
Abstract
Objective:
Analyses of representative, system-level data to examine trends in short- and longer-term readmission rates for psychiatric illnesses are largely absent. The objective of this article is to examine key trends and variables with implications for inpatient care as indicated by 30-day readmission and outpatient care as reflected by readmission within 5 years.
Methods:
Using OMHRS data from 2005 to 2015, patients who had their first inpatient admission were followed for 5 years to examine their subsequent 30-day and overall admission rates stratified by discharge time and diagnosis.
Results:
The study cohort consisted of 42,280 patients. The 30-day and 5-year readmission rates for the entire cohort were 7.2% and 35.1%, respectively. Using a time course analysis of readmission for discharges in different years, both 30-day readmission and 5-year readmission rates decreased in a linear manner from 2005 to 2010, primarily because of readmission patterns for patients diagnosed with mood disorders and schizophrenia/other psychotic disorders. It was also evident that both demographic considerations such as age and gender and variables reflective of social determinants such as education level and employment were predictive of rehospitalization risk.
Conclusions:
The trends of decreasing readmission rates may be reflective of improvements in the quality of hospital and community-based outpatient care. Such system-level indicators warrant tracking and may inform more effective tertiary prevention.
The economic burden of mental health problems in Canada is significant, and hospitalization is a primary driver of expense. 1 –3 Accordingly, hospital readmission is a pressing concern to the Canadian health care system. 4,5 Early readmission, typically benchmarked at 30 days posthospitalization, 4,6 is associated with inpatient care quality considerations such as premature discharge or a mismatch between patient needs and the level of outpatient service that was arranged. 4,6,7 Readmission that occurs after 30 days is understood to be more reflective of outpatient care quality. 4,8,9 Analyses of representative, system-level data to examine trends in readmission rates for psychiatric illnesses are lacking. The one prior provincial study in this area used a circumscribed time frame ending in 2011 that did not allow for comparison of readmission time frames, 9 and the one national study in this area is dated. 10 In response, this study examined 30-day and 5-year readmission rates using the Ontario Mental Health Reporting System (OMHRS) data from 2005 to 2015. The objective was to document key trends related to the delivery of inpatient care as reflected by early 30-day readmission and outpatient care as reflected by readmission within 5 years.
Methods
Data Source
Data for this study were obtained from OMHRS. Implemented in October 2005, OMHRS contains information on all hospital admissions for adults admitted to psychiatric beds in Ontario. OMHRS data are derived from the Resident Assessment Instrument–Mental Health (RAI-MH). The reliability and validity of the RAI-MH have been established in a number of previous studies. 11,12 The data can be requested from the Canadian Institute for Health Information (CIHI) for a fee and with certain restrictions (https://www.cihi.ca/en/ontario-mental-health-reporting-system-metadata). This study received approval from the Research Ethics Board of the Centre for Addiction and Mental Health (REB reference No. 093/2015).
Study Design
OMHRS records were obtained for all patients admitted and discharged between October 2005 and June 2015 from a psychiatric bed in Ontario. Discharge records for patients with the following criteria were extracted from the master database: (1) admitted on or after 1 October 2005 and discharged before 1 July 2010, (2) first psychiatric admission in life time to control for the potential confounding effects of previous psychiatric hospitalization, (3) aged 16 or older at admission, (4) planned discharge, and (5) length of stay (LOS) ≥3 days. Patient unique identification numbers were then used to retrieve admission records that occurred within 1825 days (5 years) following the discharge from the first inpatient episode. The primary outcomes of this study were 30-day and 5-year readmission, with readmission rates stratified by discharge time and Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), diagnostic category (Suppl. Table S1). Data were processed with Microsoft SQL server and analyzed with SPSS(v21). Multivariate logistic regression modeling was used to explore the significance of sociodemographic and service factors predictive of 30-day or 5-year readmission. The models were developed with 9 factors, including patients’ gender, age (<35 year, 35-50 years, or >50 years), marital status, language spoken, education level (<high school or ≥high school), employment status, Aboriginal status, type of hospital (general or psychiatric), and the index admission LOS (≤14 days or >14 days).
Results
Sample Characteristics
The study cohort consisted of 42,280 patients. By DSM-IV diagnostic category, 18,876 (44.6%) patients were diagnosed with mood disorders, 7614 (18.0%) with schizophrenia/other psychotic disorders, 7355 (17.4%) with substance-related disorders, 2933 (6.9%) with delirium/dementia, and 5502 (13.0%) with other diagnoses. The median age at admission was 42 years (interquartile range [IQR] 28-54), 42 years for mood disorders, 35 for schizophrenia/other psychotic disorders, 40 for substance-related disorders, 78 for delirium/dementia, and 38 for other diagnoses. Forty-eight percent of the cohort was female, and 2.8% of the cohort was identified as Aboriginal. Of the total cohort, 27.9% were admitted to a psychiatric hospital, and the median LOS was 14 days.
