
Abstract
Objective:
To determine the relationship between household food insecurity status over a 12-month period and adults’ use of publicly funded health care services in Ontario for mental health reasons during this period.
Methods:
Data for 80,942 Ontario residents, 18 to 64 years old, who participated in the Canadian Community Health Survey in 2005, 2007-2008, 2009-2010, or 2011-2012 were linked to administrative health care data to determine individuals’ hospitalizations, emergency department visits, and visits to psychiatrists and primary care physicians for mental health reasons. Household food insecurity over the past 12 months was assessed using the Household Food Security Survey Module. Logistic regression models were used to estimate the odds of mental health service utilization in the past 12 months by household food insecurity status, adjusting for sociodemographic factors and prior use of mental health services.
Results:
In our fully adjusted models, in comparison to food-secure individuals, the odds of any mental health care service utilization over the past 12 months were 1.15 (95% confidence interval [CI], 1.04 to 1.29) for marginally food-insecure individuals, 1.39 (95% CI, 1.19 to 1.42) for moderately food-insecure individuals, and 1.50 (95% CI, 1.35 to 1.68) for severely food-insecure individuals. A similar pattern persisted across individual types of services, with odds of utilization highest with severe food insecurity.
Conclusions:
Household food insecurity status is a robust predictor of mental health service utilization among working-age adults in Ontario. Policy interventions are required to address the underlying causes of food insecurity and the particular vulnerability of individuals with mental illness.
Introduction
Household food insecurity (inadequate or insecure access to food because of financial constraints) is a serious public health problem in many affluent nations, including Canada. In 2012, the most recent year for which national data are available, 12.6% of Canadian households experienced some food insecurity. 1 Food insecurity is a potent marker of nutritional inequities in Canada, 2 –4 but the associations between food insecurity and health extend far beyond nutritional vulnerability. In Canada, experiences of hunger in childhood or youth have been linked to the subsequent development of a variety of chronic conditions, including asthma and depression. 5 –7 Among Canadian adults, measures of household food insufficiency and food insecurity have been associated with multiple indicators of chronic disease and poor health 8 –11 and increased health care utilization. 2,12
The association between household food insecurity and mental illness is particularly strong, with analyses of Canadian population survey data revealing substantially higher odds of mood and anxiety disorders, 13 –15 signs and symptoms of depression, 14 and suicidal ideation, 14,16 among adults in food-insecure households, independent of other sociodemographic predictors of poor health. Similar associations have been reported in the United States, 17 –26 United Kingdom, 27,28 Australia, 29 New Zealand, 30 and globally. 31 Studies of specific patient populations (e.g., type 2 diabetes, HIV, hepatitis C) have also reported strong associations between depression and food insecurity. 32 –35 The relationship appears to be graded, with the probability of mental health problems rising with the severity of household food insecurity. 11,14 –16,23,34,36 For example, 9% of food-secure adults (18-64 years) in the 2007-2008 Canadian Community Health Survey (CCHS) reported diagnosis of a mood or anxiety disorder, but this rose to 16% with marginal food insecurity, 22% with moderate food insecurity, and 40% with severe food insecurity. 11
