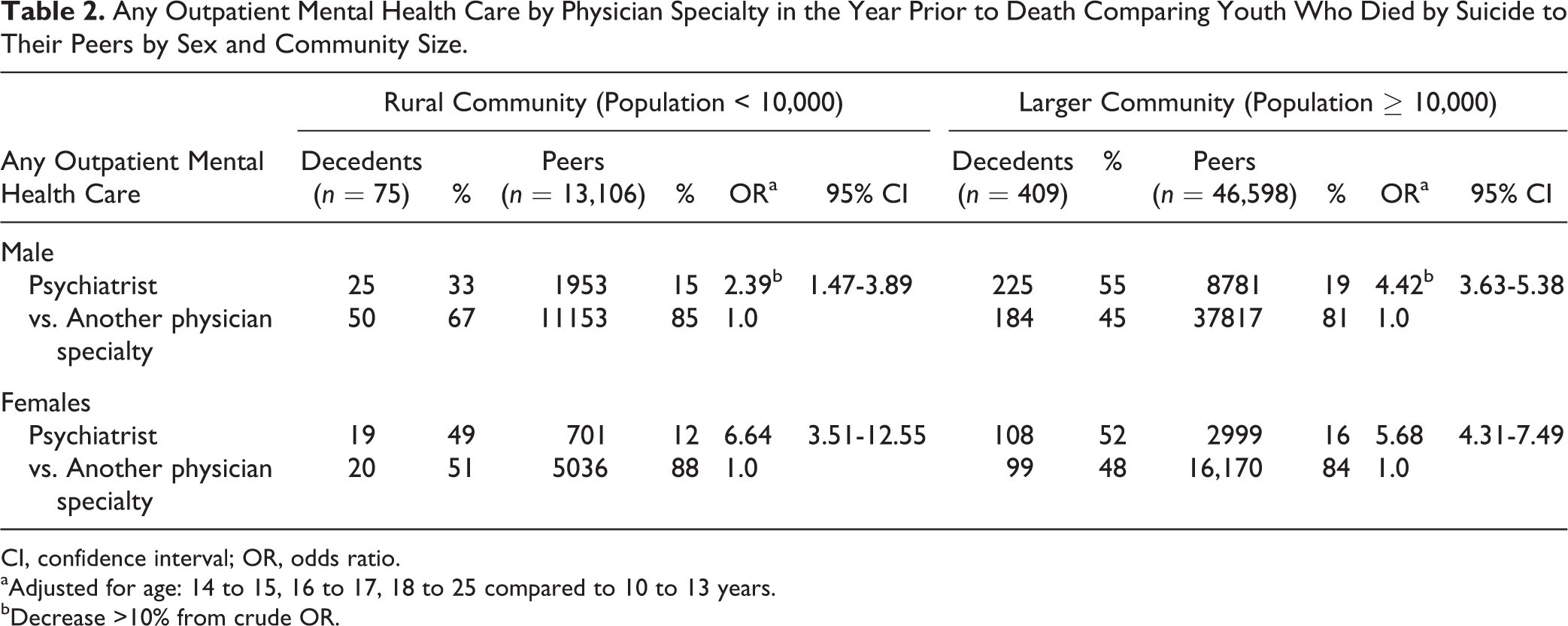
Any Outpatient Mental Health Care by Physician Specialty in the Year Prior to Death Comparing Youth Who Died by Suicide to Their Peers by Sex and Community Size.
CI, confidence interval; OR, odds ratio.
aAdjusted for age: 14 to 15, 16 to 17, 18 to 25 compared to 10 to 13 years.
bDecrease >10% from crude OR.
Among those accessing outpatient mental health care, decedents were significantly more likely than peers to be seen by a psychiatrist, among male and female youth living in rural and in larger communities (Table 2). Compared to rural males (OR, 2.39), associations were stronger for rural females (OR, 6.64) and females living in larger communities (OR, 5.68) with the latter difference statistically significant. Still, among decedents who accessed any outpatient mental health care, only one-third (rural males) to around a half (all others) saw a psychiatrist.
