
Abstract

Keywords
Introduction
Canada legalized recreational cannabis on October 17, 2018. Since then, only one Canadian study (in Quebec) examined the impact of legalization on cannabis-related hospitalizations. 1 That study focused on youth (0–19) using 5.5 months of post-legalization data, which precluded understanding the impact on trends over a longer period after legalization. While a number of recent studies have examined the impact of legalization on cannabis-related emergency department (ED) visits in Canada,2,3 cannabis-related hospitalizations should not be ignored since substance-related in-patient care is required in the most severe spectrum of cases and they contribute to significant healthcare costs. 4
The multi-phased approach of cannabis legalization in Ontario provides an opportunity to examine the impact of the different phases of cannabis sales regulation on cannabis-related hospitalizations. The Ontario legal cannabis availability approach involves a hybrid model of government operated online sales and licensed private retail stores. 5 Implementation of the model was phased, with Phase 1 of legalization (October 2018-March 2020) associated with flower and herb sales online and limited private retail storefronts; Phase 2 involved increased storefronts and availability of edibles (Mar 2020-May 2021). The aim of this study is to investigate the association between Phase 1 and 2 of legalization and cannabis-related hospitalizations in Ontario.
Methods
The study cohort (n = 12,079,699) includes all adults aged 18 + in Ontario eligible for the Ontario Health Insurance Plan (OHIP) as of October 17, 2015, using data held at ICES (formerly known as The Institute for Clinical Evaluative Sciences). All individuals were followed-up using healthcare records until May 2021. To be included, individuals must have continuous OHIP coverage and residency in Ontario for the entire study period. Age groups for our study were based on each person's age on the day of Canada's cannabis legalization. Cannabis-related hospitalizations (ICD-10-CA: F12, T40.7) between October 2015 and May 2021 were identified using the Discharge Abstract Database (DAD) and the Ontario Mental Health Reporting System (OMHRS). This method for using these specific ICD-10-CA codes to identify cannabis-related acute care is well supported (Supplementary Table 1). Positive cases were identified using the primary and non-primary diagnoses in each database. We compared trends and characteristics of the hospitalizations over three periods: pre-legalization, Phase 1, and Phase 2. Negative binomial segmented regressions were used to estimate the incidence rate ratios (IRRs) for immediate and trend changes associated with each of the 3 periods in the monthly counts of hospitalizations, examining effects of age and gender identity. Similar to prior studies, we included an indicator variable for March and April 2020 to adjust for the early COVID-19 effects. 2 Ethics approval for this study was obtained through Brock University (REB 20-134-CHUM).
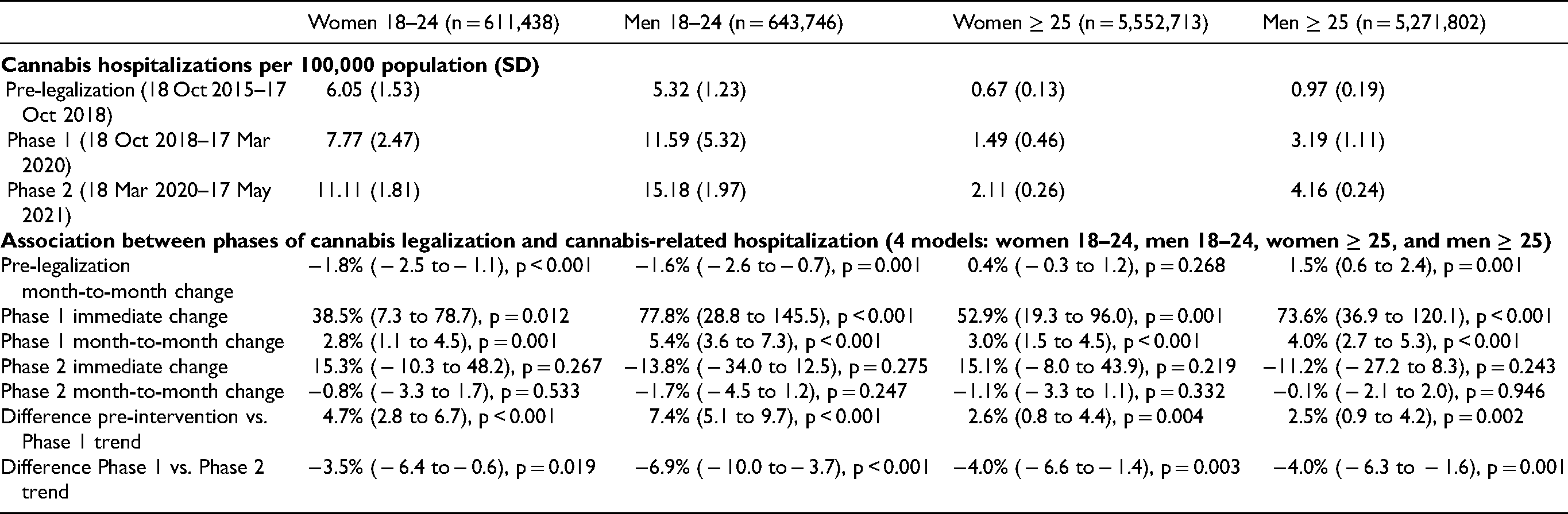
Cannabis-Related Hospitalizations Rates per 100,000 Population, and Association Between Phases of Legalization and cannabis-Related Hospitalization (Estimated from Negative Binomial Segmented Regression) with Estimated Incidence Rate Ratio for all Adults and Young Adults by Gender.