While the existing research suggests that mental health problems are common among adults affected by household food insecurity, almost all of this evidence has been drawn from self-reports of mental health status. One exception is a recent UK study using primary care records to chart higher rates of common mental disorders among food-insecure women in the perinatal period. 28 Objective measures of morbidity are needed to fully understand the burden of mental illness associated with household food insecurity in Canada. Using linked survey and administrative health care data from a large population-based sample of adults in Ontario, this study was undertaken to determine the relationship between household food insecurity status over a 12-month period and adults’ use of publicly funded health care services for mental health reasons during this period.
Methods
Data Sources
This study made use of data from 4 cycles of Statistics Canada’s CCHS, conducted in 2005, 2007-2008, 2009-2010, and 2011-2012. 37 Statistics Canada conducts the CCHS to provide regular and timely estimates of health determinants, health status, and health system use for individuals, 12 years of age and older, living in private dwellings across Canada.
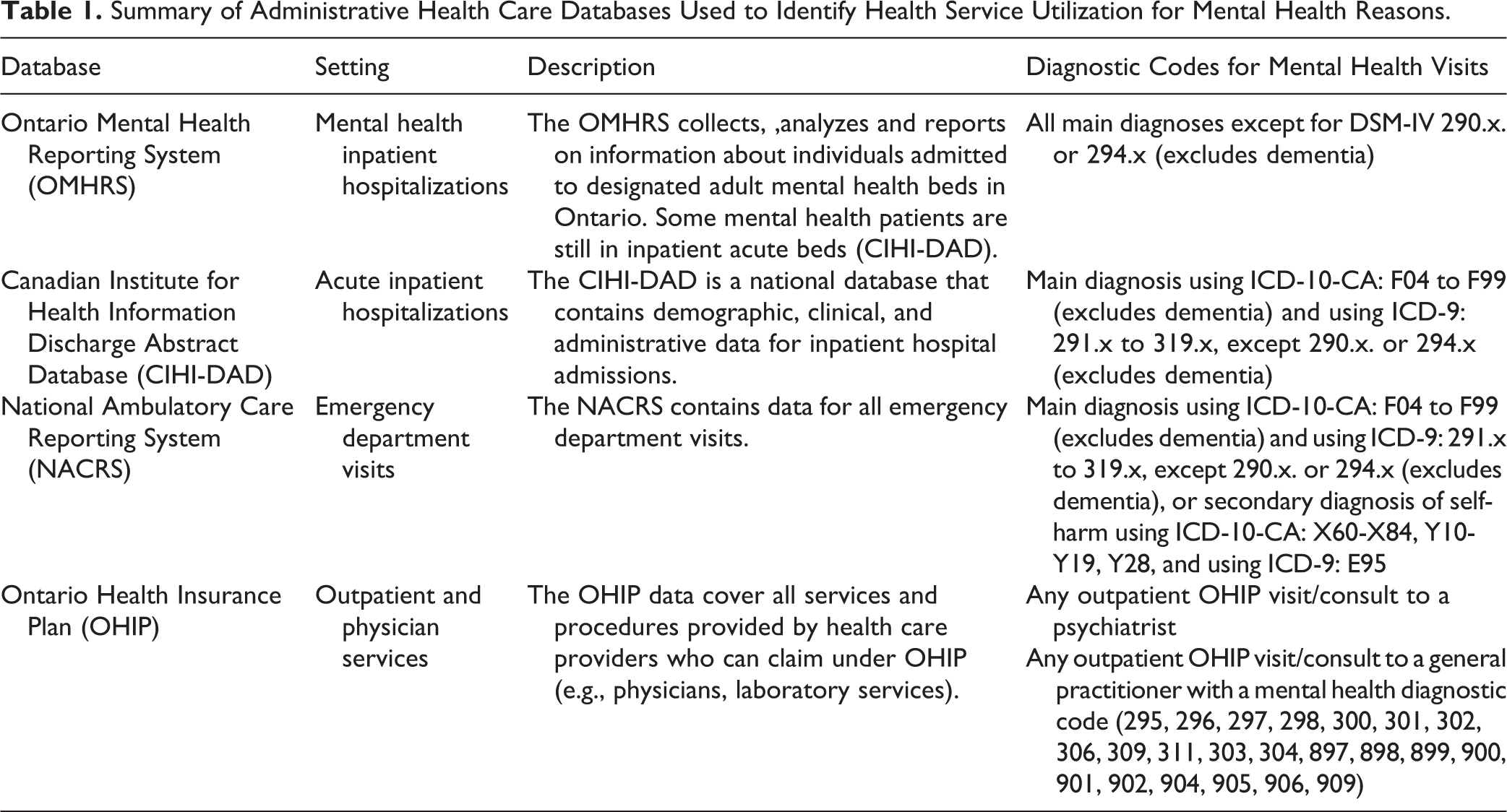
Data from CCHS were linked to administrative health care data that have been uniquely encoded and housed at the Institute for Clinical Evaluative Sciences in Toronto, Ontario, for all respondents who gave permission to have their survey data linked. This included 83% of respondents in the 4 cycles of CCHS used. We used the Canadian Institute for Health Information Discharge Abstract Database, Ontario Mental Health Reporting System, National Ambulatory Care Reporting System, and Ontario Health Insurance Plan claims. To identify health service utilization that was specifically for reasons of mental health, we used the diagnostic groupings developed for the Mental Health and Addictions Scorecard and Evaluation Framework Baseline Scorecard for inpatient and emergency department visits 38 and the modified validated algorithm for outpatient visits, 39 which includes indicators focused predominantly on care provided in outpatient physician and acute care settings. These data sets and the diagnostic codes applied to each data set to identify service utilization for mental health reasons are described in Table 1.
Summary of Administrative Health Care Databases Used to Identify Health Service Utilization for Mental Health Reasons.
Population
Our initial linked sample comprised 87,387 individuals, 18 years and older, living in the province of Ontario and with a valid Ontario health insurance number during the 4 years prior to their CCHS interview. The exclusion of individuals without a valid health insurance number for the entire period (n = 2489) and those with missing data on food insecurity status or any sociodemographic covariate (n = 3956) resulted in a final analytic sample of 80,942 individuals. If an individual was a respondent in more than 1 cycle of CCHS (n = 937), only their first record was included in this study.
To minimize the loss of sample due to missing data on household income (a problem affecting 16.8% of respondents), data on neighborhood-level income quintiles were derived by linking 2006 census data to individuals’ residential postal code data. Statistics Canada has adjusted income for household size and community size such that each community would be expected to have 20% of its population in each income quintile. This ecological proxy methodology has been found to reliably estimate household income quintile. 40
Measures
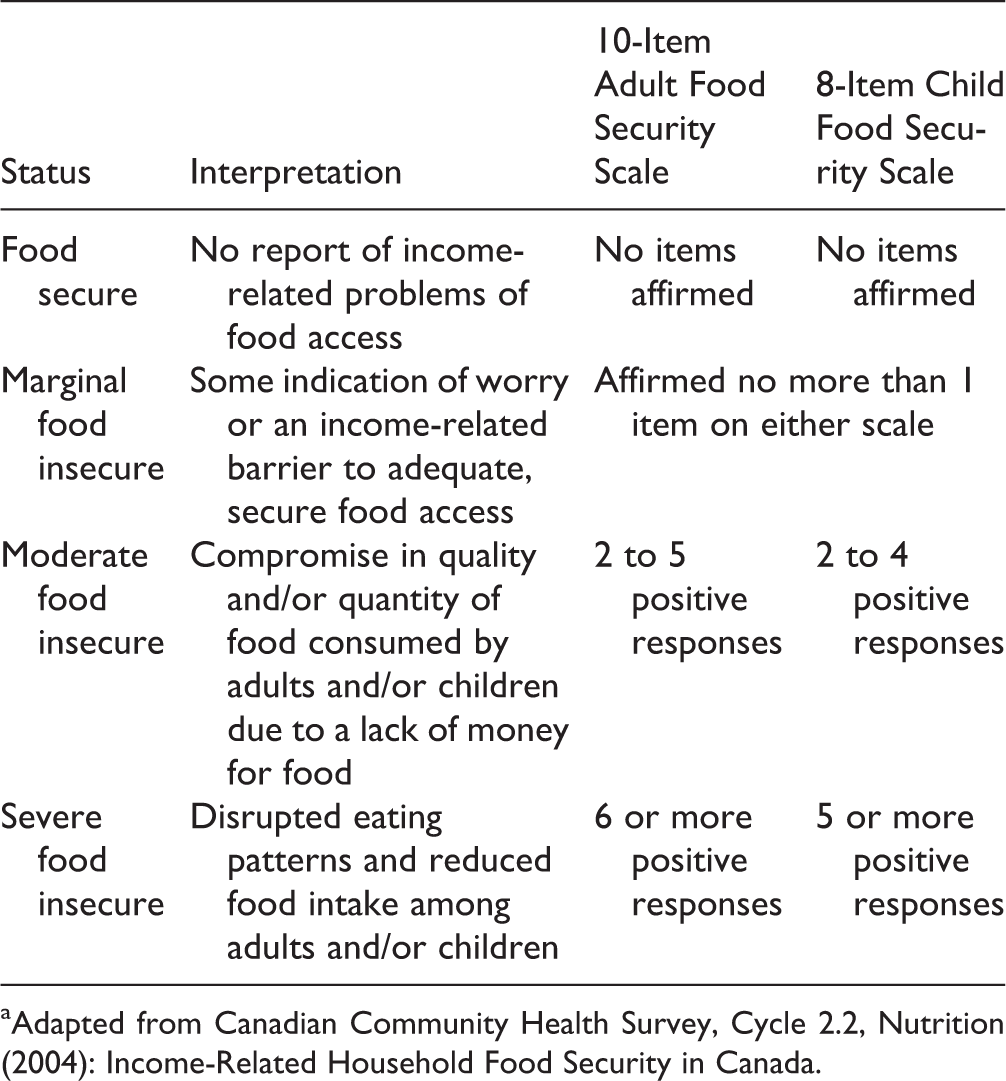
Household food security status and sociodemographic characteristics were derived from the CCHS. Household food insecurity over the past 12 months was assessed using the Household Food Security Survey Module, a validated, 18-item scale 41 (Appendix A). The conditions assessed range from experiences of anxiety that food will run out before household members have money to buy more, to modifying the amount of food consumed, experiencing hunger, and going whole days without eating. We applied Health Canada’s classification scheme to define moderate and severe household food insecurity. 41 Respondents with no affirmative responses were considered “food secure,” while those with 1 affirmative response were considered “marginally food insecure.” (Details of the classification scheme are presented in Appendix B.)