Level of Medical Care for Mental Health Reasons
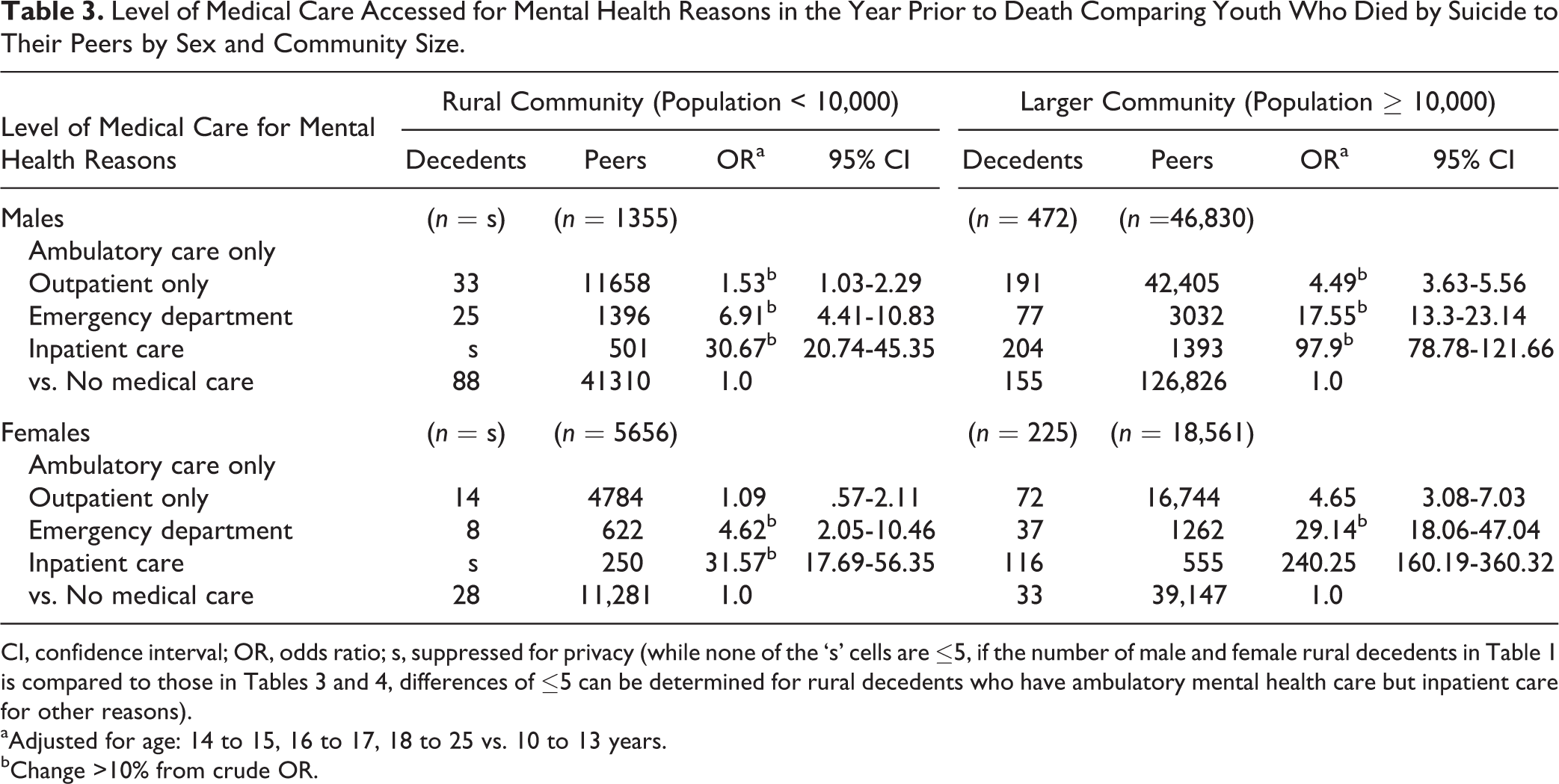
In both rural and larger communities, decedent status was significantly and positively associated with the level of care for mental health in a graded manner (Table 3). When accessing mental health care, decedents differed the most from peers on inpatient care and the least when accessing outpatient care alone. In fact, among rural males and females, decedents and peers did not differ significantly on the latter.
Level of Medical Care Accessed for Mental Health Reasons in the Year Prior to Death Comparing Youth Who Died by Suicide to Their Peers by Sex and Community Size.
