
Abstract
Recent Australian data suggest that each year 0.4% of the adult population has contact with the mental health inpatient sector, and that 80% of these report comorbid mental disorders [1]. Despite the shift towards community-based care, acute hospitalization for psychiatric disorders remains an essential component of mental health care; but the contribution of acute inpatient care to short–medium-term treatment outcomes for individuals with mental illness is not well understood or widely researched [2]. Two issues loom large in this context: one concerns the occurrence of adverse events in hospital, such as aggressive or self-harm incidents, absconding or illicit substance use; the other concerns the identification of key features of an episode of hospitalization associated with clinical outcomes (e.g. assessment or treatment protocols used, length of stay, readmissions). There is a perception that constraints in resource allocation for hospital care and community services may have contributed to hospital crowding, suboptimal lengths of stay and access block, compromising quality of care and clinical outcomes. One of the consequences of such systemwide pressures may be patient violence. The number of aggressive incidents in acute psychiatric units has increased to the extent that many mental health professionals now expect to encounter violence in their work with patients [3].
Adverse inpatient incidents
Indices used to describe the prevalence of aggressive episodes vary widely [4–8], with typical estimates around 10–15% of admissions. A range of factors have been associated with inpatient aggressive incidents, including: age [4], [9]; previous psychiatric admission [4], [7], [9]; involuntary admission [9–11]; and duration of stay [4], [5], [7], [10]; as well as staff- [5] and setting-related factors [12]. Higher rates of inpatient aggression have also been associated with several diagnostic groupings, including: schizophrenia and acute psychoses [4], [5], [7]; mania [13]; and personality disorder [10]; while lower rates have been observed among patients with depression and adjustment disorder [7]. Moreover, the risk factors for psychiatric inpatient aggression appear to differ somewhat from those associated with aggression in the community [11], [12].
In contrast to aggression [5], [12], there have been few attempts to synthesize the absconding research literature [14]. An increased risk of absconding has been associated with: being younger, male [15] or single [16]; admitted as an involuntary patient [17]; having substance use problems [14]; or a diagnosis of personality disorder or schizophrenia [15]. But several of the older studies in this area were essentially descriptive accounts of consecutive series of patients involved in adverse incidents [17]. Therefore it may be difficult to determine whether or not particular patient or setting factors actually made a contribution (e.g. rates of schizophrenia among absconding patients may appear to be higher simply because the majority of referrals to that service had a diagnosis of schizophrenia).
Length of stay and early readmission
Several studies have examined the possible determinants of length of stay and re-hospitalization rates [18–21]. Patients involved in aggressive incidents have been reported to have much longer hospital stays (e.g. 24.88 vs 12.06 days) [7], while illness severity has also been strongly associated with variations in length of stay [22], [23]. An increased length of stay has been linked to diagnoses of schizophrenia [24] and comorbid medical conditions [25], with shorter stays reported for patients with substance use problems [26]. Higher hospital admission and readmission rates have also been associated with: younger age [19], [21], [27]; single status [27]; previous hospital admissions [28]; comorbid substance use problems [2], [29]; a diagnosis of psychosis [30–32]; and inadequate access to after-care [20], [33]; together with individual and social factors, such as satisfaction with life [34] and financial problems [35].
Purpose of this paper
The Acute Services Project (ASP) was a multi-centre service evaluation project conducted in 11 mental health units. During the prospective, 12 month implementation and evaluation phase, data for each unit were collected from a broad array of sources, including electronic medical records, routine clinical modules, incident forms, and shift-based project specific logs. The purpose of the current paper was twofold: (i) to report admission-level adverse incident rates (e.g. aggression and absconding), as well as service efficiency (e.g. average length of stay) and effectiveness indices (e.g. early readmission rates); and (ii) to examine relationships among these key outcome and performance measures and associations with potential sociodemographic risk factors (e.g. gender, age group, marital status), preadmission factors (e.g. previous admission history), and concurrent, admission-related factors (e.g. legal status on admission, discharge diagnosis). Few investigators have assessed the range of outcomes reported here, using data from multiple health services and inpatient units.
Method
Participants and data sources
All of the acute inpatient units from three New South Wales area health services (Hunter, Illawarra and South Western Sydney) participated in this project, which included eight general psychiatric units (3×20, 24, 25, and 3×30 beds), two high-dependency units (8 and 9 beds), and one specialized unit (16 beds) for patients with comorbid substance abuse. For these three categories of units, the average number of occupied beds during the 12 month evaluation were, respectively, 21.94 (SD = 5.36), 7.74 (SD = 1.06) and 12.49 (SD = 2.58) beds, totalling >74 000 bed days for the year, with an average occupancy rate of 88.4%. The corresponding average numbers of nursing staff per occupied bed were 0.27, 0.35 and 0.22.
An ASP data resources guide has been prepared (available from the authors), which outlines the primary data sources, main measures and aggregated datasets, and examines potential data-reporting biases. Three main categories of data were collected: admission-level sociodemographic and clinical data; patient-level events data; and unit-level events data. These data were able to be aggregated in a variety of ways, depending on the research questions of interest. For this service evaluation project, formal approval from regional ethics committees was not required because the primary data were based on observations and ratings by local clinicians from within the participating services.
Admission-level data collection
During the 12 month evaluation there were 5546 admissions to the 11 participating units recorded in the state-wide Health Information Exchange (HIE), excluding admissions resulting in a direct transfer within the same mental health service. The HIE is a de-identified electronic medical records database that includes basic sociodemographic, clinical, admission and discharge information for each admission. We extracted HIE data at a local health service level, prior to its inclusion in the data exchange, so that it was in a common format but nevertheless able to be combined with other regional health service data (primarily using medical record numbers, mental health unit codes, and admission and discharge dates). The 5546 index admissions involved 3877 individual patients (2210 male, 1667 female). For 3759 (67.8%) of these admissions, we were able to supplement the HIE data with more comprehensive clinical data from the routine clinical modules that were introduced into the participating services during this project (e.g. triage, initial assessment, and lifetime history modules).
Patient-level events data collection
To record patient-level events on a routine, shift-by-shift basis, a patient daily log (PDL) was devised. This required the nurse responsible for each patient during the shift to note several aspects of their care and engagement (e.g. observation levels; contacts with staff and visitors; periods of leave; structured therapy participation; medications used) and to complete ratings of their observed mental state (OMS) and aggressive incident status. In the latter case up to three aggressive incidents per patient per shift could be rated using the Morrison eight-level hierarchy [36]. Following Owen et al. [37], incidents rated as 1–4 (i.e. involving physical contact or a definite intention to inflict harm) were regarded as serious or reportable aggressive incidents, in that they typically triggered the completion of an additional, more detailed incident form: a standardized Aggressive Incident Form (AIF) was used by two services (which included the Yudofsky et al. Overt Aggression scale [38]) and a generic incident form by the other service, although completion status was variable. Incidents rated 5–8 on the Morrison hierarchy (i.e. verbal threats or demands without a plan to inflict harm) were regarded as less serious (or non-reportable). The OMS was a locally devised short observational measure of current mental state, which covered five domains (emotional distress, withdrawal, disinhibition, psychosis, and cognitive impairment). The nurse responsible for each patient also recorded ‘whether the patient left the unit during the shift for any period of time, and if this time was authorized or not’. Overall, 86 688 PDL records were completed (comprising 42.3% of potential reporting occasions).
Unit-level events data collection
A ward event log (WEL) was also devised, which required the nurse in charge of each shift to record factors such as: bed availability and usage; ward movements (i.e. patient transfers, admissions, discharges); the number of involuntary patients; level of nursing experience; current staffing demands; and the number of incident forms completed during the shift. A Shift Climate Ratings (SCR) scale was also embedded in the WEL, which required the nurse in charge to complete four anchored ratings about the levels of tension, conflict, activity and social cohesion within the unit during the shift; these ratings could be summed to provide a total shift climate rating out of 10. Shifts were labelled by their approximate starting times (day: 07:00 hours; afternoon: 15:00 hours; night: 23:00 hours). The overall completion rate for the WEL was 69.9% (n = 8306 records).