Readmission
The 30-day readmission rate for the cohort was 7.2%, with 6.8% for mood disorders, 10.2% for schizophrenia/other psychotic disorders, 4.3% for substance-related disorders, 10% for delirium/dementia, and 6.9% for other diagnoses (Table 1). Thirty-day readmission was stratified by discharge time. In a time course analysis, the 30-day readmission rate steadily declined between 2005 and 2010. Compared with the 2009-2010 group, the 30-day readmission rates were significantly higher in the 2005-2006, 2006-2007, and 2007-2008 groups (P < 0.05; Table 1). This decline was not evident for substance-related disorders or delirium/dementia.
Thirty-Day and 5-Year Readmission by Diagnostic Category and Discharge Time.
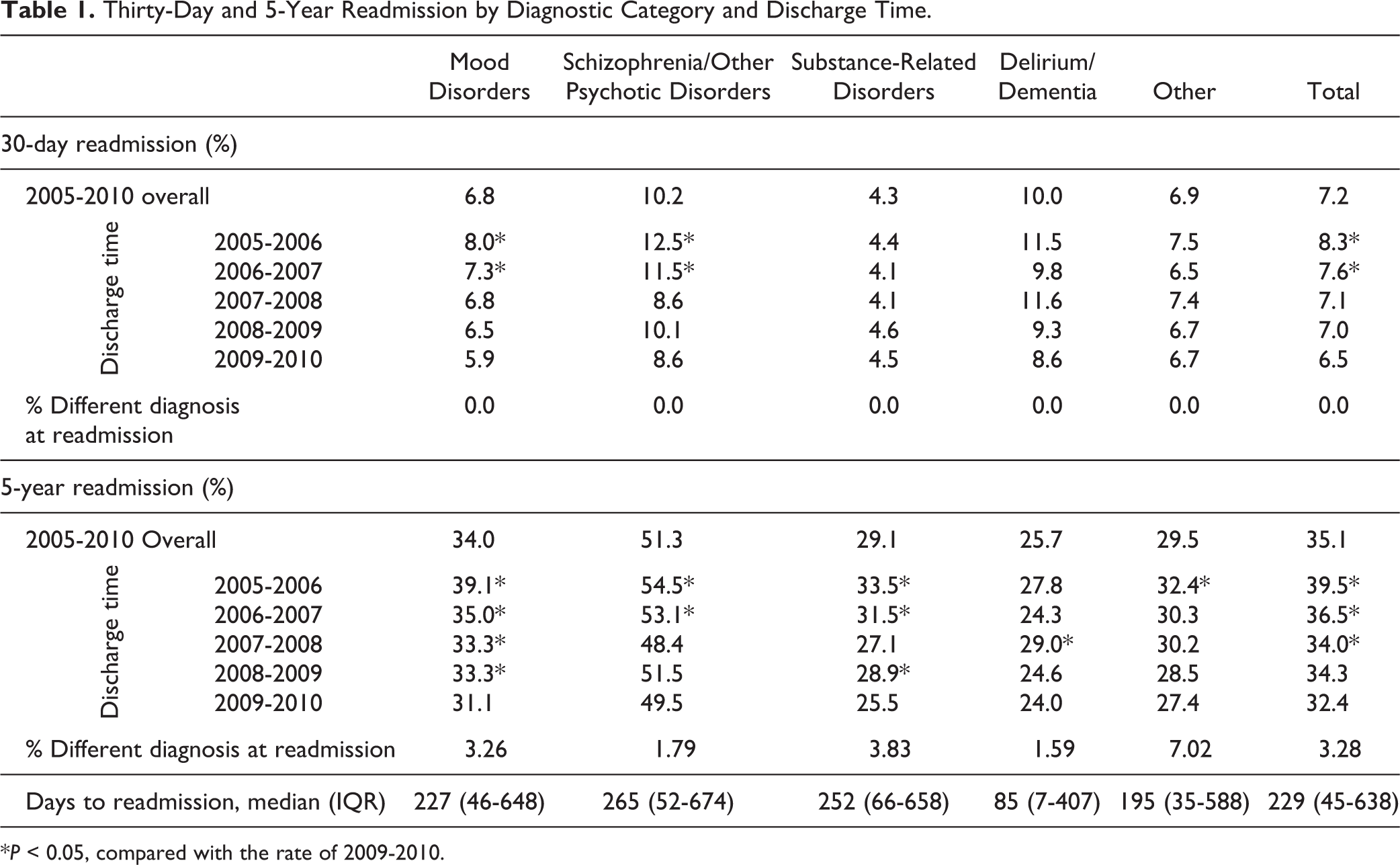
*P < 0.05, compared with the rate of 2009-2010.