CI, confidence interval; OR, odds ratio; s, suppressed for privacy (while none of the ‘s’ cells are ≤5, if the number of male and female rural decedents in Table 1 is compared to those in Tables 3 and 4, differences of ≤5 can be determined for rural decedents who have ambulatory mental health care but inpatient care for other reasons).
aAdjusted for age: 14 to 15, 16 to 17, 18 to 25 vs. 10 to 13 years.
bChange >10% from crude OR.
Nevertheless, this gradation of associations was weaker among male and female youth living in rural than larger communities. For example, the corresponding age-adjusted ORs for outpatient care alone and the ED were 1.53 versus 6.91 for rural males and 4.49 versus 17.55 for males living in larger communities, respectively.
Level of Medical Care for Other Reasons
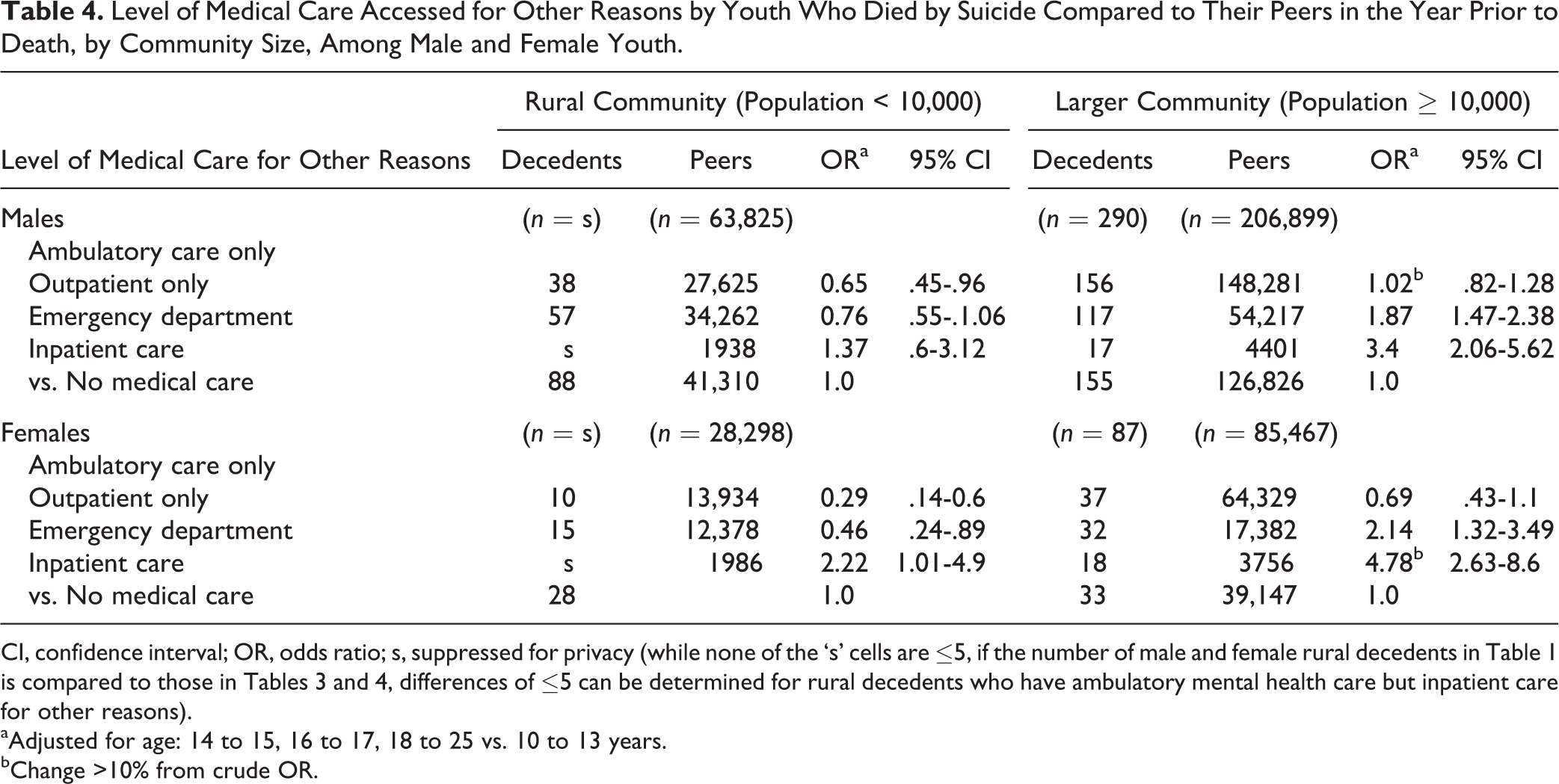
When levels of medical care for other reasons were examined (Table 4), among rural youth, decedents were less likely than peers to access outpatient medical care alone. Among male and female youth living in larger communities, decedents were more likely than peers to access ambulatory ED and inpatient care compared to no medical care.