Key outcome and predictor variables
Aggregated patient-level events data, which were available for 3242 admissions (58.5%), were used to define three of the five key admission-level outcome measures: (i) reportable (serious) aggressive incident status, admissions for which at least one reportable incident was recorded (i.e. the equivalent of 1–4 on the Morrison hierarchy [36]), either on the PDLs or the incident forms (n = 379 admissions, or 11.7%, unweighted); (ii) less serious aggressive incident status, admissions for which at least one less serious incident was recorded (i.e. the equivalent of 5–8 on the Morrison hierarchy [36]), either on the PDLs or the incident forms (n = 502 admissions, or 15.5%, unweighted); and (iii) absconding status, admissions with at least one PDL-recorded unauthorized leave incident (n = 507 admissions, or 15.6%, unweighted). The other two key admission-level outcome measures were derived from the HIE dataset (n = 5546 admissions): (i) length of hospital stay, the number of days between the admission and discharge dates, with any discharges on the same day as admission coded as a 1 day admission if they exceeded 4 h duration (mean length of stay = 14.59 days, SD = 21.77, median = 8.00 days); and (ii) early readmission status, admissions with a subsequent unplanned, early readmission (within 28 days of the index admission) to the same mental health service (n = 965 admissions, or 17.4%).
We adopted a pragmatic approach to the selection of potential predictor variables, effectively choosing variables that would be generally easier to obtain or assess (such as the more routine variables recorded in the HIE) and those with some previous evidence of associations with the selected short-term outcome variables. Because many of the potential predictors would be likely to be interrelated (e.g. unit type, legal status on admission, primary diagnosis), we also gave priority to some variables over others. For example, variables reflecting legal status on admission (i.e. voluntary vs involuntary) and discharge diagnosis were preferred over contrast-coded variables examining differences between specific units or services, in part because of the more universal relevance of such predictor variables, but also to preserve the anonymity of the 11 participating units. The categorical predictor variables of primary interest were gender; age group; marital status; legal status on admission; history and timing of previous psychiatric admissions; and ICD-10 discharge diagnosis (where we focused on diagnostic categories applying to >10% of admissions).
Statistical analysis
Data entry, aggregation and analysis techniques primarily involved Microsoft Excel programs and SPSS statistical software (version 14.0; SPSS, Chicago, IL, USA). χ2 tests or simple logistic regressions (expressed as odds ratios, ORs) were used to assess univariate associations between categorical variables. Multivariate logistic regressions were used when other factors were also taken into account (expressed as adjusted odds ratios, AORs). For the continuous outcome variables the comparable analyses were planned comparisons from analyses of variance (ANOVAs) or covariance (ANCOVA), which were used to assess group differences and patterns of change across the course of the admission (while controlling for selected covariates). Considering the relatively large sample sizes, and as a partial control for the number of statistical tests conducted, the threshold for statistical significance was set at p < 0.001 for all analyses. Weighting factors were also used in calculating overall admission-level adverse incident rates, to attempt to redress potential data-reporting biases. In practice we used the HIE sociodemographic and clinical profiles as a reference point (n = 5546 admissions) and re-scaled the aggregated patient-level events data accordingly (n = 3242 admissions), adjusting for modest data availability biases associated with health service, gender, age group, legal status on admission, and discharge diagnosis.
Results
Sample characteristics and biases
Male subjects were overrepresented (55.0%) among the index admissions, while almost two-thirds (64.5%) of these admissions involved patients aged below 40 years (mean = 37.12 years, SD = 14.42; distribution: under 25, 18.8%; 25–39, 45.7%; 40–54, 23.3%; 55 + years, 12.2%). The majority of admissions were of patients who had never married (59.8%) and had a history of psychiatric admissions (60.4%). One in six admissions (16.0%) was associated with a prior admission within 28 days of the index hospitalization. Almost half (47.6%) of the admissions were involuntary and one-quarter (24.0%) included some time in a high-dependency unit, where this option was available. Schizophrenia and related psychoses was the most frequent primary diagnostic category on discharge (33.3%), but a more accurate picture of the range of ICD-10 discharge diagnoses emerges from the multiple diagnostic assignments. Drug and alcohol use disorders (44.6%) were the most frequent, followed by schizophrenia and related disorders (38.0%), depression (25.3%), personality disorder (18.9%), adjustment disorder (14.2%), and bipolar disorder (14.0%). Comorbid physical disease was also recorded for more than one-third (35.9%) of admissions.
Acuity of presentations (from the triage module, n = 1840 admissions) was generally high, with 23.3% of admissions being in the top three triage categories (‘life threatening’, 2.1%; ‘emergency’, 5.4%; and ‘urgent’, 15.8%). This was further reflected in the risk assessments (from the initial assessment module, n = 2914 admissions), with ‘moderate’ and ‘high or extreme’ levels, respectively, being recorded for: risk of self-harm (30.9%, 13.4%); suicide (25.1%, 9.3%); absconding (18.9%, 12.0%); and harm to others (18.0%, 8.2%); totalling 26.1% of admissions with at least one ‘high or extreme’ rating. A recent suicide or other self-harm attempt was also documented in 16.3% of these admissions. High bed occupancy rates (i.e.>90% occupancy) were reported for 45.9%, 57.1% and 24.5% of shifts, respectively, in the general, high-dependency, and specialized units (χ2 (2)=270.56, p < 0.001). On average, 64.7% of beds were occupied by involuntary patients, with high rates (i.e. >75% involuntary) being typical of shifts in high-dependency units (99.1% of shifts), compared with general units (12.7%) and the specialized unit (5.7%; χ2 (2)=4975.71, p < 0.001). Overall, additional staffing demands (i.e. rated as ‘moderate’ or ‘high’ on the WEL) were reported for 41.5% of shifts, being reasonably similar in the general (47.0%) and high-dependency (42.5%) units, but less likely in the specialized unit (9.4%; χ2 (2)=487.87, p < 0.001). Participation in structured therapy was also very low, being noted on only 7.2% of PDLs from day or afternoon shifts.
A series of logistic regression analyses was conducted, with selected HIE-based variables as the predictors and data availability status (in the aggregated patient-level events dataset) as the outcome variable. Moderate associations were identified with several variables. For example, patients who were married or in a de facto relationship were underrepresented (AOR = 0.70) in relation to the availability of aggression and absconding data, whereas age group 40–54 years (AOR = 1.39) and having spent some time in a high-dependency unit (AOR = 1.60) were overrepresented. From the multiple diagnostic listings, schizophrenia (AOR = 1.44) and bipolar disorder (AOR = 1.39) were overrepresented and adjustment disorder was underrepresented (AOR = 0.71), suggesting that nursing staff were more likely to notice and record the behaviours of the former groups. There was also a tendency (p = 0.002) for female (AOR = 0.84) and voluntary patients (AOR = 0.84) to be underrepresented. These analyses enabled potential bias in reporting aggression and absconding to be taken into account in subsequent analyses and interpretation of the data. The ASP data resources guide (available from the authors) provides further details about sample characteristics, possible data reporting biases, and weighting strategies.
Incident and admission profiles
Raw PDL aggressive incident profiles are reported in the upper portion of Table 1. Overall, there were 1578 PDLs on which at least one aggressive incident was recorded, which represents only 1.8% of the PDLs. For every log that recorded a reportable incident (255 PDLs, totalling 271 incidents), there were at least five that recorded a less serious incident (1386 PDLs, totalling 2826 incidents). Across the eight levels of the Morrison hierarchy [36], there were generally comparable distributions for male and female subjects, with the only exception being level 6 (‘approached another in a threatening way’), which, if recorded, was more likely to be noted for male than female subjects (20.0% vs 10.9%, χ2 (1)=23.40, p < 0.001). In addition, there were 1150 PDLs (1.3%) on which at least one absconding incident was recorded, with slightly higher rates for male than female subjects (1.5% vs 1.1%, χ2 (1)=34.05, p < 0.001).