Outcomes included outpatient visits to psychiatrists and primary care physicians for a mental health reason and emergency department visits and hospital admissions for which the main diagnosis was a mental health problem (Table 1). Because the majority of the individuals in our sample made no use of health care services for mental health reasons over the past 12 months, service use was coded as a dichotomous variable, with use defined as 1 or more visits or hospital admissions.
Statistical Analyses
Sample characteristics were described using means and proportions. (See Supplementary Tables S1 and S2 for a comparison of characteristics of the analytic sample with respondents excluded due to missing data.) Linear trend and chi-square tests were performed to examine the association between each covariate and food insecurity status. Linear trend tests were conducted to determine the association between the number of adults with hospitalizations, emergency department visits, psychiatrist visits, and visits to primary care physicians for a mental health reason and household food insecurity status.
Binary logistic regression models were used to estimate the odds of mental health service utilization (considering any service utilization as well as the 4 specific types of service utilization described above) in the 12 months prior to the CCHS interview by household food insecurity status over this period. Models were adjusted for age, sex, and sociodemographic characteristics previously identified as significant predictors of household food insecurity status and mental health. 11,42 These variables included respondent’s education, respondent’s immigration status (defined as Canadian born or not), household structure, number of adults and number of children younger than 18 years living in the household, household income (represented by neighborhood income quintile at the census tract level), main source of household income, homeownership, and urban versus rural residence.
To differentiate health care utilization for mental health reasons in the past 12 months that reflects continued care for chronic mental health problems from that which is indicative of heightened health care needs associated with household food insecurity in the current year, we reran the regression models described above, including binary variables to indicate service utilization for mental health reasons in each of the 3 prior years.
Because Canadian population studies have repeatedly documented substantially higher rates of mood and anxiety disorders among women than men in food-insecure households, 11,13,15,36 we repeated the aforementioned logistic regression analyses of mental health care utilization, including an interaction term to test whether the observed associations between food insecurity and mental health care utilization differed by sex. No model yielded a statistically significant interaction (P > 0.05). To confirm that the relationship between food insecurity and mental health care utilization was similar for men and women, we repeated the logistic regression analysis of any health care utilization for mental health reasons, stratifying by sex.
An alpha level of P < 0.05 was used to test for significance, and all tests were 2-sided.
Results
The mean age of participants was 42.7 years, and 53.7% were female (Table 2). The prevalence of household food insecurity in the study sample was 12.1%, with 3.7% marginally food insecure, 5.2% moderately food insecure, and 3.1% severely food insecure. When stratified by household food insecurity status, participants differed significantly in age, sex, household composition, education, home ownership, income, main income source, and urban versus rural area of residence. Adults in food-insecure households were much more likely to rent rather than own their dwellings, to be reliant on social assistance, and to be either unattached and living alone or to be lone parents.
Sample Characteristics.