The 5-year readmission rate for the entire cohort was 35.1%, with 34.0% for mood disorders, 51.3% for schizophrenia/other psychotic disorders, 29.1% for substance-related disorders, 25.7% for delirium/dementia, and 29.5% for other diagnoses (Table 1). As with 30-day readmissions, the rate went down from 2005 to 2010. The rates of 2005-2006, 2006-2007, and 2008-2009 were significantly higher than the 2009-2010 group with variability by diagnostic category (Table 1). This pattern was not evident for delirium/dementia. It was also found that for all those readmitted within 30 days, primary diagnosis at readmission was the same as the first inpatient episode. Looking at 5-year readmission, for all but 3.28%, the diagnostic category for their second admission within 5 years was the same as the first admission (Table 1).
For 5-year readmission, we also analyzed the time interval between the discharge of the first inpatient stay and the second admission. The medians were 229 days (IQR 45-638) for the full cohort, with 227 days (IQR 46-648) for mood disorders, 265 days (IQR 52-674) for schizophrenia/other psychotic disorders, 252 days (IQR 66-658) for substance-related disorders, and 85 days (IQR 7-407) for delirium/dementia (Table 1).
The association of selected sociodemographic and service factors with 30-day and 5-year readmission by diagnosis is found in Table 2, with significant protective and risk considerations highlighted. Details of the regressions analysis can be found in Supplemental Tables S2 to S6. Since 9 factors were included in each model, the predictive power of the models, as indicated by the pseudo-R 2 ‘s were not high. Being female was associated with a lower risk for 5-year readmission in schizophrenia/other psychotic disorders and both 30-day and 5-year readmission in delirium/dementia. Middle age (35-50 years) was protective for 30-day readmission in mood disorders, and both 30-day and 5-year readmission in schizophrenia/other psychotic disorders but was a risk factor for 5-year readmission in substance-related disorders. Being single/divorced/separated/widowed was a significant risk factor for 5-year readmission in mood disorders, schizophrenia/other psychotic disorders, and substance-related disorders. Speaking languages other than English (French or other language) was a beneficial factor for 5-year readmission in mood disorders, schizophrenia/other psychotic disorders, and substance-related disorders. Higher education was beneficial for both 30-day and 5-year readmission in schizophrenia/other psychotic disorders but a risk factor in delirium/dementia. Not being employed was a significant risk factor for readmission in almost all diagnoses. Aboriginal origin was a risk factor for 5-year readmission in schizophrenia/other psychotic disorders. Hospital type (psychiatric hospital) was a significant risk factor for readmission in all major diagnoses. Longer LOS (>14 days) was a risk factor for 5-year readmission in mood disorders but a beneficial factor for readmission in substance-related disorders and delirium/dementia.
Odds Ratio (95% Confidence Interval) Findings of Associations between Demographic, Psychosocial and Service Variables, and 30-Day and 5-Year Inpatient Readmission.
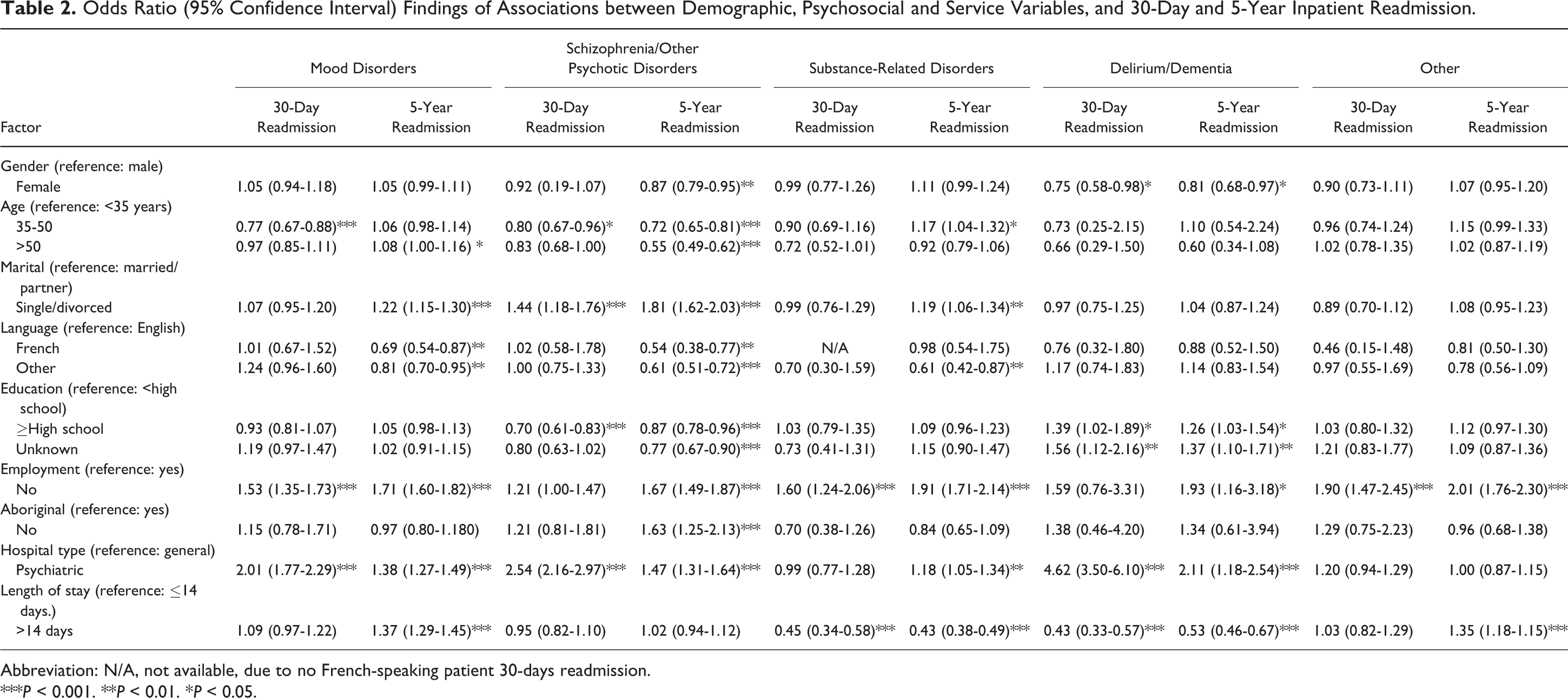
Abbreviation: N/A, not available, due to no French-speaking patient 30-days readmission.
***P < 0.001. **P < 0.01. *P < 0.05.
Discussion