Adverse incidents by gender: raw PDL counts and admission-level rates
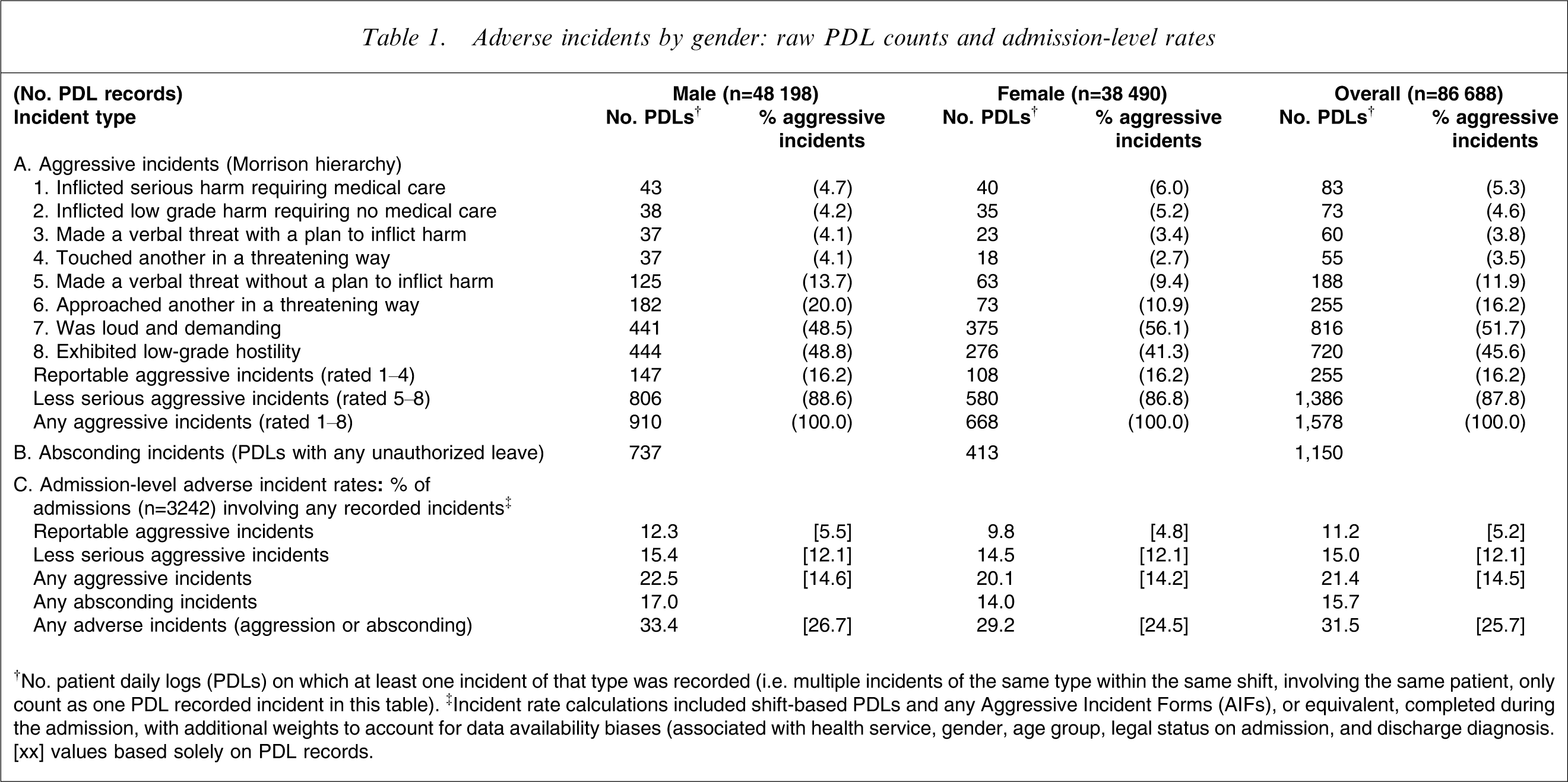
†No. patient daily logs (PDLs) on which at least one incident of that type was recorded (i.e. multiple incidents of the same type within the same shift, involving the same patient, only count as one PDL recorded incident in this table). ‡Incident rate calculations included shift-based PDLs and any Aggressive Incident Forms (AIFs), or equivalent, completed during the admission, with additional weights to account for data availability biases (associated with health service, gender, age group, legal status on admission, and discharge diagnosis)
[xx] values based solely on PDL records.
Figure 1 illustrates the timing of these PDL aggressive and absconding incidents relative to the number of days since admission. The percentage of PDL records on which incidents were recorded is displayed for each successive block of days (excluding night shifts). Logistic regression analyses were used to assess patterns of change across these blocks, using polynomial trend contrasts. The rate of less serious aggressive incidents was maximal in the first 24 h after admission, declined slightly during the next few weeks, and then dropped further during longer admissions (>28 days). This pattern is reflected in statistically significant linear and cubic trends across days since admission (linear trend: Wald-statistic, W(1)=174.25, p < 0.001; cubic trend: W(1)=25.43, p < 0.001). The rate of reportable aggressive incidents displayed no significant reduction over time. In contrast, absconding incidents increased early after admission and peaked in the second week, declining thereafter (quadratic trend: W(1)=31.96, p < 0.001).
Rates of aggressive incidents and absconding per shift across the course of the admission (n = 54 285 patient daily log (PDL) records from day and afternoon shifts).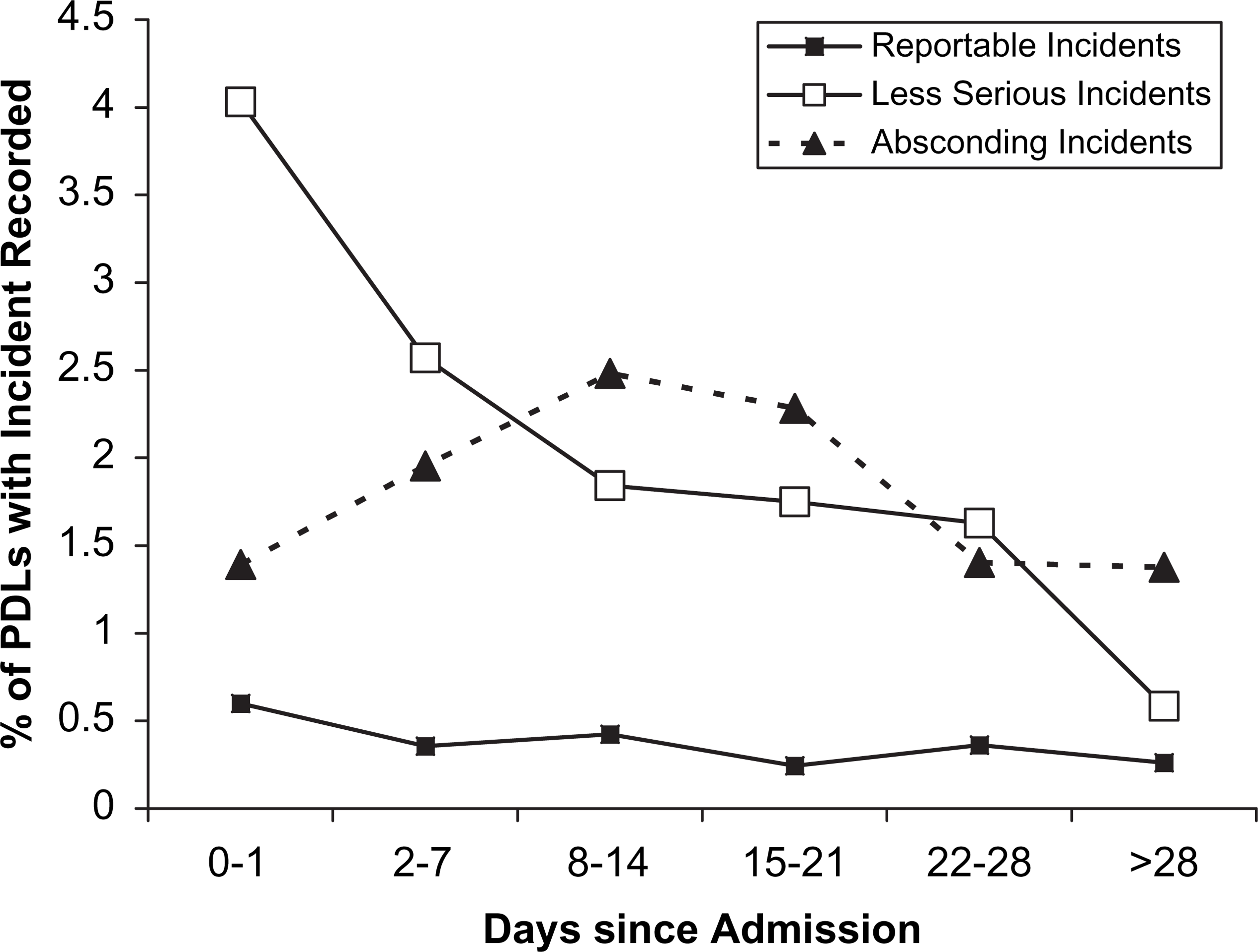
The pattern of incidents recorded on the 1145 incident forms (977 standardized AIFs and 168 generic forms) differed from that noted on the PDLs because these forms were typically used for detailing more serious incidents, although the threshold for form completion varied across the participating units. Importantly, these forms were generally completed by staff who had witnessed the particular incident, while the PDLs were mostly completed by the nurse responsible for the patient during that shift. Three-quarters (74.1%) of the specific incident forms recorded at least one reportable aggressive incident, while 58.3% recorded at least one less serious aggressive incident, with 35.0% identifying both types of aggressive incidents.