Results
Harmful use (F12.1) and dependence syndrome (F12.2) were the most common cannabis-related diagnoses accounting for 41% and 39% of hospitalizations respectively (Supplementary Table 2). Table 1 shows the rate of hospitalization per 100,000 population, and adults aged 18–24 have higher rates of hospitalization compared to adults aged 25 + across all three study phases. The monthly hospitalization rates across all four groups are presented in Supplementary Figure 1. Based on regression models, prior to legalization, significant month-to-month decreases were seen in women 18–24 at 1.6% per month (95% CI − 2.6, − 0.7%) and men aged 18–24 at 1.8% per month (95% CI − 2.5, − 1.1%); however, the incidence rate ratio increased by 1.5% per month for men 25 + (95% 0.6, 2.4%). Phase 1 was associated with a significant immediate and month-to-month increase in hospitalization across all age and gender subgroups, with greater increases in men than women. Immediate increases ranged from 38.5% in women 18–24 (95% CI 7.3%, 78.7%) to 77.8% in men 18–24 (95% CI 28.8, 245.5%). The month-to-month increases ranged from 2.8% per month in women 18–24 (95% CI 1.1, 4.5%) to 5.4% per month in men 18–24 (95% CI 3.6–7.3%). Phase 2 was not associated with immediate increases in hospitalization in both adults 18–24 and 25 + . Moreover, the month-to-month trend in each subgroup was stabilized by Phase 2.
Discussion
The initial cannabis legalization (Phase 1) led to immediate and trend increases in cannabis-related hospitalization across adults 18–24 and 25 + . As a result of Phase 1 legalization, the increases (combining immediate and monthly change) ranged from 103% for women 18–24 and up to 235% for women 18–24, which are clinically significant. These increases were greater for men than women, regardless of age groups. No further increases were associated with the introduction of edibles and the expansions of retail stores (Phase 2). While a prior study on the effects of cannabis legalization on hospitalization in youths found a 30.7% increase only among boys 10–14, 1 our study (focused on adults) found significant immediate increases for all adults, with stronger immediate and trend effects shown in men versus women; and among women, stronger effects in women 25 + vs. 18–24. In another prior study, cannabis-related ED visits increased in both phases, 2 however, our study found significant increases in hospitalizations only after initial legalization. Our study is limited by other concurrent interventions, and effects of the introduction of edibles are not distinguishable from the COVID-19 pandemic. The reporting of cannabis-related hospitalizations may have changed over time (e.g. increased clinician awareness after legalization), which may bias our results towards a significant finding for Phase 1 effects. Using the primary and non-primary diagnoses to identify cannabis-related hospitalizations may have led to over- or under-estimation. Our study found that the initial legalization was followed by clinically significant increases in cannabis-related hospitalizations; however, the subsequent increase in retail stores, availability of cannabis edibles, and COVID-19 pandemic was not associated with a further increase in hospitalizations in Ontario.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437221114785 - Supplemental material for Cannabis Legalization and cannabis-Related Hospitalizations in Ontario, Canada
Supplemental material, sj-docx-1-cpa-10.1177_07067437221114785 for Cannabis Legalization and cannabis-Related Hospitalizations in Ontario, Canada by Chungah Kim, Antony Chum, Andrew Nielsen, Frank MacMaster, Katherine Rittenbach, Sara Allin, Patricia O’Campo, Maritt Kirst and Hayley Hamilton in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
This study contracted ICES Data & Analytic Services (DAS) and used de-identified data from the ICES Data Repository, which is managed by ICES with support from its funders and partners: Canada's Strategy for Patient-Oriented Research (SPOR), the Ontario SPOR Support Unit, the Canadian Institutes of Health Research and the Government of Ontario. The opinions, results and conclusions reported are those of the authors. No endorsement by ICES or any of its funders or partners is intended or should be inferred.
Parts of this material are based on data and information compiled and provided by CIHI. However, the analyses, conclusions, opinions, and statements expressed herein are those of the author, and not necessarily those of CIHI.
Data Availability
The dataset from this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() . The full dataset creation plan and underlying analytics code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
. The full dataset creation plan and underlying analytics code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Author Contributions
Chungah Kim, Andrew Nielsen, and Antony Chum co-wrote the first draft of the study. Chungah Kim analyzed the data. Chungah Kim and Antony Chum contributed to the interpretation of the data. Antony Chum, Chungah Kim, and Andrew Nielsen co-wrote the dataset creation plan. Antony Chum conceived of the initial project and provided funding and oversight of the study. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding for the study was provided by Canadian Institutes of Health Research (Project Grant FRN# 173447, NPI: Antony Chum). The funding agencies had no role in the design and conduct of the study; the collection, management, analysis or interpretation of the data; the preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication. The project principal investigator (Antony Chum) is also supported by the Canada Research Chair Program (grant CRC-2021-00269).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.