This study provides a summary of early and longer-term readmission rates using a representative provincial data set. The 30-day readmission rate for the study cohort was 7.2%, which is lower than the previously reported rate of 9.2% using the OMHRS 2008-2010 data linked to other data sets such as the Discharge Abstract Database and the Ontario Health Insurance Program database. 9 The lower rate in the present study might be reflective of the larger cohort, controlling for previous hospitalization as a risk factor and OMHRS not capturing all psychiatric admission/readmissions. Longer-term periods of readmission have received less attention. In this study, the 5-year readmission rate of 35.1% is close to the rate of 37.9% observed in Taiwan using a similar method. 8
In the time course analysis of readmission, both 30-day readmission and 5-year readmission rates decreased in a linear manner from 2005 to 2010, primarily because of readmission patterns for mood disorders and schizophrenia/other psychotic disorders. These trends may be reflective of enhancements in the quality of hospital and community-based outpatient care or other system-level considerations such as increasing financial constraints affecting access to hospital beds. 13 –15
Most of the risk factors for readmission found in this study have been consistent with reports from other studies. 8,9 It was clear that acuity and complexity as reflected by length of initial hospital stay and hospitalization in tertiary facilities had implications for both short- and longer-term readmission. It was also evident that both static demographic considerations such as age and gender as well as variables reflective of social determinants such as education level and employment also were predictive of rehospitalization risk. Such patterns have been observed previously 8,9 and have implications for targeted approaches to reduce readmission risk. We have previously reported that being unemployed and being single/divorced/separated/widowed were significant risk factors associated with longer LOS and less functional improvement in schizophrenia patients. 16 It was of interest to note that these factors were also significant risk factors for readmissions.
With respect to limitations, it is of note that the OMHRS data set may not capture all psychiatric admissions in Ontario. Based on unpublished data from the Institute for Clinical Evaluative Sciences, it has been estimated that approximately 20% of psychiatric admissions in Ontario were not captured by OMHRS, including psychiatric admissions to intensive care units after suicide attempts and to overflow medical beds. 9 Death of older patients during the 5-year follow-up, particularly patients with dementia, may also contribute to an underestimate of the 5-year readmission rates, and we were unable to exclude planned readmissions. Such factors might contribute to a margin of systematic error in our study, but the large sample size offsets the degree of concern to at least some extent.
Supplemental Material
Supplemental_tables - Thirty-Day and 5-Year Readmissions following First Psychiatric Hospitalization: A System-Level Study of Ontario’s Psychiatric Care
Supplemental_tables for Thirty-Day and 5-Year Readmissions following First Psychiatric Hospitalization: A System-Level Study of Ontario’s Psychiatric Care by Sheng Chen, April Collins, and Sean A. Kidd in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.