Admission-level aggressive incident status for each patient (with any PDLs) was based on a combination of PDL and incident form data. In addition, overall admission-level adverse incident rates were weighted to account for data availability biases (associated with health service, gender, age group, legal status on admission, and discharge diagnosis). The lower portion of Table 1 reports weighted admission-level adverse incident rates by gender. It was estimated that one-fifth (21.4%) of admissions involved an aggressive incident, including 11.2% with at least one reportable incident and 15.0% with at least one less serious incident. The corresponding rates based solely on the PDLs were: 14.5%, 5.2% and 12.1%. It was further estimated that one-sixth (15.7%) of admissions included an episode of absconding. Consequently, 31.5% of admissions involved at least one adverse incident (i.e. aggression or absconding). Comparable admission-level rates of adverse incidents were observed for male and female subjects (Table 1).
In addition to admission-level incident rates, we also estimated the rates of aggressive incidents per month per occupied bed, using aggregated PDL and incident form data for shifts with at least a 25% PDL completion rate. The overall estimated rate of reportable aggressive incidents per month per occupied bed was 0.55 incidents, while the corresponding rate for less serious aggressive incidents was 3.73. It was also estimated that there were almost twice as many reportable aggressive incidents per month per occupied bed in the high-dependency units (0.97) than in the general units (0.53), which, in turn, had more than twice the rate of the specialized unit (0.21). Similarly, there were six to nine times as many non-reportable aggressive incidents per month per occupied bed in the high-dependency units (15.96) than in the specialized unit (2.34) or the general units (1.72).
Because complete data were available for the two HIE-based outcome measures (i.e. length of stay and early readmission status), no weighting factors were required. The mean length of stay (14.59 days, SD = 21.77) was shorter for male than female subjects (14.07 vs 15.24 days), although this difference was not statistically significant, and both subgroups had the same median length of stay (8.00 days). Approximately one-quarter of hospital admissions were for ≤2 days (distribution: 0–2 days, 24.0%; 3–7 days, 25.8%; 8–14 days, 19.1%; 15–21 days, 10.6%; 22–28 days, 6.4%; >28 days, 14.2%). One-sixth of the index admissions (17.4%) involved a subsequent readmission within 28 days (i.e. an unplanned, early readmission), with lower rates among male than female subjects (14.6% vs 20.8%, χ2 (1)=36.06, p < 0.001).
Relationships among key short-term outcome measures
Table 2 reports relationships among the five selected outcome measures, including univariate associations and adjusted associations (controlling for gender, age, marital status, admission history, legal status on admission, discharge diagnosis, health service, and, where appropriate, length of stay). Almost one-third (31.5%) of admissions involving less serious aggressive incidents also involved at least one reportable aggressive incident, compared with 8.1% of admissions without any evidence of less serious incidents, representing a fivefold increase in the relative odds (OR = 5.24), even after adjusting for the selected covariates (AOR = 4.78). Admissions involving less serious aggressive incidents were also more likely to involve an absconding incident (30.3% vs 13.0%, OR = 2.92), but this difference was non-significant after controlling for the covariates. Admissions involving reportable aggressive incidents were not associated with a significant increase in the rate of absconding, but they were associated with a higher likelihood of an unplanned, early readmission (21.6% vs 14.8%, AOR = 1.74). Adverse incident status was also strongly associated with length of stay, even after controlling for the contribution of important factors such as age, legal status, and discharge diagnosis. Admissions involving less serious aggressive incidents, reportable incidents, and episodes of absconding, respectively, were typically more than 8, 11, and 12 days longer than those without such incidents. Conversely, index admissions that were followed by an unplanned readmission within 28 days were, on average, 2½ days shorter than those without a subsequent early readmission.
Relationships between selected short-term outcome measures
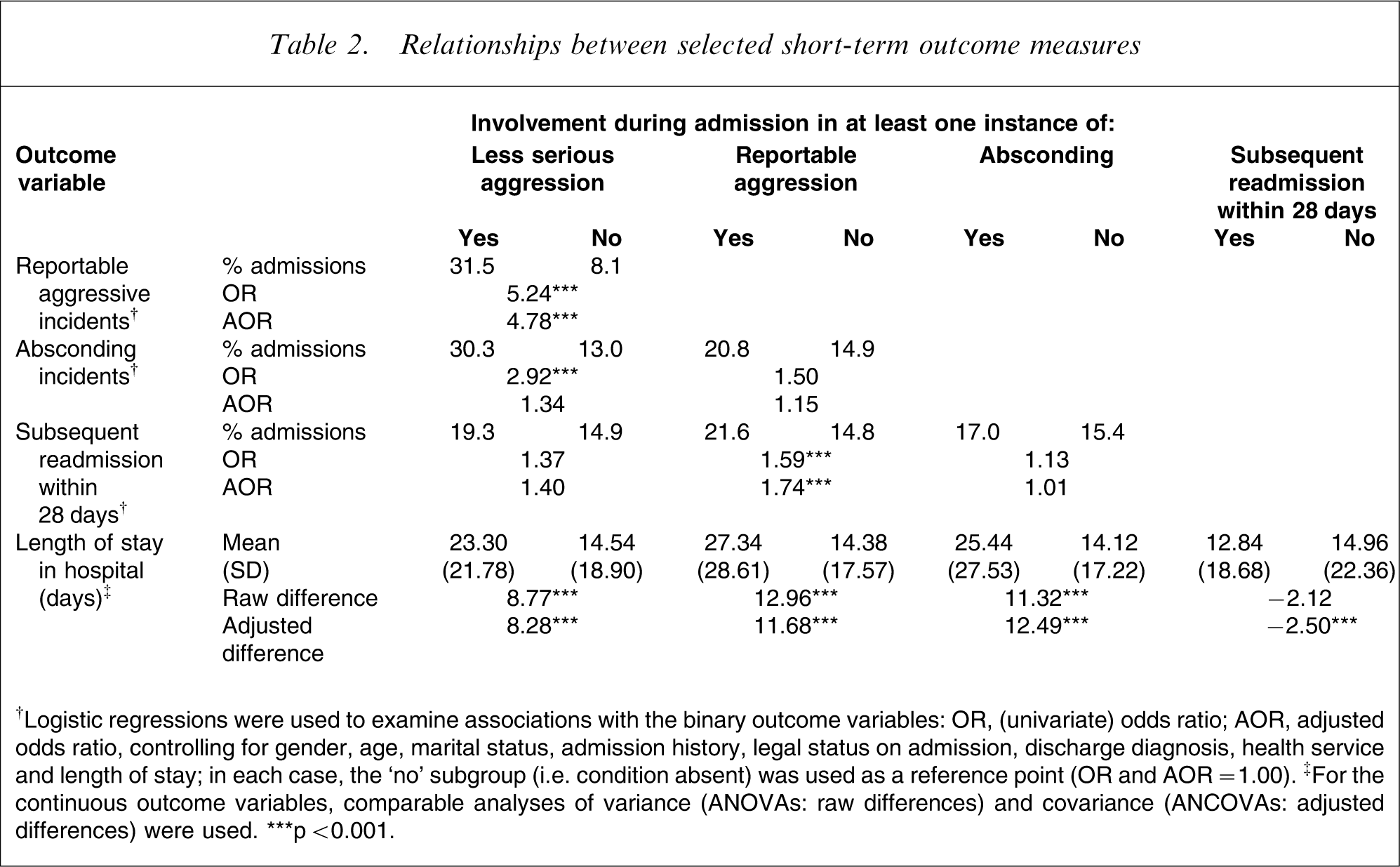
†Logistic regressions were used to examine associations with the binary outcome variables: OR, (univariate) odds ratio; AOR, adjusted odds ratio, controlling for gender, age, marital status, admission history, legal status on admission, discharge diagnosis, health service and length of stay; in each case, the ‘no’ subgroup (i.e. condition absent) was used as a reference point (OR and AOR = 1.00). ‡For the continuous outcome variables, comparable analyses of variance (ANOVAs: raw differences) and covariance (ANCOVAs: adjusted differences) were used.