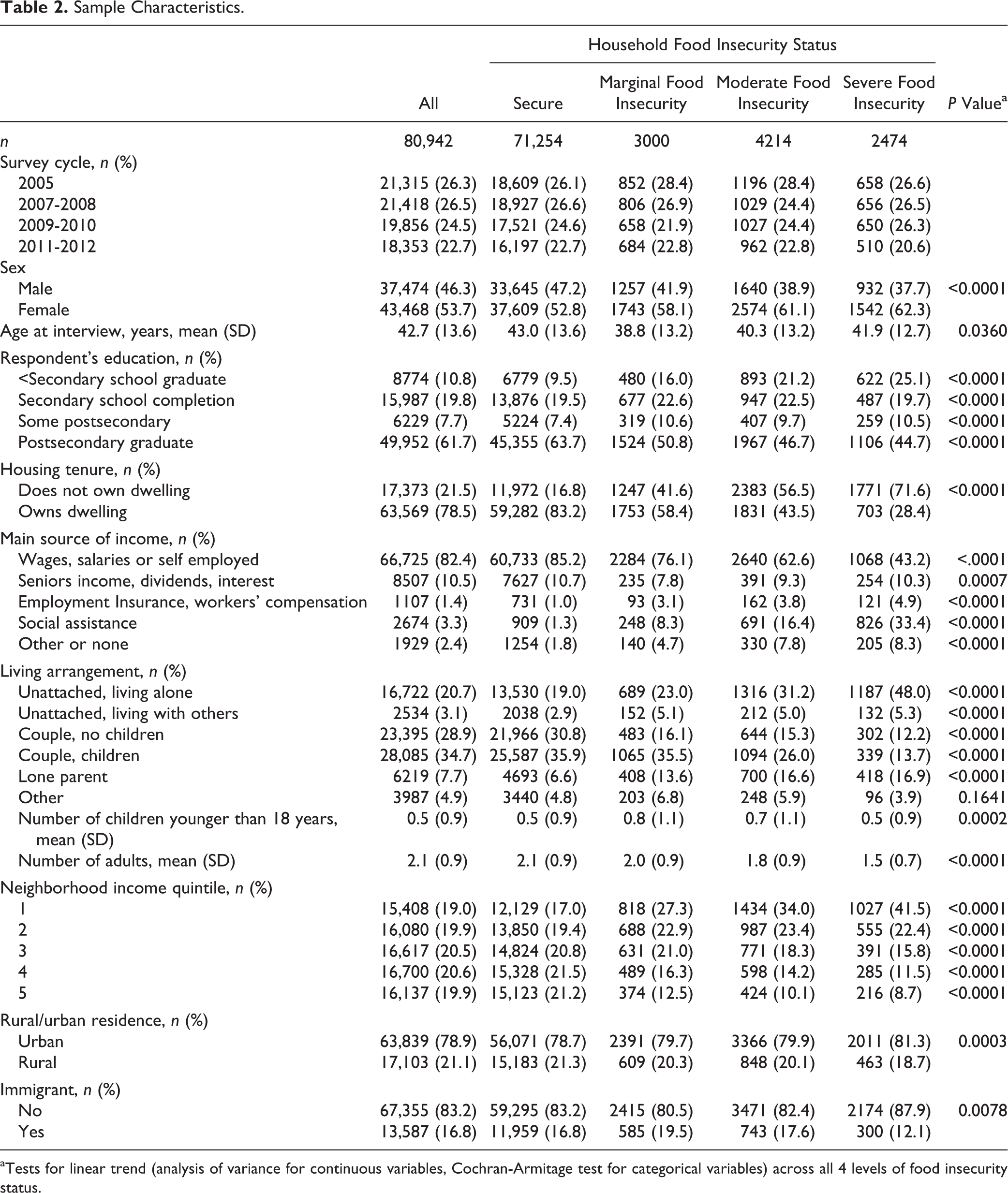
aTests for linear trend (analysis of variance for continuous variables, Cochran-Armitage test for categorical variables) across all 4 levels of food insecurity status.
In the past 12 months, 17.2% of participants received some form of health care for mental health reasons, with similar rates of utilization in each of the prior 3 years (Table 3). The proportion of participants using mental health services in the past 12 months rose significantly, with increasing severity of household food insecurity, irrespective of the type of health service considered. Whereas 40.4% of adults in severely food-insecure households had received some treatment for mental health reasons in the past 12 months, only 15.6% of adults in food-secure households had received such treatment. Similar trends were observed in mental health care service utilization in the 3 preceding years. Whereas 25.2% of food secure adults had used mental health care services in the past 12 months and prior 3 years, this proportion rose to 28.5% among the marginally food insecure, 37.6% among the moderately food insecure, and 42.9% among the severely food insecure.