Level of Medical Care Accessed for Other Reasons by Youth Who Died by Suicide Compared to Their Peers in the Year Prior to Death, by Community Size, Among Male and Female Youth.
CI, confidence interval; OR, odds ratio; s, suppressed for privacy (while none of the ‘s’ cells are ≤5, if the number of male and female rural decedents in Table 1 is compared to those in Tables 3 and 4, differences of ≤5 can be determined for rural decedents who have ambulatory mental health care but inpatient care for other reasons).
aAdjusted for age: 14 to 15, 16 to 17, 18 to 25 vs. 10 to 13 years.
bChange >10% from crude OR.
Level of Medical Care by Community Size and Age
Consistent with the findings regarding levels of medical care for mental health reasons (Table 3) and for other reasons (Table 4), community size interacted with decedent status, contributing significantly to deviances between all such models examining level of care associations by sex. However, in only one comparison did age significantly modify level of care associations (Figure 1, model 3). Among males who did not access inpatient care, the positive association between decedents being more likely than peers to access the ED for mental health reasons differed by age. Specifically, this association was significantly lower in older than younger males by almost 50% regardless of where male youth lived.
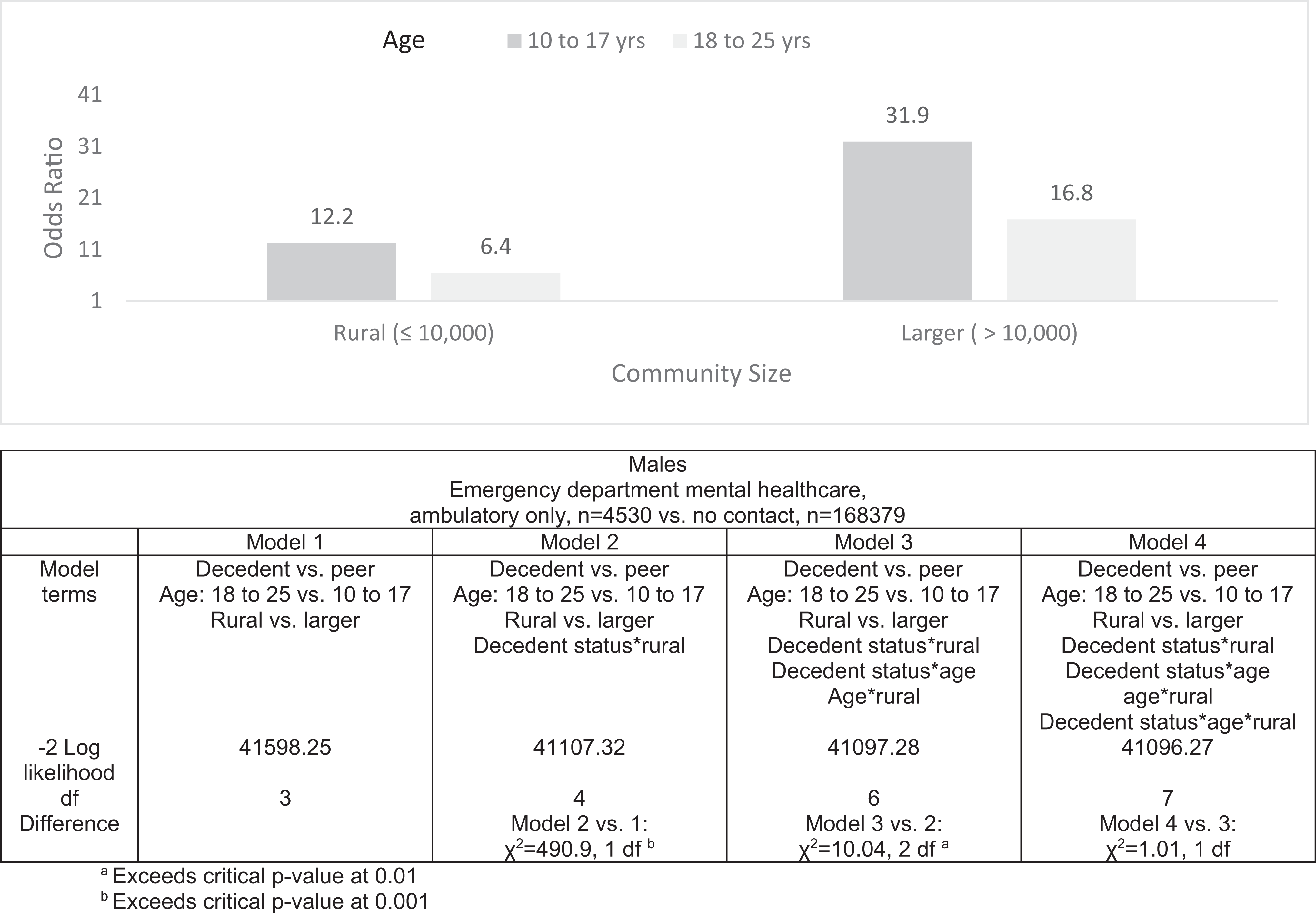
The association between decedent status and prior year emergency department mental health care, ambulatory only, by age, among male youth. aExceeds critical P value at 0.01. bExceeds critical P value at 0.001.
Discussion
To our knowledge, this is the largest population-based case control study of mental health care and other medical care accessed in the year before youth died by suicide.
As hypothesized, decedents were more likely than their peers to access any mental health care with these positive associations weaker among male and female youth living in rural versus larger communities.
With respect to levels of care, among youth (both sexes) living in rural communities, decedents were more likely than peers to access the ED for mental health reasons (regardless of their outpatient care but not be admitted) than either to access outpatient mental health care alone or to have no medical care. This pattern extended to youth (both sexes) living in larger communities as well. In fact, associations with medical care for mental health reasons followed a graded pattern, with significant positive associations becoming stronger at each successive level. Consistent with findings regarding any mental health care, this gradation was also weaker among male and female youth living in rural compared to larger communities. Furthermore, among male and female youth who accessed medical care for other reasons, decedents were more likely than peers to access ED and/or inpatient care (than no medical care) when youth lived in larger communities.