∗∗∗p < 0.001.
The observed associations between adverse incident status and length of stay raised several possibilities: involvement in adverse incidents may itself be an indicator of illness severity and/or level of risk; other clinical characteristics or features of the treatment setting may impact jointly on aggression, absconding and length of stay; duration of stay in an aversive or restrictive environment may precipitate aggression or absconding; and longer admissions may simply have an increased probability of such incidents being noticed or recorded. To further explore these issues we conducted a series of logistic regressions examining differences in rates of adverse incidents across several length of stay subgroups (while controlling for the covariates identified earlier). As shown in Table 3, the likelihood of an aggressive or absconding incident being registered increased in an essentially linear fashion with length of stay (4.8–27.6% for reportable incidents, 6.4–28.5% for less serious incidents, and 2.8–29.7% for absconding incidents). The consistency and magnitude of these associations tend to suggest that length of stay-related effects need to be carefully considered and controlled, especially when examining associations between aggregated admission-level outcome indices and other factors.
Relationships between length of stay, aggression and absconding status (n = 3242 admissions)
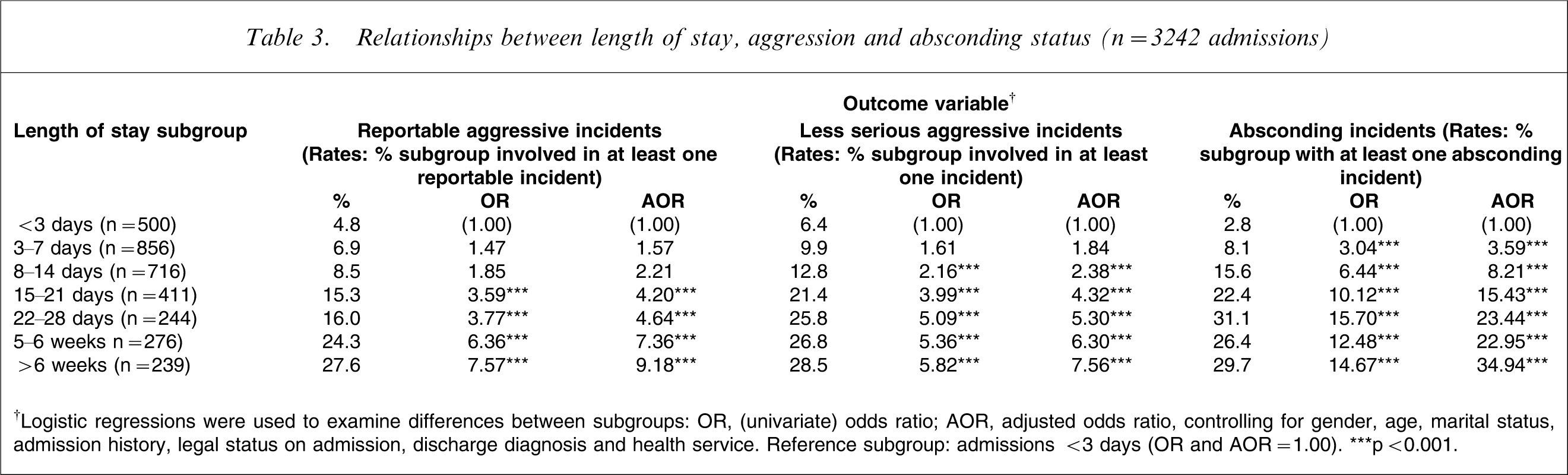
†Logistic regressions were used to examine differences between subgroups: OR, (univariate) odds ratio; AOR, adjusted odds ratio, controlling for gender, age, marital status, admission history, legal status on admission, discharge diagnosis and health service
Reference subgroup: admissions <3 days (OR and AOR = 1.00)
∗∗∗p < 0.001.
Predictors of aggression and absconding
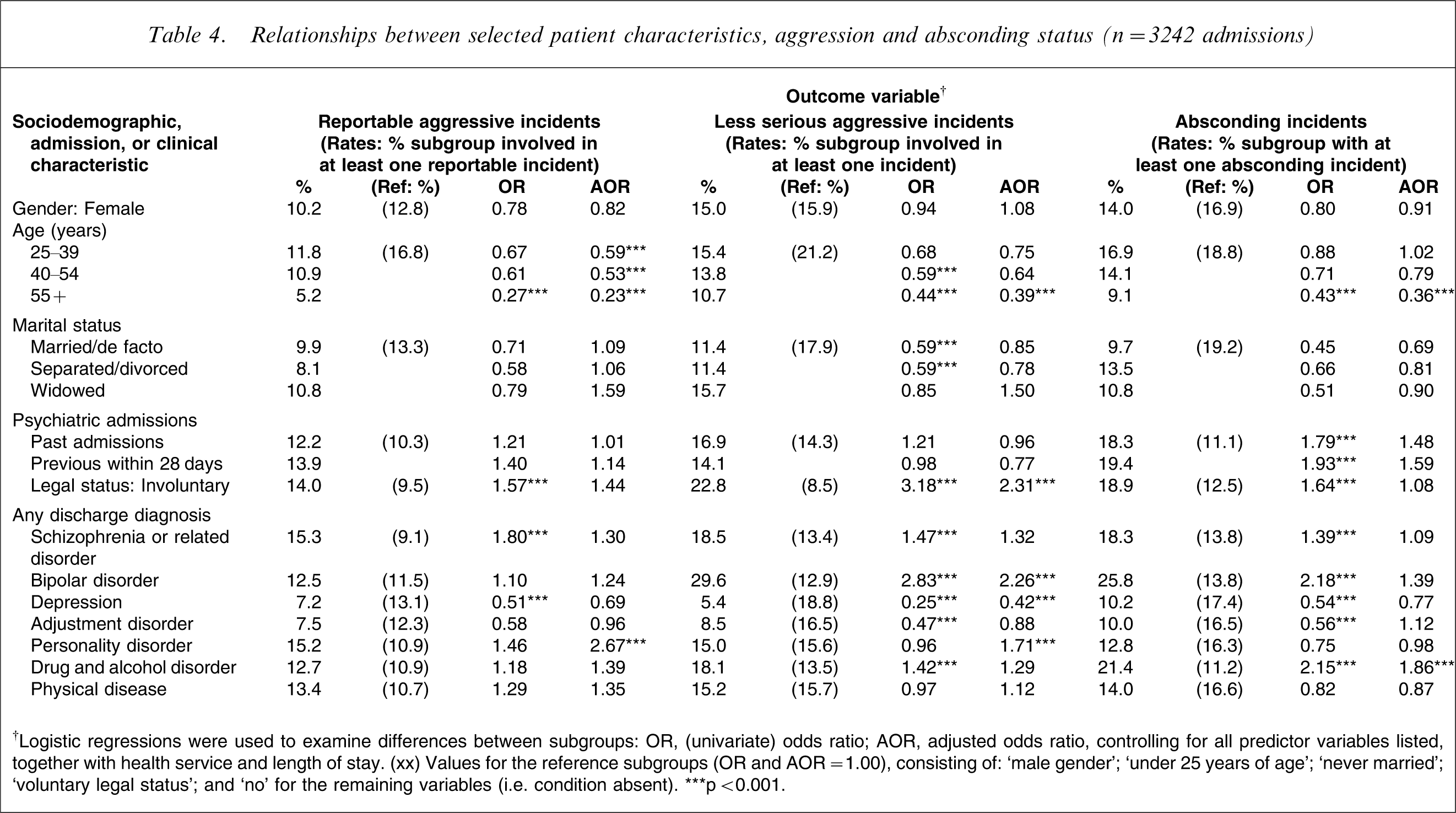
Table 4 reports relationships between selected sociodemographic, admission and clinical characteristics and admission-level adverse incident status, including univariate associations (ORs) and adjusted associations (AORs), controlling for all of the predictor variables, together with health service and length of stay. The parenthetical values in Table 4 are for the reference subgroups (e.g. male, under 25 year olds, voluntary admissions), for which OR and AOR = 1.00. Several of the predictor variables displaying univariate associations with reportable aggressive incident status (i.e. involuntary legal status on admission, OR = 1.57; schizophrenia or a related diagnosis, OR = 1.80; and depression, OR = 0.51) were no longer statistically significant after the chosen covariates were taken into account. But the picture that emerged from the multivariate associations was very straightforward, with a lower likelihood of (any) reportable incidents being observed among all of the older age groups, relative to patients under 25 years of age (5.2–11.8% vs 16.8%, AOR = 0.23– 0.59), and a higher likelihood among those with a discharge diagnosis of personality disorder (15.2% vs 10.9%, AOR = 2.67).