Mental Health Care Utilization in Past 12 Months (Concurrent with Measure of Food Insecurity Status) and 3 Years Prior, n (%).
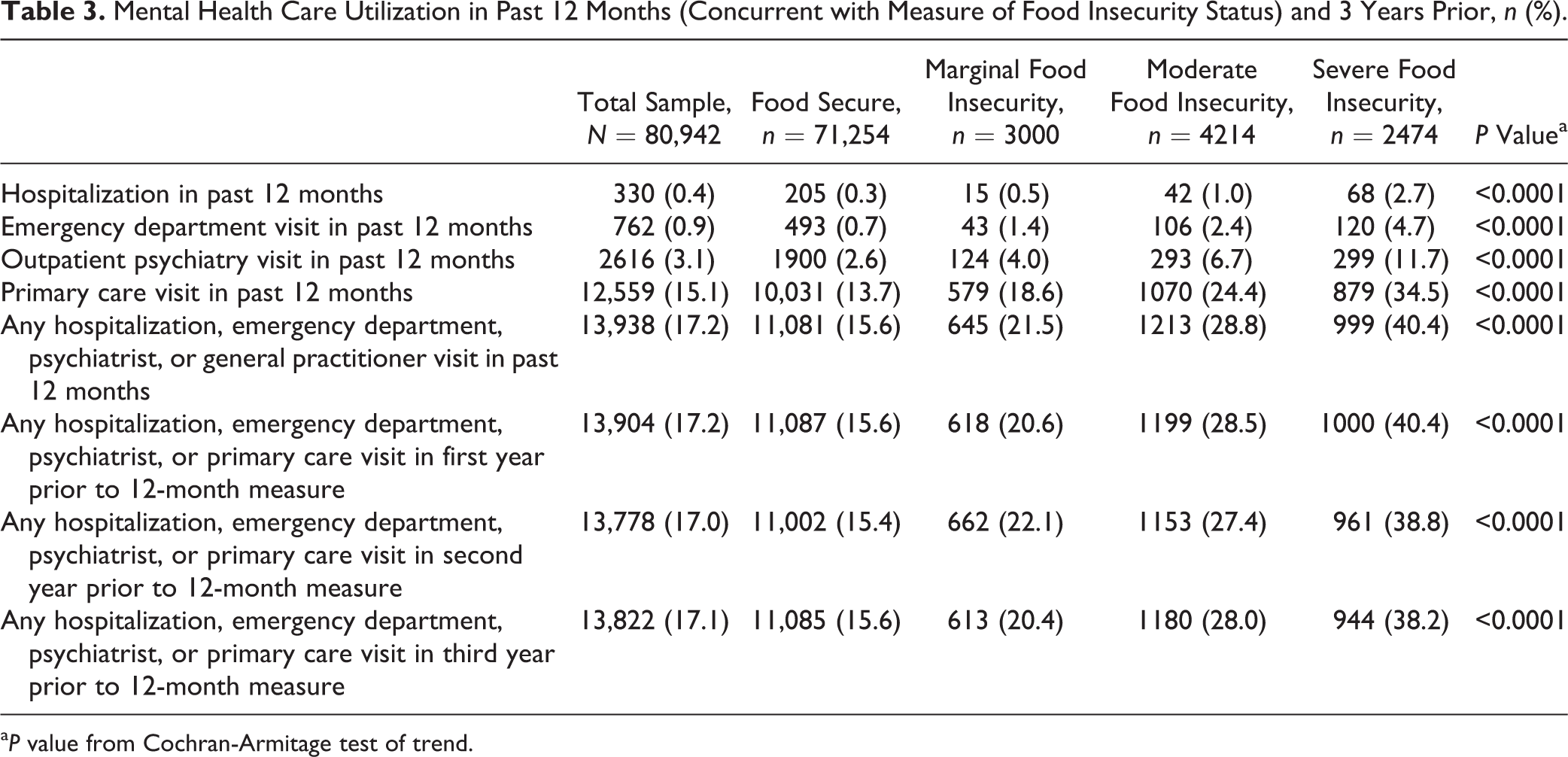
a P value from Cochran-Armitage test of trend.
When the rates of health service utilization among adults in food-insecure households were considered relative to the total number of adults seeking care for mental health problems, the food insecure comprised 37.9% of all adults hospitalized, 34.9% of those treated in an emergency department, 27.2% of those who saw a psychiatrist, and 20.0% of those who saw a family physician or general practitioner for mental health reasons in the course of the year (Figure 1). The disproportionate use of health services by adults in severely food-insecure households was particularly notable; 1 in 5 of adults hospitalized because of mental illness fell into this category.
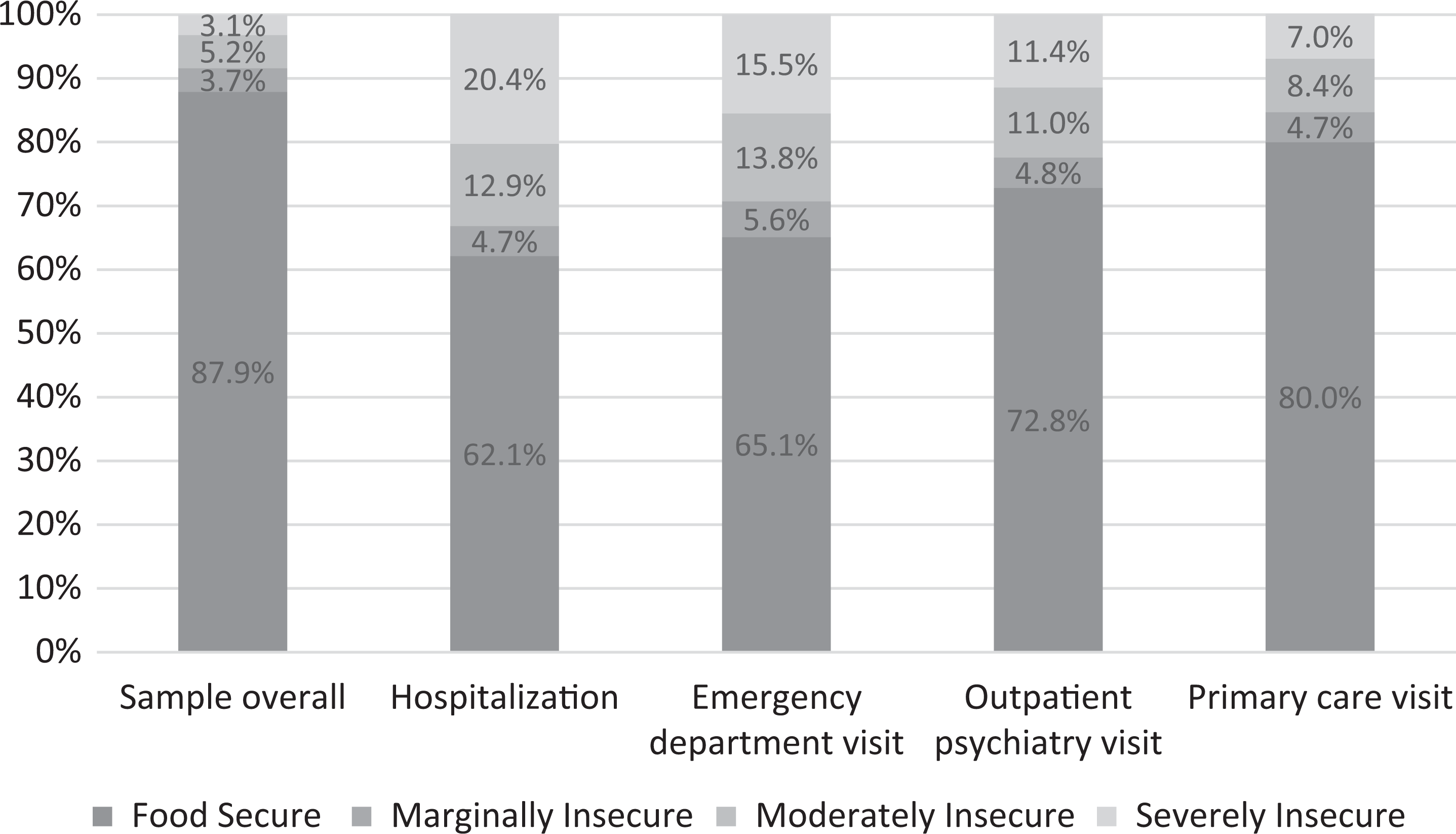
Household food insecurity status of the sample overall and among subgroups who used specific mental health care services in past 12 months.