For the most part, age did not modify access to levels of medical care for mental health or other reasons. Still, our hypothesis that positive associations with mental health care would diminish with age, particularly among male youth, received some support. Among males, the positive association with accessing ED mental health care (ambulatory only) was almost 50% lower among older (18 to 25) than younger (10 to 17 years) males, regardless of where they lived. However, there was no indication this difference was offset by an increase in the use of medical care for other reasons.
Limitations
Outpatient mental health care is confined to physicians who bill (or shadow bill) the Ontario Health Insurance Plan (OHIP). Contacts with providers paid through other means, such as psychologists, are excluded. 6,25 Thus, outpatient mental health care is underascertained with unclear effects. 7,8,15 –17 This study was not designed to examine clinical severity, community-level resources (e.g., the supply and distribution of providers), or the quality of prior care. In rural communities, it is challenging to recruit and retain specialists who tend to concentrate in urban centres. 26,27 Suicide deaths are likely underreported, 11 and sparse cells may have limited detection of significant differences (e.g., 3-way interactions). Multiple comparisons may account for some findings. The findings need replication in other jurisdictions and larger populations. Associations with care may have changed over time (e.g., a decrease among younger females after the regulatory warnings against antidepressant prescribing). 28,29
Interpretation
The universal medical care coverage, size, prospective nature, and linkage capabilities make this study unique. It is disheartening, then, that only 53% of youth who died by suicide accessed any such mental health care in the year before their death—two-thirds of females living in larger communities, double that of rural males. Previous studies of youth who died by suicide suggest almost all of these youth would have had 1 or more mental illnesses amenable to treatment. 5 In Ontario, physicians are responsible for diagnostic and medication monitoring and admission and discharge from hospitals. 30 Collectively, such estimates 6,31 along with audits conducted in Canadian studies 32,33 accentuate deficiencies in recognizing and treating mental illness among these youth. In uninsured populations, the picture may be worse.