Relationships between selected patient characteristics, aggression and absconding status (n = 3242 admissions)
†Logistic regressions were used to examine differences between subgroups: OR, (univariate) odds ratio; AOR, adjusted odds ratio, controlling for all predictor variables listed, together with health service and length of stay.
(xx) Values for the reference subgroups (OR and AOR = 1.00), consisting of: ‘male gender’; ‘under 25 years of age’; ‘never married’; ‘voluntary legal status’; and ‘no’ for the remaining variables (i.e. condition absent)
∗∗∗p < 0.001.
Being single, having a diagnosis of schizophrenia or a related disorder, a drug and alcohol disorder, or the absence of an adjustment disorder, were all associated with a higher likelihood of involvement in less serious aggression, but only in the univariate analyses (Table 4). After controlling for the covariates, five variables made a significant contribution to the prediction of less serious aggression. Patients in the oldest age group (55+, AOR = 0.39) and those with a diagnosis of depression (AOR = 0.42) were less likely to be involved in such incidents, while involuntary admissions (AOR = 2.31) and those with a diagnosis of bipolar (AOR = 2.26) or personality disorder (AOR = 1.71) were more likely to be involved in less serious aggression. A reasonably similar profile emerged among the univariate associations for absconding status, with previous psychiatric admission history making an additional contribution. But, once again, a straightforward picture emerged in the multivariate analyses, with the oldest age group (55+, AOR = 0.36) being less likely to abscond and those with a drug and alcohol disorder being more likely to abscond (on at least one occasion; AOR = 1.86).
Predictors of length of stay and early readmission
The left-hand columns of Table 5 display findings from parallel ANOVA (raw differences)- and ANCOVA (adjusted differences)-based analyses for length of stay, the only continuous outcome variable. On a univariate basis all of the predictor variable categories, except gender, were significantly associated with length of stay (i.e. age, marital status, admission history, legal status on admission and discharge diagnosis). Once again, a very straightforward picture emerged from the multivariate analyses. Significantly longer admissions were experienced by the oldest age group (55 +), who stayed an average of 8.25 days longer than those under 25 years, as well as by involuntary admissions (2.56 days longer) and those with schizophrenia (8.04 days longer), bipolar disorder (6.20 days longer), or physical disease (6.01 days longer).
Relationships between selected patient characteristics, length of stay and early readmission (n = 5546 admissions)
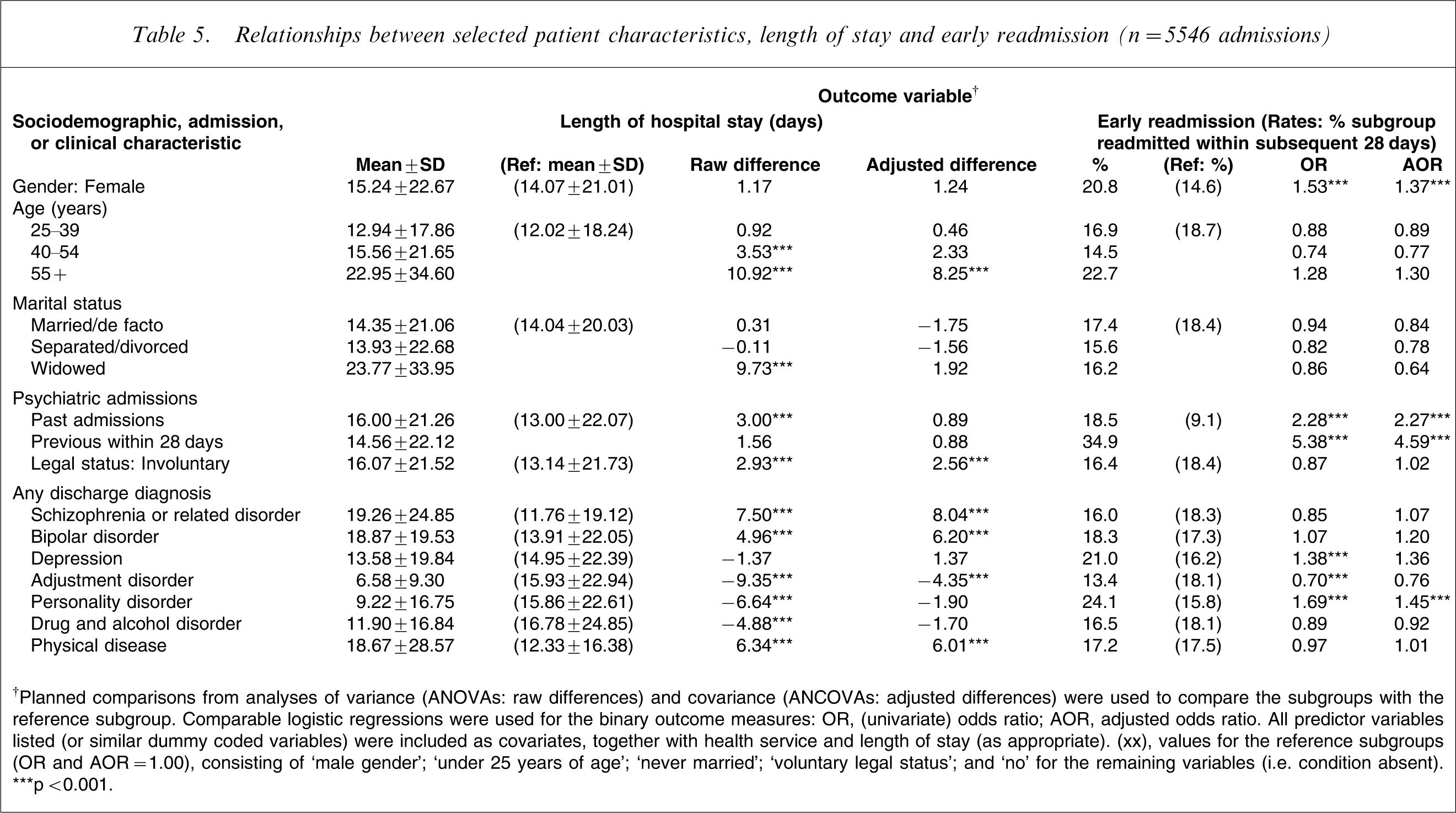
†Planned comparisons from analyses of variance (ANOVAs: raw differences) and covariance (ANCOVAs: adjusted differences) were used to compare the subgroups with the reference subgroup. Comparable logistic regressions were used for the binary outcome measures: OR, (univariate) odds ratio; AOR, adjusted odds ratio. All predictor variables listed (or similar dummy coded variables) were included as covariates, together with health service and length of stay (as appropriate).
(xx), values for the reference subgroups (OR and AOR = 1.00), consisting of ‘male gender’; ‘under 25 years of age’; ‘never married’; ‘voluntary legal status’; and ‘no’ for the remaining variables (i.e. condition absent)
∗∗∗p < 0.001.
The right-hand columns of Table 5 report comparable analyses (similar to those in Table 4) for the early readmission status outcome variable. In this instance the profiles produced in the univariate and multivariate analyses were very similar. Overall, rates of early readmission were higher among index admissions of female patients (20.8% vs 14.6%, AOR = 1.37), those with past admissions (18.5% vs 9.1%, AOR = 2.27) and those with previous admissions within the last 28 days (34.9% vs 9.1%, AOR = 4.59). Personality disorder was also associated with an increased likelihood of early readmission, even after all of the other sociodemographic, admission and clinical variables were controlled (24.1% vs 15.8%, AOR = 1.45).