After adjusting for sociodemographic variables, adults in severely food-insecure households had 2.16 times the odds (95% confidence interval [CI], 1.97 to 2.36) of using any mental health care service over the past 12 months compared with those in food-secure households (Table 4). Moderate food insecurity was associated with 1.61 times the odds (95% CI, 1.49 to 1.73) and marginal food insecurity with 1.23 times the odds (95% CI, 1.12 to 1.35) of using any mental health care service. When individuals’ use of mental health care services in the prior 3 years was taken into account, the odds ratios were attenuated, but all remained statistically significant. (See Supplementary Table S3 for the full models.) When this analysis was repeated, stratified by sex, the associations between use of any mental health care service and severity of food insecurity were fairly similar for men and women, but marginal food insecurity was not significantly associated with mental health care utilization among men (Supplementary Table S4).
Adjusted Odds (95% Confidence Interval) of Using Any Health Care Service and Each Specific Health Care Service for Mental Health Reasons over 12-Month Period, by Household Food Insecurity Status, Comparing Each Group to Adults in Food-Secure Households.
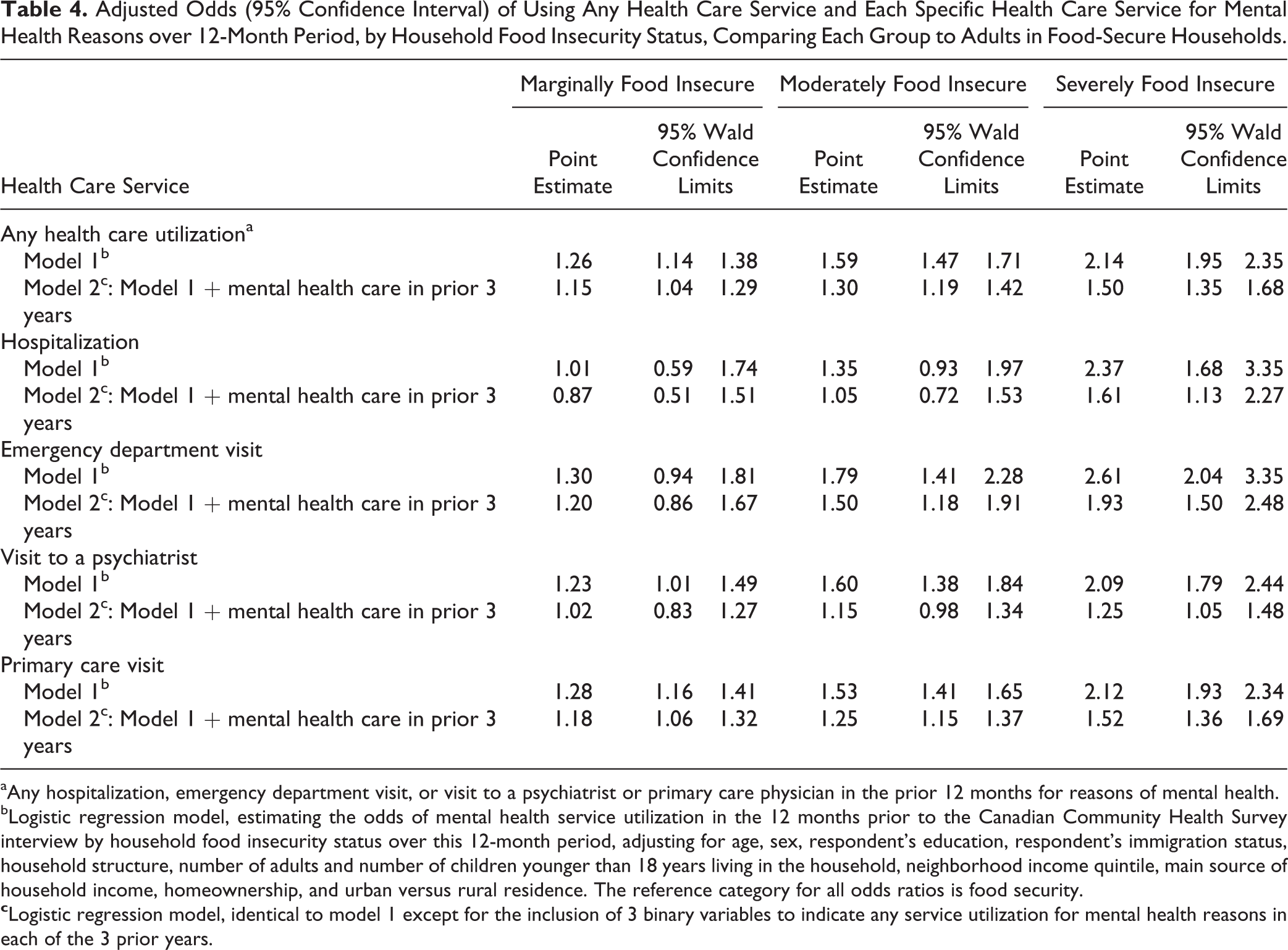
aAny hospitalization, emergency department visit, or visit to a psychiatrist or primary care physician in the prior 12 months for reasons of mental health.
bLogistic regression model, estimating the odds of mental health service utilization in the 12 months prior to the Canadian Community Health Survey interview by household food insecurity status over this 12-month period, adjusting for age, sex, respondent’s education, respondent’s immigration status, household structure, number of adults and number of children younger than 18 years living in the household, neighborhood income quintile, main source of household income, homeownership, and urban versus rural residence. The reference category for all odds ratios is food security.