Among rural youth, the weaker associations found at each level of mental health care suggest inadequacies in the availability and uptake of services in these settings. Few have studied how contextual factors (e.g., provider supply or distribution) alter mental health care access and suicide rates. One ecological study in England (all ages), among those already in contact with mental health care, found the implementation of service recommendations (e.g., 24-hour crisis teams, policies around substance misuse, and transfer of youth to adult care), along with lower rates of nonmedical staff turnover, was associated with suicide rate reductions. 34,35
This study found youth who died by suicide were much more likely than their peers to be seen in the ED and/or inpatient settings for mental health care (and for other medical reasons among youth living in larger communities). The magnitude of these associations is noteworthy: the lowest age-adjusted odds ratio was 4.62 (95% CI, 2.05-10.46) for ED mental health care (ambulatory only) among rural females. Furthermore, 48% of youth who died by suicide were seen in the ED and/or inpatient setting for any reason in the year before their death (32% for mental health and 16% for other reasons only, numerators: Tables 3 and 4). Taken together, these findings underscore the integral role hospital settings can play in accessing mental health care among male and female youth in the year before suicide. Because these contacts are not usually their last medical care contact and for males, often not within 30 days of their death, 6 hospital settings have an important window in which to intervene.
A pressing problem, though, is how to best identify youth at risk for suicide and intervene effectively in these settings. Only a small portion presenting to hospital would die by suicide in the subsequent year. Accordingly, clinical trials have targeted suicidal ideation, attempts, or self-harm (irrespective of intent). Suicide attempts and ED presentations for self-harm are strongly associated with suicide in male and female youth. 36 –39 Critical work underscores that the most promising interventions are not ED based alone but rather ‘transition’ ones, initiated in the ED and inpatient unit and extended postdischarge into the community. 40 –42 Interventions showing an effect tended to target family interactions or nonfamilial support 41 and substance use. 43 Still, in most of these trials, females predominated over males 44 likely due to their higher prevalence of suicidal ideation, attempts, and self-harm. 5,45 This may be, in part, a detection problem. One ED-based study found that among youth presenting with mental health problems, over half who screened positive for suicidal ideation did not present with a suicide-related chief complaint. These youth tended to be older, be male, and have externalizing 46 disorders, more common among suicides in male than female youth. 5
The decrease in the positive association with ED mental health care (ambulatory care only) as male youth aged has at least two implications for clinical care. First, this difference may represent developmental transitions. Compared to older youth, those younger likely receive greater supervision from family members and in school, which may translate into improved chances of securing mental health care. 47 Also at age 18, while OHIP coverage continues, youth become ineligible for children’s mental health care, 48 endangering continuity of care. 49 Thus, ongoing integration of their care and outreach (e.g., via mobile teams, technology-enhanced interventions, 50 and formal transfer of care policies 35 ) seem key to prevention efforts. Second, if this decrease in ED care is specific to male youth, signaling unmet need, then targeting developmentally sensitive, sex/gender differences in the antecedents of suicidal behaviours seems paramount. 5 In particular, externalizing disorders may need better detection and appropriate treatment to prevent later substance misuse, isolation, and suicide. 5
Conclusions
This study underscores rural disparities in mental health care despite medical insurance. It also reinforces the ED as an advantageous place to develop and evaluate preventive interventions. 2,51,52 Moreover, it points to the need for early intervention (i.e., among youth aged 10 to 17 years) and integrated services to facilitate ongoing engagement in care. Finally, it demonstrates the feasibility and value of data system linkages, increasingly used for advancing youth suicide prevention. 53 Additional research is needed to better understand how multilevel resources (i.e., community, family, individual) alter mental health care contacts with different types of settings and/or providers and suicide rates over time. To successfully prevent youth suicide, a much stronger, developmentally sensitive, well-coordinated response is needed. 54
Footnotes
Acknowledgements
We thank Dr. James Edwards, Andrew Stephen, and the staff at the Office of the Chief Coroner of Ontario for making this research possible. Parts of this material are based on data and information compiled and provided by the Canadian Institute of Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of CIHI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the Canadian Institute of Health Research (CIHR) in the form of an Operating Grant. CIHR had no direct or indirect involvement in the completion of the study or analysis of results. This project was also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results, and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.