Discussion
The five selected admission-level outcome measures can be viewed as overlapping service performance indicators or dimensions of inpatient mental health service quality [39]. The first three (i.e. reportable and less serious aggression, and absconding) are clearly adverse incidents, which have potential safety implications for patients and staff, but they also reflect a mixture of service demands and appropriateness. Adverse inpatient incidents are not entirely avoidable because one of the criteria for admission and involuntary detention is risk of harm to self and others, but their rates of expression are also likely to be influenced by care and setting factors [12]. Average length of stay is essentially a process variable or barometer that reflects a mixture of service demands, appropriateness and efficiency, while the rate of unplanned, early readmissions can be viewed as a short-term index of service effectiveness. The importance of these outcomes is highlighted by the fact that several are now listed in the key performance indicators for mental health services [40] or examined during Australian hospital accreditation processes [39].
Acuity of presentations
The majority of patients were aged under 40 (64.5%) and had never married (59.8%), a reminder that severe mental illness requiring inpatient care is predominantly a problem among younger age groups and those without enduring stable relationships. Also striking was the relatively high acuity of clinical presentations, on the basis of the initial triage categories and triage risk ratings for self-harm (44.3%), suicide (34.4%), absconding (30.9%) and harm to others (26.2%). Overall, the patient sample was severely and acutely unwell, which is reflected in the high proportion of involuntary admissions (47.6%) and the high rates of past psychiatric admissions (60.4%).
Substance use disorders, schizophrenia and related psychoses were the commonest psychiatric diagnoses, each of which has been linked to high rates of hospitalization and readmission [29], [41] and aggressive behaviour [4], [10]. More than one-third of admissions (35.9%) was associated with a diagnosis of significant physical disease, which highlights the extent of medical comorbidity and the importance of readily available resources and expertise in general medicine within psychiatric inpatient facilities. Overall, the clinical and sociodemographic characteristics of the present sample were very similar to those reported by Owen et al. [37].
Bed occupancy levels were also high, averaging 88.4%. When average bed occupancy exceeds 85%, the number of days of full occupancy increases exponentially [42] and regular bed shortages, with periodic crises, can be expected when bed occupancy rises to 90% or more. Thus, for almost half the time (45.9%) the acute general units would have been in this critical range of bed occupancy, with insufficient spare capacity to effectively manage emergency admissions. In fact, additional staffing demands were reported in two of every five nursing shifts.
Adverse incidents: rates and associations
Rates of aggression are likely to vary according to data source, the mix of incidents included, and the timeframes considered. For example, based on a single data source (the PDLs), and considering the admission as a whole, less serious aggressive incidents appear to have more than twice the probability of occurrence as reportable aggressive incidents (12.1% vs 5.2%). The overall rate of PDL aggressive incidents per admission (14.5%) was similar to the 13.7% recorded by Barlow et al. [7], but higher than the 11.6% noted by Grassi et al. [8]. Supplementing the PDL aggression rates with data from incident-based forms, whose completion is triggered by incident occurrence and unit policy, is likely to increase the overall estimates but also to distort the relationships between less serious and reportable incidents (in this instance, to 15.0% vs 11.2%). Based on PDL incident profiles (Table 1), less serious incidents were more than fivefold more likely to be noted per shift than reportable incidents (1386 vs 255 PDL forms), or 10-fold more likely based on overall incident counts (2826 vs 271 incidents). Less serious incidents also peaked during the first 24 h after admission, with a sharp decline over the subsequent 2 weeks (Figure 1), which is consistent with other studies [43]. These rates differ markedly from those reported by Owen et al. [37], where the majority of incidents (58.3%) were rated as serious, reflecting differences in incident reporting thresholds, and further highlighting the value of using routine, fixed reporting strategies such as the PDLs.
Based on incident rates per month per occupied bed, less serious incidents were almost sevenfold more likely to occur than reportable incidents (3.73 vs 0.55). This equates to an overall incident rate per bed of one every 7.1 days, which is similar to the rate reported by Walker and Seifert [6], but less than the violent incident rate reported by Owen et al. [37] of two incidents per month per occupied bed. For high-dependency units the corresponding rates (15.96 vs 0.97 per month per occupied bed) equate to an overall incident rate per bed of one every 1.8 days, clearly fostering the expectation among staff of an ongoing, aggressive workplace [3].
Reportable aggressive incidents were associated with – and can therefore be considered to occur against a background of – the more commonly occurring less serious aggression, as well as being associated with length of stay and an increased rate of unplanned, early readmissions (Table 2). Younger patients were overrepresented among admissions involving reportable aggressive incidents, which is consistent with earlier studies [4], [9], as were patients with personality disorder (Table 4), which is concordant with Nolan et al. [44] and with the Soliman and Reza study in which violence was linked with personality disorder but not with schizophrenia [10]. Although less serious aggression was linked with the same factors (i.e. younger age and personality disorder), it was also associated with involuntary status, bipolar disorder and the absence of a diagnosis of depression (Table 4). The higher rates of less serious aggression observed during the first few days after admission may reflect involuntary status and/or the levels of manic symptoms present at that time, because other studies [13] also reported links between mania and verbal aggression. Patients with severe depression may internalize their aggressive impulses or, alternatively, their anergia may help to prevent them from acting aggressively towards others [10].
There were no appreciable gender differences in rates of aggression in the present study. Previous studies among hospitalized patients have yielded contradictory results [45–48], with some reporting higher rates of less severe aggression in women [46], [49] and at least one study reporting that women were involved in more severe assaults causing injuries [43]. Clearly, the stereotype that male subjects with mental illness engage in substantially more aggressive behaviour is incompatible with the evidence, at least among hospitalized patients. Although inpatient aggression and schizophrenia have often been linked [4], [5], [7], the strength of such associations is also unclear and likely to vary with the methodological approach used. For example, although 38% of the current sample had a diagnosis of schizophrenia or a related disorder, these patients occupied exactly half of the total bed days. Consequently, with respect to simple incident counts, patients with schizophrenia would be expected to account for the highest number of adverse incidents, or any other events, even in circumstances in which there was no causal link between schizophrenia and the outcome of interest. In the current analyses, associations between schizophrenia and increased rates of adverse incidents essentially disappeared after controlling for length of stay-related effects and the other covariates (Table 4).
Absconding rates were comparable for male and female patients, with an overall rate of 15.7%, which was higher than the 12.6% rate reported by Bowers et al. [50]. There was also a tendency for younger patients and those with substance use problems to have a higher likelihood of absconding, which is consistent with earlier studies [14], [15]. Bowers et al. also noted that some of the most common reasons given by patients who absconded were treatment failure and family problems [14]. However, the gradual increase in absconding rates observed during the first 2 weeks (i.e. after the initial, clinically turbulent period in hospital) is just as likely to be associated with a positive initial treatment response, including reduced psychotic and anxiety symptoms, leading to less restrictive care. Absconding may also be related, in part, to attempts to use or obtain alcohol or illicit drugs. Because absconding from acute psychiatric units places patients and others at risk, as well as being burdensome and anxiety-provoking for staff [51], policies and practices need to be strengthened and absconding rates reduced, even if only a small number of patient factors associated with absconding can be identified.
In summary, there were different profiles for each of the categories of adverse incidents: reportable aggression was more likely to be intermittent, unrelated to time since admission, and was most strongly associated with younger age, personality disorder, less serious aggression, longer periods of hospitalization, and subsequent early readmission; less serious aggression was more likely during the initial period of hospitalization and was linked with involuntary status, bipolar and personality disorders, the absence of depression, younger age, and longer hospital stays; while absconding tended to peak during the second week of the admission and was associated with drug and alcohol disorder, younger age, and longer periods of hospitalization. The estimated overall rate of adverse incidents (around 25–30%), which included aggressive incidents (15–20%), was clearly outside of the acceptable range. But perhaps these rates should not be surprising given the relatively high acuity of clinical presentations and the overall level of comorbidity, which was consistent with the Issakidis and Andrews study [1].
Associations with length of stay and early readmission
The average length of stay of 14.59 days was comparable to Barlow et al. (13.82 days), who also reported much longer stays by patients involved in aggressive incidents (24.88 days) [7]. In the present study, length of stay was significantly associated with all of the outcome variables and several of the predictor variables, which reflects positively on its role as a barometer of the underlying processes. On average, the oldest age group stayed 8 days longer (than those under 25 years), which could reflect differences in support systems, or placement difficulties for a particular subgroup.