Considering individuals’ use of specific mental health care services, those in severely food-insecure households had significantly higher odds of being hospitalized and having visited an emergency department, primary care physician, or psychiatrist when compared with the food secure (Table 4). Adjusting for individuals’ use of mental health care services in the prior 3 years resulted in an attenuation of the observed odds, but all remained statistically significant. Moderate food insecurity was associated with significantly higher odds of having visited an emergency department, primary care physician, or psychiatrist, but the latter finding lost statistical significance when adjusted for mental health service utilization in the prior 3 years. Compared with those who were food secure, adults in marginally food-insecure households had only a significantly higher odds of seeing a psychiatrist or primary care physician for mental health reasons, and only the latter finding remained statistically significant when adjusted for prior use of health care services for mental health reasons.
Discussion
Our study showed that household food insecurity was a strong predictor of adults’ use of health care services for mental health reasons, independent of other well-established social determinants of health. This pattern persisted across all types of services, including hospitalizations, emergency department visits, and visits to psychiatrists and primary care physicians. The observed effects were graded, with more severe food insecurity associated with higher odds of health service utilization. Our findings importantly extend the previous Canadian research showing greater likelihood of mental health problems among adults in food-insecure households by revealing the disproportionate burden that adults affected by food insecurity place on health care services for mental illness.
Whereas most prior studies have relied on self-reports of symptoms and diagnosed mood and anxiety disorders, our analysis of administrative health care data for a large, population-based sample provides objective evidence of the strong link between mental health problems and household food insecurity. Our use of comprehensive data on adults’ health care utilization with recorded diagnoses of mental illness and a highly validated scale of household food insecurity and our ability to take into account prior mental health care utilization are particular strengths of this study. Although our sample is based on survey data from 2005 to 2012, the prevalence of food insecurity in Ontario was stable over this period and has not changed significantly since. 43 Insofar as those excluded because of missing data were more vulnerable (as indicated by their lower level of education and slightly higher health care utilization rates, Supplementary Tables S1 and S2), their omission would have biased our results toward the null. The fact that our study was conducted in the context of a universal health care system minimizes biases associated with financial barriers to health care access, although some adults still experience barriers to accessing mental health care services in the province. 42 In addition, it should be noted that our analysis of health care utilization provides an incomplete account of individuals’ service utilization because we could not assess the use of community mental health programs or privately provided treatment services. In addition, our use of health administrative data to categorize individuals with mental illness necessarily relies on access to such services. Since access to mental health services is known to be problematic in Ontario, and access difficulties are seen most prominently in vulnerable populations (e.g., low-income groups), 42 it is likely that we have classified food-insecure individuals in the non–mental health category. This implies that we have underestimated the relationship between mental illness ascertained through health service utilization and food insecurity and may have misclassified the vulnerable who cannot access mental health services.
We observed a gradient in health care utilization with increasing severity of household food insecurity, independent of other social determinants of health and prior treatment for mental health problems, but the methods we employed preclude causal inference. The financial stress of food insecurity has been shown to precipitate mental health problems, 24,25,36 but there is also prospective evidence that maternal depression increases the risk of food insecurity among low-income families. 44 Two studies of very-low-income women have charted bidirectional relationships between food insecurity and depression. 45 –47 However, almost all of this research is based on self-reported measures of mental health among highly selected population subgroups in the United States. Longitudinal Canadian studies are needed to elucidate the relation between adults’ mental health and food insecurity status.
Although analyses of Canadian population survey data have repeatedly found a higher prevalence of self-reported mental health problems among women than men in food-insecure households, 11,13,15,16,36 we found little difference in the relationship between food insecurity and health service utilization by sex. These findings are not necessarily contradictory. Food-insecure women may be more likely than food-insecure men to suffer from mental illness but do not differ in their use of health care services.
The intersection of food insecurity with mental illness has important implications for intervention because, irrespective of which condition came first, the coexistence of these problems can only further erode individuals’ health and their households’ circumstances. The substantially higher rate of hospitalization among severely food-insecure adults observed here implies a greater likelihood of more serious mental health problems among this group. Just as problems of mental illness impede individuals’ abilities to transition out of food insecurity, 48 the extreme material hardship denoted by severe food insecurity must compromise adults’ abilities to comply with treatment regimens and manage chronic mental health conditions. The coexistence of household food insecurity and mental illness among adults may also have implications for the health and well-being of other household members, particularly children. There is some evidence to suggest that the negative effects of household food insecurity on children’s health are in part a function of associated maternal depression. 20,27,49 While it was beyond the scope of our study to assess the health of other household members, we note that almost 42% of adults in food-insecure households in our sample lived with children, and 38% of these were lone parents. More research is needed to understand how the combination of household food insecurity and mental illness among parents is affecting their children.
The social epidemiology of food insecurity in Canada is well established, 9,50 –56 and there is growing evidence of the sensitivity of household food insecurity to policy interventions that improve household finances. 57 –61 Yet, to date, no federal or provincial policy interventions or programs have been launched with the explicit goal of reducing or preventing household food insecurity. Government responses have instead focused on initiatives to support community-based charitable food assistance programs. 62 Such programs remain the only direct response to food insecurity in Canada, despite an abundance of evidence that the assistance is insufficient to alter household circumstances. 63 –70 Health care providers have little chance of addressing patients’ food insecurity through referrals to community food programs, but by routinely screening patients for poverty and providing assistance to those struggling to “make ends meet,” they can help patients to access income supports to which they are entitled. 71
Our results lend support to calls for evidence-based policy interventions to address problems of financial hardship that underpin food insecurity. The significant reductions in food insecurity observed among social assistance recipients in other provinces following improvements to benefits 57,58 suggest that some of the food insecurity observed among our sample could be ameliorated by similar reforms in Ontario. However, most food-insecure households in our sample were not on social assistance, but reliant on income from employment or other sources, and this is similar to the situation nationally. 1 Broader, population-level interventions are needed to address vulnerability to food insecurity that is associated with inadequate and insecure incomes more generally. Relatively modest increments in income have been found to reduce food insecurity among low-income families. 59,72,73 These findings, coupled with the marked drop in food insecurity among low-income individuals when they become eligible for public old-age pensions (i.e., a guaranteed annual incomes provided to Canadian seniors),60 suggest that interventions such as Ontario’s basic income pilot 74 may be particularly effective in reducing food insecurity. Evidence of decreased health care utilization for mental health reasons following implementation of a guaranteed annual income in Manitoba in the 1970s (the MINCOME experiment) 75 indicates the potential for a basic income to alleviate mental health problems. The Ontario pilot will provide a unique opportunity to determine how the provision of a more adequate, secure income affects the food insecurity status and mental health of working-aged individuals, while also shedding light on what additional supports are needed to address the co-occurrence of these problems.
In summary, food insecurity is associated with high rates of mental health service utilization, indicating a high burden of mental illness among those with food insecurity. The relationship is graded with more severe food insecurity associated with a higher burden of mental health service utilization. The joint burden of food insecurity and mental illness is worrisome given the heavy burden of each condition separately. Individuals with food insecurity and mental illness represent a uniquely vulnerable population that warrants attention from a policy and health service intervention perspective. Community-based interventions intended to aid those suffering from mental illness need to be prepared to offer additional supports to those struggling to meet basic needs, but evidence-based policy interventions are required to address the underlying causes of household food insecurity. At the same time, more research is needed to determine the optimal policy instruments, services, and supports to address the co-occurrence of food insecurity and mental illness.
Supplemental Material
supplementary_material_revised - The Relation between Food Insecurity and Mental Health Care Service Utilization in Ontario
supplementary_material_revised for The Relation between Food Insecurity and Mental Health Care Service Utilization in Ontario by Valerie Tarasuk, Joyce Cheng, Craig Gundersen, Claire de Oliveira, and Paul Kurdyak in The Canadian Journal of Psychiatry
Footnotes
Appendix A CCHS Household Food Security Survey Module a
The following questions are about the food situation for your household in the past 12 months.
You and other household members always had enough of the kinds of foods you wanted to eat. You and other household members had enough to eat but not always the kinds of food you wanted. Sometimes you and other household members did not have enough to eat. Often you and other household members didn’t have enough to eat.
- Don’t know/refuse to answer [Go to end of module]
Question Q1 is not used directly in determining household food security status.
Now I’m going to read you several statements that may be used to describe the food situation for a household. Please tell me if the statement was often true, sometimes true, or never true for you and other household members in the past 12 months.
Often true Sometimes true Never true
- Don’t know/refuse to answer
Often true Sometimes true Never true
- Don’t know/refuse to answer
Often true Sometimes true Never true
- Don’t know/refuse to answer
—IF CHILDREN UNDER 18 IN HOUSEHOLD, ASK Q5 AND Q6; OTHERWISE, SKIP TO FIRST LEVEL SCREEN—
Now I’m going to read a few statements that may describe the food situation for households with children.
Often true Sometimes true Never true
- Don’t know/refuse to answer
Often true Sometimes true Never true
- Don’t know/refuse to answer
—IF CHILDREN UNDER 18 IN HOUSEHOLD, ASK Q7; OTHERWISE SKIP TO Q8—
Often true Sometimes true Never true
- Don’t know/refuse to answer
The following few questions are about the food situation in the past 12 months for you or any other adults in your household.
Yes No (Go to Q9)
- Don’t know/refuse to answer
Almost every month Some months but not every month Only 1 or 2 months
- Don’t know/refuse to answer
Yes No
- Don’t know/refuse to answer
Yes No
- Don’t know/refuse to answer
Yes No
- Don’t know/refuse to answer
Yes No (IF CHILDREN UNDER 18 IN HOUSEHOLD, ASK Q13; OTHERWISE SKIP TO END)
- Don’t know/refuse to answer
Almost every month Some months but not every month Only 1 or 2 months
- Don’t know/refuse to answer
—IF CHILDREN UNDER 18 IN HOUSEHOLD, ASK Q13-16; OTHERWISE SKIP TO END—
Now, a few questions on the food experiences for children in your household.
Yes No
- Don’t know/refuse to answer
Yes No
- Don’t know/refuse to answer
Almost every month Some months but not every month Only 1 or 2 months
- Don’t know/refuse to answer
Yes No
- Don’t know/refuse to answer
Yes No
- Don’t know/refuse to answer
Appendix B. Determination of Household Food Insecurity Status Based on the Household Food Security Survey Module 1
| Status | Interpretation | 10-Item Adult Food Security Scale | 8-Item Child Food Security Scale |
|---|---|---|---|
| Food secure | No report of income-related problems of food access | No items affirmed | No items affirmed |
| Marginal food insecure | Some indication of worry or an income-related barrier to adequate, secure food access | Affirmed no more than 1 item on either scale | |
| Moderate food insecure | Compromise in quality and/or quantity of food consumed by adults and/or children due to a lack of money for food | 2 to 5 positive responses | 2 to 4 positive responses |
| Severe food insecure | Disrupted eating patterns and reduced food intake among adults and/or children | 6 or more positive responses | 5 or more positive responses |
aAdapted from Canadian Community Health Survey, Cycle 2.2, Nutrition (2004): Income-Related Household Food Security in Canada.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by a programmatic grant from the Canadian Institutes of Health Research (CIHR; FRN 115208). The analysis was also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by CIHR, ICES, or the MOHLTC is intended or should be inferred. The study sponsors had no role in the design of the study; the collection, analysis, or interpretation of data; the writing of the report; or the decision to submit the article for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.