The substantial variation in average length of stay across diagnostic groupings (from 6.58 days for adjustment disorder to 19.26 days for schizophrenia; Table 5) supports an association with illness severity [22], [23], but also with variations in levels of risk, treatment efficiency and responsiveness. On average, admissions involving schizophrenia were 8 days longer (than those without this disorder), those involving bipolar disorder or physical disease were 6 days longer, while those involving adjustment disorder were 4 days shorter. Other studies have also found associations between an increased length of stay, schizophrenia [24] and comorbid medical conditions [25]. Shorter stays by patients with adjustment disorder may indicate a more rapid resolution of the particular factors contributing to admission, greater responsiveness to any pharmacological or psychosocial interventions, or better support systems. On average, admissions involving reportable aggression, less serious aggression, or absconding were 11, 8, and 12 days longer, respectively, which is generally consistent with earlier studies [4], [7]. This suggests that, regardless of diagnosis, the presence of an adverse incident is itself an indicator of illness severity and/or treatment responsiveness or, at the very least, a guide to ongoing risk (of harm to self or others), which is a basis for retention in hospital.
The overall rate of readmission within 28 days (17.4%) exceeded the proposed benchmark figure of 10% used in recent population-based mental health service provision models [52]. Factors such as the high acuity of presentations, average occupancy rates around 90%, and the relatively short median length of stay, may be contributing to suboptimal discharge planning and poorer linkages with community-based services. Furthermore, the impact of these factors could be different for some groups of patients. For example, rates of early readmission were higher among female patients and those with previous admission histories or personality disorder. There may also be a subgroup of women with low levels of support, particular patterns of behaviour (e.g. self-harm) and multiple early readmissions, who account for the observed effects [2], [53].
In the present study there was a fourfold increase in the likelihood of an early readmission among patients for whom the current admission was itself an unplanned, early readmission (34.9% vs 9.1%). These findings demonstrate that, despite some evidence to the contrary [41], the concept of a revolving door [19], [29] is a reality for a small subgroup of patients, particularly younger women with personality disorder, and perhaps also for patients involved in reportable aggressive incidents. It may also be possible that extending the length of stay of those at risk for early readmission, by approximately 2 days to consolidate discharge plans, would reduce the readmission rate. But such an extension may not impact on subsequent hospitalization [54] and there may even be subgroups among whom a longer stay is predictive of readmission [41].
In summary, longer periods of hospitalization were associated with involuntary status, involvement in aggression and absconding incidents, diagnoses of schizophrenia, bipolar disorder or comorbid physical disease, the absence of adjustment disorder, and with older age, while the likelihood of a subsequent unplanned, early readmission was linked with female gender, personality disorder, a previous admission history, and a shorter hospital stay during the index admission.
Limitations
The current dataset largely consisted of naturalistic clinical information from acute adult psychiatric inpatient units, which was collected by clinical staff of those units and systematically compiled for this evaluation. Being part of routine clinical work, there was variation between units and over time in data-collection policies and practices. For example, PDLs were completed for around half of the potential reporting occasions, with some subgroups having disproportionate representation. A mixture of factors are likely to contribute to potential biases, including patient and staff characteristics, and variations in reporting practices. Patients with different risk profiles on admission may attract different levels of care or staff reporting responsibilities or, alternatively, some patients may simply display behaviours that increase their likelihood of being noticed. But in broad terms we consider the reporting biases observed in the present study to be small to moderate. For example, unweighted aggression rates were only slightly higher than the weighted estimates (reportable incidents: 11.7% vs 11.2%; less serious incidents: 15.5% vs 15.0%).
The other limitations of this project included an absence of patient self-report data (e.g. on symptoms, treatment engagement); reliance on short-term outcomes; and the lack of preadmission and post-discharge information from community-based services (e.g. relating to treatment history and continuity of care). In the present paper the emphasis was also on admission-level analyses, which raised some analytical issues that other studies have failed to address. For example, as illustrated in Table 3, the likelihood of any adverse incident being registered during an admission rose in a linear fashion with length of stay, even after controlling for a range of sociodemographic, clinical and service factors. Although several explanations are possible, the two that we favour most are (i) a simple measurement effect, namely, the larger the sample of a person's behaviour that is observed (in this instance, an increasing number of shifts), the more likely it is that at least one instance of a given behaviour will be recorded; and (ii) all other predictors aside, involvement in adverse incidents may itself be a useful indicator of illness severity, or greater risk, and therefore associated with an increased length of stay. At the very least, the analyses reported here suggest that potential length-of-stay-related effects need to be considered when examining associations between sociodemographic, clinical and setting factors and aggregated admission-level outcomes (or, alternatively, indices of interest should be expressed as rates per unit of time).
Conclusions
To a substantial degree, the present study's findings are descriptive in nature. They show an acute inpatient mental health system operating under considerable strain (e.g. high acuity levels and rates of involuntary admission; complex comorbidities; occupancy levels within the critical range; limited structured therapy programmes; and substantial rates of unplanned, early readmission). The system was also taxed by moderate to high levels of patient aggression, not just serious aggressive incidents but the more common and constantly wearing instances of threatening behaviour, loud or demanding conduct and low-grade hostility, all of which adds to the picture of a system struggling to manage its patients safely and effectively. We also suspect that many of the sources of strain in contemporary inpatient care lie beyond the bounds of the hospital, including a lack of evidence-based community care, inadequate access to services, and insufficient levels of supported accommodation and supported employment programmes.
The complexities illustrated in the present study, by simultaneously examining several short-term outcome measures, also support the need for a multi-level approach to intervention. Intervention strategies during the first few days following admission may need to focus on minimizing immediate harm, given the risks identified on presentation, the higher levels of less serious aggressive incidents, and the level of clinical acuity during this period. Staff training in risk assessment and management, including aggression minimization [5], [55], is obviously an essential component for this phase of the treatment response. But for many patients specific intervention programmes should ideally be initiated during their hospital stay and formalized within more comprehensive discharge plans that promote continuity of treatment to the community (e.g. specific programmes targeting anger and aggression, absconding risk, treatment adherence, substance abuse, relapse prevention, and broader lifestyle issues, including physical health and smoking). In addition to potential safety benefits for patients and staff, more intensive or better targeted inpatient interventions, which contribute to a more rapid resolution of the factors contributing to adverse inpatient incidents, are also likely to promote more effective inpatient stays, better discharge planning, and fewer unplanned readmissions. However, achieving all of these objectives is likely to be beyond the resources currently allocated to general public sector inpatient mental health care, where median length of stay is as short as 8 days and pressures for rapid patient turnover are so high. The finding that more than one-quarter of admissions involve adverse incidents, and one-sixth result in an unplanned readmission, is evidence that these objectives are not being achieved.
Finally, despite some concerns about potential reporting biases, the naturalistic datasets associated with the present study comprise a substantial multi-level data resource with which to explore relationships between patient, care and setting factors and the selected short-term outcomes. The focus of the current paper was on admission-level rates and indices and associations with sociodemographic and clinical characteristics routinely collected by health services. Future papers will examine shift-level fluctuations in mental state and unit climate, together with the contributions of other patient- and unit-level events to the selected outcomes.
Footnotes
Acknowledgements
The Acute Services Project was sponsored by the Centre for Mental Health (NSW Department of Health and Aged Care, Sydney) and received funding between 1999 and 2002. This project would not have been possible without considerable ongoing support from the three participating health services (Hunter, Illawarra, and South Western Sydney) and we would like to formally acknowledge the assistance received from the nursing, medical, allied health and administrative staff within those services. We would also like to thank the other members of the project steering committee (Beverley Raphael, Scott Clark, Irwin Pakula, Jennifer Chipps, Gavin Stewart, Carolyn Muir, Greg Hugh, Kate Adams and Denise Allen); the project officers (Rachel Garrett, Carol Martin, Debbie Forrester, Jane Walton, Richa Gupta and Ghizala Rashid); the clerical and support staff (Louisa D'Accione, Rhonda Callister, Marcella Hart, Kylie Julian, Karen Flannigan, Tracy McLaughlan, Leah Bennett, Gloria Stoker and Kylie Freeman); our consultants (Lindsay Oades, Brin Grenyer and Mark McEwan); and the regional clinical information management staff (Tony Druce, Chris Lowe, John Taylor, Lyn Kentish, Natalie Fowler and Andrew Muller).